
Abstract
The population in the areas neighboring the Semipalatinsk Nuclear Test Site (SNTS) in the eastern region of Kazakhstan faces increased cardiovascular disease (CVD) risk. Previous research has not explored gene polymorphisms related to CVD in this population. Therefore, the present study examines the prevalence of six CVD-associated genotypes in three generations exposed to SNTS radiation. The genotyping of ApoE Leu28 → Pro, AGT Met174 → Thr, AGT Met235 → Thr, eNOS T786 → C, PON1 Gln192 → Arg, and EDN 1 Lys198 → Asn was performed using real-time polymerase chain reaction. The present study encompassed a cohort of 218 participants with a familial history of arterial hypertension and/or carotid artery disease spanning at least three generations. The analysis unveiled significant disparities in the prevalence of ApoE Leu28 → Pro, eNOS T786 → C, and PON1 Gln192 → Arg genotypes across different generations. Furthermore, a substantial variation in the distribution of the eNOS T786 → C genotype was observed between individuals of Kazakh and Russian ethnicities. Nevertheless, no significant discrepancies were detected in the frequencies of the investigated genotypes between genders. Further research in this area is warranted to enhance the understanding of the genetic factors contributing to CVD in the population exposed to radiation from the SNTS. Specifically, future studies should broaden the scope of genetic polymorphisms investigated and include representatives of healthy individuals who have not been exposed to radiation as controls.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The Semipalatinsk Nuclear Test Site (SNTS), located in the eastern region of the Republic of Kazakhstan, holds an important place in global nuclear testing history and its consequences. Over the span of 40 years, from 1949 to 1989, the Soviet Union conducted approximately 456 nuclear tests at this site, comprising atmospheric, underground, and underwater explosions. However, during the initial period from 1949 to 1962, the tests were carried out without sufficient consideration for the long-term consequences, with the primary objective being the advancement of the Soviet Union's nuclear capabilities and military strategies. Consequently, significant amounts of radioactive materials were released into the atmosphere, exacerbated by unfavorable weather conditions that led to the dispersion of fallout and subsequent contamination of the surrounding land, water reservoirs, and vegetation. The health effects arising from the nuclear tests conducted at the SNTS have had enduring consequences on the region and its residents [1].
The population residing in the vicinity of the SNTS faces an increased risk of various health disorders, including a heightened prevalence of cardiovascular disease (CVD). A study conducted by Markabayeva et al. shed light on the elevated rates of essential arterial hypertension (AH) among individuals exposed to radiation at varying doses. The research demonstrated a dose-dependent effect, revealing that the odds of developing AH were 1.52 times higher for individuals exposed to radiation within the dose range of 20–59 mSv, 1.67 times higher for those exposed to doses of 60–185 mSv, and 1.93 times higher for individuals exposed to doses exceeding 186 mSv, compared to those exposed to doses below 20 mSv [2]. Another study by Markabayeva et al. revealed a significant positive correlation between radiation dose and levels of low-density lipoproteins and total cholesterol [3]. Furthermore, a large cohort study on stroke patients exhibited higher rates of associated CVDs such as AH, atrial fibrillation, and chronic heart failure among individuals exposed to radiation at the SNTS compared to unexposed individuals. The study also established a dose–response relationship with the mortality risk of ischemic stroke [4].
A wide range of gene mutations have been identified as contributors to the development of CVD. These mutations lead to the altered synthesis of specific enzymes, triggering a cascade of pathological reactions that worsen and manifest cardiovascular pathology. For instance, the apolipoprotein E (APOE) gene on chromosome 19 regulates lipoprotein levels in the blood. The leucine-to-proline substitution at position 28 (Leu28 → Pro) in this gene has been associated with coronary artery disease (CAD) [5]. On chromosome 1, the angiotensinogen (AGT) gene has been linked to myocardial infarction through the methionine-to-threonine substitution at position 174 (Met174 → Thr) [6]. Similarly, the methionine-to-threonine substitution at position 235 (Met235 → Thr) in AGT is a risk factor for CAD [7]. The endothelial nitric oxide synthase (eNOS) gene, located on chromosome 7, is associated with both AH and CAD due to the thymine-to-cysteine substitution at position 786 (T786 → C) [8]. The paraoxonase 1 (PON1) gene, found on chromosome 7, contains the glutamine-to-arginine substitution at position 192 (Gln192 → Arg), which is linked to CAD [9]. The endothelin 1 (EDN1) gene, situated on chromosome 6, exhibits the lysine-to-asparagine substitution at position 198 (Lys198 → Asn), associated with a range of CVDs, including AH and CAD [10].
