
Abstract
Spreading depolarizations (SDs) are profound disruptions of cellular homeostasis that slowly propagate through gray matter and present an extraordinary metabolic challenge to brain tissue. Recent work has shown that SDs occur commonly in human patients in the neurointensive care setting and have established a compelling case for their importance in the pathophysiology of acute brain injury. The International Conference on Spreading Depolarizations (iCSD) held in Boca Raton, Florida, in September of 2018 included a discussion session focused on the question of “Which SDs are deleterious to brain tissue?” iCSD is attended by investigators studying various animal species including invertebrates, in vivo and in vitro preparations, diseases of acute brain injury and migraine, computational modeling, and clinical brain injury, among other topics. The discussion included general agreement on many key issues, but also revealed divergent views on some topics that are relevant to the design of clinical interventions targeting SDs. A draft summary of viewpoints offered was then written by a multidisciplinary writing group of iCSD members, based on a transcript of the session. Feedback of all discussants was then formally collated, reviewed and incorporated into the final document. It is hoped that this report will stimulate collection of data that are needed to develop a more nuanced understanding of SD in different pathophysiological states, as the field continues to move toward effective clinical interventions.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
First described in the 1940s, spreading depolarizations (SDs) are profound disruptions of homeostasis that slowly propagate through gray matter and induce suppression of cortical activity (termed “spreading depression”). For decades after their first description, SDs were generally regarded as a research curiosity and often were exploited merely as a laboratory tool to study brain function. However, work of an international research consortium (Co-Operative Studies on Brain Injury Depolarizations, COSBID.org) has conclusively shown that SDs occur commonly in human patients and established a compelling case for their importance in the pathophysiology of acute brain injury. Since the first COSBID meeting in 2003, its members have generally focused on recording SDs in the setting of neurocritical care, and testing the idea that SDs contribute to injury. Over the last 15 years, the SD field, including both clinical and preclinical research, has grown quite dramatically, largely due to the translational success of this work and growing recognition of the potential therapeutic importance of SDs in stroke, traumatic brain injury, and other disorders. As the field has grown, the annual COSBID meeting has evolved into the International Conference on Spreading Depolarizations (iCSD), an open meeting which welcomes and discusses a broad range of perspectives that bear on SD mechanisms and consequences. iCSD is attended by investigators studying various animal species including invertebrates, in vivo and in vitro preparations, diseases of acute brain injury and migraine, computational modeling, and clinical brain injury, among other topics. This article is a report of a formal discussion session at the second iCSD meeting, held at Boca Raton, Florida, September 22–24, 2018, with participants from 14 countries (http://www.cosbid.org/wp-content/uploads/2018/10/iCSD2018-program_FINAL.pdf). The goal of the session was to discuss the question of “Which SDs are deleterious to brain tissue?” and gain a sense of what factors may render some SDs more injurious than others. This is not intended to be a consensus statement, nor is it intended to provide a comprehensive review of the relevant literature. In contrast, the transcript from the session was used as a framework to capture the main opinions that were expressed. It is hoped that this report may be useful to stimulate collection of data that are needed to resolve key issues, as we continue to develop a more nuanced understanding of SD in different pathophysiological states.
Harmful Effects of SD
Multiple discussants emphasized that there is strong data, accumulated over decades, showing that SDs can be harmful to brain. Recent reviews were referenced, summarizing the case that SDs can cause the development and expansion of ischemic lesions, including both animal and clinical studies co-authored by some of the attendees. Multiple mechanisms have been described to explain damage caused by SD in this context, and it was noted that consistent supporting data can be found across the spectrum of studies from reduced preparations (brain slices) and animal models through to clinical recordings. The progression of deterioration is stepwise with SDs in animals and patients and can be attributed to the SD itself, rather than other physiologic variables. Much of the causative evidence is derived from monitoring several variables simultaneously. These data show that pathologic changes in major tissue variables, such as reduced cerebral blood flow or intracellular Ca2+ loading, develop in a spreading manner as a consequence of SD. The major mechanisms by which SDs are thought to cause cellular injury include ATP depletion, excitotoxicity, and spreading ischemia. Spreading ischemia is an SD-induced, local decrease in cerebral blood flow that is observed in both animals and patients and prolongs the electrophysiologic, depolarized state. It was pointed out these sequences have been demonstrated in many patients, and it was argued that deleterious effects of SD in causing tissue death have been nearly proven clinically.
