
Abstract
Hepatocellular carcinoma is one of the most common cancers and an important health problem all over the world. Its prognosis is poor. For better patient care, early diagnosis is essential. Although new imaging techniques have a big impact on hepatocellular carcinoma diagnosis, histopathological examination is still the gold standard for precise diagnosis. Histopathological evaluation gives exact diagnosis in the meaning of tumor size, histological subtypes, grading, and differential diagnosis from metastasis and other tumors. Immunohistochemistry as a part of diagnostic histopathological technique plays an important role in routine practice. Immunohistochemistry is useful for confirming of hepatocytic origin, supporting hepatocellular malignancy, and differential diagnosis. It also gives prognostic information. There are growing attempts to classify tumors by their molecular genetic signatures. This is also actual for hepatocellular carcinoma. This mini review focuses on the histopathology of hepatocellular carcinoma including subtypes; differential diagnosis and immunohistochemistry as an ancillary diagnostic tool, updated or added entities, i.e., combined hepatocellular-cholangiocarcinoma; small hepatocellular carcinoma; correlation with molecular studies; and future perspectives.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hepatocellular carcinoma (HCC) is the most common type of primary liver carcinomas. It is one of the most common cancers all over the world that is also one of the leading cause of cancer death [1,2,3]. Its prognosis is poor with current therapeutic approaches. HCC most frequently develops in the cirrhotic background. It can also occur in non-cirrhotic liver [4]. It has well-known risk factors such as HBV and HCV hepatitis, alcoholic and non-alcoholic fatty liver disease (AFLD and NAFLD), genetic metabolic diseases and toxins (e.g., aflatoxin). The mail gender is also a risk factor [4, 5]. Although vaccination and improved antiviral therapies resulted in some achievements for common viral etiologies, viral hepatitis is the major cause of cirrhosis especially in East Asia [3, 6]. For western countries, AFLD and NAFLD are becoming more important etiologies for HCC [6, 7]. Although previously it was considered that HCC’s risk was limited to patients with liver cirrhosis, nowadays, a significant fraction of fatty liver disease associated HCC is found in non-cirrhotic liver or liver showing mild fibrosis [3, 8, 9].
HCC differs from many cancers by its diagnostic algorithm. In general, malignancy diagnosis depends on biopsy findings. But in current practice, HCC is diagnosed mainly by imaging findings, even treated with locoregional therapies without a biopsy confirmation [10]. Indeed, since the 2000s, biopsy is no longer required in most cases for the diagnosis of HCC developed on cirrhosis, according to the current guidelines [4, 11]. Liver biopsies for HCC are becoming rare, being performed only for lesions that are atypical on imaging [4]. Typical imaging findings on CT/MRI of HCC are hypervascularity in arterial phase and washout in portal venous phase [12, 13]. But imaging diagnosis has some disadvantages. If not associated with larger dominant tumors, HCC with cirrhotomimetic pattern is well below the threshold for imaging detection and is an exclusive histological diagnosis at present [9]. A small proportion of HCC may be hypovascular especially early HCCs, and a small proportion of nodules with radiological features suggestive of HCC may not be hepatocellular. It is not a safe tool for diagnosis of small lesions which are 1–2 cm in diameter. Histopathological HCC subtyping is nearly impossible with imaging. Mixed tumors, especially combined hepatocellular carcinoma-cholangiocarcinoma (cHCC-CC), can give inconclusive imaging findings. HCC subtypes with sclerotic stroma can imitate cholangiocarcinoma (CC). Further, most of the imaging algorithms depend on cirrhotic background findings. HCCs in the non-cirrhotic background need to be differentiated from metastasis. The specificity of CT and MRI ranges between 85 and 100%. Sensitivity depends on the lesion size, and it decreases in tumors less than 2 cm in diameter. Also, false positives, as high as 33%, have been reported with the radiology techniques for diagnosing HCC. Biopsy has advantage over imaging as comparison with non-lesional liver tissue provides vital information. Biopsy tissue and archived blocks are important source for teaching, getting expertise for pathologist and knowledge sharing [2, 14]. In many other tumors in which they are mostly diagnosed by histopathological examination such as colorectal adenocarcinoma and non-small cell lung cancer or melanoma, there is a big success in diagnosis and treatment options. Indeed, in a study by Pote et al., the authors had to create “virtual biopsy” material obtained from the whole tissue section of hepatic resection materials to overcome the small number of available biopsy specimens [11].
Although new imaging techniques have a big impact on hepatocellular carcinoma diagnosis, histopathological examination is still the gold standard for precise diagnosis. In another way, archived biopsy material is needed for further studies in the new “omics” era. Thus, liver biopsy and histopathologic examinations have gained more interest nowadays.
Pathology of HCC
Histopathological examination starts with macroscopic evaluation. This is especially important for resection specimens. I suggest checking preoperative imaging findings before sectioning; thus, a correlation between macroscopic and imaging results can be rendered. Next to standard gross evaluation parameters such as weight, measures, color changes, consistency, tumor size, encapsulation, existence of multifocality or satellites, surgical margins if it is a partial resection; there are some important details for hepatectomy materials. “Small HCC” is defined by tumor size which is smaller than 2 cm in diameter [15]. Small HCCs have been further classified into early HCC and small progressed HCC, based on morphological features. Early HCC has a vague nodular appearance with incomplete or absent fibrous capsule, well-differentiated morphology, and often steatosis. Progressed HCCs, on the other hand, are clearly malignant appearing with distinct nodular architecture, destructive or pushing growth, and frequent vascular invasion. Early HCC has a longer time to recurrence and a higher 5-year survival rate than progressed HCC [8]. Although not mandatory, it is also good practice to categorize HCC according to macroscopic findings [16]. In some studies, macroscopic tumor classification has suggested prognostic impact [17, 18]. A study by Lee et al. from Seul had shown that gross features are independent predictor of overall and disease-free survival regardless of tumor size. They classified 242 HCC resection specimens based on the gross appearance into vaguely nodular, expanding nodular, multinodular confluent, nodular with perinodular extension, and infiltrative types. Infiltrative type had the worse prognosis whereas vaguely nodular and expanding nodular had more favorable prognosis [17]. The other important issue is determining of macroscopic vascular invasion which has impact on prognosis and staging. It has some value to define the localization of the tumor thrombus in the portal vein, i.e., in the main portal vein or its branches [19]. In the last edition of WHO Blue book series on Digestive System Tumors, four main macroscopic patterns of HCC were defined that are important for staging: a single distinct nodule, a large dominant nodule with satellite nodules which are defined as nodules within 2 cm of the main nodule, multiple tiny nodules (up to hundreds) like cirrhotic nodules (aka diffuse or cirrhotomimetic pattern), and lastly, multiple distinct nodules. One more important detail is evaluation of non-tumoral liver because it has impact on defining etiology and follow up purposes in which liver fibrosis has negative impact for recurrences and new tumor developments [20].