Research has previously not been investigating the gene polymorphisms associated with CVD development in populations exposed to radiation fallout from the SNTS. Hence, the objective of this study was to assess the genotypes of ApoE Leu28 → Pro, AGT Met174 → Thr, AGT Met235 → Thr, eNOS T786 → C, PON1 Gln192 → Arg, and EDN1 Lys198 → Asn in three generations of individuals residing in the contaminated areas surrounding the SNTS. The present study’s findings are crucial for advancing targeted prevention and intervention strategies to improve cardiovascular health within the affected population.
Materials and Methods
Subject Recruitment
The present study focuses on individuals with CVD. The study participants were selected from the State Scientific Automated Medical Registry (SSAMR), a valuable data source on the population affected by the SNTS [11]. The SSAMR collects detailed information on these individuals, categorized by specific diseases. In 2003, Kazakhstan implemented a law aimed at providing social protection to individuals impacted by the activities of the SNTS, leading to the establishment of the SSAMR [12]. This law includes various forms of compensation, such as screenings and medical examinations, as part of the rehabilitation process for those exposed to radiation.
Participants had to meet the criteria of having at least three generations of family members with CVD to be included in the study. The first generation (grandparents) resided in the villages of Abayskiy, Beskaragayskiy, and Borodulikhinskiy districts, which are situated near the SNTS, and experienced significant radioactive fallout between 1949 and 1962 during open or surface nuclear tests. The second generation (parents) consisted of children of those directly exposed to the SNTS activities. This generation includes individuals affected by the SNTS from 1962 to 1989, when underground nuclear tests were conducted with occasional leaks. The third generation (grandchildren) comprises individuals born after 1989 when no further explosions occurred at the SNTS [13]. To verify radiation exposure from the SNTS, official documents were used, including "kolkhoz books" used for registering rural residents by the Soviet administration and "polygon certificates" issued by Kazakh authorities in the 1990s to confirm residency in the affected areas.
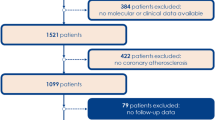
The SSAMR contains approximately 14,000 registered individuals exposed to radiation and reside in the Abayskiy, Beskaragayskiy, and Borodulikhinskiy districts. Among them, 3014 individuals are registered as having CVD (AH and CAD). Three generations were verified within the same family as possible for 386 individuals. One representative from each family was contacted via telephone and invited to participate in the study, along with their relatives from other generations. Of the 386 eligible individuals, 218 agreed to participate in the study and provided blood samples for genetic testing. The majority of study participants were of Kazakh ethnicity, reflecting the current ethnic structure of the country [14]. However, the sample was skewed toward a higher predominance of middle-aged females (second generation), who were more motivated to take part in the study than their older or younger counterparts.
Data on metabolic parameters were extracted from accompanying medical records. The most recent measurements of total cholesterol levels and blood glucose within the past three months were obtained, along with height and weight. Total cholesterol was categorized as normal (< 5.17 mmol/L), borderline (5.17–6.18 mmol/L), and high (≥ 6.19 mmol/L) [15]. Blood glucose was classified as normal (< 5.6 mmol/L), impaired (5.6–6.9 mmol/L), and diabetic (≥ 7.0 mmol/L) [16]. Body mass index (BMI) was calculated based on height and weight measurements using the formula: weight in kilograms divided by height in meters squared, and classified as normal (< 24.9), overweight (25.0–29.9), and obese (≥ 30.0) [17].
