
Abstract
Purpose
In postmenopausal women under L-T4 therapy, which was subsequently accompanied by calcium carbonate (CC) supplementation taken 6–8 h after tablet L-T4, TSH levels were greater than prior to adding CC. Total cholesterolemia [CHOL], fasting glycemia [FG], systolic and diastolic blood pressure [SBP, DBP] were also greater than baseline. Our aim was to explore the effects of either liquid or softgel capsule L-T4, while maintaining CC ingestion 6–8 h, later on TSH levels, CHOL, FG, SBP, and DBP.
Methods
We proposed to 50 hypothyroid postmenopausal women under tablet L-T4 therapy, to switch to either liquid or softgel capsule L-T4 at the same daily dose while maintaining CC ingestion 6–8 h later. Sixteen women accepted [group I; liquid (n = 9), capsule (n = 7)], while 34 continued tablet L-T4 [group II, (n = 34)].
Results
After 3 months, in group I, TSH decreased significantly (1.23 ± 0.49 vs. 1.80 ± 0.37 mU/L, P < 0.01), as did FG (80.7 ± 7.9 vs. 83.4 ± 6.3 mg/dL, P < 0.05); CHOL, SBP, and DBP decreased, though insignificantly. In contrast, in group II, TSH, FG, CHOL, SBP increased insignificantly, and DBP increased borderline significantly (69.7 ± 9 vs. 66.3 ± 6.5, P < 0.10). Compared to baseline (before adding CC), in group I, TSH was significantly lower (P < 0.01) and the other indices similar; in group II, TSH, FG, and SBP were significantly higher (P < 0.05), DBP borderline significantly higher (P < 0.10) and CHOL insignificantly higher. Performance of liquid L-T4 and capsule L-T4 was similar.
Conclusion
Delaying CC ingestion even by 6–8 h after taking tablet L-T4 is not entirely satisfactory, unlike liquid or softgel L-T4.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
One type of medications that impair the intestinal absorption of L-T4, at least in its classic formulation (tablet) is represented by calcium salts [1,2,3,4,5,6]. Of calcium carbonate, citrate and acetate, unequivocal evidence of such malabsorption exists for calcium carbonate.
We had studied 50 postmenopausal hypothyroid women whose serum TSH levels were stable when tablet L-T4 had been taken alone [7]. However, when they added supplementation with calcium carbonate, which was taken 1–2 h after tablet L-T4 for 2.3 ± 1.1 years, TSH increased significantly (on average, from 1.93 to 3.33 mU/L [+73%]), with nine women not meeting anymore the ≤4.12 mU/L target levels of TSH recommended by guidelines [8]. Thus, we confirmed the sole study on a cohort of hypothyroid patients who take simultaneously tablet L-T4 and calcium [2]. In that study, which was conducted on a small number of patients and with a 3 months-exposure to calcium carbonate, the extent of TSH increase was congruent with our data [7]. In our cohort [7], when calcium carbonate was delayed by 6–8 h after tablet L-T4, fall of TSH was not entirely satisfactory because measured levels were greater than at baseline, prior to adding calcium. Also, a number of biochemical and clinical indices in the metabolic/cardiovascular domain are known to be sensitive to small changes in serum TSH even within its reference range [9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33] (for examples, see Table 1). Of these indices, we studied [7] total cholesterol (CHOL), fasting blood glucose (FG), systolic and diastolic blood pressure (SBP and DBP), and they decreased significantly when calcium was delayed by 6–8 h. However, all these four indices were greater than baseline, though not always significantly. As previously suggested, the detrimental effect of calcium carbonate is truly its binding to L-T4, operating at physiologic gastric pH only [2, 7, 34].
Because we have previously shown that novel formulations of L-T4 (oral liquid solution and softgel capsule) are virtually refractory to the impaired absorption of L-T4 caused by medications [1, 4, 35,36,37], we wished to ascertain whether full normalization of TSH and of the said indices (SBP, DBP, CHOL, and FG) could be achieved by switching the patients to either liquid L-T4 or capsule L-T4, as per their preference, upon maintaining the same daily dose and interval (6–8 h) from subsequent calcium carbonate ingestion.
