
Abstract
Purpose
Prior work has shown that higher circulating concentrations of fibroblast growth factor-21 (FGF-21) are associated with an increased likelihood of developing colorectal cancer. We conducted a prospective study to assess the relationship between circulating FGF-21 and odds of developing early neoplastic lesions in the colorectum.
Methods
A total of 94 study participants were included from the ursodeoxycholic acid (UDCA) trial, a phase III, randomized, double-blind, placebo-controlled clinical trial of the effect of 8–10 mg/kg of body weight UDCA vs. placebo. Logistic regression analyses were conducted to evaluate the association between baseline FGF-21 concentrations and odds of developing a metachronous adenoma.
Results
Of the characteristics compared across tertiles of FGF-21 concentrations, including age, race, sex, BMI, and other variables, only a previous personal history of colorectal polyps prior to entry into the UDCA trial was statistically significantly related to FGF-21 levels, with a proportion of 26.7%, 56.7%, and 50.0% across the first, second, and third tertiles, respectively (p < 0.05). Higher circulating concentrations of FGF-21 were statistically significantly associated with greater odds of developing a metachronous colorectal adenoma. After adjusting for potential confounders and when compared with the lowest tertile of FGF-21, the adjusted ORs (95% CIs) for metachronous colorectal adenoma in the second and third tertiles were 4.72 (95% CI, 1.42–15.72) and 3.82 (95% CI, 1.15–12.68), respectively (p trend < 0.05).
Conclusion
Our results reveal for the first time that, in addition to a recently discovered association with colorectal cancer, circulating FGF-21 concentrations are significantly and directly associated with odds of developing metachronous colorectal adenoma.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In the USA, colorectal cancer (CRC) is the third most common cancer diagnosed in men and women combined [1, 2]. In 2020, 147,950 new cases of CRC are expected to occur [1]. Although incidence and mortality rates have been declining over the past two decades [2], CRC remains the second most common cause of cancer deaths, with 51,020 estimated to have occurred in 2019 [1]. The overall death rate has continued to decline [1], but in those younger than 50 years old, the CRC death rate has increased by 13% [2].
One of the hallmarks of cancer is chronic inflammation [3], with CRC being one of the cancers in which tumors are associated with chronic inflammation; this inflammation is present from the tumor’s earliest stages [4]. Previous work has also shown that long-term treatment with non-steroidal anti-inflammatory (NSAID) drugs has been effective at lowering both CRC incidence and mortality [4]. Another hallmark of cancer is metabolic alteration, which, along with metabolic reprogramming, could be implicated in colorectal tumorigenesis [3, 5, 6]. Thus, identifying the inflammatory and metabolic markers that are associated with developing CRC could be beneficial in identifying at-risk individuals and targeting their specific treatment.
Prior work has identified one such biomarker, fibroblast growth factor-21 (FGF-21) [6]. In their work, Qian et al. found that higher circulating concentrations of FGF-21 are associated with an increased likelihood of developing colorectal cancer [6]. FGF-21 is secreted by the liver and is part of the FGF subfamily [7]. FGF-21, considered an endocrine FGF, acts as a circulating hormone to regulate simple sugar intake, and is also associated with inflammation, and whole-body and immune homeostasis [6, 7]. As CRC is affected by inflammatory pathways, FGF-21 could also play a role in colorectal carcinogenesis [6].
There have been few epidemiological studies investigating the association between FGF-21 and cancer. Previous studies looked at the role of FGF-21 as a diagnostic biomarker in renal and breast cancers [8, 9], while others identified FGF-21 out of a series of biomarkers as being associated with increased risk of developing CRC [6, 10]. The purpose of the current study is to build upon the findings of these previous reports by using a prospective study design in order to assess the relationship between circulating FGF-21 and odds of developing early neoplastic lesions in the colorectum.
Methods
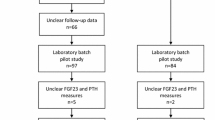
The study subjects included in this analysis were participants in the ursodeoxycholic acid (UDCA) trial at the University of Arizona Cancer Center [11]. Initially, this phase III, randomized, double-blind, placebo-controlled clinical trial was conducted to determine the effect of UDCA on metachronous colorectal neoplasia [11]. In order to be eligible for the trial, participants had to have an adenomatous polyp, detected via colonoscopy, resected 6 months prior to randomization into the trial, while the endpoint colonoscopy occurred at least 6 months after randomization [11]. The median time on the treatment was 31.8 months, while the median time on the placebo was 32.0 months [11]. The primary results of the trial showed that among the 1192 participants who completed the trial, there was no significant difference in the development of adenomas between the intervention and placebo groups [11]. Of the 1192 participants, 94 participants with data for baseline and follow-up colorectal adenomas were selected for the analysis of plasma FGF-21 concentrations. Of these 94 participants, 45 received UDCA, while 49 were on placebo. Their blood samples were collected at baseline and stored at − 80 °C. The trial was approved by the University of Arizona Human Subjects Committee and Institutional Review Board.