Selection of Candidate Genes
The selection of candidate genes was carried out through an extensive analysis of three primary data sources. Firstly, the 1,000 Genomes project, renowned for its comprehensive collection of human genotypes and phenotypes on a global scale, was utilized [18]. Secondly, the Text-mined Hypertension, Obesity, and Diabetes candidate gene database were consulted to compile information on genes associated with these specific disorders [19]. Lastly, the CADgene database [20], focusing on genes related to CAD, was included in the analysis. By meticulously examining the information contained in these databases, a set of six candidate genes was identified for further investigation: ApoE Leu28 → Pro, AGT Met174 → Thr, AGT Met235 → Thr, eNOS T786 → C, PON1 Gln192 → Arg, and EDN1 Lys198 → Asn.
DNA Extraction and Genotyping of Samples
Peripheral venous blood samples of 10 ml were collected from each participant using EDTA vacuum tubes for DNA extraction. The DNA extraction process utilized commercially available DNA-Express Genetics kits (Lytech, Inc.) following the manufacturer's instructions. The concentration and purity of the extracted DNA were assessed using a NanoDrop™ 2000/2000C spectrophotometer. The isolated DNA was subsequently stored at – 20 °C for future use.
Genotyping of the samples was conducted utilizing commercially available SNP-EXPRESS kits (Lytech, Inc.) specific to each SNP of interest. The genotyping procedure involved real-time polymerase chain reaction (RT-PCR) performed on a QuantStudio 5 device (Applied Biosystems, Thermo Fisher Scientific).
Among the 218 study participants screened, data on AGT Met174 → Thr and AGT Met235 → Thr genotypes were available for all participants (n = 218), while data on ApoE Leu28 → Pro, eNOS T786 → C, PON1 Gln192 → Arg, and EDN1 Lys198 → Asn genotypes were obtainable for 214 participants only. This discrepancy may be attributed to rare gene variants characterized by a high degree of polymorphism or structural DNA alterations that impede standard genotyping methods from detecting the alleles under investigation.
Statistical Analysis
Categorical variables were presented using absolute numbers and percentages to provide a comprehensive overview of the data. Between-group differences were evaluated using the likelihood ratio and Fisher’s exact tests. As for the continuous variable in the study, namely age, its distribution deviated from normality. Therefore, the median and the interquartile range (IQR) were reported. The observed genotypes were categorized as normal homozygote, heterozygote, and mutant homozygote to classify the genetic variations. Hardy–Weinberg equilibrium was applied to assess the ratio of genotype and allele frequencies, ensuring genetic equilibrium within the studied population. Statistical analyses were performed using IBM SPSS Statistics Version 24 (IBM, Armonk, NY, USA). The significance level for all tests was set at p < 0.05.
Results
Table 1 provides an overview of the demographic characteristics of the study participants. The data shows that most individuals belonged to the second generation (64.2%), while the first and third generations had relatively smaller representations (12.4% and 23.4%, respectively). The median age of the first generation was 68.00 years, the second generation was 52.00 years, and the third generation was 23.00 years. Additionally, most study participants were females, comprising 148 individuals or 67.9% of the total sample.
Table 2 presents the metabolic parameters of the study participants as documented in the accompanying medical records. Overall, there were notable differences among representatives of all three generations in total cholesterol, BMI, and blood glucose, with the first generation exhibiting the highest levels across all parameters studied. Conversely, representatives of the third generation demonstrated the lowest levels across all parameters. These distinctions are primarily attributed to age differentials among the three generations, contributing to the burden of disease.
Table 3 presents the distribution of genetic polymorphisms among representatives of the first, second, and third generations. Significant differences were observed in the frequencies of the ApoE Leu28 → Pro genotype. Among the 214 tested individuals, the second generation had the highest proportion of normal homozygotes and heterozygotes (56.0% and 71.4% of individuals, respectively). Significant between-generation differences were also observed in the distribution of the eNOS T786 → C genotype, with the second generation having the highest proportion of normal homozygotes and heterozygotes. Notably, the mutant homozygous allele was more common in representatives of the third generation (46.1%). Moreover, the frequency of the PON1 Gln192 → Arg genotype also differed significantly among the three generations, with normal homozygotes and heterozygotes being more common in the second generation (57.6% and 71.6%, respectively), while the mutant homozygous allele was predominant in the third generation (66.7%).
Table 4 presents the distribution of genetic polymorphisms by gender and ethnicity. Notably, the majority of individuals with a homozygous allele in eNOS T786 → C were females (17 individuals, 65.4%). However, none of the observed differences reached statistical significance. Regarding ethnicity, the only significant difference was observed for the eNOS T786 → C genotype.