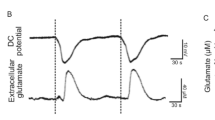
Additional comments supporting these points focused on the energy challenge presented by SD. SD is an unusual phenomenon, in that membrane potential is almost completely dissipated for tens of seconds to minutes and the energy required to repolarize is extreme. In addition to the massive amount of energy used to reestablish ionic gradients after SD, there are dramatic structural changes that must also be reversed. These changes include cellular swelling, fragmentation of endoplasmic reticulum, disruption of dendritic spines and other distortions have been well described during SD. Despite this challenge, mature neurons in healthy brain are able to recover relatively quickly and regain function, at least from SDs occurring in isolation. Yet on-line microdialysis recordings from patients, obtained with either rapid-sampling or continuous on-line microdialysis, SD results in sharp decreases in local brain glucose levels. Since this was observed regardless of the initial health of the tissue, it was interpreted that SD invariably moves the brain toward a more metabolically compromised state. While there are some tissue metabolic reserves (e.g., astrocytic glycogen) that mitigate the risk of complete failure, repetitive SDs are expected to progressively drive glucose to detrimental levels. From this perspective, it was argued that SDs are always detrimental to tissue, at least from a metabolic standpoint. Temporal clusters of SDs were considered particularly harmful, as metabolic reserves cannot be re-established between each event.
A note of caution was raised that, in some circumstances, evidence for the relationship between SD and injury progression is strictly correlative rather than causative. A further caution was that the experimental manipulations (e.g., potassium application) that investigators use to induce SD might be sufficient to increase infarct volumes, without additional detrimental effects of the SDs themselves. This can lead to erroneous conclusions about the effects of SDs. In support of this view, a paper presented at this meeting found that SDs induced by optogenetic stimulation, which presumably has no impact by itself, had no effect on infarct volumes. Thus, the role of the stimulus should be carefully controlled and considered in conducting and interpreting experimental SD studies.
Continuum of susceptibility to damaging effects of SD
The discussion moved quickly to the question of “what determines the conditions under which SDs are harmful?” Much progress has been made on this point, both in the laboratory and in clinic. The idea of a continuum of vulnerability to SD, depending on the baseline metabolic capacity of tissue (e.g., due to distance from focal lesion, or global differences in perfusion between patients), has been articulated in recent reviews. Animal studies have provided detailed information about the regional heterogeneity of tissue surrounding a focal injury, and it was emphasized that stark differences in consequence can be seen even over quite small distances, such as locations relative to the nearest arteriole. The clinical implications of this general point were illustrated with two case reports describing very different outcomes associated with SD. In the first, a middle-aged man had more than 100 SDs over the initial days after surgical removal of a hematoma, yet had an excellent outcome with no deficits. In contrast, another patient deteriorated dramatically after only 4–5 SDs, with a transition of the electrocorticogram (ECoG) from healthy to flat during the SD cluster. Discussion focused on the differences in perfusion and characteristics of the SDs in the two different cases. In the first case, good perfusion was maintained throughout the recording period, and SDs were of short duration, conditions that together meant that metabolite resupply could keep up with the challenge of the scores of events. In contrast, much longer-lasting SDs were seen in the context of damage in the second case. Prolonged SD events are observed if blood flow is substantially decreased, and tissue dies when they are prolonged for extended periods (e.g., ~ 20 min).