Materials and methods
Patients
The cohort of 50 patients as well as the criteria to define abnormal CHOL, FG, SBP, and DBP, was described in detail previously [7]. Hypercholesterolemia is CHOL level ≥200 mg/dL, hyperglycemia is FG ≥100 mg/dL or being on drug treatment for elevated glucose, hypertension is elevated systolic blood pressure (SBP) ≥130 mm Hg or elevated diastolic blood pressure (DBP) ≥85 mm Hg, or being on antihypertensive drug treatment in a patient with a history of hypertension [7].
In brief, from the database of the Osteoporosis Outpatients Center of our University Hospital, we selected these 50 women (age 71.7 ± 5.1 years [median] 71) because (i) they had primary hypothyroidism that was treated with tablet L-T4 (45–60 min prior to breakfast, at a daily dose of 1.43 ± 0.24 µg/Kg body weight [median = 1.47]), and had TSH stabilized at target levels ≤4.12 mU/L (1.93 ± 0.51 mU/L); (ii) they were subsequently supplemented with oral calcium carbonate ± vitamin D (without taking any other drug/supplement known to impair the intestinal absorption of L-T4), which was ingested 1–2 h after tablet L-T4. Calcium carbonate was taken at the daily dose of 600 or 1000 mg/d elemental calcium. When vitamin D had been given, it was taken at 800 IU/d [7]. L-T4 therapy had been taken for 4.4 ± 2.0 years before supplementation with calcium carbonate ± vitamin D was added. In turn, women received this supplementation for 2.3 ± 1.1 years, during which tablet L-T4 continued to be taken [7]. We found that 9/50 women (referred to a group A) had TSH levels >4.12 mU/L and that the remaining 41 women (referred to a group B) had serum TSH, significantly increased compared to prior of adding the calcium supplementation (2.98 ± 0.51 vs. 1.90 ± 0.40 mU/L, P < 0.01), though TSH was <4.12 mU/L [7]. As previously reported [7], our intervention was to extend the interval between L-T4 and calcium, so that calcium was taken in the afternoon, 6–8 h after tablet L-T4. Patients were seen again after three months, and pertinent data recorded.
As anticipated above in the Introduction, because TSH and the four TSH-sensitive indices (CHOL, FG, SBP, and DBP) were greater than the corresponding baseline levels (that is, before adding calcium ± vitamin D), we made a second intervention. We proposed all 50 women to switch L-T4 from the tablet to the preferred novel formulation (liquid solution or softgel capsule) while maintaining the same daily dose of L-T4, timing from breakfast and 6–8 h delay from subsequent ingestion of calcium carbonate. Sixteen women accepted such proposal (1/9 from group A and 15/41 from group B). Precisely, 9/16 women opted for the liquid solution and 7/16 for the softgel capsule. In the present study, the 16 women who opted for the switch are referred to as group I, while the remaining 34 are referred to as group II. After 3 months, serum TSH and the four indices were measured again in both group I and II. Informed consent was obtained from all individual participants included in the study.
Our hypothesis was that, compared to the corresponding values when L-T4 was taken as a tablet 6–8 h prior to calcium carbonate, values of TSH, CHOL, FG, SBP, and DBP (and frequency of hypercholesterolemia, hyperglycemia and hypertension) had to be lower in group I but similar in group II. A secondary interest was to see if there was any superiority of one novel formulation of L-T4 compared to the other.
Statistics
Data are presented as mean ± SD. Differences between means were analysed by ANOVA, except differences between TSH levels, which were analyzed by the Wilcoxon signed rank test because of their non-gaussian distribution. Differences between proportions were analysed by the two-tailed chi-square (χ2) test or Fisher’s exact, as appropriate. P values of <0.05 minimum were considered statistically significant, whereas P values comprised between 0.10 and 0.05 were considered as borderline significant.