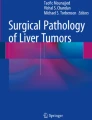
In microscopic examination, conventional HCC (cHCC) is composed of hepatocyte-like cells which produce microtrabecular, macrotrabecular, pseudoglandular/pseudoacinar, and solid (compact) growth patterns. Macrotrabecular pattern is defined as 6–20 cell thickness [21]. Absence of normal portal tracts, presence of unpaired/non-triadal arteries, and invasion of septa and reticulin loss are the important malignancy findings in case of HCC [3, 7]. In early cases, caution for cellularity helps to notice dysplastic or malignant nature of the lesion. Trabecular structure is the most common growth pattern. By definition, trabeculae should have more than 3 cell thickness. Tumor cells may have eosinophilic, steatotic, or sometimes clear cytoplasm. A variety of intrahepatocytic inclusions may be seen that include Mallory-Denk bodies, D-PAS (Periodic Acid Schiff with diastase) positive eosinophilic globules, and pale bodies. Bile production is a diagnostic feature for hepatocellular differentiation [9]. Conventional HCCs can be well, moderate, or poorly differentiated. In well-differentiated and moderately differentiated HCCs, the tumor cells are clearly hepatocytic in nature and demonstrate obvious cytologic atypia (Fig. 1a, b). Poorly differentiated HCCs may show a trabecular or solid growth pattern with marked cellular pleomorphism. The malignant nature of these lesions is immediately obvious based on histology; however, immunohistochemistry (IHC) is often needed to confirm their hepatocytic nature [18]. While histological grading of HCC has an important prognostic role, there is a heterogeneity on the microscopic assessment of this tumor [22]. The most common grading system in the literature is Edmondson and Steiner system. It divides HCC into four grades based on cytological features with grade 1 being the best differentiated. Current three-tier classification (well, moderately, and poorly differentiated) of HCC that is also suggested in the last WHO blue book is somewhat similar to this system, but it combines architectural and nuclear features [2, 4, 16]. Approximately 40% of masses of 1–3 cm diameter comprise different HCC tumor types (with mixed architectural and cytological features) and different degrees of differentiation in the same tumor [4]. Tumor size, and therefore tumor heterogeneity, also affects the reliability of HCC grading in the biopsy [23].

Conventional HCC. H&E. a Lower power. b Higher power
Histopathologic Subtypes
There are several subtypes of HCC which account approximately 35% of HCCs. These subtypes are steatohepatitic, clear cell, macrotrabecular-massive (MTM), scirrhous, chromophobe, fibrolamellar, and neutrophil-rich and lymphocyte-rich subtypes, in decreasing order. Except clear cell and lymphocyte-rich subtypes, all other subtypes have key molecular features. In general, clear cell and lymphocyte-rich subtypes have better prognosis; MTM variant and neutrophil-rich subtypes have worse prognosis when compared with the cHCC. The steatohepatitic and chromophobe subtypes have a similar prognosis with cHCC. All subtypes excluding fibrolamellar carcinoma can be seen cirrhotic and non-cirrhotic livers; fibrolamellar carcinoma does occur in non-cirrhotic background by definition.
The steatohepatitic variant of HCC shows steatohepatitis like findings such as steatosis, Mallory-Denk bodies ballooning of tumor cells, inflammation, and pericellular fibrosis. It is the most common variant (5–20%). It is frequently associated with one more known risk factor for NAFLD [24]. In the literature, there are steatohepatitic HCC cases which are reported in the absence of background fatty liver disease or metabolic syndrome [24, 25]. Its molecular features are IL-6/JAK/STAT activation and lower frequency of CTNNB1, TERT, and TP53 mutations when compared to other HCCs.
The clear cell variant of HCC is composed of predominantly (> 80%) “clear cells” as is its name. To discriminate from lipid droplets can be challenging; indeed, some degree of steatosis can be seen in this subtype. This subtype can imitate other clear cell tumors such as clear cell renal cell carcinoma. Especially in small biopsy samples, this differential should be kept in mind.
The MTM variant demonstrates prominent thick trabeculae in most of the tumor (at least 50%). In the literature, thickness of trabeculae varies between 6 and 20 cells [21, 26]. It is defined as more than 10 cells in WHO Blue book. Radiologically, MTM-HCC was reported to preferentially demonstrate irregular rim–like arterial phase enhancement on gadoxetate-enhanced magnetic resonance imaging [24]. This variant has aggressive features with frequent vascular invasion, poor differentiation, CK19 positivity, and poor clinical outcome. It is also frequently with HBV infection and has high serum alpha-fetoprotein (AFP) levels. In a study by Ziol et al., even focal existence of macrotrabecular pattern such as seen in biopsy samples is still with poor outcome [27]. Thus, it is advisable to give the percentage of the macrotrabecular pattern in pathology reports for the data cumulation.
The scirrhous variant of HCC is characterized by dense intratumoral fibrous stroma, occupying at least 30–50% of the tumor. It can develop beneath liver capsule leading to pedunculated gross view. The cellular component is made up of mature hepatocyte-like cells rimmed by smaller tumor cells that resemble hepatic stem/progenitor cells with frequent expression of stemness-related markers, such as CK19, CK7, and epithelial cell adhesion molecule (EpCAM). This variant has overlapping imaging findings with cholangiocarcinoma (CC) due to dense fibrous stroma results in imaging findings that overlap with those of. In the other hand, fibrosis can occur either after various regimens of oncologic treatment (chemotherapy, transarterial chemoembolization, irradiation) or in untreated patients. HCC exhibiting post-treatment fibrosis should not be classified as scirrhous [3]. The key molecular features are TSC1/TSC2 mutations and transforming growth factor-beta signaling activation [21]. From the clinical outcome view, even it has been reported with aggressive features compared with cHCC; its prognosis is not clear yet.