SDs that occur during migraine were discussed as a related example of non-damaging SDs. SD is thought to underlie the propagation of visual aura, and, unlike brain injury, events are initiated by intense activation of a region of healthy visual cortex rather than by focal ischemia or trauma. Discussants noted that despite a lifetime of repetitive SDs, there is no reported long-term deficit to visual cortex or its function. The acute visual disturbances during SD (scintillation due to the advancing SD wave front, and scotoma due to the brief suppression of cortical activity in the wake of SD) can be resolved in this tissue that is otherwise healthy prior to SD onset. The comparison with seizures was also raised as a good way of thinking about the continuum of SDs effects. Although the acute effects of seizures are magnitudes smaller than SDs, they can also have disparate effects on tissue metabolism and fate, depending on the state of the tissue involved. Related discussion focused on the need to build on prior published work examining the close relationship between seizures and SD, and the conditions under which one may trigger the other.
There was agreement that the character of an SD changes depending on where it occurs in the brain, and multiple discussants emphasized the severe technical limitation in the ability to detect where SDs originate and propagate. Current clinical recording methods rely on use of a single 1 × 6 subdural electrode strip which covers ~ 5 cm of brain. This extensive spatial sampling was considered a major advantage since it allows SD recordings, in an ideal case, from an injury focus into more normal brain. SDs with long durations characteristic of an evolving lesion are often recorded. However, it was pointed out that recordings of SDs with only short durations do not necessarily indicate that the SDs are less injurious, but only that they are less injurious at the recording sites. In injured brain (e.g., in stroke or trauma), it could be assumed that SD usually has damaging effects where it is initiated in vulnerable ischemic or penumbral regions, which may or may not be captured in the recordings, depending on the location of the electrode strip. One opinion therefore is that detection of any SD suggests that there is likely SD-induced damage occurring in vulnerable regions near the developing lesion focus, even if it has a short duration at recording sites. This viewpoint has important implications for the design of clinical intervention strategies, but needs to be fully reconciled with the prior comment that some patients can have scores of SDs and still have excellent outcomes.
A case example reported at the iCSD meeting illustrated the dilemma of different SD effects depending on brain location. The recordings of this patient demonstrated dramatically different SD durations, and different sensitivity to pharmacological inhibition, at two different recording locations. There was consensus that it would be helpful to have methods to observe SDs over larger regions, especially surrounding focal brain injuries, and the question was raised as to which other types of monitoring might be most helpful. Examples considered included clinical monitoring of inflammatory status, use of multiple subdural ECoG strips, scalp electroencephalogram, depth electrodes, and markers of metabolic status. Brain imaging methods, including regional blood flow assessments, were also considered as useful clinical adjuncts to continuous focal monitoring. The size of a region of ischemia is likely important in determining the functional impact of injury-induced SDs. Follow-up discussion on this point is included in the companion report (“What should a clinician do when spreading depolarizations are observed in a patient?”), as it focused on the sensitivity of clinical outcome measures.
Potential Beneficial Effects of SD
As noted above, there is a rich history of preclinical SD research spanning the decades from the original discovery of SD in rabbits in the 1940s. This work includes brain slices, small animal models, and a wide array of biochemical, electrophysiological, and imaging methods. While a great number of these studies are motivated by an interest in detrimental effects of SD, the literature also includes diverse reports of other SD effects, including some that may confer benefit. Examples noted during the session included synaptic strengthening induced by SD, increases in neurotrophic factors, neuroprotective preconditioning, and neurogenesis. One study presented at this meeting suggested that SDs limit expansion of intracerebral hemorrhage in the mouse. The strong hyperemic response to SD that can be observed in healthy tissues could also have positive effects, perhaps relevant to tissues outside vulnerable penumbral zones. It may not be surprising that an event as extreme as SD can modify quite a range of processes in complex brain tissue, but the discussion addressed the issue of whether some of these actions of SD are beneficial in the context of a brain-injured patient. This theoretical possibility is sometimes raised as a caution when considering therapeutic interventions to block SD in injured brain. Multiple discussants emphasized that it is very reasonable for a phenomenon like SD to have either beneficial or detrimental effects, depending on the tissue circumstances. The process of inflammation was cited as a relevant analogy, where in some cases inflammatory processes can be essential for disease mitigation, but in others can contribute to cellular injury. Likewise, hyperthermia was noted as an evolutionarily conserved process that provides benefit by fighting infection, yet is aggressively counteracted therapeutically in the intensive care unit because of the clear detrimental effects in that particular context.
