
Abstract
These two case reports are of fatal injuries from less-lethal weapons (tear gas guns) using pebbles as an unconventional ammunition. Reported here are the fatal outcomes of two 19-year-old males, one with head trauma and the other with abdominal trauma. They were admitted to the ED and subjected to immediate exploratory operations, but they passed away. On autopsy, the first case demonstrated a right frontal bone fracture with subdural hemorrhage and a 3 × 2.5 cm pebble retained in the skull. The second case showed severe liver laceration in close vicinity to a cubical pebble (3.2 × 3 cm). The mechanical forces involved in skull fracture and autopsy are discussed. In the current cases, the relatively larger weight and size together with the surface configuration of the pebble projectile were the main influential factors that contributed to the severity of damage and fatality.These case reports are a working example of the effect of the mass of projectiles in increasing the power of penetration. The direct shooting to the head and the abdomen together with the misuse of these weapons are capable of inflicting fatal injuries.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
A typical firearm projectile is blasted off due to a certain amount of kinetic energy. This kinetic energy is generated from burning gunpowder [1]. Less-than-lethal weapons such as tear gas and rubber bullet guns are made for police/law enforcement forces for benign control of crowds and dispersing riots by shooting tear gas or rubber bullets [2]. It is a conventional single-shot, break-open weapon, with a floating firing pin mechanism that ensures safety when accidentally dropped [3, 4]. A new brand called Airsoft gas grenade launcher was recently reported [5].
The tear gas weapon is a non-lethal weapon, usually a 37-mm riot gun or a 12-gauge shotgun. Therefore, it has a caliber that provides a safe distance from riots with an effectiveness that can control crowds up to 150 m [6].
Non-lethal weapons are designed to cause pain and minimize the incidence of injury or death [3]. Non-lethal bullets are designed to be fired at the lower body; they can be lethal if fired directly at the head and/or at close range [1, 7]. Different parts of the body show varying degrees of vulnerability, with a high risk to areas such as the eye, head (cranial, maxillofacial), neck (airway or neurovascular structures), and chest (lung and cardiac) [8].
The manufacturers who claim the relative safety of such weapons are usually dependent on their proper use. However, individuals may purchase and fire themwithout following proper instructions or training. Improper use would amount to excessive force resulting in severe damage and death [7,8,9]. Riot-related injuries in the past 3 years were mainly caused by stones, rocks, and tear gas canisters [10, 11].
Few reports in the literature describe the mechanical effects of tear gas guns in the development of traumatic brain injuries (TBI). Most penetrating brain injuries result from road traffic accidents, firearm injuries in suicidal attempts, or assault attacks. Globally, TBI is a leading cause of health problems and disability. The yearly incidence of TBI is variously estimated to range from 27 to 69 million worldwide. Several survivors sustained permanent and significant impairments [12]. As regards abdominal injuries, mortality occurs in 10–13% of all injured patients with gunshots representing the third leading cause of death [13, 14]. Abdominal gunshot wounds are responsible for more than 90% of deaths among young adults aged 15 to 24 years old [13].
Our case reports are unique because of the use of pebbles as an unconventional projectile in a less-lethal weapon resulting in fatality.
Ethics
The data used in this retrospective report are in accordance with ethical standards. The ethics approval for this study was 0306110 on May 15, 2023, by the Ethics Committee of the Faculty of Medicine – Alexandria University (IRB NO: 00012098—FWA NO: 00018699).
Case 1
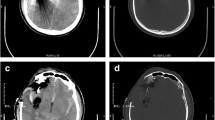
A 19-year-old male patient was brought to the ED with a gunshot in his right cerebral hemisphere. His vital signs were as follows: a heart rate of 112 beats/min, blood pressure of 135/80 mm Hg, and respiratory rate of 20 breaths/min. GCS was 8 and pupils were dilated and fixed. According to the ambulance report, the patient was brought to the hospital 2–3 h after the accident. He was hemodynamically stable and intubated. CT scan of the brain showed an oval, well-circumscribed, hyper-dense mass in the right frontal and temporal regions near the midline representing a retained foreign body inside the skull that caused brain edema and intraventricular hemorrhage (Fig. 1).

Initial CT scan of the brain showing an oval well-circumscribed hyper-dense foreign body mass settled inside in the right frontal and temporal regions near the midline, causing brain edema and intraventricular hemorrhage
The patient was moved to the surgical theatre, and a trial to remove that mass was performed through the lateral aspect of the skull. There was a small partial loss of the right frontal bone (Fig. 2). An initial attempt to control epidural and subdural bleeding was made by neurosurgeons at the hospital. At this point, the anesthesiologist reported that the patient’s systolic blood pressure had dropped to 70/40 mm Hg, so the neurosurgeon had to temporarily end the operation leaving the foreign body in its place. The patient was transferred to theICU, waiting for the patient’s vital signs to stabilize and to evaluate the possibility of further surgical interference. However, the patient died after 2 days and the body was transferred for autopsy. In the mortuary, dissection guided by CT was carried out. There was a loss of part of the right frontal bone (Fig. 2) associated with multiple skull fractures, and the inlet size was 4 × 3 cm on the right side of the frontal bone. The oblong pebble 3 × 3.5 cm was found embedded within the brain tissues with no blast chamber tunnel.

