
Abstract
About 350 million people worldwide have type 2 diabetes (T2D). The major risk factor of T2D is impaired glucose tolerance (pre-diabetes) with 10 % of pre-diabetes subjects develop T2D every year. Understanding of mechanisms of development of T2D from pre-diabetes is important for prevention and treatment of T2D. Chronic stress and chronic low-grade inflammation are prominent risk factors for T2D development in pre-diabetic subjects. However, molecular mechanisms mediating effect of stress and inflammation on development of T2D from pre-diabetes remain unknown. One of such mechanisms might involve kynurenine (KYN) pathway (KP) of tryptophan (TRP) metabolism. We suggested that chronic stress- or chronic low-grade inflammation-induced upregulation of formation of upstream KTP metabolites, KYN and 3-hydroxyKYN, combined with chronic stress- or chronic low-grade inflammation-induced deficiency of pyridoxal 5′-phosphate, a co-factor of downstream enzymes of KTP, triggers overproduction of diabetogenic downstream KYN metabolites, kynurenic acid (KYNA) and 3-hydroxyKYNA (also known as xanthurenic acid (XA)). As the initial assessment of our working hypothesis, we evaluated plasma levels of up- and downstream KP metabolites in the same samples of T2D patients. KYN, XA, and KYNA levels in plasma samples of T2D patients were higher than in samples of non-diabetic subjects. Our results provide further support of “kynurenine hypothesis of insulin resistance and its progression to T2D” that suggested that overproduction of diabetogenic KP metabolites, induced by chronic stress or chronic low-grade inflammation, is one of the mechanisms promoting development of T2D from pre-diabetes. Downstream metabolites of KP might serve as biomarkers of T2D and targets for clinical intervention.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
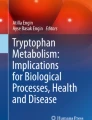
About 350 million people worldwide have type 2 diabetes (T2D). The major risk factor of T2D is impaired glucose tolerance (pre-diabetes) with 10 % of pre-diabetes subjects develop T2D every year. Understanding of mechanisms of T2D development from pre-diabetes is important for prevention and treatment of T2D. Stress [1] and inflammation [2] are prominent risk factors for development of T2D in pre-diabetic subjects. However, molecular mechanisms mediating effect of stress and/or inflammation on development of T2D from pre-diabetes remain unknown. Clinical and experimental data on the involvement of tryptophan (TRP) metabolites in pathogenesis of T2D was reviewed in 1985 [3]. Since its publication, new studies revealed the role of chronic stress and chronic low-grade inflammation in regulation of kynurenine (KYN) pathway (KP) of tryptophan (TRP) metabolism. TRP, an essential (for human) amino acid, is a substrate for biosynthesis of methoxyindoles (serotonin, N-acetylserotonin, and melatonin). Most of TRP (about 95 %) is metabolized along KYN pathway, the major source of NAD in humans [4] (Fig. 1). Stress hormones and/or inflammatory factors (e.g., IFNG and LPS) activate upstream steps of KP, i.e., conversion of TRP into KYN and KYN into 3-hydroxykynurenine (3-HKYN), due to activation of TRP- or indoleamine-2,3-dioxygenases (TDO or IDO), and of KYN-monooxygenase (KMO), respectively [5]. The key enzymes of downstream metabolism of KYN and 3-HKYN require pyridoxal-5-phosphate (P5P) as a co-factor: aminotransferases (KAT), metabolizing KYN into KYNA and 3-HKYN into 3-HKYNA, and kynureninase (KYNase), metabolizing 3-HKYN into 3-HAA [4]. (3H-KYNA was discovered in 1935 and named xanthurenic acid (XA)) [6].

