
Abstract
Page kidney is a condition where external compression of the renal artery and renal parenchyma leads to subsequent ischaemia and activation of renin-angiotensin-aldosterone axis. A 42-year-old female with hirsutism, hypertension and diabetes was diagnosed with a right adrenal mass and underwent laparoscopic adrenalectomy. Her hypertension worsened postoperatively and was managed medically. Subsequently she developed a right flank pain on the fifth postoperative day and died suddenly the next day. Autopsy revealed a pale body with cushingoid appearance. Surgical scars were healthy. Internal examination of the abdomen revealed a haemoperitoneum of 500 ml together with a large subcapsular haematoma measuring 1000 ml surrounding the right kidney, compressing the right renal artery. Kidneys were pale and the right kidney was soft and friable. Cortical surface of the right kidney demonstrated a possible surgical puncture site with an overlying thrombus together with a contused inferior vena cava. Other organs were pale but appeared otherwise normal. Histology revealed diffuse cortical necrosis of right kidney and features of adult respiratory distress syndrome in the lungs. Haemorrhagic shock following laparoscopic adrenalectomy for right adrenal tumor was declared as the cause of death, contributed by the development of the Page kidney. Trauma of several aetiologies including laparoscopic abdominal surgery may contribute to Page kidney. It presents with flank pain, hypertension and renal mass. Since postoperative blood loss usually manifests as hypotension, resulting hypertension may mislead the attending clinicians. Once diagnosed, it can be managed with surgical drainage and antihypertensives.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Page kidney or Page phenomenon is a condition that results from external compression of the kidney. It is rare and associated with new-onset hypertension and recent history of blunt trauma to the kidney [1]. It was first demonstrated by Page in 1939 in animal models by wrapping the kidneys with cellophane to induce perinephritis and removal of the offending kidney resolved the condition [2]. In 1955, Page and Engel described a calcified renal sub-capsular hematoma in a 19-year-old football player causing hypertension which was cured by nephrectomy [3]. Since then, there have been multiple reports of similar cases where the etiology is shifting from accidental trauma to surgical procedures [1, 4, 5].
External compression of the renal artery and renal parenchyma with subsequent ischemia and activation of the renin-angiotensin-aldosterone axis is implicated in its pathogenesis [4, 6]. This external compression is caused by the accumulation of blood in the perinephric area. Hypertension or its complications, flank pain and renal mass are the main features of presentation [6]. Computed tomography (CT), renal ultrasound (US) scanning or magnetic resonance imaging (MRI) can be used to diagnose this condition [5]. It is treated symptomatically with Angiotensin Converting Enzyme (ACE) inhibitors and by surgical drainage. It is a rare condition and deaths associated with this condition are not recorded in literature.
Case history
A 42-year-old diabetic female with a history of left hemithyroidectomy was investigated for hypertension and hirsutism. Contrast-enhanced CT scan showed a right adrenal mass and evidence of chronic renal parenchymal disease. She underwent laparoscopic right adrenalectomy for the surgical resection of the adrenal mass. From admission to the post-surgical period, her systolic blood pressure was fluctuating from 130 mm Hg to a maximum value of 170 mm Hg.
During the post-surgical period, she was periodically tachycardic. There was no marked reduction in the hemoglobin value and she was managed with analgesics, antibiotics and routine diabetic medications. Up to the second post-operative day, her blood pressure was on the lower side and as a result, the antihypertensive treatment was withheld. These medications were restarted on the third day since her blood pressure rose again to pre-operative levels. Her hemoglobin, blood urea/electrolytes and serum creatinine levels were monitored until the second post-operative day and were within the normal ranges. She had been managed during both the pre-operative and post-operative periods in the medical ward since she was initially admitted to the medical ward.
She was recovering from the surgery in the medical ward with no major complications until she complained of right flank pain on the fifth post-operative day. It was managed as a possible renal colic and an x-ray kidney ureter bladder (KUB) was planned for the next day. At that time, her blood pressure and hemoglobin level were not monitored, despite persistent tachycardia. She suddenly deteriorated and died on the sixth post-operative day despite attempts of resuscitation.
