
Abstract
Background
Mechanical ventilation is frequently performed in patients with ischemic stroke (IS), intracerebral hemorrhage (ICH), and subarachnoid hemorrhage (SAH). In this study, we used statewide administrative claims data to examine the rates of use, associated conditions, and in-hospital mortality rates for mechanically ventilated stroke patients.
Methods
We used statewide administrative claims data from three states and ICD-9-CM codes to identify patients admitted with stroke and those who received mechanical ventilation and tracheostomy. Descriptive statistics and exact 95 % confidence intervals were used to report rates of mechanical ventilation, tracheostomy, and in-hospital mortality. Logistic regression analysis was performed to identify conditions associated with mechanical ventilation based on previously described risk factors.
Results
798,255 hospital admissions for stroke were identified. 12.5 % of these patients underwent mechanical ventilation. This rate varied by stroke type: 7.9 % for IS, 29.9 % for ICH, and 38.5 % for SAH. Increased age was associated with a decreased risk of receiving mechanical ventilation (RR per decade, 0.91). Of stroke patients who underwent mechanical ventilation, 16.3 % received a tracheostomy. Mechanical ventilation was more likely to occur in association with status epilepticus (RR, 5.1), pneumonia (RR, 4.9), sepsis (RR, 3.6), and hydrocephalus (RR, 3.3). In-hospital mortality rate for mechanically ventilated stroke patients was 52.7 % (46.8 % for IS, 61.0 % for ICH, and 54.6 % for SAH).
Conclusions
In this large population-based sample, over half of mechanically ventilated stroke patients died in the hospital despite the fact that younger patients were more likely to receive mechanical ventilation. Future studies are indicated to elucidate mechanical ventilation strategies to optimize long-term outcomes after severe stroke.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Ischemic stroke, Intracerebral hemorrhage, and Subarachnoid hemorrhage often cause respiratory failure from injury to vital structures responsible for respiration, arousal, and airway protection. Although mechanical ventilation is frequently initiated as a life-saving intervention, little is known about the rates of use of this intervention and its association with mortality at a population level. Prior studies have been largely limited to single-center series and have reported conflicting findings. In one relatively small population-based study, Mayer et al. reported mechanical ventilation rates of 5 % in IS, 26 % in ICH, and 47 % in SAH [1]. The same study found that two-thirds of these mechanically ventilated patients died during their hospitalization. Another study of mechanically ventilated ICH patients reported a 90 % in-hospital mortality rate [2]. Other studies have reported significantly better outcomes such as 50 % survival at 3 years for mechanically ventilated ICH patients and good functional outcome in 20 % of patients after mechanical ventilation for IS [3–5]. Given the variability in single-center studies and the limited population-based data on mechanical ventilation after stroke, we used statewide administrative claims data to examine the rates of use and associated in-hospital mortality rates of this intervention.
Methods
Design
The rates of use and in-hospital mortality rates of mechanical ventilation in patients with stroke (IS, ICH, or SAH) were examined using statewide administrative claims data collected by the states of California, Florida, and New York. These data comprise discharge data for all patient visits at non-federal acute care emergency departments and acute care hospitals. These data are electronically reported to the respective state health agencies and then are checked for inconsistent or invalid elements and codes. The data are then provided in a de-identified format to the Healthcare Cost and Utilization Project of the Agency for Healthcare Research and Quality [6]. Data with an anonymous patient identifier allowing for longitudinal tracking across visits were available from 2005 to 2011 for California, 2005–2012 for Florida, and 2006–2011 for New York.
Patient Population
Previously validated International Classification of Diseases, 9th Edition, Clinical Modification (ICD-9-CM) codes were used to identify patients discharged with a first-recorded diagnosis of IS (433.x1, 434.x1, and 436), ICH (431), or SAH (430) [7]. After excluding potentially concomitant codes for traumatic causes of brain injury, admissions for rehabilitation care, and late complications of cerebrovascular disease, these codes were found to be both sensitive and specific for identifying patients admitted with IS (sensitivity: 86 % specificity: 95 %), ICH (sensitivity: 82 % specificity: 93 %), and SAH (sensitivity: 98 % specificity: 92 %). To focus on incident cases of stroke, we included only the first stroke admission for each patient during the study period.