Major up- and downstream steps of tryptophan–kynurenine metabolic pathway
Stress hormones (e.g., cortisol) might cause P5P deficiency by activation of P5P phosphatase [7] while inflammation induces P5P functional deficiency because of increased demand for P5P as a co-factor of more than 200 stress- or inflammation-induced enzymes [8]. Since KYNase is more sensitive to deficiency of P5P than KAT, P5P deficiency diverts 3-HKYN metabolism from formation of 3-HAA to production of XA, and, consequently, to accumulation of KYN and KYNA, depending on the severity of PLP deficiency [9]. Experimental studies suggested diabetogenic effects of KP metabolites, such as XA-induced hyperglycemia [10]; increased urine excretion of XA in rat model of diabetes [11]; and impairment of biosynthesis [12] and biological activity of insulin by KYN, XA, KYNA, and their derivatives [13, 14]. Thus, chronic stress and chronic low-grade inflammation directly activate enzymes of the upstream steps of KP and divert downstream steps of KP (due to P5P deficiency) from biosynthesis of NAD toward formation of diabetogenic downstream metabolites. We proposed that resulting overproduction of diabetogenic KYN, 3H-KYN, 3-HAA, XA, and KYNA is one of the mechanisms of chronic stress- or chronic low-grade inflammation-induced development of T2D in pre-diabetes [15] (Fig. 2).

Dysregulation of tryptophan–kynurenine metabolic pathway in T2D
This hypothesis might be further supported by our finding of positive correlation of plasma levels of KYN with severity of insulin resistance (IR) and pancreatic beta-cell function evaluated by homeostatic model assessment (HOMA-IR and HOMA2-B, respectively) in hepatitis C (HCV) virus patients. The importance of this finding is stressed by the fourfold increased incidence of IR in HCV [16]. Increased urine excretion of XA was reported in three pre-diabetic [17] and 20 T2D patients [11]. However, we are not aware of studies of both up- and downstream diabetogenic KP metabolites in the same plasma samples of T2D patients. As an initial step in evaluation of “kynurenine hypothesis of insulin resistance and its progression to T2D” [15], we compared plasma concentrations of TRP, KYN, KYNA, XA, and 3-HAA in T2D patients and healthy, non-diabetic subjects (control group).
Methods
Subjects
Patients
Overnight fasting plasma samples were collected from 30 (18 female and 12 male) T2D patients: 24 Hispanics, four American Caucasians, and two African Americans. T2D was diagnosed according to criteria of American Diabetes Association. All patients were taking metformin, 500 mg (16 patients) or 1000 mg/day (14 patients).
Healthy Subjects (Controls)
There were 24 subjects (12 females and 12 males): 12 American Caucasians, six Hispanics, and six African Americans. Study was approved by Tufts Medical Center IRB.
Determination of Kynurenines
Plasma samples were stored at −50 °C until analysis. Plasma levels of TRP–KYN metabolites were analyzed by gas chromatography–mass spectrometry method by Brains On-Line LLC, CA, USA.
Statistical Analysis
Results are presented as mean ± standard deviation (TRP and KYN in μM/L and KYNA, XA, and 3-HAA in nM/L). Non-parametric tests were used as indicated below.
Results
T2D patients were older (53.8 ± 8.3 years) than control subjects (43.3 ± 10.9 years) (p = 0.01, Mann–Whitney test, two-tailed).
Glucose levels of T2D patients were 157.87 ± 22.4 mg/dL (range 118–182).
Upstream Metabolites of TRP–KYN Pathway
There were no differences between TRP levels in plasma samples of T2D patients and control subjects (Table 1).
KYN levels were higher in plasma samples from T2D patients than in control subjects (Table 1).
KYN/TRP ratio, a clinical marker of IDO/TDO activity [18], was higher in plasma samples of T2D (2.88) than in samples of control subjects (2.51), although the differences did not achieve statistical significance.
Downstream Metabolites of TRP–KYN Pathway
XA and KYNA levels were higher in plasma samples of T2D patients than in control subjects (Table 1).
3-HAA levels in plasma samples of T2D patients were lower than in control subjects although difference did not achieve statistical significance (Table 1).
There were no differences between 3-HKYN levels of T2D patients (16.97 ± 7.1) and control subjects (16.72 ± 8.6).
