
Abstract
Purpose
Gallbladder cancer is a highly mortal disease with poor prognosis because of late presentation of disease. Survivin and X-linked inhibitor of apoptosis (XIAP) are one of the two important members of inhibitors of apoptosis. Thus, this study aimed to look at the expression of Survivin and XIAP in gallbladder cancer patients.
Methods
Survivin and XIAP expression were investigated in tissues of gallbladder cancer patients (40 cases) and compared with cholelithiasis as control (40 cases) by using immunohistochemistry. Their expression was correlated with clinicopathological parameters.
Results
Significantly higher (p < 0.05), Survivin protein was expressed in gallbladder cancer (n = 67.5%) than control (n = 35%). But it did not show any significant association with any of the clinicopathological parameter while XIAP was not expressed in the GBC patients (p > 0.05).
Conclusion
Overexpression of Survivin in gallbladder cancer suggests its possible role and association with poor prognosis. But XIAP has not been found to be associated with gallbladder carcinogenesis.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Gallbladder cancer (GBC) is an aggressive and highly lethal malignancy [1], the most common cancer of the biliary tract and the sixth most common gastrointestinal cancer [2]. GBC has astonishing symptomatology which results in advanced disease at the time presentation lead to the poor prognosis [3]. Gallbladder carcinogenesis is a multi-step process which results from sequential genetic alterations at different stages of evolution. Development of biomarkers for early detection of GBC is a need of the day [4]. Inhibition of apoptosis is a main factor in the uncontrolled proliferation of cancer cells and is closely related to the tumorigenesis and progression of malignant tumors [5]. Many studies have shown that inhibition of apoptosis plays an important role in tumor growth and drug resistance [6]. Inhibitor of apoptosis (IAP) is identified as a family of endogenous inhibitors of caspases [7, 8].
X-linked IAP (XIAP) and Survivin is the most potent member of human IAPs [9]. XIAP directly binds to caspase-3, -7, -9, and prevents their activities to initiate or execute apoptotic pathways [10]. XIAP has been shown to be overexpressed in most human cancer cell lines and cancer tissues including hepatocellular carcinoma tissues [11]. Irregular expression of XIAP is described in the pathology of several human malignancies. However, only a few large-scale studies provide translational evidence of an association between XIAP expression and clinical outcomes [12,13,14,15,16].
Survivin is an intracellular, multifunctional protein which controls cell proliferation, inhibition of apoptosis, and the promotion of angiogenesis [17, 18]. Survivin overexpression has been studied in various cancers like breast, esophagus, pancreas, bladder, uterus, cervix, ovary, large-cell non-Hodgkin’s lymphoma, and leukemia, neuroblastomas, melanomas, gastric tumors, colon, stomach, liver, oral, thyroid, laryngeal, osteosarcoma, and prostate cancer [18, 19]. Increased Survivin and XIAP expression might serve as diagnostic and prognostic markers in cancer and can be used as therapeutic targets [18]. Their expression pattern is still unknown in gallbladder cancer patients in the area of Indo-Gangetic plain. In the present study, we examined the expression of Survivin and XIAP in gallbladder cancer and correlating its expression with clinicopathological characteristics.
Material and Methods
Study Design
The present case-control study was performed to examine the expression analysis of Survivin and XIAP in gallbladder cancer patients by immunohistochemistry.
Setting
This study has been carried in a single surgical unit of the Institute of Medical Sciences, Banaras Hindu University, Varanasi in collaboration with the Department of Pathology, BHU. The study included gallbladder cancer patients as cases and cholelithiasis as control. The study was performed from September 2013 to July 2015. The study was approved by the institute’s ethics committee.
Participants
Newly diagnosed cases of gallbladder cancer were included in the study. Diagnosis was confirmed by histopathology of excised specimen of gallbladder after surgery. Control group included patients of cholelithiasis who underwent laparoscopic/open cholecystectomy. Patients who had received chemotherapy prior to operation were excluded from the study. Patients with synchronous tumor elsewhere were also not included in the study.