Discussion
The present epidemiological study represents the first investigation into the polymorphisms of six genes associated with CVD in three generations of individuals exposed to radiation from the SNTS. The present study identified significance between-generation differences in the distribution of ApoE Leu28 → Pro, eNOS T786 → C, and PON1 Gln192 → Arg genotypes, as well as a significance between-ethnicity difference in the distribution of the eNOS T786 → C genotype. However, no differences were found between representatives of both sexes. The primary objective of the present study was to develop targeted strategies for managing CVD in the population affected by the SNTS.
CVD, including AH and CAD, is a multifactorial disorder influenced by a combination of modifiable and genetic risk factors. Modifiable risk factors include dietary habits, physical activity, personality traits, and occupational and environmental exposures [21]. On the other hand, numerous genetic polymorphisms have been associated with the development of CVD, and polygenic risk scores have been proposed to assess the cumulative genetic risk contribution. Furthermore, evidence of familial clustering of AH and CAD suggests a familial predisposition to early-onset disease. Hypercholesterolemia, in particular, has been identified as a precipitating factor for these conditions. Several genes have been implicated in hypercholesterolemia, and individuals carrying specific genetic mutations may benefit from early initiation of statin therapy beyond dietary interventions [22]. Homozygous mutations confer a significantly higher risk of developing early-onset CAD, although rare, affecting approximately 1 case in 1 million individuals. Heterozygotes also face an increased risk of developing the disease, with a prevalence estimated at 1 in 250 to 500 individuals [23].
Although the present study did not specifically investigate genetic polymorphisms associated with familial hypercholesterolemia, such as mutations in the LDLR, APOB, and PCSK9 genes [23], other genotypes known to be associated with hypercholesterolemia were examined. The observed intergenerational differences in the frequency of certain genotypes warrant further investigation. While the exact contribution of radiation exposure from the SNTS remains unclear, it may have played a role.
In addition to environmental exposures, lifestyle exerts a considerable influence on the development and progression of CVD. Dietary habits represent a main aspect of CVD prevention and management. Notably, the Kazakhstani diet is recognized as one of the world's unhealthiest, characterized by elevated sodium levels. On average, a Kazakhstani consumes approximately 17 g of salt per day, surpassing the World Health Organization's recommended limit by fourfold [24].Tobacco use constitutes another significant risk factor for CVD. Despite a declining trend in smoking prevalence, recent data indicate that nearly 40% of men in Kazakhstan smoke [25]. Presently, there is limited emphasis on primary prevention strategies for CVD in Kazakhstan, as evidenced by a dearth of nationally implemented programs [26]. Despite an exhaustive search, studies specifically addressing CVD-related lifestyle factors within this population group were not identified. However, it is plausible to speculate that this population shares lifestyle characteristics with the broader Kazakhstani populace, thereby carrying an elevated risk for CVD.
Membership in a specific ethnic group may contribute to a predisposition for carrying certain mutations. Despite a comprehensive search of evidence-based medicine databases, limited studies are available investigating the frequencies of genotypes associated with ApoE, AGT174, AGT235, eNOS, PON1, and EDN1 in the Kazakh population. For instance, Berkinbayev et al. examined APOE gene polymorphisms in ethnic Kazakhs related to coronary heart disease, identifying associations between various APOE gene alleles and the disease but not reporting the frequency of these alleles [27]. Sikhayeva et al. investigated the distribution of the EDN1 gene in the Kazakh population with type 2 diabetes mellitus, reporting a frequency of 58% for normal homozygotes, 35% for heterozygotes, and 7% for mutant homozygotes [28]. Zhou et al. conducted a study to determine the frequency of AGT174 genotypes in hypertensive patients of Kazakh ethnicity residing in Xinjiang province, China. They compared it with healthy controls of the same ethnicity. The study revealed a frequency of 74.2% for normal homozygous alleles in hypertensive patients, while healthy controls had a frequency of 78.0%. Additionally, the combined prevalence of heterozygous and mutant homozygous alleles among hypertensive patients was 25.8%, whereas 22.0% in controls [29].