Endpoint Definition
Adenoma recurrence was defined as any colonoscopy-detected adenoma or cancer at least 6 months after randomization to the UDCA trial. However, it is possible that some of the “recurrent” lesions may have been missed at the baseline colonoscopy and, as such, the lesions were referred to as “metachronous” instead of “recurrent” in the present study. Endoscopy and pathology reports, with central pathology review, were done at each study site. Data for adenoma size, histology, number, and location were also extracted.
Analysis of FGF-21
Enzyme-linked immunosorbent assay (ELISA) was used to measure plasma FGF-21 concentrations. The C-terminal ELISA was performed according to the manufacturer’s instructions (BioVendor International, Asheville, NC). Briefly, participant samples were incubated for 60 min in wells pre-coated with polyclonal anti-human FGF-21 antibody. Samples were then washed and incubated with a biotin-labeled polyclonal anti-human FGF-21 antibody. Streptavidin-HRP conjugate was then added and incubated for 30 min following another wash. After a reaction with 3,3′,5,5′-tetramethylbenzidine (TMB) substrate solution, weak acid was added to stop the reaction, and the resultant yellow color was measured using spectrophotometry at a wavelength of 450 nm. Standard curves were then constructed by plotting absorbance values against concentrations of reference materials and then applied to the experimental samples to determine FGF-21 concentrations.
Statistical Analyses
Chi-square tests were used to assess differences in categorical baseline characteristics across FGF-21 tertiles and colorectal adenoma recurrence, while ANOVA was employed for continuous variables. Fisher’s exact test was used for categorical variables with cell sizes < 5. To determine an association between FGF-21 tertiles and odds of colorectal adenoma recurrence, logistic regression modeling was employed. Variables that were assessed for potential confounding were age, sex, race, aspirin use, BMI category, history of polyps, history of smoking, and family history of CRC; those which changed the point estimate by more than 10% were defined as confounders. Thus, the final adjusted model included BMI category, history of polyps, and family history of CRC as well as age and sex. Though age and sex did not change the point estimate by more than 10%, they were included due to being risk factors of CRC as established in the literature (12). All analyses were conducted using SAS 9.4 (SAS Institute Incorporated, Cary, NC).
Results
Table 1 illustrates the baseline characteristics of study participants across tertiles of FGF-21. Those with FGF-21 concentrations in the second and third tertiles were statistically significantly more likely to have a history of polyps prior to entering the parent trial (56.7% and 50%, respectively, compared with those in the lowest tertile of FGF-21 (26.7%, P = 0.05)). No other differences were observed by tertile of FGF-21 for age, sex, race, marital status, education, smoking, aspirin use, BMI, or family history of colorectal cancer.
Table 2 presents the same baseline participant characteristics by the presence or absence of a metachronous adenoma; no statistically significant differences were observed. Those who had a metachronous adenoma were more likely to be male (64.6%) than female (35.4%) and tended to be aspirin users (37.5% vs. 23.9% in those with no metachronous adenoma). Furthermore, these participants tended to be overweight (50.0%) and have a history of polyps (53.3%) compared with those with no metachronous adenoma (43.5% and 34.8%, respectively). These participants with metachronous adenoma were also less likely to have a family history of colon cancer as 22.9% reported such history versus 41.3% in those with no metachronous adenoma.
In Table 3, the odds ratios (ORs) with 95% confidence intervals (CIs) of metachronous adenoma by tertile of FGF-21 levels (pg/mL) are shown. When compared with the lowest tertile of FGF-21, the adjusted ORs for the second and third tertile were 4.72 (95% CI, 1.42–15.72) and 3.82 (95% CI, 1.15–12.68), respectively (P < 0.05).