Immunohistochemistry Analysis
Expression analysis of Survivin and XIAP was performed by immunohistochemistry. An anti-Survivin (BioGenex, ready to use) and XIAP (R&D systems) antibody was used for immunohistochemical analysis. Sections of 2 to 3 μ size were placed on 1% poly-l-lysine coated slides and fix at 60 °C for 1 h. The paraffin-embedded tissues were de-paraffinized with xylene and rehydrated through graded ethanol washes. The sections were autoclaved in antigen retriever in citrate buffer (pH 6.0) at 95 °C for 10 min for the first cycle and at 97 °C for 10 min in the second cycle cooled to 26 °C, treated with 3% H2O2 for 20 min to block endogenous peroxidase activity, and then washed with Tris buffer (pH 7.6) for 3 min three times. Then, the sections were incubated with primary antibody (Survivin and XIAP) overnight at 4 °C. For the next day, it was washed with Tris buffer and followed by application of secondary antibody for 30 min. And again washing was performed.
After that diaminobenzidine tetrahydroxychloride chromogen (DAB; Dako, Glostrup, Denmark) was applied for 1 to 10 min until brown colors developed. The sections were counterstained with hematoxylin. A negative control had been keep running in the meantime by simply omitting the primary antibody.
Immunohistochemistry Scoring of Survivin & XIAP
The final results of immunohistochemical analysis had been elucidated by an experienced pathologist who was simply blinded for the certain diagnosis and prognosis for every single case. Both the percentage of positive cells and the strength of the staining were considered in the following method. Five degree magnification visions were chosen randomly under the optical microscope, the calculation of results being as followed: the percentage of positive cells in 0 to 5% was counted 0, 5 to 25% was counted 1, 26 to 50% was counted 2, 51 to 75% was counted 3, and ≥ 76% was counted 4. In respect of staining strength, the score for tumor cells without stain is 0, straw yellow for 1, brown for 2, and tan for 3. The staining index score was the sum of the items above (Survivin score and XIAP score). For the purpose of statistical analysis, 3 was used as a cutoff value to distinguish tumors with a low (< 3) or high (≥ 3) level of expression [20].
Study Size
The sample size was determined by the number of cases came in the outpatient department of the university hospital during the study period.
Statistical Methods
All statistical analyses were performed using SPSS version 16 (SPSS Inc., Chicago, USA). Chi-square Pearson and Fisher’s exact test was used to find the association between various histopathological variables with various molecular subtypes. A p value of less than 0.05 (p < 0.05) was considered as statistically significant.
Results
Participants
The study was carried out in newly diagnosed cases of gallbladder cancer and cholelithiasis as control.
Descriptive Data
A total of 40 patients of GBC (8 men and 32 women) with a mean age of 52.8 ± 10.6 years and 40 of cholelithiasis (9 men and 31 women) with a mean age of 45.68 ± 14.6 years were enrolled. Most common presenting symptoms of GBC cases were pain in the right upper abdomen which was present in 34 (85%) patients. Other symptoms include dyspepsia, belching, and jaundice, which were present in 15(37.5%), 9(22.5%), and 4(10%) of GBC cases, respectively. Ultrasonography (USG) finding shows GB mass in 45% of GBC cases. GB wall thickening and gallstone were present in 35 and 60% of GBC cases, respectively. Liver infiltration was present in 22.5% GBC cases while liver metastasis was present in only two cases. Enlargement of pericholedocal lymph node were present in 25% of the cases. Multiple and single gallstones were present in 24 (60%) and 16 (40%) cases of cholelithiasis. CT scan finding showed that GB mass has been observed in 60.6% of GBC cases. GB wall thickening, GB stone, and liver metastasis was present in 51.5, 60.6, and 3% of GBC cases, respectively. Eighty-five percent of cases were of adenocarcinoma histopathology. Single case of mucinous and signet-ring cell carcinoma histopathology. One third of the patients were of stage III. There was only a single case of stage I in GBC patients (Table 1).