Tryptophan–Kynurenine Metabolites and Metformin
Considering that metformin was reported to elevate plasma levels of TRP [19] and inhibit TDO expression in breast cancer cells under constitutive and inducible conditions [20], we analyzed the potential effect of dose of metformin on studied markers in T2D patients.
Plasma levels of KYN in T2D patients (n = 16) treated with 500 mg of metformin were higher than in control subjects (2.64 ± 0.96 and 1.76 ± 0.48 μM/L, respectively, p < 0.005, Mann–Whitney, two-tailed test). Plasma KYN levels of T2D patients treated with 1000 mg of metformin (n = 14) had tendency to be slightly higher than controls (2.04 ± 0.23, p < 0.03).
Correlations Between TRP–KYN Metabolites
XA levels were strongly correlated with KYNA in plasma samples of both control subjects and T2D patients (Table 2).
Plasma levels of KYN were correlated with levels of TRP and KYNA in plasma samples of both control subjects and T2D patients (Table 2).
TRP plasma levels were correlated with XA in control subjects but show rather weaker correlation in T2D patients. Correlation between TRP and KYNA was found in control subjects but not in TD patients (Table 2).
There were no correlations between 3-HAA levels and other studied metabolites and between age and levels of all studied metabolites in plasma samples of T2D patients and control subjects (Spearman’s Rank, two-tailed test) (data not shown).
Glucose levels positively correlated with TRP, KYN, and KYNA (Table 2).
Discussion
Major findings of the present study are the increased plasma levels of KYN and downstream KP metabolites, KYNA and XA, in T2D patients. Increases of KYN/TRP ratio and decreases of 3-HAA plasma levels of T2D did not reach the level of statistical significance.
Previous studies assessed KP metabolites in urine [21] and skin [22] of T2D patients. Serum KYN metabolites were evaluated only in patients with diabetic retinopathy, a complication of both T2D and T1D [23]. None of these studies assessed P5P-dependent KYN metabolites, XA, KYNA, and 3-HAA.
The increase of KYN observed in the present study suggests activation of TDO or IDO. This suggestion might be further supported by tendency to increase KYN/TRP ratio, an index of TDO/IDO activity, in T2D patients. Since TDO and IDO could not be activated concurrently [24], increased plasma levels of KYN (and KYN/TRP ratio) might result from either TDO or IDO activation. Inflammatory factors (e.g., IFNG, LPS), but not stress hormones, concurrently with IDO stimulate rate-limiting enzyme of pteridine pathway with consequent formation of neopterin. Assessment of plasma levels of neopterin helps to differentiate between TDO- and IDO-induced elevations of KYN [25]. Without assessment of neopterin levels, it is impossible to attribute the observed differences in KYN/TRP ratio to activation of TDO or IDO. It is noteworthy that we found plasma neopterin levels positively correlated with HOMA-IR and negatively with P5P in 592 participants of the study of Adult Boston Community Dwellers of Puerto Rican Origin [26].
Considering that metformin might elevate plasma levels of TRP [19] and inhibit TDO expression [20], one might expect higher TRP and lower KYN levels in patients treated with 1000 mg than 500 mg of metformin. However, we, on contrary, observed higher KYN levels in T2D patients treated with lower (500 mg) dose of metformin. Therefore, present results do not support the notion that metformin increases plasma TRP and inhibits TDO [19, 20]. One might suggest that our data is dependent on better control of T2D with higher (1000 mg) than lower (500 mg) dose of metformin, i.e., that KYN plasma levels reflected the severity of pathogenic changes of the disease rather than effect of medication.