Discussion
Colorectal cancer remains a fairly common cancer among the US population as it is the third most diagnosed cancer in both men and women [1, 2]. Even so, incidence and mortality have decreased because of various factors such as increased aspirin use, utilization of screening tests, and improved treatments [2]. However, there are still underlying causes of CRC that are yet to be understood. Colorectal cancer is one of the better-known examples of a tumor being associated with chronic inflammation [4], which has been established as a hallmark of cancer [3]. CRC can arise sporadically, or be associated with somatic or hereditary genetic mutations, or develop due to chronic inflammation in the intestine, such as in those with irritable bowel disease (IBD) [4, 12]. However, NSAIDs were shown to delay or even prevent CRC cases caused by hereditary mutations [13, 14]. Since such mutations do not have a precedent of chronic inflammation, this could be indicative of inflammatory processes occurring at the tumor onset [4]. FGF-21 may contribute to this aspect of colorectal carcinogenesis. FGF-21, mostly released from the liver, acts as a circulating hormone [15] and is able to normalize glucose, lipid, and energy homeostasis [7], factors which in turn could affect colorectal carcinogenesis [6]. Previous work has also found FGF-21 to be associated with metabolic and immune systems [6, 16], as well as having involvement in inflammation [6, 7]. Thus, due to the relationship of both CRC and FGF-21 with inflammation and metabolism [6], FGF-21 could also affect CRC risk. In the current work, the potential of FGF-21 to contribute to the development of early colorectal adenoma was examined.
Prior reports [6, 10] have established an association between higher concentrations of FGF-21 and increased risk of early and late stages of CRC. These conclusions were reflected in the current study, where, in a predominantly older, male, and white population, preliminary results indicated that higher concentrations of FGF-21 may increase the risk of metachronous colorectal adenomas. Previously, Hanks et al. [17] found that in a healthy population, circulating FGF-21 levels increased with age. The risk of developing CRC also increases with advancing age [18]. The results of the current study with regard to age, though not statistically significant, are reflective of this trend as those with higher levels of FGF-21 were older than those with the lowest levels of FGF-21. Furthermore, those who had a metachronous adenoma were, on average, older than those with no metachronous adenomas. Thus, it is possible that the older age led to increased FGF-21 levels which in turn increased the risk of developing CRC. Lastly, though the incidence of CRC is equal in men and women [18], the current study found a higher proportion of men having metachronous adenoma overall, and men were more likely than to be categorized into the two higher tertiles of FGF-21 than women. Perhaps the higher levels of FGF-21 could have accelerated the occurrence of CRC in men, an avenue worth exploring in future longitudinal studies. Of note, however, is that adjustment for both age and sex increased the odds of metachronous colorectal adenoma, suggesting a confounding, and not an independent, effect of these factors on the disease.
Another interesting find, though not statistically significant, was the relationship between the use of aspirin, an NSAID, and reduced odds of metachronous adenoma. As mentioned previously, NSAIDs, which reduce inflammation, were found to decrease the risk of CRC [19]. A meta-analysis of four randomized clinical trials found that taking aspirin of at least 75 mg daily for several years reduced the incidence of CRC by 30–40% [20]. In the current study, aspirin use was more common among those who had a metachronous adenoma (37.5%) compared with those who did not (23.9%). Though these results are contrary to the literature, it is possible that the study participants were taking other NSAIDs. This would warrant a further, more in-depth analysis with a larger sample size and more information on NSAID use.
One significant finding from the current study was related to having a personal history of polyps, another risk factor for CRC [18]; those with higher concentrations of FGF-21 were more likely to have a history of polyps. Previous studies found elevated FGF-21 serum levels starting in the early stages of breast cancer [9] and in response to liver carcinogenesis [21]. The latter study also suggested hepatic FGF-21 to be a stress responder that is produced as a response to injury and regeneration [8, 21]. Thus, in those with a history of polyps, due to the stress and injury caused on the body by those polyps, it is possible this to have caused the FGF-21 levels to elevate.
Just as with the report of Qian et al. [6], the current work found an increased risk of metachronous adenoma with increased concentrations of FGF-21. The highest risk was exhibited in the second tertile, a trend paralleled in the Qian et al. study [6]. However, the current findings showed slightly higher odds in the second tertile; the models were adjusted for both similar and different factors. The results exhibited here are similar to those of other studies that have investigated the relationship between FGF-21 and cancer. In renal cancer, it was found that higher FGF-21 serum level is a prognostic biomarker [8]. It is hypothesized that due to FGF-21’s insulin-enhancing properties [22], the tumor could induce such FGF-21-produced insulin, which in turn would be absorbed by the growing tumor [8]. Additionally, in breast cancer, FGF-21 levels were reduced following therapy [23]. Though the results are promising, they are worth investigating more as it is hard to discern if the high levels of FGF-21 led to the colorectal metachronous adenoma, or they increased as a result of the carcinogenesis or the stress caused on the body by the disease. Furthermore, serum FGF-21 levels could also be induced by other factors such as fasting, obesity, liver injury, cirrhosis, and type 2 diabetes [7, 8, 21, 24, 25]. The present study controlled for some of these conditions, but not all were assessed. Thus, these other factors, as well as the underlying mechanism of FGF-21 on CRC, also need to be parsed out in future studies.