Injury in right frontal bone—surgical stitches to the left of the injury
The cause of death was documented as ballistic injury (brain laceration and hemorrhage due to pebble entry) (Fig. 3).

Brain laceration and epidural and subdural hemorrhages on dissection
The police arrested the perpetrator and delivered the weapon to the forensic district for evaluation, which confirmed its use in the incident (Fig. 4).

The used weapon and a pebble dislodged from the barrel, kept in a plastic container
Case 2
A 19-year-old male arrived at the hospital after an injury to his abdomen. There was a lacerated wound in the RUQ with severe bleeding. His vital signs were blood pressure of 160/80 mm Hg, a heart rate of 60 beats/min, and a GCS of 6. He was administered 1L ringer lactate; Cefazolin 1–2 gm IV/IM. No imaging was done. Urgent exploratory laparotomy was performed to deal with projectile-related intra-abdominal injuries. Unfortunately, the patient died on the table. He was referred to the mortuary for an autopsy. The surgical dissection on the right side of the abdominal wall enlarged the entrance wound on the skin, so the original dimensions could not be measured (Fig. 5). There was a laceration of the liver (Fig. 6) and intestines. On the left side of the omentum, there was a cubical pebble 3.2 × 3 cm with a slightly pointed angle on one side (Fig. 7).