Chromophobe HCC is characterized as with clear (i.e., chromophobic) cytoplasm of the tumor cells and focal areas of striking nuclear atypia in a background of otherwise “bland-looking” cytology. Initially, it was named as “chromophobe HCC with abrupt anaplasia”. The key molecular feature of this subtype is alternative lengthening of telomeres. In the meaning of clinical outcomes, the prognosis seems to be similar to cHCC [21]. .
The fibrolamellar subtype of HCC (aka fibrolamellar carcinoma) has distinctive clinical characteristics. It occurs most commonly in children and young adults. It is not associated with chronic liver disease or cirrhosis. Although fibrolamellar carcinoma was reported in cirrhotic background, these cases are probably misdiagnosed or actually a cHCC with fibrolamellar foci [14, 28]. It has also unique microscopic findings that are large eosinophilic tumor cells with large vesicular nuclei and prominent nucleoli, pale bodies, and separated by dense parallel/lamellar/multilayered fibrosis [21, 24]. Tumor cells express CD68, frequently CK7 and CK19 [8]. Fibrolamellar carcinoma shares the fibrous stroma feature with scirrhous HCC, but tumor cell morphology and stromal fibrosis patterns are different enough for differential diagnosis. The molecular feature of fibrolamellar HCC which also serves as a useful diagnostic tool and also pathognomonic for this subtype is DNAJB1-PRKACA gene fusion. Its prognosis seems to be the same with cHCC in non-cirrhotic background.
The neutrophil-rich variant is characterized histomorphologically by diffuse neutrophilic infiltration within the HCC. It has some supportive clinical findings such as elevated leukocyte counts, C-reactive protein, and IL-6. Focal sarcomatoid foci can be seen in this variant. The G-CSF production by the tumor cells is the key molecular finding.
The lymphocyte-rich variant of HCC demonstrates massive intratumoral lymphocytic infiltration. It has also been referred to as lymphoepithelioma-like HCC or HCC with lymphocyte-rich stroma [24]. The molecular features of this subtype have not been fully elucidated yet, but it has frequent programmed death-ligand 1 (PD-L1) expression. Interestingly, it does not show an association with Epstein-Barr virus infection, unlike similar tumors of some other organs such as the stomach or nasopharynx [14, 24]. Lymphocyte-rich HCC is possibly more susceptible to immunotherapies.
Differential Diagnosis
Differential diagnosis of HCC should be started with checking clinical and imaging findings. In a cirrhotic patient with or without elevated serum AFP levels, the mass lesion in the liver is mostly a primary liver cancer and in most of the cases is a HCC [3]. In this scenario, large/macro regenerative nodules (MRNs), dysplastic nodules (DNs), and CCs should be included in differential diagnosis. In the absence of known chronic liver disease or cirrhosis, metastasis, focal nodular hyperplasia (FNH), and hepatocellular adenoma (HA) are the top differential diagnoses. Of course, HCC can be seen in non-cirrhotic livers in the case of fibrolamellar carcinoma.
MRNs represent cirrhotic nodules that are > 5 mm and devoid of any cytological or architectural atypia [8]. Usually, they do not cause a differential diagnosis problem on the microscopic evaluation.
DNs are defined with cytological or architectural atypia. They are usually 5–15 mm in diameter and can be detected either by imaging or at the time of macroscopic evaluation. In liver, cytological atypia is defined by either small cell or large cell change. Indeed, large cell change is defined as large hepatoid cells with normal or high nucleus/cytoplasm (N/C) ratio. These cells frequently show multinucleation; nuclei can be hyperchromatic and pleomorphic. Large cell change is a frequent finding in hepatectomy specimens, and it is most likely a reactive phenomenon. On the other hand, small cell change is accepted as a form of actual dysplasia. These hepatocytes show decreased cell volume, high N/C ratio, and minimal nuclear pleomorphism. DNs care classified as low grade (LGDN) and high grade (HGDN) by their cytologic and/or architectural patterns [3, 8]. LGDNs are often distinct from the surrounding liver because of fibrous tissue around the nodule. They show mild increase in cell density (less than 1.3 times compared with surrounding liver parenchyma) and lack cytologic atypia (small cell change), although they may show large cell change. Unpaired arteries are sometimes present in small numbers. The cell plates display normal thickness, and the lesion contains portal tracts and central veins. LGDNs are difficult to separate from MRNs on needle biopsies. HGDNs show cytologic atypia in the form of small cell change and increased cell density (1.3–2 times when compared with the perinodular parenchyma), but the features are insufficient to diagnose HCC. Partial sinusoidal capillarization along with few non-triadal arteries can be seen. Pseudoacini are absent or rare. Secondary nodules arising in HGDN (“nodule in nodule”) most likely represent HCC arising in HGDN [8, 15]. The distinction between HGDN and early HCC can be difficult in some cases, and the presence of pseudoacini formation more than focal and thickened hepatic cell plates, presence of stromal invasion into portal tracts, fibrous septa, or adjacent parenchyma and loss of reticulin network helps make the diagnosis of HCC, but invasive features may be absent in biopsies.
While HA and FNH have also been described in cirrhotic livers, they are most often seen in non-cirrhotic livers [8]. FNH is a benign hepatocellular lesion which is more common than HA. It is thought to be a regenerative response to vascular changes. FNH is characterized by nodular architecture, hypervascular central scar associated with thick fibrous septa between hepatocyte nodules, inflammatory infiltrate, presence of ductular reaction, and sinusoid dilation; there are intervening fibrous bands that radiate from a central scar and contain abundant, proliferating bile ductules [3]. When it is big enough and has typical imaging findings, its diagnosis is straightforward. In atypical cases, it needs to be differentiated from other mass lesions. In these atypical cases, i.e., without central scar or in cirrhotic background, immunohistochemistry can be useful.