Results
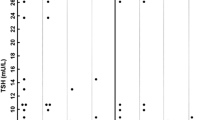
For the sake of completeness, results will be presented starting from baseline. The exact values in terms of mean ± SD (for data handled as continuous variables) and percentages (for data handled as categorical variables), and corresponding statistics are given in Tables 2, 3; Figs. 1, 2.

Changes in TSH and TSH-sensitive indices in hypothyroid women both L-T4-replaced and calcium carbonate-supplemented, who were switched from tablet L-T4 into a novel L-T4 formulation (liquid solution or softgel capsule)

Percent changes in categorical TSH and TSH-sensitive indices in hypothyroid women both L-T4
Postponing calcium by 6–8 h after tablet L-T4 vs. postponing calcium by 1–2 h or vs. baseline
In either group, delaying ingestion of calcium by 6–8 h after having taken tablet L-T4 affected in the favorable direction (that is, decrease) serum levels of TSH, CHOL, FG, and values of both SBP and DBP compared to delaying ingestion of calcium by 1–2 h (Table 2; Fig. 1). Taking into account that the size of group II (n = 34) was double than the size of group I (n = 16), in group II statistically significant were changes in TSH, CHOL, and DBP, and trendwise significant changes in SBP; in group I, statistically significant were changes in TSH, CHOL, and SBP. However, even though all parameters decreased, they were not exactly superimposable to the baseline values (Table 2). Indeed, in group II, TSH was significantly greater, and FG and DBP insignificantly greater than baseline; in group I, TSH, FG, and DBP were insignificantly greater than baseline (Table 2).
The changes illustrated as continuous variables in Table 2 are showed as categorical variables in Table 3. While there was a general decline in proportions associated with delaying ingestion of calcium by 6–8 h after having taken tablet L-T4 compared to delaying by 1–2 h, the former proportions were greater than those at baseline (L-T4 taken alone), with a statistical level of significance reached only in group II and for two indices (TSH and CHOL). In addition to proportion of FG ≥100mg/dL in group I, only the proportion of serum TSH >4.12 mU/L in either group matched the corresponding baseline proportions (Table 3). However, in two patients of group I the 100 mg/dL threshold was missed by 6 mg/dL, and in three patients of group II the 4.12 mU/L threshold was missed by just a few decimals (data not shown).
Follow-up (continuing to postpone calcium by 6–8 h after L-T4, but L-T4 taken as liquid or capsule in group I)
In group II, the proportion of serum TSH >4.12 mU/L continued to be zero, though it ranged 3.70–3.95 mU/L in 5/34 patients. In contrast, the highest post-switch TSH in group I was 2.50 mU/L [data not shown]. In group II, indices continued to increase either significantly (TSH, CHOL, FG, and SBP) or borderline significantly (DBP) (Table 2). In contrast, in group I, indices decreased (TSH and FG significantly, CHOL and SBP borderline significantly) or were unchanged (DBP) (Table 2). As shown in the footnote for Table 2, the percent changes of TSH and each index after switch (group I) or after continuing to take tablet L-T4 (group II) over the corresponding values at the preceding measurement (when both groups were taking tablet L-T4 6–8 h prior to calcium) were statistically different (TSH, SBP, DBP, or borderline significant (CHOL, FG) in group I compared to group II.
Table 3 and Fig. 2 illustrate changes in terms of categorical variables. In group I, the proportions of women with abnormality of SBP, DBP CHOL and FG decreased (the last three indices becoming 0%). In contrast, in group II, those proportions increased (significantly for SBP and FG, borderline significantly for DBP, and insignificantly for CHOL).
When comparison is with baseline, in group II increase in serum TSH, FG, and SBP was significantly greater, and increase in CHOL was trendwise significant (Table 2). In contrast, indices in group I were very similar (DBP, FG) or even lower (TSH significantly, and CHOL borderline significantly) compared to the corresponding baseline values (Table 2).
Figures 1 and 2 show that there was no clear superiority of one new formulation over the other.