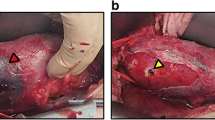
At the autopsy, an external examination revealed cushingoid features including facial hirsutism, central obesity and dorso-cervical fat pad with thin limbs. Surgical scars of the recent surgery were healthy and there was no evidence of neglect. Internal examination of the abdomen revealed a hemoperitoneum of 500 ml with a large sub-capsular hematoma measuring 1000 ml surrounding the right kidney. The hematoma was compressing the right renal artery (Fig. 1a). Both kidneys were pale while the right kidney was soft and friable. Its cortical surface demonstrated a possible surgical puncture site with an overlying thrombus (Fig. 1b) and cortex and medulla were pale with loss of cortico-medullary demarcation. The pelvicalyceal system appeared normal while the right renal artery and its branches were intact. The inferior vena cava was contused at the level of drainage of the right renal vein and appeared unhealthy (Fig. 2) indicating the features of compression by the hematoma. The rest of the abdominal organs together with pelvic organs and thoracic organs were also pale due to the hemorrhage. The brain appeared macroscopically normal. The right lobe of the thyroid gland was also enlarged, probably following the previous hemi-thyroidectomy, and contained multiple nodules.

Compression of the right renal artery (bold arrow) by the hematoma (a) and surgical puncture site (thin arrow) on cortical surface of right kidney with an overlying thrombus (b)

Contused inferior vena cava (arrow) at the level of drainage of right renal vein
Histology of the organs revealed cerebral edema, perivenular congestion with extensive macro-vesicular steatosis of the liver and adult respiratory distress syndrome in the hyper-inflated lungs, indicating a multi-organ involvement following hemorrhage. In the kidney in question, there was histopathological evidence of diffuse cortical necrosis (Fig. 3). Histopathological examination of the left kidney was unremarkable. Hemorrhagic shock following laparoscopic adrenalectomy for the right adrenal tumor was declared as the cause of death, contributed by the development of the Page kidney.

Diffuse cortical necrosis in the right kidney, H&E x50 (a), x100 (b)
Discussion
Page kidney is a rare treatable cause of hypertension. The trauma of several etiologies, ranging from sports-related trauma, road traffic accidents, intentional violence, renal transplant, biopsy and other abdominal surgery may contribute to Page kidney [4,5,6,7,8]. Typically, the patient presents with flank pain, a sudden drop in hemoglobin with new-onset or worsening of existing hypertension. In many previous cases, the condition was presented after a significant time following the causative trauma [3,4,5, 8]. A review of case reports on Page kidney has revealed the presence of an average blood pressure of 177/95 mm Hg at the time of diagnosis in such situations [4]. In this case, the subject presented with flank pain, however assumed to be due to a renal calculus and it was only several days after the infliction of surgical trauma, unlike most cases reported previously. Continuous monitoring of basic parameters was not undertaken in this case, missing the possibility of diagnosing Page kidney.
Page kidney is readily identified by using radiology, via CT, US or MRI, and the availability of high-quality modern imaging modalities has been attributed as a cause of identifying a shift in etiology of Page kidney [4, 5, 9]. In this case, the treating team aimed at investigating a renal calculus and the aforementioned imaging studies were not carried out, which would have led to the diagnosis of the condition.
In the literature, the treatment options for Page kidney include drainage of the sub-capsular hematoma either by laparoscopy or open surgery [9]. Page described bilateral adrenalectomy as a successful treatment modality [1]. This patient was medically managed with antihypertensives, which affect the renin-angiotensin-aldosterone axis. In this case, although the patient was already on antihypertensive medications, her blood pressure monitoring was not carried out with the onset of flank pain, which is a significant mismanagement.
In this case, remote trauma to the kidney would have been caused by the intra-abdominal surgery, adrenalectomy and her hypertension is playing a role as well. A high level of suspicion regarding the condition and early use of imaging modalities would have prevented the complications. A death contributed by Page kidney is as rare as the disease itself and never recorded in the medical literature. In this case, in determination of the cause of death, medically and legally, the autopsy findings play a major role. Multi-organ involvement following hemorrhage needs to be carefully looked for at the autopsy. Furthermore, any lapse in patient care could be identified by scrutinizing the patient’s in-ward records.
In a patient who had undergone nephrectomy for Page kidney following trauma two years ago, the histopathological examination of the specimen showed that the renal parenchyma was replaced by necrotic fibrocollagenous eosinophilic material with compressed glomeruli and tubules [8]. In the current case, histopathology of the offending kidney revealed diffuse cortical necrosis. Since there had been no histopathology reports of deaths or acute cases due to Page kidney in the literature, this histopathological finding can be assumed to be a feature of this condition.
An adequate and timely post-operative monitoring of pain, bleeding and blood pressure was lacking. In this case, the patient was hypertensive post-operatively as opposed to the usual picture of hemorrhagic post-operative patient with hypotension. This might have been a reason why that internal hemorrhage was not suspected in this patient. Also, the relevant surgical team who has the expertise in such complications was not appropriately involved in the management and ideally, this patient should have been managed at a post-operative surgical unit. Although rare, complications such as Page kidney should be considered in the post-operative management of similar cases.