Of particular interest in the present study is the finding of significant between-ethnic differences in the frequency of eNOS genotypes. Specifically, the study findings indicate that among individuals of Kazakh ethnicity, 12.6% were identified as homozygous mutant carriers, whereas among individuals of Russian ethnicity, the prevalence was 10.9%. These results suggest a slightly higher occurrence of the mutation in the Kazakh population compared to the Russian population. However, no earlier research reported the frequency of this genetic polymorphism, specifically in the Kazakh population. Nonetheless, several studies examine individuals of Russian or Ukrainian ethnicity. For instance, Gruzdeva, in her doctoral thesis, reported the frequency of eNOS polymorphisms in patients with CAD and AH of Russian ethnicity. According to her findings, the prevalence of normal homozygous carriers was 47.0%, while heterozygous carriers accounted for 48.5% of the population, and only 4.5% were carriers of the mutant homozygote [30]. Additionally, Dosenko et al. reported the frequency of the eNOS T786 → C genotype in patients with acute coronary syndrome (ACS) of Ukrainian ethnicity compared to healthy controls of the same ethnicity. Among ACS patients, the prevalence of normal homozygous carriers was 47.5%, while 48.2% in controls. The prevalence of heterozygous carriers among ACS patients was 36.2% compared to 45.8% in controls, and the prevalence of homozygous mutant carriers was 16.3% compared to 6.0% in healthy controls. In the present study, among participants of Russian ethnicity, 27.3% were normal homozygous carriers, 61.8% were heterozygous carriers, and 10.9% were homozygous mutant carriers [31]. It is important to note that there is insufficient data on the genetic polymorphisms of eNOS genotypes in representatives of various ethnicities residing in Kazakhstan, highlighting the need for further research in this area.
The present study has several limitations, the major being the unavailability of a control group. This limitation is because the study relied on the SSAMR, which only included individuals exposed to radiation. Consequently, it was challenging to include individuals from the general population as not all individuals exposed to radiation from the SNTS are listed in the SSAMR. Another limitation arises from the inability to differentiate between AH and CAD since they are categorized together in the SSAMR. Despite a total sample size of 218 individuals, distributed among 68 families, it was not feasible to ensure a more comprehensive examination of the consistency of observed polymorphisms across all generations within each family. In addition, the study's sample composition is disproportionately skewed toward women, who constituted 67.9% of the sample size, and predominantly represents the second generation, with a median age of 52 years. This skewed representation could be attributed to the tendency of middle-aged females to participate more readily in the study, while males exhibited a higher reluctance. This phenomenon has been observed in earlier surveys and could be linked to heightened health-related anxiety among females [32].
Despite these limitations, the study exhibits several strengths. Notably, it boasts a reasonable sample size, access to data spanning three generations exposed to radiation from the SNTS, and the examination of six genes linked to cardiovascular pathology. However, it is imperative for future research to address the limitation of not incorporating healthy controls. Moreover, forthcoming studies should encompass a broader array of genetic polymorphisms and explore their correlation with specific cardiovascular events. Additionally, there is a need to recruit a larger sample size to observe the consistency of genetic polymorphisms across all generations within the same family. Furthermore, there is a pressing need to involve the fourth generation of the exposed population in genetic epidemiology research. Further genetic analyses could delve into additional genetic variants associated with CVD risk. Leveraging advanced genomic technologies, such as whole-genome sequencing, could yield comprehensive insights into the genetic determinants of CVD within this population. Furthermore, investigating the intricate interplay among environmental exposures, lifestyle factors, and genetic predispositions in the genesis of CVD is paramount.
In addition to its research implications, the present study holds practical significance. Firstly, there is a necessity to implement strategies aimed at the primary prevention of CVD through lifestyle modifications and to enhance strategies targeting the secondary prevention of CVD through screening and treatment, which is suboptimal at the level of the rural population [26]. Moreover, a personalized medicine approach could be implemented. Tailoring treatment plans based on an individual's genetic profile can help optimize therapeutic outcomes, allowing for targeted interventions and medication selection [33].