HA is a rare, benign neoplasm that is most often seen in women in the reproductive age group and is strongly associated with oral contraceptive use. Based on molecular and genomic data, HAs are classified as HNF1A inactivated, inflammatory, and beta-catenin-activated inflammatory subtypes. HA can be single or multiple. Its histomorphology shares some features with HCC such as composing of relatively monomorphic hepatocytes and lacks true portal tracts and thin-walled unpaired arteries. Next to clinical features, clues for the differentiation from HCCs are non-cirrhotic background, thin hepatocyte plates, absence of pseudoacini structures, and intact reticulin network. However, one needs to be aware that HAs with steatosis can show focal loss of reticulin, which can be misleading, especially on small biopsies. It is worth acknowledging that some HAs cannot be reliably differentiated from well-differentiated HCCs, especially on small biopsies [8].
Combined Hepatocellular-Cholangiocarcinoma
Combined (mixed) hepatocellular-cholangiocarcinoma (cHCC-CC) is defined as a primary liver cancer showing unequivocal presence of both hepatocytic and cholangiocytic differentiation in the same tumor (Fig. 2a–c). The 2 components histologically can either be juxtaposed with or intermingled with each other. There is no definite cutoff value as to the minimal proportion of each component present in a tumor to render a diagnosis of cHCC-CCA [24]. Collision tumor or two separate primaries of HCC and CC in the same liver do not qualify for cHCC-CC diagnosis. It is recommended that diagnosis is based on routine histopathology with hematoxylin and eosin (H&E); immunostains are supportive but not essential for diagnosis [29].

cHCC-CC. H&E and CK19. a Lower power. b Higher power. c CK19
Special Stains
The reticulin stain is one of the routinely ordered histochemical stain for microscopic examination of liver biopsies. It is also an essential for evaluation of hepatocellular mass lesions. Reticulin stain helps by delineating the thick trabeculae and loss of reticulin network [8]. Loss of normal reticulin network and thickened trabecular structures are the clues for HCC. It should be kept in mind that reticulin fiber disruption can also be seen in steatohepatitis and steatosis. HGDNs and HAs can show patchy reticulin loss.
Mucin stains have some role in the differential diagnosis with adenocarcinomas which show mucin production mostly. By the way, mucin production was reported in some fibrolamellar carcinomas in the literature [28].
Immunohistochemistry has multiple roles in evaluation of hepatic mass lesions: confirmation of hepatocellular origin, determining the hepatocellular malignancy, differential diagnosis with other hepatocellular lesions and metastasis, and lastly giving prognostic information. At the beginning, one needs to keep this in mind that none of the markers is 100% sensitive or specific [9]. It is imperative that the pathologist is aware of the potential pitfalls (false positivity and false negativity) associated with each marker and should not make the diagnosis on the basis of a marker alone. It is important to be judicious in stain interpretation, keeping in mind the clinical features, imaging findings, and morphology of the lesion in every case [4].
In determining hepatocellular origin, there is a list of markers. The most known markers are HepPar-1, Arginase-1(Arg-1), Glypican-3 (GPC-3), AFP, polyclonal carcinoembryonic antigen (pCEA), CD10, and bile salt export protein (BSEP). The last 3 markers are known as canalicular markers which show canalicular staining pattern. In general, for supporting hepatocellular origin, a panel of Arg-1, HepPar-1 and a canalicular marker can be useful. Arg-1 is the most specific and sensitive marker (approximately 90%) for hepatocellular origin [3, 30, 31]. Arg-1 can be positive in non-hepatocellular tumors such as pancreatic carcinoma, prostate carcinoma, breast carcinoma, colorectal adenocarcinoma, CC, and hepatoid carcinomas [3]. HepPar-1 has also high sensitivity and specificity in HCC close to 80%. However, in high-grade tumors, its expression is less than 50%. CCs and metastatic esophageal and gastric and pulmonary adenocarcinomas can show strong positivity with this marker. It can be positive in small intestinal adenocarcinoma and hepatoid carcinomas too [3, 31]. GPC-3 is normally expressed in fetal liver and placenta, but it is negative in normal liver and benign hepatocellular tumors (see next). Thus, GPC-3 expression is a good indicator of malignancy in a hepatocellular tumor. But its staining can be patchy or focal. So, a negative result cannot rule out HCC [4]. On the other hand, GPC-3 is not a specific marker for hepatocellular lineage. It can be positive in metastatic adenocarcinomas and germ cell tumors. It is the same for AFP; it can be expressed in germ cell tumors [3, 9, 32, 33]. In general, the sensitivity of nearly all these markers decreases with loss of differentiation. But the sensitivity of AFP staining increases in poor differentiated tumors. The canalicular markers have a near 100% specificity for hepatocytic differentiation [8]. Unfortunately, in a poorly differentiated hepatocellular tumor, canalicular staining can be lost, too [3]. It is noteworthy that some of the HCC subtypes can show interesting or different staining patterns. For example, fibrolamellar carcinomas are positive with CK7 and CD68; scirrhous HCCs are positive with CK19, CK7, and EpCAM.
Confirmation of malignancy in a given hepatocellular tumor and differential diagnosis between hepatocellular mass lesions are best done with a panel of markers again. GPC-3, glutamine synthetase (GS), heat shock protein 70 (HSP70), CD34, CK19/CK7, and Ki67 are the most useful markers for evaluation malignancy in a hepatocellular lesion. In most papers, a combination of first three markers is suggested [2, 7, 9, 23, 25]. Positive staining with at least of these three markers has been shown to be specific for the diagnosis of HCC [30]. When these three markers, GPC3, HSP70, and GS, were applied as an immunohistochemical panel to a set of benign and malignant nodules that had been resected from cirrhotic livers, the positivity for any two of the three markers was found to indicate malignancy with 72% sensitivity and 100% specificity [2, 34]. Normal liver and benign hepatocellular lesions do not express GPC-3, in most of the cases [31]. But GPC-3 positivity has been reported in DNs especially in HGDNs [3], and it can show patchy staining in cirrhotic HCV cases. In a review article, GPC3 positivity was reported as < 30% of their HCC cases [8]. Our experience is the same (personal observation). Though a positive GPC3 is useful in making the diagnosis of HCC, a negative result cannot rule it out (Fig. 3a, b).

GPC-3 (a) and GS (b) positivity in HCC
HSP70 can be positive in isolated periseptal hepatocytes, apoptotic hepatocytes, and stellate cells and focally in HGDNs. For a diagnosis of HCC, HSP70 should show strong nuclear positivity [8].