Measurements
We used ICD-9-CM procedure codes that have been previously validated as 86 % sensitive and 98 % specific to ascertain mechanical ventilation (96.70–96.72) [8]. Since the accuracy of the ICD-9-CM code for tracheostomy (31.1–31.2) has not been previously validated, we performed a retrospective chart review at our institution to determine its sensitivity and specificity. This was done by identifying 25 hospitalizations for stroke (IS, ICH, or SAH) and a concomitant diagnosis code for tracheostomy (31.1–31.2) as well as 25 stroke hospitalizations with no concomitant tracheostomy code. A neurology board-certified neurocritical care fellow (SL) performed retrospective chart review of these encounters, while blinded to the ICD-9-CM codes, to identify whether tracheostomy had been performed during each hospitalization.
Statistical Analysis
The rates of use of mechanical ventilation and tracheostomy and the mortality rates for patients undergoing mechanical ventilation were assessed using standard descriptive statistics with exact 95 % confidence intervals (CI). We used the χ2 test to compare proportions and means with standard deviations (SD) to compare continuous variables. Factors associated with mechanical ventilation were examined using a modified form of logistic regression that accounts for the fact that our outcomes were not rare [9]. These models included previously reported risk factors for mechanical ventilation: demographic characteristics (i.e., age, gender, race etc.), stroke type (i.e., IS, ICH, or SAH), markers of illness severity (sepsis, cerebral edema, hypoxemia, status epilepticus, seizures, pneumonia), and the Elixhauser comorbidity index [10–13].
Results
Validation of ICD-9-CM codes 31.1–31.2 by chart review of 50 patient encounters indicated a sensitivity of 100 % and specificity of 96 % for tracheostomy.
There were 798,255 hospital admissions for IS, ICH, or SAH. Overall, 99,782 (12.5 %; 95 % CI 12.4–12.6 %) of these patients underwent mechanical ventilation. This rate varied by stroke type: 7.9 % (95 % CI 7.8–7.9 %) for IS, 29.9 % (95 % CI 29.6–30.1 %) for ICH, and 38.5 % (95 % CI 38.1–39.0 %) for SAH. Demographic characteristics, stroke type, and associated illness severity markers stratified by mechanical ventilation occurrence are summarized in Table 1.
Compared to those with IS, mechanical ventilation was more likely in those with ICH [relative risk (RR), 3.6; 95 % CI 3.56–3.65] or SAH (RR, 3.9; 95 % CI 3.8–4.0). Increased age was associated with decreased risk of mechanical ventilation (RR per decade, 0.91; 95 % CI 0.91–0.92). Several markers of illness severity were associated with higher risk of mechanical ventilation: status epilepticus (RR, 5.1; 95 % CI 4.8–5.4), pneumonia (RR, 4.9; 95 % CI 4.8–5.1), sepsis (RR, 3.6; 95 % CI 3.5–3.6), and hydrocephalus (RR, 3.3; 95 % CI 3.3–3.4). Demographic characteristics and associated illness severity markers stratified by stroke type are summarized in Table 2.
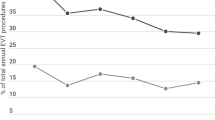
Of those stroke patients who received mechanical ventilation, 16.3 % (95 % CI 16.0–16.5 %) underwent tracheostomy. Tracheostomy rates were similar among stroke subtypes: 16.6 % (95 % CI 16.3–17.0 %) among IS patients, 15.5 % (95 % CI 15.1–15.9 %) among ICH patients, and 16.6 % (95 % CI 16.1–17.2 %) among SAH patients.