Discussion
In postmenopausal hypothyroid women, we show that postponing ingestion of calcium carbonate to after lunch (6–8 h after table L-T4) is not entirely satisfactory for bringing serum TSH to levels equal to or lower than those measured prior to adding calcium carbonate supplementation to the L-T4 replacement therapy. However, the goal is achieved if tablet L-T4 is substituted by liquid or capsule L-T4.
We showed that TSH elevations resulting from calcium carbonate supplementation do affect certain TSH-sensitive peripheral indices [9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34] (see Introduction and Table 1). Some studies summarized in Table 1 are worthy of being discussed in more detail because containing data for TSH levels comparable to the extreme TSH levels (0.85–6.9 mU/L) that were measured in the 50 women from baseline through the last observation.
In 2205 Korean postmenopausal euthyroid women, the frequency of metabolic syndrome increased progressively across TSH quartiles [16]. CHOL, LDL-CHOL, triglycerides, and DBP were significantly associated with serum TSH levels. Multivariate logistic regression analysis determined that TSH levels strongly contributed to metabolic syndrome in 490 euthyroid type 2 diabetic subjects, women had higher mean serum TSH levels and lower FT4 concentration than diabetic men [17]. Stratifying the study population according to quartiles of TSH levels, subjects in the highest TSH quartile were more likely to be women, with higher values of BMI and waist circumference, higher triglycerides and non-HDL CHOL concentrations, and higher visceral adiposity index, when compared to those in the lowest quartile. Already across the first three TSH quartiles, there was a gradual increase in CHOL, triglycerides, in both SBP and DBP, and in frequency of use of metformin. A Korean study enrolled 17,061 euthyroid subjects without diabetes among participants who had undergone consecutive thyroid function tests between 2006 and 2012 as a part of yearly health check-up program [18]. TSH changes were determined by subtracting baseline TSH level from TSH level at 1 year before diagnosis of diabetes or at the end of follow-up in subjects who did not develope diabetes. The risk of incident type 2 diabetes was significantly increased with each 1.0 μIU/mL increment in TSH after adjustment for multiple confounding factors (hazard ratio = 1.13, 95% CI 1.07–1.20, P < 0.001). The authors concluded that increase in circulating TSH could be an additional risk factor for the development of type 2 diabetes in euthyroid subjects.
Noteworthy is also a study on 30,656 Norwegian individuals (18,182 women) without known thyroid disease [10]. Moving across the six TSH bands within the reference range of 0.5–3.5 mU/L, both in men and women there was a gradual increase in the geometric mean of serum CHOL, LDL-CHOL, and triglycerides. Subgroup analyses showed statistically significant associations for all lipids in men above 50 years of age and for triglycerides in all age groups. For women, associations were statistically significant in all age groups except for HDL-CHOL in women below 50 years of age. Unfortunately, exact data were not tabulated. The authors concluded that association with serum lipids (CHOL, LDL-CHOL, and triglycerides) was linear across the entire reference range of TSH, and that—within the range of TSH that is considered clinically normal—increasing levels of TSH are associated with less favorable lipid concentrations [10]. The same Norwegian group [28] reported that within the said reference range of TSH (0.50–3.5 mU/L), there was a linear increase in blood pressure with increasing TSH. The average increase in SBP was 2.0 mmHg per mU/L increase in TSH among men, and 1.8 mm Hg in women. The corresponding increase in DBP was 1.6 mm Hg in men and 1.1 mmHg in women. Comparing TSH of 3.0–3.5 mU/L (upper part of the reference range) with TSH of 0.50–0.99 mU/L (lower part of the reference range), the odds ratio for hypertension was 1.98 (95% CI 1.56–2.53) in men and 1.23 (95% CI 1.04–1.46) in women [28]. Another Norwegian population-based study 5872 subjects (3249 being women aged 56.5 ± 14.5 years) [29] found that within the normal serum TSH range (0.20–4.00 mIU/L), there was a significant and positive relation between serum TSH and both SBP and DBP. Particularly, serum TSH was a significant predictor for DBP in both genders and also for SBP in females. Moreover, after adjusting for age, body mass index and smoking status, SBP was 1.4 mm Hg and DBP 1.6 mm Hg higher in males in the highest TSH quartile vs. males in the lowest TSH quartile. The corresponding differences in females were 4.0 and 2.7 mm Hg, respectively. All these Norwegian data [10, 28, 29] agree with our data on the 50 postmenopausal women, including the 2.31 mmHg increase in SBP and 2.0 mmHg increase in DBP, for every 1.0 mU/L increase in serum TSH over the TSH range of 0.85 to 6.9 mU/L [7].