Immunohistochemical Expression of Survivin and XIAP
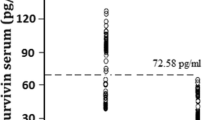
We found that the over expression rate of Survivin in the gallbladder cancer tissues was 67.5% (27 of 40 patients) (Table 2). The expression of Survivin in gallbladder cancer (Fig. 1a) was significantly higher than that in the cholelithiasis patients (p < 0.01) (Fig. 1b). Expression of Survivin is mostly nuclear but cytoplasmic expression is also present in many cases. Intensity was moderate in 16 (40%) of the GBC cases. Dense and mild intensity was present in 8 (20%) and 12 (30%) of GBC cases, respectively (Fig. 1a). While four (10%) cases showed a negative expression of Survivin in GBC cases (Table 2). It did not show any association with any of the clinicopathological parameters (Table 3). In this study, XIAP was not found to be expressed in any of the GBC (Fig. 2a) and cholelithiasis groups (p > 0.05). Some cells shown focal positivity but intensity was mild and XIAP score came to be < 3 and considered as low expression or negative expression. In some immunohistochemistry (IHC) slides, hepatic parenchymal cells showed positive expression but gallbladder tumor cells were negatively stained (Fig. 2b).

a Immunohistochemical expression of Survivin in GBC showing nuclear as well as cytoplasmic staining. b Immunohistochemical expression of Survivin in cholelithiasis showing nuclear as well as cytoplasmic staining

a Immunohistochemical expression of XIAP tumor cells negatively expressed while RBC positively stained. b Immunohistochemical expression of XIAP in hepatocyte XIAP expressed in cytoplasm
Discussion
Survivin is usually an crucial regulator associated with cell death, apoptosis, and cell division along with proliferation that is almost never expressed in regular cells. The expression of Survivin is high during fetal development but low in healthy adult tissues. However, the expression of Survivin increases in most malignant tumors. As a result, Survivin has been considered a potential tumor marker and an important therapeutic target [17]. We investigated the comprehensive evaluation of the gene expression of XIAP and Survivin in human gallbladder cancers.
In the present study, a higher expression of Survivin (67.5%) was observed in GBC than control (p < 0.05). Similar to our results, a recent study also illustrated a higher Survivin expression in esophageal cancer than in normal tissues and found to be associated with poor prognosis. Therefore, they suggested Survivin as a crucial target for hyperthermia in the esophageal cancer treatment [21]. There was no statistical significant association was found with stage, grade, histopathological type, and lymph node and liver metastasis with Survivin expression in our study. Wei et al., (2006) observed that Survivin expression had no specificity, positive predictive value for cell differentiation, and grade as well as clinical stage of GBC [22]. Similarly, other studies also did not find any significant correlation of Survivin with clinicopathological parameters [23,24,25]. Jha et al., (2012b) showed an elevated expression of Survivin in breast cancer cases than control [26]. Wei et al., (2006) studied the expression of Survivin in primary gallbladder cancer in Chinese population and concluded that Survivin might play an important synergistic role in the development of primary gallbladder cancer [22]. The immunohistochemical analysis showed a reduced Survivin expression in hepatocellular carcinoma (HCC) compared with the paired cirrhotic tissue, and only a minority of HCC cores displayed nuclear Survivin immunoreactivity [27]. High-level expression of Survivin was also found in circulating tumor cells in peripheral blood [28]. Khan et al. (2009) have shown that synthetic Survivin enhances the proliferation, drug resistance, and cellular invasion of tumor cells [29]. Similar to our results, Nigam et al., (2014) also found a significant higher mRNA expression of Survivin in GBC in comparison to control and did not observe any significant correlation with different clinicopathological parameters [30]. No significant correlation between Survivin expression and prognosis in biliary tract cancer was also observed in previous reports [31]. XIAP expression was found to be higher in thyroid cancer, particularly in classical papillary thyroid carcinoma, compared to benign thyroid nodules such as nodular hyperplasia and follicular adenoma [32]. However, we did not find any significant difference between the groups (p > 0.05) in case of XIAP expression. An increased expression of XIAP in esophageal squamous cell carcinoma was shown, and its expression was positively correlated with differentiation and p-TNM stage [20]. It had been suggested that the interaction of XIAP and Survivin promotes the invasion of tumor cells and enhances the metastatic spread in vivo [33]. Chen et al., (2013) investigated expression trends of the five tumor-related proteins, Survivin, cIAP1, cIAP2, XIAP, and Livin, in normal bladder tissues and bladder cancer tissues and observed an increasing trend in expression levels of each IAP high-grade bladder tissue compared with low-grade tissue [34]. Others also demonstrated that the over expression of XIAP and Survivin, was involved in the development of prostate disorders [35]. All these studies supported our results which contribute to the development of gallbladder cancer.