As to downstream KYN metabolites, increased urine excretion of XA was reported in diabetic patients [11] but was not assessed in plasma (or serum) samples. Elevation of serum KYNA, the other P5P-dependent metabolite, was reported in diabetic retinopathy but without assessment of XA [23]. The present study found increased levels of both XA and KYNA in plasma samples of T2D patients. It is noteworthy that correlation between TRP and XA was weaker in T2D patients than in controls while correlation between TRP and KYNA was not detected at all in T2D patients. Such a difference suggests dysregulation of physiological steps of XA and KYNA production. Formation of XA, KYNA, and 3-HAA depends on P5P-sensitive enzymes. While most experimental studies revealed association of P5P deficiency with decreased production of 3-HAA and increased formation of XA [9], data on effect of P5P deficiency on KYNA production is controversial: decreased [27] and unchanged [28] urinary KYNA excretion was reported in rats and mice fed by P5P-deficient diet [29]. It is noteworthy that, at least, 50 % drop of normal cellular P5P concentrations are required to initiate changes in KYN metabolites [9]. In humans, 28 days of a vitamin B6-deficient diet resulted in increased KYN, XA, and KYNA urine excretion after TRP load [30].
The present data of increased plasma levels of KYN and downstream KP metabolites, KYNA and XA, in the same plasma samples of T2D patients might provide further support for “kynurenine hypothesis of insulin resistance (IR) and its progression to T2D” (Fig. 2) [15].
The present findings are in agreement with observations of increased plasma KYN, XA, and KYNA levels and KYN/TRP ratio and decreased levels of P5P in patients with diabetes in comparison with patients with normal glucose metabolism among subjects with stable angina pectoris [31] that were reported after presentation of our data at ICNA (September, 2014) and submission of this manuscript (November, 2014).
Therefore, dysregulation of KP was observed to associate with IR in HCV patients [17], in diabetic patients with stable angina pectoris [31], and in T2D patients (present report).
Chronic stress- or chronic low-grade inflammation-induced upregulation of upstream steps of KP combined with P5P deficiency, resulting in shifting of downstream KYN metabolism from formation of NAD toward production of diabetogenic KYN derivatives, might contribute to increased association of IR (and T2D) with aging, neurodegenerative diseases (e.g., Parkinson’s, Alzheimer’s, and Huntington’s), and schizophrenia and treatment by antipsychotic medications, viral infections (e.g., HIV and HCV), and depression [32, 33].
Further evaluations of “kynurenine hypothesis of insulin resistance and its progression to T2D” have to consider the limitations of the current study: across-the-board rather than prospective design; relatively small number of samples; not age-, gender-, and race-matched controls; and treatment with metformin. If confirmed, metabolites of KP might be the next new biomarkers of IR and T2D and new targets for prevention and treatment of IR and T2D [34].
Abbreviations
- T2D:
-
Type 2 diabetes
- IR:
-
Insulin resistance
- TRP:
-
Tryptophan
- NAD:
-
Nicotinamide adenine dinucleotide
- IFNG:
-
Interferon gamma
- LPS:
-
Lipopolysaccharide
- KP:
-
Kynurenine pathway of TRP metabolism
- KYN:
-
Kynurenine
- KYNA:
-
Kynurenic acid
- 3-HKYN:
-
3-hydroxykynurenine
- 3-HKYNA:
-
3-hydroxykynurenic acid
- XA:
-
Xanthurenic acid
- 3-HAA:
-
3-hydroxyanthranilic acid
- KMO:
-
Kynurenine 3-monooxygenase
- P5P:
-
Pyridoxal 5′-phosphate
- KAT:
-
Kynurenine aminotransferase
- KYNase:
-
Kynureninase
- IDO:
-
Indoleamine-2,3-dioxygenase
- TDO:
-
Tryptophan-2,3-dioxygenase
- HIV:
-
Human immunodeficiency virus
- HCV:
-
Hepatitis C virus
- HOMA:
-
Homeostatic model assessment
References
Hackett RA, Steptoe A, Kumari M (2014) Association of diurnal patterns in salivary cortisol with type 2 diabetes in the Whitehall II study. J Clin Endocrinol Metab 99:4625–4631. doi:10.1210/jc.2014-2459
Olefsky JM, Glass CK (2010) Macrophages, inflammation, and insulin resistance. Annu Rev Physiol 72:219–246
Connick JH, Stone TW (1985) The role of kynurenines in diabetes mellitus. Med Hypotheses 18:371–376
Schwarcz R, Bruno JP, Muchowski PJ, Wu HQ (2012) Kynurenines in the mammalian brain: when physiology meets pathology. Nat Rev Neurosci 13:465–477
Alberati-Giani D, Ricciardi-Castagnoli P, Kohler C, Cesura AM (1996) Regulation of the kynurenine metabolic pathway by interferon-gamma in murine cloned macrophages and microglial cells. J Neurochem 66:996–1004
Musajo L (1935) L’acido xanthurenico. Rend Accad Nazl Lincci 21:368–371
Mahuren JD, Dubeski PL, Cook NJ, Schaefer AL, Coburn SP (1999) Adrenocorticotropic hormone increases hydrolysis of B-6 vitamers in swine adrenal glands. J Nutr 129:1905–1908
Paul L, Ueland PM, Selhub J (2013) Mechanistic perspective on the relationship between pyridoxal 5′-phosphate and inflammation. Nutr Rev 71:239–244
Rios-Avila L, Nijhout HF, Reed MC, Sitren HS, Gregory JF 3rd (2013) A mathematical model of tryptophan metabolism via the kynurenine pathway provides insights into the effects of vitamin B-6 deficiency, tryptophan loading, and induction of tryptophan 2,3-dioxygenase on tryptophan metabolites. J Nutr 143:1509–1519. doi:10.3945/jn.113.174599
Kotake Y (1955) Xanthurenic acid, an abnormal metabolite of tryptophan and the diabetic symptoms caused in albino rats by its production. J Vitaminol (Kyoto) 1:73–87
Ikeda S, Kotake Y (1984) Urinary excretion of xanthurenic acid and zinc in diabetes: 1) separation of xanthurenic acid-Zn2+ complex by ion-exchange chromatography. Acta Vitaminol Enzymol 6:23–28
Okamoto H (1981) Regulation of proinsulin synthesis in pancreatic islets and a new aspect to insulin-dependent diabetes. Mol Cell Biochem 37:43–61
Murakami E, Kotake Y (1972) Studies on the xanthurenic acid-insulin complex. 3. Distribution of xanthurenic acid and formation of xanthurenic acid-insulin complex in serum. J Biochem 72:251–259
Meyramov G, Korchin V, Kocheryzkina N (1998) Diabetogenic activity of xanturenic acid determined by its chelating properties? Transplant Proc 30:2682–2684
Oxenkrug G (2013) Insulin resistance and dysregulation of tryptophan-kynurenine and kynurenine-nicotinamide adenine dinucleotide metabolic pathways. Mol Neurobiol 48:294–301. doi:10.1007/s12035-013-8497-4
Oxenkrug GF, Turski WA, Zgrajka W, Weinstock JV, Summergrad P (2013) Tryptophan-kynurenine metabolism and insulin resistance in hepatitis C patients. Hepat Res Treat 2013: 149247
Manusadzhian VG, Kniazev IA, Vakhrusheva LL (1974) Mass spectrometric identification of xanthurenic acid in pre-diabetes. Vopr Med Khim 20:95–97
Midttun O, Ulvik A, Pedersen E, Ebbing M, Bleie O et al (2011) Low plasma vitamin B-6 status affects metabolism through the kynurenine pathway in cardiovascular patients with systemic inflammation. J Nutr 141:611–617
Marchetti P, Masiello P, Benzi L, Cecchetti P, Fierabracci V, Giannarelli R, Gregorio F, Brunetti P et al (1989) Effects of metformin therapy on plasma amino acid pattern in patients with maturity-onset diabetes. Drugs Exp Clin Res 15:565–570