Of those stroke patients who received mechanical ventilation, 11.8 % (95 % CI 11.5–12.1 %) were discharged home (IS: 11.0 %, ICH 10.2 %, SAH 17.6 %). In contrast, 37.3 % (95 % CI 37.2–37.4 %) of patients with stroke who did not undergo mechanical ventilation were discharged home (IS: 37.4 %, ICH 30.7 %, SAH 55.9 %). Of all patients with stroke who underwent tracheostomy, 4.3 % (95 % CI 3.9–4.6 %) were discharged home (IS: 4.3 %, ICH: 3.8 %, SAH 5.2 %), while 36.2 % (95 % CI 36.1–36.3 %) of all patients with stroke who survived after receiving mechanical ventilation but did not undergo tracheostomy were discharged home (IS: 36.5 %, ICH 28.7 %, SAH: 50.4 %).
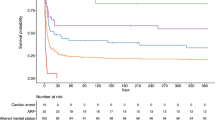
The in-hospital mortality rate for mechanically ventilated stroke patients was 52.7 % (95 % CI 52.4–53.0 %). Mortality rates among mechanically ventilated patients varied by stroke type: 46.8 % (95 % CI 46.3–47.2 %) for IS, 61.0 % (95 % CI 60.5–61.5 %) for ICH, and 54.6 % (95 % CI 53.8–55.3 %) for SAH. In contrast, the mortality rate for stroke patients who did not receive mechanical ventilation was 5.8 % (95 % CI 5.7–5.8 %) overall, 4.7 % (95 % CI 4.7–4.8 %) for IS, 12.7 % (95 % CI 12.5–13.0 %) for ICH, and 9.1 % (95 % CI 8.7–9.5 %) for SAH (Fig 1). Overall, in-hospital mortality was 8.6 (95 % CI 8.5–8.7) times more likely in mechanically ventilated stroke patients compared to those not mechanically ventilated. Compared to those undergoing mechanical ventilation for IS, mechanically ventilated ICH and SAH patients were 2.7 (95 % CI 2.66–2.75) and 2.5 (95 % CI 2.5–2.6) times more likely to die in the hospital.

In-hospital mortality rates stratified by mechanical ventilation status and stroke subtype
Conclusion
In this large population-based sample, 12.5 % of stroke patients underwent mechanical ventilation. Over half of these patients died despite the fact that younger patients were more likely to receive mechanical ventilation. Approximately one out of six mechanically ventilated stroke patients received a tracheostomy.
Although the in-hospital mortality rates in this study seem remarkably high among patients undergoing mechanical ventilation, they are lower than those reported in Mayer et al’s population-based study from the year 2000. It is unclear whether these lower mortality rates reflect differences in patient population, changes in approaches to end-of-life care, advances in critical care, or other factors. Consistent with prior studies, patients with ICH and SAH were more likely to receive mechanical ventilation and more likely to die in the hospital (regardless of mechanical ventilation status) compared to patients with IS. These findings further support the notion that overall, patients with IS have a better short-term prognosis compared to ICH and SAH [1, 14, 15]. Of note, even though the in-hospital mortality rates for patients with SAH were high, these patients were more likely to be discharged home compared to those with IS or ICH regardless of whether they received mechanical ventilation. There are several possible explanations for this divergent finding that is dissimilar from Mayer et al’s findings that reported 88 % in-hospital mortality rate for mechanically ventilated patients with SAH [1]. One possible explanation is that mechanical ventilation improves outcomes by facilitating current therapeutics for patients with SAH, for example, by enabling aneurysm securement and aggressive volume resuscitation. Another explanation is that the events leading up to mechanical ventilation in patients with SAH, such as acute hydrocephalus may be reversible compared to physiological processes that underlie IS and ICH. Despite the variability in outcome, rates of tracheostomy for ICH and SAH patients were similar to IS patients. This similarity may suggest that other unmeasured variables such as the expectations of the patient or their surrogates may significantly contribute to the decision to undergo tracheostomy.