The strengths of the present study included its prospective design and utilization of a clinical trial study population with measured FGF-21 levels and thoroughly detailed clinical information. The study also had limitations. Although the original study included a large phase III clinical trial study population, for this study, the sample size of those with baseline and follow-up colorectal adenomas was relatively small. Thus, the results may not be generalizable to the general US population, and more detailed analyses could not be conducted. These participants were also not randomly selected from the original clinical trial population, which may have affected the randomization attained by the original trial. However, imbalances were not seen in the baseline characteristics. In addition, the concentrations of FGF-21 were measured cross-sectionally, and true adenoma recurrence could not be measured as there was a possibility that some baseline adenomas were missed by the colonoscopy. Lastly, though confounding was controlled for in the statistical models, residual confounding may still be present.
The current study aimed to contribute to the small but growing field surrounding and examining the relationship between circulating FGF-21 and odds of developing early neoplastic lesions in the colorectum. Overall, higher concentrations of FGF-21 were associated with increased odds of metachronous adenoma development. In the future, identifying such inflammatory and metabolic markers which may lead to CRC could be beneficial in detecting at-risk individuals and targeting their specific treatment. If FGF-21, in particular, was found to be a reliable biomarker in detecting early CRC, then it could be used to improve targeted CRC surveillance. However, more in-depth studies with larger sample sizes focusing specifically on FGF-21 will be needed to establish a clearer connection.
Data Availability
The data may be requested from the principal investigator and may be subject to IRB approval.
References
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70:7–30.
Siegel RL, Miller KD, Fedewa SA, Ahnen DJ, Meester RG, Barzi A, et al. Colorectal cancer statistics, 2017. CA Cancer J Clin. 2017;67(3):177–93.
Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144(5):646–74.
Lasry A, Zinger A, Ben-Neriah Y. Inflammatory networks underlying colorectal cancer. Nat Immunol. 2016;17(3):230–40.
Dela Cruz MD, Ledbetter S, Chowdhury S, Tiwari AK, Momi N, Wali RK, et al. Metabolic reprogramming of the premalignant colonic mucosa is an early event in carcinogenesis. Oncotarget. 2017;8(13):20543–57.
Qian J, Tikk K, Weigl K, Balavarca Y, Brenner H. Fibroblast growth factor 21 as a circulating biomarker at various stages of colorectal carcinogenesis. Br J Cancer. 2018;119(11):1374–82.
Degirolamo C, Sabba C, Moschetta A. Therapeutic potential of the endocrine fibroblast growth factors FGF19, FGF21 and FGF23. Nat Rev Drug Discov. 2016;15:51–69.
Knott ME, Minatta JN, Roulet L, Gueglio G, Pasik L, Ranuncolo SM, et al. Circulating fibroblast growth factor 21 (Fgf21) as diagnostic and prognostic biomarker in renal cancer. J Mol Biomarker Diag. 2016;1(Suppl 2):015. https://doi.org/10.4172/2155-9929.S2-015.
Knott ME, Ranuncolo SM, Nuñez M, Armanasco E, Puricelli LI, De Lorenzo MS. Levels of fibroblast growth factor 21 (FGF21) in serum as diagnostic biomarker in patients with breast cancer. Proceedings: AACR 106th Annual Meeting 2015; April 18-22, 2015; Philadelphia, PA. Cancer Res. 2015;75(15 Suppl):Abstract no.1577. https://doi.org/10.1158/1538-7445.AM2015-1577.
Harlid S, Myte R, Van Guelpen B (2017). The metabolic syndrome, inflammation, and colorectal cancer risk: an evaluation of large panels of plasma protein markers using repeated, prediagnostic samples. Med Inflamm. https://doi.org/10.1155/2017/4803156. Epub 2017 Mar 22.
Alberts DS, Martinez ME, Hess LM, Einspahr JG, Green SB, Bhattacharyya AK, et al. Phase III trial of ursodeoxycholic acid to prevent colorectal adenoma recurrence. J Natl Cancer Inst. 2005;97(11):846–53.
Jess T, Frisch M, Simonsen J. Trends in overall and cause-specific mortality among patients with inflammatory bowel disease from 1982 to 2010. Clin Gastroenterol Hepatol. 2013;11(1):43–8.