GS is normally expressed in pericentral areas and in a limited non-hepatocellular tumors. It was reported that for diagnosis of HCC, GS should be diffusely positive in at least 50% of the tumor cells [8]. Thus, diffuse, selective, and strong positivity should be sought for each marker. It should be kept in mind, GS can be expressed in HGDNs [3]. In beta-catenin-activated HAs, GS shows diffuse positivity. FNH has a typical “map-like” staining with GS (Fig. 4).

“Map-like” staining in FNH with GS
CD34 demonstrates the sinusoidal capillarization which can be seen in HGDNs and HCCs with an extensive manner by the increasing cellular and architectural atypia. Focal capillarization of sinusoids may be seen in FNH and HAs [3] (Fig. 5).

Diffuse sinusoidal capillarization with CD34 in HCC
Ductular markers such as CK7 and CK19 help to evaluate the absence or existence of ductular reaction. Cirrhotic nodules are rimmed by a ductular reaction. FNH shows ductular proliferation. In contrast, a gradual loss of ductular reaction correlates with progression of cirrhotic to dysplastic nodule and further to HCC [3] (Fig. 6).

Absence of ductular reaction in contrast with peritumoral cirrhotic parenchyma (upper part). a H&E. B CK19 staining
Ki67 is the least useful marker for HCC diagnosis in general. But it can help in catching small and well-differentiated hepatocellular neoplasms by showing a little more extensive positivity in lesion when compared with non-lesional background.
Immunohistochemistry can also give prognostic information for HCC patients. Several biomarkers have been investigated in HCC for prognostication and treatment decisions. CK19 positivity in HCC is with poor prognosis like other stem-cell markers such as CD133, EpCAM, Kit. Immunohistochemical staining for endothelium-specific markers CD31, CD34, or vWF allow semi-quantitative assessment of microvessel density, which is a significant prognostic indicator. High microvessel density had been found to be associated with poor prognosis [2]. Microvascular invasion (MVI) is a poor prognostic sign in HCC. Although in a study by Carr et al. it was suggested that serum GGT was significantly associated with MVI [35], currently, MVI is diagnosed in histopathological examination of resection specimens. There are studies for prediction of MVI in needle biopsies [23]. In these studies, immunohistochemical analysis of PIVKA-II and H4K20me2 combination [11] and demonstration of vessel encapsulating tumor clusters (VETC) by CD34 staining were reported as powerful predictors of MVI on biopsy specimens [36]. Moreover, in another study, it was claimed that sorafenib is effective in prolonging the survival of VETC+, but not VETC−, patients. Thus, VETC pattern may act as a predictor of sorafenib benefit for HCC [37]. The presence of microvascular invasion or satellites is associated with a high risk of recurrence, and such a profile might prime the indication of liver transplantation in patients before recurrence detection [1].
IHC markers are also increasingly being used for the decisions of molecular targeted therapy and as a predictor of therapeutic response. Immune biomarkers such as immune checkpoint inhibiting antibodies anti-PD-1, anti-PD-L1, and anti-CTLA-4 are useful for decisions regarding adjuvant therapy [2].
Molecular Genetic Landscape and Microenvironment
There are growing attempts to classify tumors by their molecular genetic signatures. This is already integrated to diagnosis in central nervous system tumors and hematolymphoid neoplasms. HCC is a heterogeneous tumor. In studies with next-generation sequencing (NGS), intratumoral heterogeneity (ITH) frequency was reported from 5.21 to 88.27% in HCCs [38]. ITH challenges precise genomic profiling and may lead to target treatment failure. Genetic and epigenetic alterations that progressively accumulate in a background of chronic liver injury and inflammation lead to the initiation and progression of HCC, involving a multi-step process [39]. As an inflammation-associated tumor, it is well evidenced that the immunosuppressive microenvironment of HCC can promote immune tolerance and evasion [40]. Although viral hepatitis are the most common etiologies of the cirrhosis globally, our knowledge of genetic and epigenetic changes in HCC upon viral infections is still limited. Sun et al. in their genome-wide study examined the differences between HBV- and HCV-infected hepatocellular carcinomas. They concluded that there are different epigenetic changes of HBV/HCV-related hepatocarcinogenesis [6].
In recent years, tumor-infiltrating immune cells have been intensively analyzed and characterized. For numerous solid tumors, including primary liver cancer, associations between certain immune cell populations and response to therapy as well as on prognosis have been proposed [41]. Although the precise significance of the tumor immune microenvironment is still not fully understood, a high density of myeloid cells is often associated with a poor prognosis, and a high density of infiltrating T-effector cells is often associated with a good prognosis. Thus, understanding the immune microenvironment may predict, guide and improve immunotherapy. During the progression of liver diseases, inflammation is considered a driving factor and a prerequisite for liver cancer.