Also a Greek study on 311 euthyroid individuals (185 women, 126 men, mean age 43.9 ± 9 years) found an association of serum TSH levels falling in the reference range (0.36–4 mU/L) with both SBP and DBP [31]. In the subgroup with TSH levels 0.36–2.5 mU/L (n = 238), TSH levels positively and significantly correlated with SBP and DBP. Hypertensive patients had higher TSH levels and belonged more frequently to the subgroup with TSH >2.0 mU/L compared to the normotensive patients. A similar observation had been reported in a collaborative American and French study [30]. Finally, a Japanese study on 26 normotensive and euthyroid patients with serum creatinine <1.00 mg/dL found that serum TSH, including levels within the normal range, was positively correlated with vascular resistance at the afferent arteriole (Ra), but not at the efferent arteriole (Re) [32]. Serum TSH was significantly and negatively correlated with renal plasma flow, renal blood flow, and glomerular filtration rate (GFR). In multiple regression analysis, serum TSH was significantly positively associated with Ra after adjustment for age and mean blood pressure [32].
A Spanish study evaluated 3533 male participants of the Aragon Workers’ Health Study with normal TSH and FT4 levels, across quintiles of these variables [33]. Compared with the lowest TSH quintile, the risk of metabolic syndrome was greater at the higher quintiles. Interestingly, FG also increased with TSH primarily below the median TSH, DBP showed similar changes across the entire TSH range, whereas body mass index, triglycerides, and HDL-CHOL changed only at the highest normal TSH values. In a Brazilian population-based study on 10,935 participants (54.3% women), age, body mass index, waist measurement, FG and fasting and postload insulin and HOMA-IR increased according to TSH quintiles [13]. Subjects in the fifth TSH quintile presented an odds ratio of association with insulin resistance of 1.86 (95% CI 1.26–2.75), regardless of gender.
Limitations of our study are the retrospective nature and the type of patients being restricted to the elderly women (age 71.7 ± 5.1 years; median 71). On the other hand, the size of our study group (n = 50) is 2.5 times greater than the only cohort study, though prospective, on hypothyroid patients co-treated with both tablet L-T4 and calcium carbonate [2]. Strengths of our study are (i) to have highlighted the fact that drug-induced elevation of serum TSH, even within the reference range, is not innocuous, and (ii) to have complemented the tablet L-T4 data with data after switch from tablet L-T4 to either novel formulation of L-T4 in groups of similar size (liquid L-T4, n = 9; softgel capsule L-T4, n = 7). The post-switch amelioration of serum TSH and four TSH-sensitive indices, while maintaining calcium carbonate ingestion 6–8 h after having taken liquid or capsule L-T4, was such that 4/5 parameters turned out to be lower than the baseline values (i.e., when taking table L-T4 prior to adding calcium carbonate supplementation). These post-switch data are not surprising considering that, in previous studies on other patients, liquid L-T4 counteracted successfully elevations of serum TSH observed when tablet L-T4 was taken 1–4 h prior of ingesting calcium alone or calcium plus other drugs known to impair intestinal absorption of L-T4 [4, 36,37,38].
It appears reasonable to conclude that elevations of serum TSH, even in the upper part of the reference range, caused by malabsorption of L-T4 are not unconsequential. Also, persons under treatment with drugs known to impair intestinal absorption of L-T4 in whom hypothyroidism is diagnosed would be better off starting to be prescribed either liquid or softgel L-T4 [39]. Similarly, hypothyroid patients under tablet L-T4 therapy who introduce any of those drugs would be better off switching tablet L-T4 to either novel formulation of L-T4. The corollary of failure to use ab initio or to switch to novel formulations of L-T4 is the suggestion to monitor hypothyroid patients who also take drugs known to impair intestinal absorption of L-T4 with periodic measurements not only of serum TSH but also of TSH-sensitive indices associated with metabolic and cardiovascular outcomes.