Theoretical considerations aside, there was debate in the group about the existence of actual data supporting the beneficial effects of SD in the context of focal injury. At the present time, there appears to be little or no direct evidence that SD has meaningful beneficial effects in patients, in contrast to the strong accumulated evidence for contribution to injury. Furthermore, it was noted that any evidence for benefit would have to be dramatic to outweigh the potential therapeutic gains of treating and preventing SDs. Some discussants argued that this conclusion could be very biased by the fact that our field has focused mainly on the injury aspects of SD. Thus, we have to acknowledge the issue of selection bias in all of our discussions. It was further noted that we may be biased by the use of invasive clinical monitoring that targets the most injurious SDs near a lesion focus in the context of severe injury. The suggestion was made that without the ability to detect SD non-invasively, we may be missing a great deal, including events that are non-injurious and yet have other important effects, perhaps in non-damaged brain regions or in patients with less severe injuries. Again it was emphasized that non-invasive methods to study SD in non-injured animals and human subjects would help advance this discussion beyond provocative conjecture.
In response, a challenge was laid out for our field to rigorously test the hypothesis that there are meaningful effects of SD that improve outcome from injury, since this hypothesis has not been directly tested in animal models. For example, the notion that SD enables adaptive neuroplasticity that facilitates functional recovery could be tested by mapping reorganization of neuronal receptive fields in somatosensory cortex after focal ischemia, with versus without suppression of acute SDs by N-Methyl-D-aspartic acid receptor antagonists. The effect of SD to induce neurogenesis could also be examined in the context of injury, rather than only in healthy control animals. Similarly, it was suggested that preconditioning effects should be examined in relation to SDs that occur post-injury, to determine whether they mitigate against damage from a subsequent ischemic insult, such as occurs with delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage. Such studies should include measures of behavioral outcome to examine functional benefit to recovering animals.
Broader Biological Implications
There was robust and contentious discussion on the question of whether SDs are an evolutionarily conserved mechanism. This was inspired, in part, from reports at iCSD meetings about SDs in invertebrate animals. In locusts, SDs occur in the central nervous system after water immersion and induce a functional block that improves animal survival. These interesting observations are being extended with behavioral studies in Drosophila (fruit fly). A similar result in mammals was presented at this meeting, showing that earlier onset of SD after cardiac arrest in the rat is associated with better neurological outcome. In a purely speculative discussion, potential beneficial effects of SD were then considered from a human evolutionary perspective. It was suggested that, in the context of brain injury, adverse effects of SD could increase a group’s survivability by further incapacitating a weakened, injured member (i.e., analogous to “thinning the herd”). An alternate suggestion was that SD could provide an adaptive advantage following a traumatic brain injury by causing a quiet (rather than seizing) state of physical incapacitation (i.e. loss of consciousness), thus reducing the risk of detection by predators, if there is widespread, rapid depolarization. Others objected that there is no evidence of such widespread depolarization onset and that SD travels just as slowly in the large gyrencephalic human brain as it does in locust ganglia. It was further cautioned that the field should not fall victim to Stephen Jay Gould’s “Panglossian paradigm,” the assumption that every feature or process in biology was selected or ideally adapted for a specific purpose. Rather, susceptibility to SD may be an unavoidable consequence of the close packing of neurons and, rather than conferring any evolutionary advantage, may be an inherent vulnerability of nervous systems of sufficient complexity and organization. However, these ideas are challenged by the fact that some nervous tissue, such as nuclei of the lower brain and mammalian autonomic ganglia, are resistant to SD despite neuronal packing density similar to SD-vulnerable tissue. Discussion of these broader biological implications of SD has expanded at recent iCSD meetings, and a review manuscript is currently being prepared.