The molecular classification of hepatocellular carcinoma is still developing. The pathogenesis of hepatocellular carcinoma (HCC) is a complex process. During the last decade, advances in genomic technologies enabled delineation of the genomic landscape of HCC, resulting in the identification of the common underlying molecular alterations. The tumor microenvironment, regulated by inflammatory cells, including cancer cells, stromal tissues, and the surrounding extracellular matrix, has been extensively studied using molecular data. The integration of molecular, immunological, histopathological, and clinical findings has provided clues to uncover predictive biomarkers to enhance responses to novel therapies [39]. In a French study, HCCs were classified into G1-G6 based on transcriptomics. G1-G3 subclasses demonstrated correlation with histological features of poor differentiation, frequent macrovascular invasion, foci of clear cells, sarcomatous change, compact and macrotrabecular pattern, and foci of pleomorphic and multinucleated cells. G4-G6 subclasses revealed low cell proliferation, association with small tumor size, lack of satellite nodules, or MVI and tumors were well-differentiated [42]. In another study by Hoshida et al., three common molecular subclasses defined were named as S1, S2, and S3 by using the unsupervised clustering-based definition [43]. Briefly, class S1 was associated with a higher risk of early recurrence and invasive/disseminative phenotype. This class showed a predominance of WNT pathway activation and interaction with transforming growth factor-β (TGF-β) activation. Class S2 tumors were associated with high levels of plasma AFP levels, MYC, and AKT activation signatures, and enrichment of positive EpCAM signatures. The TP53 mutation associated with stepwise malignant transformation was higher in the S1 and S2 classes than in the S3 class, while the β-catenin mutation was more common in well-differentiated S3 tumors. The authors recommended targeted agents such as β-catenin and PI3K inhibitors according to the molecular classifications. Another French group investigated molecular-phenotypic correlations in HCCs by pathological review, immunohistochemistry, gene expression profiling, and sequencing in resected HCC samples [44]. They found that CTNNB1 (40%) and TP53 (21%) mutations were mutually exclusive and defined two major groups of HCC characterized by distinct phenotypes. Sia et al. defined an “immune-class” in their study [45]. Key features of this class include actual presence and activation of immune cells, enhanced cytolytic activity, protein expression of PD-1 and PD-L1, and enrichment of gene signatures predictive of response to immunotherapies. They identified 2 subclasses, characterized by adaptive or exhausted immune responses. And claimed that some HCCs might be susceptible to therapeutic agents designed to block the regulatory pathways in T cells, such as PD-L1, PD-1, or TGF -β 1 inhibitors. Liu et al. examined crucial genes involved in HCC through multidimensional methods and revealed potential molecular mechanisms. They found 164 differentially expressed genes (DEGs) (92 downregulated genes and 72 upregulated genes) [5]. Ding et al. analyzed HCCs and surrounding non-tumor tissues to identify genetic and epigenetic variations within liver tumors, among hepatic lesions, and between primary and relapsing tumors [46]. They determined the monoclonal origins of individual tumors using a single sample collection approach that captured more than 90% of mutations that are detected in all regions of tumors. Phylogenetic and phyloepigenetic analyses revealed interactions and codependence between the genomic and epigenomic features of HCCs. Methylation analysis revealed a field effect in cirrhotic liver tissues that predisposes them to tumor development. Comparisons of genetic features revealed that 52% of recurrent HCCs derive from the clonal lineage of the initial tumor. Another microenvironment study was done by Kurebayashi et al. by using multiplex immunohistochemistry [47]. They classified the immune microenvironment of HCC into three immunosubtypes (immune-high, immune-mid, and immune-low) with additional prognostic impact on histological and molecular classification of HCC. In their study, the immune-high subtype was found as associated with poorly differentiated HCC, CK19, and/or Sal-like protein 4 (SALL4), high-grade HCC, and Hoshida’s S1/Boyault’s G2 subclasses. Furthermore, patients with high-grade HCC of the predominant immune-high subtype had significantly better prognosis. Kang et al. studied the immunogenomic characteristics of hepatocellular carcinomas (HCCs) with immune cell stroma (HCC-IS) by using in situ hybridization for EBV, immunohistochemistry, multiplex immunofluorescence staining, and whole exome and transcriptome sequencing [48]. They concluded that immune classifiers could help identify patients who might respond better to immunotherapies and those who need additional molecular inhibitors such as the TGF-β inhibitor. They also found that a high density of Epstein-Barr virus-positive tumor-infiltrating lymphocytes is associated with inferior prognostic outcomes, possibly as a result of immune escape due to significant CD8 T cell exhaustion.
Liquid Biopsy in HCC
A liquid biopsy collects the sample of body non-solid biological tissue, such as blood for different analyses. Several other body fluids could also be used for specific liquid biopsy applications, such as cerebrospinal fluid (CSF) for central nervous system tumors, saliva for head and neck tumors, pleural fluid for thoracic and metastatic cancers, ascites for abdominal and metastatic cancers, stool for gastrointestinal tract cancers, urine for urinary tract cancers, and bile for the gallbladder cancer [49]. Compared with invasive procedures, circulating tumor DNA (ctDNA) has been proposed as an alternative source to perform molecular profiling of tumor DNA in cancer patients. The detection of abnormal forms of circulating cell-free DNA (cfDNA) that originate from cancer cells (ctDNA) provides a novel tool for cancer detection and disease monitoring. This may also be an opportunity to optimize the early diagnosis of HCC. In recent years, many studies have investigated the specific gene changes from HCC tumor tissues that can also be observed in ctDNA as potential specific biomarkers [50].
Computational Pathology in HCC
In developments on computational area, the whole slide image (WSI) of a biopsy specimen and selecting interested foci (region of interest—ROI) on the slides are possible. Deep learning is a type of artificial intelligence (AI) method, commonly used in computational pathology, which is able to “learn” how to perform tasks based on examples. Advances in computational technology and data storage make it possible to rapidly generate a large number of WSI datasets. As a result, computational pathology, which handles and analyzes digitized image data, has come under the spotlight in the field of pathological research. There are studies on HCC pathology with this technology; in two of them, diagnostic results are promising [51, 52].
Data Availability
Not applicable.
References
Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet. 2018;391:1301–14. https://doi.org/10.1016/S0140-6736(18)30010-2.
Rastogi A. Changing role of histopathology in the diagnosis and management of hepatocellular carcinoma. World J Gastroenterol. 2018;24(35):4000–13. https://doi.org/10.3748/wjg.v24.i35.4000.
Mezale D, Strumfa I, Vanags A, Kalva A, Balodis D, Strumfs B, et al. Diagnostic algorithm of hepatocellular carcinoma: classics and innovations in radiology and pathology. 2018. https://doi.org/10.5772/intechopen.76136.
Agni RM. Diagnostic histopathology of hepatocellular carcinoma: a case-based review. Semin Diagn Pathol. 2017;34(2):126–37. https://doi.org/10.1053/j.semdp.2016.12.008.
Liu ZK, Zhang RY, Yong YL, Zhang ZY, Li C, Chen ZN, et al. Identification of crucial genes based on expression profiles of hepatocellular carcinomas by bioinformatics analysis. PeerJ. 2019;7:e7436. https://doi.org/10.7717/peerj.7436.
Sun S, Li Y, Han S, Jia H, Li X, Li X. A comprehensive genome-wide profiling comparison between HBV and HCV infected hepatocellular carcinoma. BMC Med Genet. 2019;12:147. https://doi.org/10.1186/s12920-019-0580-x.
Ueno A, Masugi Y, Yamazaki K, Kurebayashi Y, Tsujikawa H, Effendi K, et al. Precision pathology analysis of the development and progression of hepatocellular carcinoma: implication for precision diagnosis of hepatocellular carcinoma. Pathol Int. 2020;70:140–54. https://doi.org/10.1111/pin.12895.