In conclusion, overexpression of Survivin in gallbladder cancer suggested its possible role and association with poor prognosis. But XIAP has not been found to be associated with gallbladder carcinogenesis. More expressional study in peripheral blood could be useful both in the diagnosis and prognosis of GBC. Further studies in larger sample size are needed to establish the role of both the proteins in gallbladder cancer.
References
Hueman M, Vollmer C, Pawlik T. Evolving treatment strategies for gallbladder cancer. Ann Surg Oncol. 2009;16:2101–5. https://doi.org/10.1245/s10434-009-0538-x.
Cobourn N, Cleary S, Tan J, Law CH. Surgery for gallbladder cancer: a population-based analysis. J Am Coll Surg. 2008;207:371–82.
Boutros C, Gary M, Baldwin K, Somasundar P. Gallbladder cancer: past, present and an uncertain future. Surg Oncol. 2012;21(4):e183–91.
Dixit R, Shukla VK, Pandey M. Molecular alterations in gallbladder cancer. World J Pathol. 2012;1:31–4.
Qiu Y, Li X, Yi B, et al. Protein phosphatase PHLPP induces cell apoptosis and exerts anticancer activity by inhibiting Survivin phosphorylation and nuclear export in gallbladder cancer. Oncotarget. 2015;6(22):19148–62.
Henry LR, Lee HO, Lee JS, et al. Clinical implications of fibroblast activation protein in patients with colon cancer. Clin Cancer Res. 2007;13(6):1736–41.
Yang YL, Li XM. The IAP family: endogenous caspase inhibitors with multiple biological activities. Cell Res. 2000;10(3):169–77.
Ngan CY, Yamamoto H, Seshimo I, et al. Quantitative evaluation of vimentin expression in tumour stroma of colorectal cancer. Br J Cancer. 2007;96(6):986–92.
Zhu L, Cheng X, Ding Y, et al. Bone marrow-derived myofibroblasts promote colon tumorigenesis through the IL-6/JAK2/STAT3 pathway. Cancer Lett. 2014;343(1):80–9.
LeBleu VS, Taduri G, O’Connell J, et al. Origin and function of myofibroblasts in kidney fibrosis. Nat Med. 2013;19(8):1047–53.
Tu SP, Chi AL, Ai W, et al. p53 inhibition of AP1-dependent TFF2 expression induces apoptosis and inhibits cell migration in gastric cancer cells. Am J Physiol Gastrointest Liver Physiol. 2009;297(2):G385–96.
Kashkar H. X-linked inhibitor of apoptosis: a chemoresistance factor or a hollow promise. Clin Cancer Res. 2010;16:4496–502.
Srinivasula SM, Ashwell JD. IAPs: what’s in a name? Mol Cell. 2008;30:123–35.
Tamm I, Kornblau SM, Segall H, et al. Expression and prognostic significance of IAP-family genes in human cancers and myeloid leukemias. Clin Cancer Res. 2000;6:1796–803.
Liu SS, Tsang BK, Cheung AN, et al. Anti-apoptotic proteins, apoptotic and proliferative parameters and their prognostic significance in cervical carcinoma. Eur J Cancer. 2001;37:1104–10.
Krajewska M, Kim H, Kim C, et al. Analysis of apoptosis protein expression in early-stage colorectal cancer suggests opportunities for new prognostic biomarkers. Clin Cancer Res. 2005;11:5451–61.
Ryan BM, Konecny GE, Kahlert S, et al. Survivin expression in breast cancer predicts clinical outcome and is associated with HER2, VEGF, urokinase plasminogen activator and PAI-1. Ann Oncol. 2006;17:597–604.