Conclusions
There was general agreement that some or many SDs are harmful, particularly under tissue conditions of metabolic compromise, and some took the view that all SDs should be considered detrimental in the context of acute brain injury. On the other hand, it was generally accepted that SDs can be benign in certain contexts such as healthy brain or migraine aura, and some have emphasized the possibility even of beneficial effects. The distinction between benign and beneficial emerged as an important one, since the presence of benign effects for some SDs or some brain regions would not contraindicate interventional therapies to block harmful SDs. Beneficial or protective effects of SD, on the other hand, might raise serious caution against such approach. This consideration suggested the need for studies that directly address the hypothesis of beneficial effects in the context of brain injury, which to date have not been conducted. The need to define endpoints that would demonstrate benefit was emphasized. Given the importance of energy depletion in rendering SDs more deleterious, it was also suggested that future therapeutic efforts should consider improving tissue perfusion, rather than solely focusing on SD blockade. Such approaches would be particularly attractive if SD has beneficial effects or if treatments to block SDs carry worrisome side effects. Finally, there was consensus that more studies are needed on the initial persistent SD after global insults, such as anoxic SD after cardiac arrest. Not only is cardiac arrest underrepresented in this field, but such studies would allow more direct comparison to insect studies and hence a better understanding of SD from an evolutionary perspective. Not the least, Leão’s original studies compared SD in normal brain and after global ischemia, and his results continue to serve as a benchmark for our understanding today.
Acknowledgements
We thank the Neurocritical Care Society and also thank the iCSD meeting sponsors: Moberg ICU Solutions, Raumedic, Hemedex, Integra, Natus, Nihon Kohden, Philips, Ad-Tech, Neurovisio, Perimed, Moor Instruments, PMT Corporation, Glia Media, and UC Gardner Neuroscience Institute. We thank Chanju D Fritch for assistance with documenting and preparing a transcript of the session. Authors’ work on this topic was supported by grants from NIH (NS106901, P20GM109089 (CWS); K23NS105950, U54NS100064 (ER); EB024793, CTSA Pilot Grant (subaward of UL1 TR001414), TR000147 (YA); NS102978 and NS104742 (KCB); K08NS091499 (NH), NS092181 (SCJ); T32 HL007736 (KMR); NS083858 (SAK); The Welcome Trust (MGB); Medical Research Council, UK (SJ); No. GINOP-2.3.2-15-2016-00048 (EF); DFG DR 323/5-1, DFG DR 323/10-1, FP7 no 602150 CENTER-TBI (JPD); Department of Defense: W81XWH-BAA-15-1, W81XWH-18-DMRDP-PTCRA, Moberg ICU Solutions subcontract, Office of the Assistant Secretary of Defense for Health Affairs, through the Defense Medical Research and Development Program under Award No. W81XWH-16-2-0020 (JAH); Discovery Grants from NSERC Canada (MR, RDA) and the Stroke Foundation of Canada (RDA). Claude D. Pepper Older Americans Independence Center (CBM). Opinions, interpretations, conclusions, and recommendations are solely those of the authors and are not necessarily endorsed by the Department of Defense or the National Institutes of Health.
Author information
Authors and Affiliations
Contributions
All authors contributed to the discussion session at the 2018 iCSD meeting that formed the basis of the manuscript. C.W.S. drafted the manuscript based on a transcript from the discussion session. All authors provided feedback and revisions that were incorporated into the final document.
Corresponding author
Ethics declarations
Conflict of interest
Dr. Henninger serves on the advisory board of Omniox, Inc. and serves as consultant to Astrocyte Pharmaceuticals, Inc.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Proceedings from the International Conference on Spreading Depolarizations 2018.
Rights and permissions
About this article

Cite this article
Shuttleworth, C.W., Andrew, R., Akbari, Y. et al. Which Spreading Depolarizations Are Deleterious To Brain Tissue?. Neurocrit Care 32, 317–322 (2020). https://doi.org/10.1007/s12028-019-00776-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-019-00776-7