Exploration of the abdomen of the victim on autopsy

Liver laceration on dissection

The pebble that caused the abdominal injury
The cause of death was documented as ballistic injury (hemorrhagic shock with liver laceration due to pebbles entry).
The police arrested the perpetrator and delivered the weapon to the forensic district for evaluation, which again confirmed its use in the incident (Fig. 4).
Weapon and pebble examination
The typical pebble is a blunt projectile. It measures 3 cm × 3.5 cm and weighs 50–70 g. It is discharged from the smooth-bore non-rifled 37/38 mm gas gun which is a specially modified riot-control gun with a low muzzle velocity (Fig. 4). The tear gas launcher technical specifications were as follows: diameter 38 mm ± 1 mm, size (length) 125 mm ± 2 mm, weight148g ± 5 g, total chemical weight 65 g ± 3 g, delay time 2 ~ 3 s, burn time 20 ± 5 s, range over 100 m, charge cs mixture (cs amount and concentration are able to be adjusted), projectile material aluminum, and shelf life 5 years. The pebble here is used in place of a tear gas container and travels along the gun’s long axis to strike the target on the end.
Discussion
Less-lethal guns such as tear gas guns and rubber bullet guns are designed to incapacitate targets without killing them but they are dangerous and may inflict serious injuries. We present herein two cases of using pebbles as an unconventional projectile in a non-lethal weapon, which is considered an uncommon cause of fatal injuries. A professional forensic pathologist would encounter several challenges in the analysis and interpretation of such deaths. This is because using pebbles as low-velocity projectiles is quite uncommon and its mechanism of action and outcome needs special consideration [15].
The blast effect of a tear-gas weapon is composed of three components: the propellant, the wadding, and the chemical agent in the form of fine powder [16]. The gas jet alone generated by the tear-gas cartridge possesses the characteristics of a missile and is capable of producing considerable acceleration of foreign bodies inserted in the front part of the barrel like pebbles [17].
The use of unconventional ammunition/projectiles is a main point to be considered in both presented cases. The operator used tear gas cartridges or other projectiles to generate energy and propel the pebbles through the muzzle as a missile. It was reported that stones or pebbles were used in the past, prior to the introduction of lead shots [18]. However, the actual flight path and terminal impact performance were and are still unpredictable due to the imperfect round shape.
No exit wound was found in either case; thus, all the kinetic energy possessed by the projectile was dispersed within the tissues and this might explain the severity of the injuries encountered.
There are a multitude of variables that can impact the injury severity and pattern, including the nature of projectile material, form, muzzle velocity, the flight path of projectiles, the firing distance, and the region of impact on the body [8]. Moreover, the fitness and type of tissue hit help determine the attained damages [19].
The degree of damage inflicted by any weapon is related to the amount of kinetic energy transferred to the target at the time of impact which is proportional to the mass and velocity of the projectile based on the equation: KE = 1⁄2 mv2 (where KE is kinetic energy, m is mass, and v is velocity) [20].
In the presented cases, the pebbles acted as a gunshot causing penetrating trauma. This produced bleeding and brain laceration in the first case and multisystem organ damage and hemorrhage in the second case. In both cases, the pebbles were retained inside the body, damaging the bone, blood vessels, and internal organs.
Despite the head being a target of fatal assaults, direct head-penetrating trauma is not necessarily immediately fatal. Bhootra and Bhana (2004) reported that all fatalities occurred within 1–3 days of injury [21]. This coincided with our first case.
An Iraqi study done by Hoz et al. (2020) also found that several cases of head trauma caused by tear gas canisters through frontal, parietal, and occipital bones did not die immediately [11].
Penetrating trauma is a common outcome of abdominal gunshot wounds and accounts for up to 90% of the mortality linked to penetrating abdominal injuries [22, 23]. The injuries most commonly involve the viscera and sometimes the abdominal aorta [8, 14, 23].
Traumatic evisceration had been reported in a case due to the penetration of two stone fragments; however, in that case, the victim survived [23]. Borovsky et al. (2017) found that projectiles shot from unconventional weapons such as a sling have serious traumatic potential and can cause blunt trauma such as fractures of the trunk, limb, and facial skull bone, depending on the weight and shape of the projectile and the distance from the source of danger. Asymmetrically shaped projectiles weighing more than 100 g were the most dangerous. Projectiles weighing more than 100 g can cause bone fractures of the trunk and limbs at distances of up to 60 m from the target and may cause serious head injuries to an unprotected person (Abbreviated Injury Scale 4–5) at distances up to 200 m from the target [19]. Guérant et al. (2018) described a case where a man was killed by rubber bullet weapons (a single-shot handgun with mini Gomm Cogne ammunition: 12 rubber spherical pellets, 7.4 mm in diameter). The findings were consistent with an intra-buccal shot and an ingestion-inhalation of blood and projectiles [24].
Conclusions
Regarding the two cases we are summarizing, pebbles were used as unconventional ammunition in a non-rifled 37-mm less-lethal weapon (tear gas gun). The findings showed concordance with those caused by the discharge of a single projectile with a low-velocity weapon. The case reports were a working example of the effect of the mass of projectiles in increasing the power of penetration. The direct shooting to the head and the abdomen together with the misuse of these weapons are capable of inflicting fatal injuries.