Strengths of this study include a large and diverse sample of patients from three states that represent approximately 25 % of the US population, thus enabling population-based inferences of care utilization and practice trends. There are important limitations of this study that should be considered. Although the ICD-9-CM codes used in this study were validated with high accuracy, the lack of clinical details such as stroke severity, cause of death, and long-term functional outcomes limits understanding of the relationships between the variables that were studied. For instance, it is unclear whether mechanical ventilation was a marker of severity of illness or whether it independently contributed to the observed high mortality rates (for example by causing hypotension during endotracheal intubation or by necessitating sedation that clouds the neurological examination). Additionally, the lack of long-term functional outcomes data limits understanding of the true effectiveness of the intervention among survivors. The specific circumstances for initiating mechanical ventilation may have also influenced the measured outcomes. For example, a greater proportion of patients with SAH may have been intubated to facilitate medical and surgical management whereas this is less likely in IS and ICH patients. Similarly, the threshold for initiating mechanical ventilation may vary depending on the individual patient’s characteristics such as age and medical comorbidities. Finally, since the exact mechanisms of death are unknown, it is unclear to what extent withdrawal of care (persuaded by a “self-fulfilling prophecy”) or medical complications of stroke contributed to the mortality rates.
In conclusion, this study suggests a substantial rate of in-hospital mortality among mechanical ventilated stroke patients. Given the frequent utilization of this intervention in stroke, and the substantial-associated mortality, future studies are indicated to elucidate mechanical ventilation strategies to optimize long-term outcomes after severe stroke.
References
Mayer SA, Copeland D, Bernardini GL, et al. Cost and outcome of mechanical ventilation for life-threatening stroke. Stroke. 2000;31(10):2346–53.
El-Ad B, Bornstein NM, Fuchs P, Korczyn AD. Mechanical ventilation in stroke patients—is it worthwhile? Neurology. 1996;47(3):657–9.
Roch A, Michelet P, Jullien AC, et al. Long-term outcome in intensive care unit survivors after mechanical ventilation for intracerebral hemorrhage. Crit Care Med. 2003;31(11):2651–6.
Grotta J, Pasteur W, Khwaja G, et al. Elective intubation for neurologic deterioration after stroke. Neurology. 1995;45(4):640–4.
Santoli F, De Jonghe B, Hayon J, et al. Mechanical ventilation in patients with acute ischemic stroke: survival and outcome at one year. Intensive Care Med. 2001;27(7):1141–6.
Agency for Healthcare Research and Quality. HCUP methods series: methodological issues when studying readmissions and revisits using hospital administrative data. http://www.hcup-us.ahrq.gov/reports/methods/2011_01.pdf. Accessed 4 July 2014.
Tirschwell David L, Longstreth WT Jr. Validating administrative data in stroke research. Stroke. 2002;33:2465–70.
De Coster C, Li B, Quan H. Comparison and validity of procedures coded With ICD-9-CM and ICD-10-CA/CCI. Med Care. 2008;46(6):627–34.
Zhang J, Yu KF. What’s the relative risk? A method of correcting the odds ratio in cohort studies of common outcomes. JAMA. 1998;280(19):1690–1.
Wijdicks EF, Scott JP. Causes and outcome of mechanical ventilation in patients with hemispheric ischemic stroke. Mayo Clin Proc. 1997;72(3):210–3.
Gujjar AR, Deibert E, Manno EM, et al. Mechanical ventilation for ischemic stroke and intracerebral hemorrhage: indications, timing, and outcome. Neurology. 1998;51(2):447–51.
Zhu H, Hill MD. Stroke: the Elixhauser Index for comorbidity adjustment of in-hospital case fatality. Neurology. 2008;71(4):283–7. doi:10.1212/01.wnl.0000318278.41347.94.
Berrouschot J, Rössler A, Köster J, et al. Mechanical ventilation in patients with hemispheric ischemic stroke. Crit Care Med. 2000;28(8):2956–61.
Burtin P, Bollaert PE, Feldmann L, et al. Prognosis of stroke patients undergoing mechanical ventilation. Intensive Care Med. 1994;20(1):32–6.
Jorgensen HS, Nakayama H, Raaschou HO, Skyhoj T. Intracerebral hemorrhage versus infarction: stroke severity, risk factors, and prognosis. Ann Neurol. 1995;38:45–50.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Lahiri, S., Mayer, S.A., Fink, M.E. et al. Mechanical Ventilation for Acute Stroke: A Multi-state Population-Based Study. Neurocrit Care 23, 28–32 (2015). https://doi.org/10.1007/s12028-014-0082-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-014-0082-9