Conclusion
The present epidemiological study investigated the association between six genes and CVD in three generations of individuals exposed to radiation from the SNTS. The findings revealed significant intergenerational differences in the distribution of ApoE Leu28 → Pro, eNOS T786 → C, and PON1 Gln192 → Arg genotypes. However, the exact role of radiation exposure from the SNTS in contributing to these differences remains uncertain and requires further exploration. Additionally, the present study shed light on the potential impact of ethnicity on the prevalence of specific genetic mutations, as demonstrated by a significant difference in the frequency of the eNOS T786 → C genotype between individuals of Kazakh and Russian ethnicity. These results have implications for developing more precise and tailored interventions to address the specific needs of the population affected by radiation exposure from the SNTS. Future research endeavors should aim to elucidate the observed associations' mechanisms and expand the investigation to encompass a wider range of genetic polymorphisms and their relationship to cardiovascular events.
Data availability
The data used and analyzed during the current study are available from the corresponding author upon reasonable request. The data are not publicly accessible due to their personal nature.
References
Drozdovitch, V., Schonfeld, S., Akimzhanov, K., Aldyngurov, D., Land, C. E., Luckyanov, N., et al. (2011). Behavior and food consumption pattern of the population exposed in 1949–1962 to fallout from Semipalatinsk nuclear test site in Kazakhstan. Radiation and Environmental Biophysics, 50(1), 91–103. https://doi.org/10.1007/s00411-010-0334-9
Markabayeva, A., Bauer, S., Pivina, L., Bjørklund, G., Chirumbolo, S., Kerimkulova, A., et al. (2018). Increased prevalence of essential hypertension in areas previously exposed to fallout due to nuclear weapons testing at the Semipalatinsk Test Site, Kazakhstan. Environmental Research, 167, 129–135. https://doi.org/10.1016/j.envres.2018.07.016
Markabayeva, A. M., Kerimkulova, A. S., Pivina, L. M., Rakhypbekov, T. K., Apsalikov, K. M., Ospanova, A. S., et al. (2015). Lipid profile among the population exposed to radiation from Semipalatinsk nuclear test site, Kazakhstan. Human Ecology (Russian Fed), 22, 7–14. https://doi.org/10.17816/humeco16985
Semenova, Y., Rakhimova, I., Nurpeissov, T., Alikeyeva, G., Khaibullin, T., Kovalchuk, V., et al. (2022). Epidemiology of stroke and transient ischemic attacks in the population of the territories adjacent to the former Semipalatinsk Nuclear Test Site, Kazakhstan. Radiation and Environmental Biophysics, 61(1), 17–28. https://doi.org/10.1007/s00411-021-00955-1
Orth, M., Weng, W., Funke, H., Steinmetz, A., Assmann, G., Nauck, M., et al. (1999). Effects of a frequent apolipoprotein E isoform, ApoE4Freiburg (Leu28–>Pro), on lipoproteins and the prevalence of coronary artery disease in whites. Arteriosclerosis, Thrombosis, and Vascular Biology, 19(5), 1306–1315. https://doi.org/10.1161/01.atv.19.5.1306
Li, Y. Y., Wang, H., Wang, H., & Zhang, Y. Y. (2021). Myocardial infarction and AGT p.Thr174Met polymorphism: A meta-analysis of 7657 subjects. Cardiovascular Therapeutics. https://doi.org/10.1155/2021/6667934
Zhao, H., Zhao, R., Hu, S., & Rong, J. (2020). Gene polymorphism associated with angiotensinogen (M235T), endothelial lipase (584C/T) and susceptibility to coronary artery disease: a meta-analysis. Bioscience Reports, 40(7), BSR20201414.