Burn J, Gerdes A-M, Macrae F, Mecklin J-P, Moeslein G, Olschwang S, et al. Long-term effect of aspirin on cancer risk in carriers of hereditary colorectal cancer: an analysis from the CAPP2 randomised controlled trial. Lancet. 2011;378(9809):2081–7.
Labayle D, Fischer D, Vielh P, Drouhin F, Pariente A, Bories C, et al. Sulindac causes regression of rectal polyps in familial adenomatous polyposis. Gastroenterol. 1991;101(3):635–9.
Itoh N. Hormone-like (endocrine) Fgfs: their evolutionary history and roles in development, metabolism, and disease. Cell Tissue Res. 2010;342(1):1–11.
Youm Y-H, Horvath TL, Mangelsdorf DJ, Kliewer SA, Dixit VD. Prolongevity hormone FGF21 protects against immune senescence by delaying age-related thymic involution. PNAS. 2016;113(4):1026–31.
Hanks LJ, Gutiérrez OM, Bamman MM, Ashraf A, McCormick KL, Casazza K. Circulating levels of fibroblast growth factor-21 increase with age independently of body composition indices among healthy individuals. J Clin Transl. 2015;2(2):77–82.
Amersi F, Agustin M, Ko CY. Colorectal cancer: epidemiology, risk factors, and health services. Clin Colon Rectal Surg. 2005;18(3):133–40. https://doi.org/10.1055/s-2005-916274.
Hamoya T, Fujii G, Miyamoto S, Takahashi M, Totsuka Y, Wakabayashi K, et al. Effects of NSAIDs on the risk factors of colorectal cancer: a mini review. Genes Environ. 2016;38:6. https://doi.org/10.1186/s41021-016-0033-0.
Rothwell PM, Wilson M, Elwin C-E, Norrving B, Algra A, Warlow CP, et al. Long-term effect of aspirin on colorectal cancer incidence and mortality: 20-year follow-up of five randomised trials. Lancet. 2010;76(9754):1741–50.
Yang C, Lu W, Lin T, You P, Ye M, Huang Y, et al. Activation of liver FGF21 in hepatocarcinogenesis and during hepatic stress. BMC Gastroenterol. 2013;13(1):67.
Markan KR, Naber MC, Ameka MK, Anderegg MD, Mangelsdorf DJ, Kliewer SA, et al. Circulating FGF21 is liver derived and enhances glucose uptake during refeeding and overfeeding. Diabetes. 2014;63(12):4057–63.
Akyol M, Alacacioglu A, Demir L, Kucukzeybek Y, Yildiz Y, Gumus Z, et al. The alterations of serum FGF-21 levels, metabolic and body composition in early breast cancer patients receiving adjuvant endocrine therapy. Cancer Biomark. 2017;18(4):441–9.
Chavez AO, Molina-Carrion M, Abdul-Ghani MA, Folli F, DeFronzo RA, Tripathy D. Circulating fibroblast growth factor-21 is elevated in impaired glucose tolerance and type 2 diabetes and correlates with muscle and hepatic insulin resistance. Diabetes Care. 2009;32(8):1542–6.
Mraz M, Bartlova M, Lacinova Z, Michalsky D, Kasalicky M, Haluzikova D, et al. Serum concentrations and tissue expression of a novel endocrine regulator fibroblast growth factor-21 in patients with type 2 diabetes and obesity. Clin Endocrinol. 2009;71(3):369–75.
Funding
This study was funded by the National Cancer Institute Cancer Center Support (Grant P30CA023074; NIH/NCI RO1CA140285; NIH/NCI; NIH/NCI P01CA041108).
Author information
Authors and Affiliations
Contributions
Dr. Ana Florea, Dr. Elizabeth Jacobs, and Dr. Peter W. Jurutka were responsible for the design, acquisition of data, and interpretation of data. Dr. Ana Florea and Dr. Elizabeth Jacobs were responsible for data analyses. Dr. Lindsay Kohler, Dr. Robin Harris, and Dr. Yann Klimentidis made substantial contributions to manuscript preparation and interpretation of data. All authors assisted with the drafting and critical revisions of the article by making important intellectual contributions, approved the work to be published, and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethics Approval
This study has been approved by the University of Arizona Institutional Review Board.
Consent to Participate
All participants provided written and signed informed consent forms.
Consent to Publish
All participants provided written and signed informed consent forms.
Code Availability
No special or custom code was used.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Florea, A., Harris, R.B., Klimentidis, Y.C. et al. Circulating Fibroblast Growth Factor-21 and Risk of Metachronous Colorectal Adenoma. J Gastrointest Canc 52, 940–946 (2021). https://doi.org/10.1007/s12029-020-00515-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12029-020-00515-8