Failure to provide adequate post-operative care would result in death or major consequences in an otherwise treatable case. During the death investigation, it should be noted whether the standard protocols and best practices were adhered to, in post-operative care. In a rare case like this, it would be worthwhile to note whether all the relevant stakeholders in clinical decision-making were involved, at the appropriate setting or not. In a medico-legal context, an allegation of medical negligence would arise in this case in relation to the misdiagnosis and the lapses in post-operative care. In such a case, the forensic practitioner’s role would consist of conducting thorough postmortem examinations, analyzing medical records and providing expert opinions on causation and the standard of care.
In Sri Lanka where this case was reported, when medical negligence is suspected, patients or their families can lodge complaints with the statutory body for health care providers or pursue civil legal cases to seek compensation. The Sri Lanka Medical Council has the authority to investigate complaints related to professional misconduct or negligence by medical practitioners registered under their authority and take disciplinary actions ranging from warnings, suspension or erasure from the register [10].
Lessons learned from communications such as this case report serve as a reminder of the importance of vigilance in suspecting and identifying rare but potentially fatal cases such as Page kidney. Furthermore, this case highlights the possibility of medical negligence arising due to lapses in pre-operative evaluation and post-operative care.
References
Haydar A, Bakri RS, Prime M, Goldsmith DJ. Page kidney–a review of the literature. J Nephrol. 2003;16(3):329–33.
Page IH. The production of persistent arterial hypertension by cellophane perinephritis. JAMA. 1939;113(23):2046–48. https://doi.org/10.1001/jama.1939.02800480032008.
Engel WJ, Page IH. Hypertension due to renal compression resulting from subcapsular hematoma. J Urol. 1955;73(5):735–39. https://doi.org/10.1016/S0022-5347(17)67466-4.
Dopson SJ, Jayakumar S, Velez JCQ. Page kidney as a rare cause of hypertension: case report and review of the literature. Am J Kidney Dis. 2009;54(2):334–39.
McCune TR, Stone WJ, Breyer JA. Page kidney: case report and review of the literature. Am J Kidney Dis. 1991;18(5):593–99.
Chung J, Caumartin Y, Warren J, Luke PPW. Acute Page kidney following renal allograft biopsy: a complication requiring early recognition and treatment. Am J Transplant. 2008;8(6):1323–28. https://doi.org/10.1111/j.1600-6143.2008.02215.x.
Smyth A, Collins CS, Thorsteinsdottir B, Madsen BE, Oliveira GHM, Kane G, et al. Page kidney: etiology, renal function outcomes and risk for future hypertension. J Clin Hypertens. 2012;14(4):216–21.
Sokhal AK, Prakash G, Saini DK, Singh K, Sankhwar S, Singh BP. Page kidney: a rare but surgically treatable cause of hypertension. Saudi J Kidney Dis Transplantation. 2018;29(1):193. https://doi.org/10.4103/1319-2442.225183.
McFadden JD, Hawksworth JS. Page kidney: an unusual complication of a renal transplant biopsy. Case Rep Urol. 2018. https://doi.org/10.1155/2018/8768549.
Sri Lanka Medical Council. (2009) Instructions on serious professional misconduct to medical practitioners and dentists. https://slmc.gov.lk/images/PDF_Main_Site/serious%20professional%20misconduct2021-12.pdf.
Acknowledgements
None.
Funding
The authors did not receive support from any organization for the submitted work.
Author information
Authors and Affiliations
Contributions
All authors contributed to the conception and design of the work; the acquisition, analysis, and interpretation of data work; drafting the work and reviewing it critically for important intellectual content. All authors approved the final of the version to be published.
Corresponding author
Ethics declarations
Competing interests
The authors have no relevant financial or non-financial interests to disclose.
Ethical statement
The presented autopsy case was conducted for medico-legal purposes and the findings are available in public domain. However, we used this information for academic purposes, including teaching and publication, according to the institutional guidelines with informed written consent of the next of kin and without divulging the identity of the individual.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Kumarasinghe, G., Sivasubramanium, M., Ekanayake, K.B. et al. A fatal misdiagnosis of page kidney – case report. Forensic Sci Med Pathol (2024). https://doi.org/10.1007/s12024-024-00807-6
Accepted:
Published:
DOI: https://doi.org/10.1007/s12024-024-00807-6