Limitations of the study
The current study is not without limitations. First, the exact wound mechanics are not clearly understood, particularly the projectile firing range and angle. Second, despite numerous reports accounting for direct tear gas-related fatalities, we were not able to find previous investigations of a missile of similar description. Finally, the pebbles showed variation in shape; therefore, mathematical modeling of the flight path is presumed to be unpredictable.
Key points
-
1.
A pebble was used as ammunition in a less-lethal weapon instead of the designed ammunition/projectile.
-
2.
Direct shots to the head and the abdomen using less-lethal weapons turned out to be fatal.
Data availability
The datasets analyzed during the current study are not publicly available due to data privacy, but it can be available on reasonable request.
References
DiMaio VJM. Gunshot wounds: practical aspects of firearms, ballistics and forensic techniques. 2nd ed. Boca Raton, FL: CRC Press; 1999.
Jussila J. Future police operations and non-lethal weapons. Med Confl Surviv. 2001;17:248–59.
Tumbarska A. Non-lethal weapons”–a concept difficult to define. Security Future. 2017;1(4):138–41. https://stumejournals.com/journals/confsec/2017/4/138.
Voiglio EJ, Fanton L, Caillot JL, Neidhardt JP, Malicier D. Suicide with “non-lethal” firearm. Lancet. 1998;352:882.
Airsoft grenade launcher: launch bb showers & rubber slugs. Available from: https://www.redwolfairsoft.com/guns/airsoft-grenade-launchers. Accessed 14 Apr 2023.
Milkor 37/38mm and 40mm Stopper. Available from: https://en.wikipedia.org/wiki/Milkor_37/38mm_and_40mm_Stopper. Accessed Apr 2023.
Alhillo HT, Arnaout MM, Radhi HS, Al-Dhahir MA , Moscote-Salazar LR , Hoz SS. Direct head injury caused by a tear gas cartridge. Questions on safety: a case report from Iraq and review of the literature. J clin neurosci. 2018;56:179–82.
Haar RJ, Iacopino V, Ranadive N, Dandu M, Weiser S. Death, injury, and disability from kinetic impact projectiles in crowd-control settings: a systematic review. BMJ Open. 2017;7: e018154. https://doi.org/10.1136/bmjopen-2017-018154.
Clarot F, Vaz E, Papin F, Clin B, Vicomte C, Proust B. Lethal head injury due to tear-gas cartridge gunshots. Forensic Sci Int. 2003;137:45–51. https://doi.org/10.1016/s0379-0738(03)00282-2.
El Zahran T, Mostafa H, Hamade H, Mneimneh Z, Kazzi Z, El Sayed MI. Riot-related injuries managed at a hospital in Beirut. Lebanon Am J Emerg Med. 2021;42:55–9.
Hoz SS, Aljuboori ZS, Dolachee AA, Al-Sharshahi ZF, Alrawi MA, Al-Smaysim AM. Fatal penetrating head injuries caused by projectile tear gas canisters. World Neurosurg. 2020;138:e119–23. https://doi.org/10.1016/j.wneu.2020.02.050. Epub 2020 Feb 17 PMID: 32081822.
Dewan MC, Rattani A, Gupta S, Baticulon RE, Hung YC, Punchak M, Agrawal A, Adeleye AO, Shrime MG, Rubiano AM, Rosenfeld JV, Park KB. Estimating the global incidence of traumatic brain injury. J Neurosurg. 2018;130(4):1080–97. https://doi.org/10.3171/2017.10.JNS17352. PMID: 29701556.
Forbes J, Burns B. Abdominal gunshot wounds [internet]. stat pearls Available from: StatPearls Publishing, Treasure Island. 2020. https://www.ncbi.nlm.nih.gov/books/NBK564335/.
Morris DS, Sugrue WJ. Abdominal injuries in the war wounded of Afghanistan: a report from the International Committee of the Red Cross Hospital in Kabul. Br J Surg. 1991;78(11):1301–4. https://doi.org/10.1002/bjs.1800781108. PMID: 1760686.
Wan Y, Griffiths S, Ganau M. Neurosurgical care of nonpowder firearm injuries: a narrative review of the literature. Emerg Med Int. 2019;2019:4680184. https://doi.org/10.1155/2019/4680184.PMID:31827929;PMCID:PMC6886332.
Rothschild MA, Maxeiner H, Schneider V. Cases of death caused by gas or warning firearms. Med Law. 1994;13(5–6):511–8.
Artillery in the English Civil Wars. Available from: https://www.worldhistory.org/article/1931/artillery-in-the-english-civil-wars/2022. Accessed 13 Apr 2023.
http://news.bbc.co.uk/2/shared/spl/hi/middle_east/03/v3_ip_timeline/html/1987.stm.
Borovsky I, Lankovsky Z, Kalichman L, Belkin V. The traumatic potential of a projectile shot from a sling. Forensic Sci Int. 2017;272:10–5. https://doi.org/10.1016/j.forsciint.2016.10.006. Epub 2016 Oct 26 PMID: 28088089.
Simon G, Heckmann V, Tóth D, Kozma Z. Brain death of an infant caused by a penetrating air gun injury. Leg Med. 2019;39:41–4.
Bhootra BL, Bhana BD. an unusual missile-type head injury caused by a stone: case report and medicolegal perspectives. Am J Forensic Med Pathol. 2004;25(4):355–7. https://doi.org/10.1097/01.paf.0000146375.81986.ea.
Mejia A, Myers JG, Stewart RM, Dent DL, Root HD, Pruitt BA. Air gun injuries to the abdominal aorta: report of two cases and review of the literature. J Trauma. 2003;54(6):1235–8. https://doi.org/10.1097/01.TA.0000022464.15355.5C. PMID: 12813350.
García Reyes A, Alpizar Rivas Ó, Sánchez Ramírez M, Oliva Mompean F. Traumatic evisceration secondary to a stone as a projectile. Cir Esp (Engl Ed). 2021;99(7):536. https://doi.org/10.1016/j.cireng.2021.06.005. Epub 2021 Jun 23. PMID: 34172415.
Guérant M, Vaz MA, Peoc’h M, Gaillard Y, Boyer B. Suicidal shot in the mouth with rubber bullets. Leg Med (Tokyo). 2018;32:52–6. https://doi.org/10.1016/j.legalmed.2018.02.009. Epub 2018 Mar 2 PMID: 29523001.
Acknowledgements
Sincere thanks to Prof. Dr. Haidy Megahed, Professor of Forensic Medicine and Clinical Toxicology, Faculty of Medicine, Alexandria University for the editing effort.
Sincere thanks to Dr. Mennatallah Hassan Attia, Ass. Professor of Forensic Medicine and Clinical Toxicology, Faculty of Medicine, Alexandria University, for her help.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that there have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Zein-Elabdin, H., Ghanem, M.A. Two case reports of fatal injuries sustained from tear gas guns loaded with pebbles as missiles. Forensic Sci Med Pathol (2023). https://doi.org/10.1007/s12024-023-00756-6
Accepted:
Published:
DOI: https://doi.org/10.1007/s12024-023-00756-6