Do MT, Kim HG, Tran TT, Khanal T, Choi JH, Chung YC, Jeong TC, Jeong HG (2014) Metformin suppresses CYP1A1 and CYP1B1 expression in breast cancer cells by down-regulating aryl hydrocarbon receptor expression. Toxicol Appl Pharmacol 280:138–148. doi:10.1016/j.taap.2014.07.021
Khattab M, Abul-Fadl M, Khalafallah A, Hamza S (1972) Studies on the urinary excretion of certain tryptophan metabolites in diabetics. J Egypt Med Assoc 55:531–541
Calandra P (1977) Identification of tryptophan metabolites in the healthy epidermis of diabetics. Acta Diabetol Lat 14:1426-37
Munipally PK, Agraharm SG, Valavala VK, Gundae S, Turlapati NR (2011) Evaluation of indoleamine 2,3-dioxygenase expression and kynurenine pathway metabolites levels in serum samples of diabetic retinopathy patients. Arch Physiol Biochem 117:254–258. doi:10.3109/13813455.2011.623705
Hayaishi O (1976) Properties and function of indoleamine 2,3-dioxygenase. J Biochem 79:13–21
Sucher R, Schroecksnadel K, Weiss G, Margreiter R, Fuchs D, Brandacher G (2010) Neopterin, a prognostic marker in human malignancies. Cancer Lett 287:13–22
Oxenkrug G, Tucker KL, Requintina P, Summergrad P (2011) Neopterin, a marker of interferon-gamma-inducible inflammation, correlates with pyridoxal-5′-phosphate, waist circumference, HDL-cholesterol, insulin resistance and mortality risk in adult Boston community dwellers of Puerto Rican origin. Am J Neuroprot Neuroregen 3:48–52
Shibata K, Mushiage M, Kondo T, Hayakawa T, Tsuge H (1955) Effects of vitamin B6 deficiency on the conversion ratio of tryptophan to niacin. Biosci Biotechnol Biochem 59:2060–2063
Yeh JK, Brown RR (1977) Effects of vitamin B-6 deficiency and tryptophan loading on urinary excretion of tryptophan metabolites in mammals. J Nutr 107:261–271
Bender DA, Njagi EN, Danielian PS (1990) Tryptophan metabolism in vitamin B6-deficient mice. Br J Nutr 63:27–36
Midttun O, Ulvik A, Ringdal Pedersen E, Ebbing M, Bleie O, Schartum-Hansen H, Nilsen RM, Nygard O et al (2011) Low plasma vitamin B-6 status affects metabolism through the kynurenine pathway in cardiovascular patients with systemic inflammation. J Nutr 141:611–617
Pedersen ER, Tuseth N, Eussen SJ, Ueland PM, Strand E, Svingen GF, Midttun Ø, Meyer K et al (2015) Associations of plasma kynurenines with risk of acute myocardial infarction in patients with stable angina pectoris. Arterioscler Thromb Vasc Biol 35:455–462. doi:10.1161/ATVBAHA.114.304674
Oxenkrug G, Ratner R, Summergrad P (2013) Kynurenines and vitamin B6: link between diabetes and depression. J Bioinformatics Diabetes 1:1–9. doi:10.14302/issn.2374-9431.jbd-13-212
Oxenkrug G (2015) 3-Hydroxykynurenic acid and type 2 diabetes: implications for aging, obesity, depression, Parkinson’s disease and schizophrenia. In: Engin A, Engin AB (eds) Tryptophan metabolism: implications for biological processes, health and diseases, molecular and integrative toxicology. Springer International Publishing, Switzerland, pp 173–195. doi:10.1007/978-3-319-15630-9_8
Polyzos KA, Ketelhuth DF (2015) The role of the kynurenine pathway of tryptophan metabolism in cardiovascular disease. An emerging field. Hamostaseologie 35:128–136. doi:10.5482/HAMO-14-10-00562
Acknowledgments
This study is supported by NIMH104810. The author highly appreciates BioreclamationIVT, NY, USA, for providing plasma samples and Marieke van der Hart, PhD, for the excellent help with biochemical analyses
Conflict of Interest
The author declares that he has no competing interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Oxenkrug, G.F. Increased Plasma Levels of Xanthurenic and Kynurenic Acids in Type 2 Diabetes. Mol Neurobiol 52, 805–810 (2015). https://doi.org/10.1007/s12035-015-9232-0
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12035-015-9232-0