Change history
28 June 2019
An amendment to this paper has been published and can be accessed via a link at the top of the paper.
References
C.R. Schneyer, Calcium carbonate and reduction of levothyroxine efficacy [letter]. JAMA 279, 750 (1998)
N. Singh, P.N. Singh, J.M. Hershman, Effect of calcium carbonate on the absorption of levothyroxine. JAMA 283, 2822–2825 (2000)
I. Zamfirescu, H.E. Carlson, Absorption of levothyroxine when coadministered with various calcium formulations. Thyroid 21, 483–486 (2011)
S. Benvenga, F. Di Bari, R. Vita, Undertreated hypothyroidism due to calcium or iron supplementation corrected by oral liquid levothyroxine. Endocrine 56, 138–145 (2017)
P. Colucci, C. Seng Yue, M. Ducharme, S. Benvenga, A review of the pharmacokinetics of levothyroxine for the treatment of hypothyroidism. Eur. Endocrinol. 9, 40–47 (2013)
S. Benvenga, When thyroid hormone replacement is ineffective? Curr. Opin. Endocrinol. Diabetes Obes. 20, 467–477 (2013)
E. Morini, A. Catalano, A. Lasco, N. Morabito, S. Benvenga, l-thyroxine malabsorption due to calcium carbonate impairs blood pressure, total cholesterolemia, and fasting glycemia. Endocrine (2018). https://doi.org/10.1007/s12020-018-1798-7
J.R. Garber, R.H. Cobin, H. Gharib et al. Clinical practice guidelines for hypothyroidism for hypothyroidism in adults: cosponsored by the American Association of Clinical Endocrinologists and the American Thyroid Association. Thyroid 22, 1200–1235 (2012)
I.L. Klein, S. Danzi, in Werner and Ingbar’s the Thyroid: a Fundamental and Clinical Text, ed. by L.E Bravermann, D.S Cooper (Wolters Kluver, Lippincott, Willimas & Wilkins, Philadelphia, 2013), p. 575–582
B.O. Asvold, L.J. Vatten, T.I. Nilsen, T. Bjøro, The association between TSH within the reference range and serum lipid concentrations in a population-based study. The HUNT Study. Eur. J. Endocrinol. 156, 181–186 (2007)
T.N. Le, F.S. Celi, E.P. Wickham 3rd, Thyrotropin levels are associated with cardiometabolic risk factors in euthyroid adolescents. Thyroid 26, 1441–1449 (2016)
B. Xu, H. Yang, Z. Wang, T. Yang, H. Guo, P. Cheng, W. He, M. Sun, H. Chen, Y. Duan, Elevated thyroid stimulating hormone levels are associated with metabolic syndrome in a Chinese community-based population of euthyroid people aged 40 years and older. J. Biomed. Res. 30, 476–482 (2016)
I.M. Benseñor, A.C. Goulart, C. Molina Mdel, É.J. de Miranda, I.S. Santos, P.A. Lotufo, Thyrotropin levels, insulin resistance, and metabolic syndrome: a cross-sectional analysis in the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). Metab. Syndr. Relat. Disord. 13, 362–369 (2015)
A. Javed, P.B. Balagopal, A. Vella, P.R. Fischer, F. Piccinini, C. Dalla Man, C. Cobelli, P.D. Giesler, J.M. Laugen, S. Kumar, Association between thyrotropin levels and insulin sensitivity in euthyroid obese adolescents. Thyroid 25, 478–484 (2015)
J. Alam, M.N.-E.-T.M. Mukti, M. Hoque, I. Ali, M. Kamal, S.C. Mallik, S. Choudhury, Cross sectional evaluation of thyroid hormone levels in non-diabetic and diabetic patients in Bangladeshi population. Asian J. Biol. Sci. 6, 228–233 (2013)
H.T. Park, G.J. Cho, K.H. Ahn, J.H. Shin, S.C. Hong, T. Kim, J.Y. Hur, Y.T. Kim, K.W. Lee, S.H. Kim, Thyroid stimulating hormone is associated with metabolic syndrome in euthyroid postmenopausal women. Maturitas 62, 301–305 (2009)