Vyas M, Jain D. A practical diagnostic approach to hepatic masses. Indian J Pathol Microbiol. 2018;61:2–17. https://doi.org/10.4103/IJPM.IJPM_578_17.
Quaglia A. Hepatocellular carcinoma: a review of diagnostic challenges for the pathologist. J Hepatocell Carcinoma. 2018;5:99–108. https://doi.org/10.2147/JHC.S159808.
Park BV, Gaba RC, Huang YH, Chen YF, Guzman G, Lokken R. Histology of hepatocellular carcinoma: association with clinical features, radiological findings, and locoregional therapy outcomes. J Clin Imaging Sci. 2019;9:52. https://doi.org/10.25259/JCIS_111_2019.
Poté N, Cauchy F, Albuquerque M, Cros J, Soubrane O, Bedossa P, et al. Contribution of virtual biopsy to the screening of microvascular invasion in hepatocellular carcinoma: a pilot study. Liver Int. 2018;38:687–94. https://doi.org/10.1111/liv.13585.
Cassinotto C, Aubé C, Dohan A. Diagnosis of hepatocellular carcinoma: an update on international guidelines. Diagn Intervent Imaging. 2017;98:379–91. https://doi.org/10.1016/j.diii.2017.01.014.
Huh J, Kim KW, Kim J, Yu E. Pathology-MRI correlation of hepatocarcinogenesis: recent update. J Pathol Transl Med. 2015;49(3):218–29. https://doi.org/10.4132/jptm.2015.04.15.
Calderaro J, Ziol M, Paradis V, Zucman-Rossi J. Molecular and histological correlations in liver cancer. J Hepatol. 2019;71(3):616–30. https://doi.org/10.1016/j.jhep.2019.06.001.
Torbenson MS, Ng IOL, Park YN, Roncalli M, Sakamoto M. Hepatocellular carcinoma. In: WHO classification of tumours editorial board, editor. Digestive system tumours. WHO classification of tumours series. 5th ed. Lyon: International Agency for Research on Cancer; 2019. p. 229–39.
Martins-Filho SN, Alves VAF. The strengths and weaknesses of gross and histopathological evaluation in hepatocellular carcinoma: a brief review. Surg Exp Pathol. 2019;2:23. https://doi.org/10.1186/s42047-019-0047-6.
Lee Y, Park H, Lee H, Cho JY, Yoon YS, Choi YR, et al. The clinicopathological and prognostic significance of the gross classification of hepatocellular carcinoma. J Pathol Transl Med. 2018;52:85–92. https://doi.org/10.4132/jptm.2017.11.13.
Jang JY, Lee JS, Kim HJ, Shim JJ, Kim JH, Kim BH, et al. The general rules for the study of primary liver cancer. J Liver Cancer. 2017;17:19–44. https://doi.org/10.17998/jlc.17.1.19.
Zhang XP, Chen ZH, Zhou TF, Li LQ, Chen MS, Wen T, et al. A nomogram to predict early postoperative recurrence of hepatocellular carcinoma with portal vein tumour thrombus after R0 liver resection: a large-scale, multicenter study. Eur J Surg Oncol. 2019;45:1644–51. https://doi.org/10.1016/j.ejso.2019.03.043.
Shimada S, Kamiyama T, Orimo T, Nagatsu A, Asahi Y, Sakamoto Y, et al. Long-term prognostic factors of patients with hepatocellular carcinoma who survive over 10 years after hepatectomy. J Surg Oncol. 2020;121:1209–17. https://doi.org/10.1002/jso.25910.
Kim H, Jang M, Park YN. Histopathological variants of hepatocellular carcinomas: an update according to the 5th Edition of the WHO Classification of Digestive System. J Liver Cancer. 2020;20(1):17–24. https://doi.org/10.17998/jlc.20.1.17.
Martins-Filho SN, Paiva C, Azevedo RS, Alves VAF. Histological grading of hepatocellular carcinoma—a systematic review of literature. Front Med. 2017;4:193. https://doi.org/10.3389/fmed.2017.00193.
Di Tommaso L, Spadaccini M, Donadon M, Personeni N, Elamin A, Aghemo A, et al. Role of liver biopsy in hepatocellular carcinoma. World J Gastroenterol. 2019;25(40):6041–52. https://doi.org/10.3748/wjg.v25.i40.6041.
Lo RCL. An update on the histological subtypes of hepatocellular carcinoma. Hepatoma Res. 2019;5:41. https://doi.org/10.20517/2394-5079.2019.021.
El Jabbour T, Lagana SM, Lee H. Update on hepatocellular carcinoma: pathologists’ review. World J Gastroenterol. 2019;25(14):1653–65. https://doi.org/10.3748/wjg.v25.i14.1653.
Jeon Y, Benedict M, Taddei T, Jain D, Zhang X. Macrotrabecular hepatocellular carcinoma. An aggressive subtype of hepatocellular carcinoma. Am J Surg Pathol. 2019 Jul;43(7):943–8. https://doi.org/10.1097/PAS.0000000000001289.
Ziol M, Poté N, Amaddeo G, Laurent A, Nault JC, Oberti F, et al. Macrotrabecular-massive hepatocellular carcinoma: a distinctive histological subtype with clinical relevance. Hepatology. 2018;68(1):103–12. https://doi.org/10.1002/hep.29762.
Torbenson M. Fibrolamellar carcinoma: 2012 update. Scientifica (Cairo). 2012;2012:743790. https://doi.org/10.6064/2012/743790.
Brunt E, Aishima S, Clavien PA, Fowler K, Goodman Z, Gores G, et al. cHCC-CCA: Consensus terminology for primary liver carcinomas with both hepatocytic and cholangiocytic differentiation. Hepatology. 2018;68(1):113–26. https://doi.org/10.1002/hep.29789.
Pittman ME. Hepatocellular carcinoma: a practical review for the surgical pathologist. Diagn Histopathol. 2018;24(12):500–7. https://doi.org/10.1016/j.mpdhp.2018.09.005.
Koehne de Gonzalez A, Lagana SM. Update on ancillary testing in the evaluation of high-grade liver tumors. surgical pathology. Surg Pathol. 2018;11:367–75. https://doi.org/10.1016/j.path.2018.02.004.