Jha K, Shukla M, Pandey M. Survivin expression and targeting in breast cancer. Surg Oncol. 2012a;21:125–31.
Meijer L, Jézéquel A, Roberge M. Survivin in apoptosis control and cell cycle regulation in cancer. Prog Cell Cycle Res. 2003;5:447–52.
Zhou S, Ye W, Shao Q, Qi Y, Zhang M, Liang J. Prognostic significance of XIAP and NF-κB expression in esophageal carcinoma with postoperative radiotherapy. World J Surg Oncol. 2013;11:288.
Qin S, Xu C, Li S, et al. Hyperthermia induces apoptosis by targeting Survivin in esophageal cancer. Oncol Rep. 2015;34(5):2656–64.
Wei D, Qi Z, Wei-wen L, Yun-le W. Expression of laminin and survivin in primary gallbladder carcinoma. Chin J Pathophysiol. 2006;22(11):2207–11. (Abstract)
Tanaka M, Chijiiwa K. Carcinoma of the gallbladder: an appraisal of surgical resection. Surgery. 1994;115:751–6.
Kennedy SM, O’Driscoll L, Purcell R, et al. Prognostic importance of survivin in breast cancer. Br J Cancer. 2003;88:1077–83.
Al-Joudi FS, Iskandar ZA, Hasnan J, et al. Expression of survivin and its clinicopathological correlations in invasive ductal carcinoma of the breast. Singap Med J. 2007;48(7):607.
Jha K, Kumar M, Shukla VK, Pandey M. Survivin expression and correlation with clinico-pathological parameters in breast cancer. World J Pathol. 2012b;1:23–30.
Augello C, Caruso L, Maggioni M, et al. Inhibitors of apoptosis proteins (IAPs) expression and their prognostic significance in hepatocellular carcinoma. BMC Cancer. 2009;9:125.
Yie SM, Luo B, Ye NY, Xie K, Ye SR. Detection of Survivin-expressing circulating cancer cells in the peripheral blood of breast cancer patients by a RT-PCR ELISA. Clin Exp Metastasis. 2006;23:279–89.
Khan S, Aspe JR, Asumen MG, et al. Extracellular, cell-permeable survivin inhibits apoptosis while promoting proliferative and metastatic potential. Br J Cancer. 2009;100:1073–86.
Nigam J, Chandra A, Kazmi HR, et al. Expression of survivin mRNA in gallbladder cancer: a diagnostic and prognostic marker? Tumor Biol. 2014;35:9241–6.
Won HS, Lee MA, Chung ES, et al. Comparison of thymidine phosphorylase expression and prognostic factors in gallbladder and bile duct cancer. BMC Cancer. 2010;10:564.
Yim JH, Yoon JH, Kim SA, et al. Expression of X-linked inhibitor of apoptosis protein in neoplastic thyroid disorder. J Korean Med Sci. 2011;26:1191–5. https://doi.org/10.3346/jkms.2011.26.9.1191.
Mehrotra S, Languino LR, Raskett CM, Mercurio AM, Dohi T, Altieri DC. IAP regulation of metastasis. Cancer Cell. 2010;17:53–64. https://doi.org/10.1016/j.ccr.2009.11.021.
Chen X, Wang T, Yang D, et al. Expression of the IAP protein family acts cooperatively to predict prognosis in human bladder cancer patients. Oncol Lett. 2013;5:1278–84.
Rodríguez-Berriguete G, Fraile B, de Bethencourt FR, et al. Role of IAPs in prostate cancer progression: immunohistochemical study in normal and pathological (benign hyperplastic, prostatic intraepithelial neoplasia and cancer) human prostate. BMC Cancer. 2010;10:18. https://doi.org/10.1186/1471-2407-10-18.
Acknowledgements
Departmental research grant for financial support.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Dixit, R., Raza, M., Kumar, M. et al. Expression Analysis of Survivin and XIAP in Gallbladder Cancer: a Case-control Study in Indo-Gangetic Plain. J Gastrointest Canc 49, 487–492 (2018). https://doi.org/10.1007/s12029-017-0008-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12029-017-0008-9