A. Giandalia, G.T. Russo, E.L. Romeo, A. Alibrandi, P. Villari, A.A. Mirto, G. Armentano, S. Benvenga, D. Cucinotta, Influence of high-normal serum TSH levels on major cardiovascular risk factors and Visceral Adiposity Index in euthyroid type 2 diabetic subjects. Endocrine 47, 152–160 (2014)
J.E. Jun, S.M. Jin, J.H. Jee, J.C. Bae, K.Y. Hur, M.K. Lee, S.W. Kim, J.H. Kim, TSH increment and the risk of incident type 2 diabetes mellitus in euthyroid subjects. Endocrine 55, 944–953 (2017)
V. Velkoska Nakova, B. Krstevska, M. Bosevski, Ch Dimitrovski, V. Serafimoski, Dyslipidaemia and hypertension in patients with subclinical hypothyroidism. Prilozi 30, 93–102 (2009)
Y. Zhang, P. Lu, L. Zhang, X. Xiao, Association between lipids profile and thyroid parameters in euthyroid diabetic subjects: a cross-sectional study. BMC Endocr. Disord. 15, 12 (2015). https://doi.org/10.1186/s12902-015-0008-3
V.L. Langén, T.J. Niiranen, P. Puukka, J. Sundvall, A.M. Jula, V.L. Langén, T.J. Niiranen, P. Puukka, J. Sundvall, A.M. Jula, Association between thyroid-stimulating hormone and blood pressure in adults: an 11-year longitudinal study. Clin. Endocrinol. 84, 741–747 (2016)
T. Ittermann, D. Tiller, C. Meisinger, C. Agger, M. Nauck, R. Rettig, A. Hofman, T. Jørgensen, A. Linneberg, J.C. Witteman, O.H. Franco, K.H. Greiser, K. Werdan, A. Döring, A. Kluttig, B.H. Stricker, H. Völzke, High serum thyrotropin levels are associated with current but not with incident hypertension. Thyroid 23, 955–963 (2013)
Y. Duan, W. Peng, X. Wang, W. Tang, X. Liu, S. Xu, X. Mao, S. Feng, Y. Feng, Y. Qin, K. Xu, C. Liu, C. Liu, Community-based study of the association of subclinical thyroid dysfunction with blood pressure. Endocrine 35, 136–142 (2009)
R. Luboshitzky, A. Aviv, P. Herer, L. Lavie, Risk factors for cardiovascular disease in women with subclinical hypothyroidism. Thyroid 12, 421–425 (2002)
D. Liu, F. Jiang, Z. Shan, B. Wang, J. Wang, Y. Lai, Y. Chen, M. Li, H. Liu, C. Li, H. Xue, N. Li, J. Yu, L. Shi, X. Bai, X. Hou, L. Zhu, L. Lu, S. Wang, Q. Xing, W. Teng, A cross-sectional survey of relationship between serum TSH level and blood pressure. J. Hum. Hypertens. 24, 134–138 (2010)
W.X. Jian, J. Jin, L. Qin, W.J. Fang, X.R. Chen, H.B. Chen, Q. Su, H.L. Xing, Relationship between thyroid-stimulating hormone and blood pressure in the middle-aged and elderly population. Singap. Med. J. 54, 401–405 (2013)
L. Petrosyan, Relationship between high normal TSH levels and metabolic syndrome components in type 2 diabetic subjects with euthyroidism. J. Clin. Transl. Endocrinol. 2, 110–113 (2015)
B.O. Asvold, T. Bjøro, T.I. Nilsen, L.J. Vatten, Association between blood pressure and serum thyroid-stimulating hormone concentration within the reference range: a population-based study. J. Clin. Endocrinol. Metab. 92, 841–845 (2007)
A. Iqbal, Y. Figenschau, R. Jorde, Blood pressure in relation to serum thyrotropin: the Tromsø study. J. Hum. Hypertens. 20, 932–936 (2006)
O. Gumieniak, T.S. Perlstein, P.N. Hopkins, N.J. Brown, L.J. Murphey, X. Jeunemaitre, N.K. Hollenberg, G.H. Williams, Thyroid function and blood pressure homeostasis in euthyroid subjects. J. Clin. Endocrinol. Metab. 89, 3455–3461 (2004)