Chen D, Li Z, Song Q, Qian L, Xie B, Zhu J. Clinicopathological features and differential diagnosis of hepatocellular carcinoma in extrahepatic metastases. Medicine (Baltimore). 2018;97(50):e13356. https://doi.org/10.1097/MD.0000000000013356.
Uthamalingam P, Das A, Behra A, Kalra N, Chawla Y. Diagnostic value of glypican3, heat shock protein 70 and glutamine synthetase in hepatocellular carcinoma arising in cirrhotic and non-cirrhotic livers. J Clin Exp Hepatol. 2018;8:173–80. https://doi.org/10.1016/j.jceh.2017.09.005.
Walther Z, Jain D. Molecular pathology of hepatic neoplasms: classification and clinical significance. Pathol Res Int. 2011:403929. https://doi.org/10.4061/2011/403929.
Carr B, Ince V, Bag HG, Ersan V, Usta S, Yilmaz S. Microscopic vascular invasion by hepatocellular carcinoma in liver transplant patients. Clin Pract. 2020;17(3):1487–97.
Renne SL, Woo HY, Allegra S, Rudini N, Yano H, Donadon M, et al. Vessels encapsulating tumor clusters (VETC) is a powerful predictor of aggressive hepatocellular carcinoma. Hepatology. 2019;71(1):183–95. https://doi.org/10.1002/hep.30814.
Fang JH, Xu L, Shang LR, Pan CZ, Ding J, Tang YQ, et al. Vessels that encapsulate tumor clusters (VETC) pattern is a predictor of Sorafenib benefit in patients with hepatocellular carcinoma. Hepatology. 2019;70:824–39. https://doi.org/10.1002/hep.30366.
Huang A, Wang YP, Wang J, Fu PY, Zhang X, Cao Y, et al. Limited bias effect of intratumoral heterogeneity on genetic profiling of hepatocellular carcinoma. J Gastrointest Oncol. 2020;11(1):112–20. https://doi.org/10.21037/jgo.2019.09.13.
Yim SY, Lee JS. The genomic landscape and its clinical implications in hepatocellular carcinoma. J Liver Cancer. 2019;19(2):97–107. https://doi.org/10.17998/jlc.19.2.97.
Fu Y, Liu S, Zeng S, Shen H. From bench to bed: the tumor immune microenvironment and current immunotherapeutic strategies for hepatocellular carcinoma. J Exp Clin Cancer Res. 2019;38:396. https://doi.org/10.1186/s13046-019-1396-4.
Roderburg C, Wree A, Demir M, Schmelzle M, Tacke F. The role of the innate immune system in the development and treatment of hepatocellular carcinoma. Hepat Oncol. 2020;7(1):HEP17. https://doi.org/10.2217/hep-2019-0007.
Boyault S, Rickman DS, de Reyniès A, Balabaud C, Rebouissou S, Jeannot E, et al. Transcriptome classification of HCC is related to gene alterations and to new therapeutic targets. Hepatology. 2007;45:42–52. https://doi.org/10.1002/hep.21467.
Hoshida Y, Nijman SM, Kobayashi M, Chan JA, Brunet JP, Chiang DY, et al. Integrative transcriptome analysis reveals common molecular subclasses of human hepatocellular carcinoma. Cancer Res. 2009;69:7385–92. https://doi.org/10.1158/0008-5472.
Calderaro J, Couchy G, Imbeaud S, Amaddeo G, Letouzé E, Blanc JF, et al. Histological subtypes of hepatocellular carcinoma are related to gene mutations and molecular tumour classification. J Hepatol. 2017;67:727–38. https://doi.org/10.1016/j.jhep.2017.05.014.
Sia D, Jiao Y, Martinez-Quetglas I, Kuchuk O, Villacorta-Martin C, Castro de Moura M, et al. Identification of an immune-specific class of hepatocellular carcinoma, based on molecular features. Gastroenterology. 2017;53:812–26. https://doi.org/10.1053/j.gastro.2017.06.007.
Ding X, He M, Chan AWH, Song QX, Sze SC, Chen H, et al. Genomic and epigenomic features of primary and recurrent hepatocellular carcinomas. Gastroenterology. 2019;157:1630–45. https://doi.org/10.1053/j.gastro.2019.09.005.
Kurebayashi Y, Ojima H, Tsujikawa H, Kubota N, Maehara J, Abe Y, et al. Landscape of immune microenvironment in hepatocellular carcinoma and its additional impact on histological and molecular classification. Hepatology. 2018;68:1025–41. https://doi.org/10.1002/hep.29904.
Kang HJ, Oh JH, Chun SM, Kim D, Ryu YM, Hwang HS, et al. Immunogenomic landscape of hepatocellular carcinoma with immune cell stroma and EBV-positive tumor-infiltrating lymphocytes. J Hepatol. 2019 Jul;71(1):91–103. https://doi.org/10.1016/j.jhep.2019.03.018.
Ye Q, Ling S, Zheng S, Xu X. Liquid biopsy in hepatocellular carcinoma: circulating tumor cells and circulating tumor DNA. Mol Cancer. 2019;18:114. https://doi.org/10.1186/s12943-019-1043-x.
Wu X, Li J, Gassa A, Buchner D, Alakus H, Dong Q, et al. Circulating tumor DNA as an emerging liquid biopsy biomarker for early diagnosis and therapeutic monitoring in hepatocellular carcinoma. Int J Biol Sci. 2020;16(9):1551–62. https://doi.org/10.7150/ijbs.44024.
Liao H, Xiong T, Peng J, Xu L, Liao M, Zhang Z, et al. Classification and prognosis prediction from histopathological images of hepatocellular carcinoma by a fully automated pipeline based on machine learning. Ann Surg Oncol. 2020;27:2359–69. https://doi.org/10.1245/s10434-019-08190-1.
Lu L, Daigle BJ. Prognostic analysis of histopathological images using pre-trained convolutional neural networks: application to hepatocellular carcinoma. Peer J. 2020;8:e8668. https://doi.org/10.7717/peerj.8668.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
None.
Code Availability
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Karadag Soylu, N. Update on Hepatocellular Carcinoma: a Brief Review from Pathologist Standpoint. J Gastrointest Canc 51, 1176–1186 (2020). https://doi.org/10.1007/s12029-020-00499-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12029-020-00499-5