K. Saltiki, P. Voidonikola, K. Stamatelopoulos, E. Mantzou, C. Papamichael, M. Alevizaki, Association of thyroid function with arterial pressure in normotensive and hypertensive euthyroid individuals: a cross-sectional study. Thyroid Res. 1(1), 3 (2008)
A. Tsuda, M. Inaba, M. Ichii, A. Ochi, Y. Ohno, S. Nakatani, S. Yamada, K. Mori, H. Tahara, E. Ishimura, Relationship between serum TSH levels and intrarenal hemodynamic parameters in euthyroid subjects. Eur. J. Endocrinol. 169, 45–50 (2013)
M. Laclaustra, Y. Hurtado-Roca, M. Sendin, M. Leon, M. Ledesma, E. Andres, A. Fernandez-Ortiz, E. Guallar, J.M. Ordovas, J.A. Casasnovas, Lower-normal TSH is associated with better metabolic risk factors: a cross-sectional study on Spanish men. Nutr. Metab. Cardiovasc. Dis. 25, 1095–1103 (2015)
C. Virili, A. Antonelli, M.G. Santaguida, S. Benvenga, M. Centanni, Gastrointestinal malabsorption of thyroxine. Endocr. Rev. 40(1), 118–136 (2019)
P.M. Mannucci, A. Nobili, L. Pasina, REPOSI Collaborators (REPOSI is the acronym of REgistro POliterapie SIMI, Società Italiana di Medicina Interna). Polypharmacy in older people: lessons from 10 years of experience with the REPOSI register. Intern. Emerg. Med. 13(8), 1191–1200 (2018)
R. Vita, G. Saraceno, F. Trimarchi, S. Benvenga, Switching levothyroxine from the tablet to the oral solution formulation corrects the impaired absorption of levothyroxine induced by proton-pump inhibitors. J. Clin. Endocrinol. Metab. 99, 4481–4486 (2014)
C. Virili, L. Giovanella, P. Fallahi, A. Antonelli, M.G. Santaguida, M. Centanni, P. Trimboli, Levothyroxine therapy: changes of TSH levels by switching patients from tablet to liquid formulation. A systematic review and meta-analysis. Front Endocrinol. 9, 10 (2018). https://doi.org/10.3389/fendo.2018.00010
R. Vita, F. Di Bari, S. Benvenga, Oral liquid levothyroxine solves the problem of tablet levothyroxine malabsorption due to concomitant intake of multiple drugs. Expert. Opin. Drug Deliv. 14, 467–472 (2017)
C. Virili, P. Trimboli, F. Romanelli, M. Centanni, Liquid and softgel levothyroxine use in clinical practice: state of the art. Endocrine 54(1), 3–14 (2016)
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
S.B. received novel formulations of LT4 from IBSA Institute Biochimique (Lugano, Switzerland) and IBSA s.r.l. (Lodi, Italy) to be given to patients for conducting clinical studies. In addition, S.B. was an invited speaker at symposia organized by IBSA. However, IBSA had no role in any phase of the writing of this manuscript. The remaining authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of our institutional research committee at University Hospital of Messina and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Morini, E., Catalano, A., Lasco, A. et al. In thyroxine-replaced hypothyroid postmenopausal women under simultaneous calcium supplementation, switch to oral liquid or softgel capsule l-thyroxine ensures lower serum TSH levels and favorable effects on blood pressure, total cholesterolemia and glycemia. Endocrine 65, 569–579 (2019). https://doi.org/10.1007/s12020-019-01908-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12020-019-01908-x