Ciftci, C., Melil, S., Cebi, Y., Ersoz, M., Cagatay, P., Kilicgedik, M., et al. (2008). Association of endothelial nitric oxide synthase promoter region (T-786C) gene polymorphism with acute coronary syndrome and coronary heart disease. Lipids in Health and Disease, 7, 5. https://doi.org/10.1186/1476-511X-7-5
Hernandez-Diaz, Y., Tovilla-Zarate, C. A., Juarez-Rojop, I. E., Gonzalez-Castro, T. B., Rodriguez-Perez, C., Lopez-Narvaez, M. L., et al. (2016). Effects of paraoxonase 1 gene polymorphisms on heart diseases: Systematic review and meta-analysis of 64 case-control studies. Medicine (Baltimore), 95(44), e5298. https://doi.org/10.1097/MD.0000000000005298
Ahmed, M., & Rghigh, A. (2016). Polymorphism in Endothelin-1 gene: An overview. Current Clinical Pharmacology, 11(3), 191–210. https://doi.org/10.2174/1574884711666160701000900
Apsalikov, K. N., Lipikhina, A., Grosche, B., Belikhina, T., Ostroumova, E., Shinkarev, S., et al. (2019). The State Scientific Automated Medical Registry, Kazakhstan: An important resource for low-dose radiation health research. Radiation and Environmental Biophysics, 58(1), 1–11. https://doi.org/10.1007/s00411-018-0762-5
Republic of Kazakhstan. (1992). Law of the Republic of Kazakhstan dated December 18, 1992, No. 1787-XII. In: On the social protection of citizens affected by nuclear tests at the Semipalatinsk nuclear test site.
Schwerin, M., Schonfeld, S., Drozdovitch, V., Akimzhanov, K., Aldyngurov, D., Bouville, A., et al. (2010). The utility of focus group interviews to capture dietary consumption data in the distant past: Dairy consumption in Kazakhstan villages 50 years ago. Journal of Developmental Origins of Health and Disease, 1(3), 192–202. https://doi.org/10.1017/S2040174410000243
Ministry of National Economy of the Republic of Kazakhstan. (2017). Demographic Yearbook of Kazakhstan. Statistical compilation. Astana: Ministry of National Economy of the Republic of Kazakhstan, Committee on Statistics.
RingMD: High Cholesterol. Retrieved February 27, 2024, from https://www.ring.md/topics/high-cholesterol
American Diabetes A. (2009). Diagnosis and classification of diabetes mellitus. Diabetes Care, 32 Suppl 1(Suppl 1), S62–S67. https://doi.org/10.2337/dc09-S062
Weir, C. B., & Jan, A. (2024). BMI classification percentile and cut off points. StatPearls.
Nikpay, M., Goel, A., Won, H. H., Hall, L. M., Willenborg, C., Kanoni, S., et al. (2015). A comprehensive 1,000 Genomes-based genome-wide association meta-analysis of coronary artery disease. Nature Genetics, 47(10), 1121–1130. https://doi.org/10.1038/ng.3396
Dai, H. J., Wu, J. C., Tsai, R. T., Pan, W. H., & Hsu, W. L. (2013). T-HOD: A literature-based candidate gene database for hypertension, obesity and diabetes. Database (Oxford). https://doi.org/10.1093/database/bas061
Liu, H., Liu, W., Liao, Y., Cheng, L., Liu, Q., Ren, X., et al. (2011). CADgene: a comprehensive database for coronary artery disease genes. Nucleic Acids Research, 39(Database issue), 991–6. https://doi.org/10.1093/nar/gkq1106
Goldsborough, E., 3rd., Osuji, N., & Blaha, M. J. (2022). Assessment of cardiovascular disease risk: A 2022 update. Endocrinology and Metabolism Clinics of North America, 51(3), 483–509. https://doi.org/10.1016/j.ecl.2022.02.005
O’Sullivan, J. W., Raghavan, S., Marquez-Luna, C., Luzum, J. A., Damrauer, S. M., Ashley, E. A., et al. (2022). Polygenic risk scores for cardiovascular disease: A scientific statement from the American Heart Association. Circulation, 146(8), e93–e118. https://doi.org/10.1161/CIR.0000000000001077
Goldstein, J. K., Hobbs, H. H., & Brown, M. S. (2001). Familial hypercholesterolemia. In C. R. Scriver, A. L. Beaudet, W. S. Sly, & D. Valle (Eds.), The metabolic & molecular bases of inherited disease (8th ed., pp. 2863–2913). McGraw-Hill.
World Health Organization. (2019). WHO studies reveal Kazakhstan has among the highest levels of salt intake globally. Retrieved February 22, 2024, from https://www.who.int/europe/news/item/07-03-2019-who-studies-reveal-kazakhstan-has-among-the-highest-levels-of-salt-intake-globally
Glushkova, N., Smailova, D., Namazbayeva, Z., Mukasheva, G., Zhamakurova, A., Kuanyshkalieva, A., et al. (2021). Prevalence of smoking various tobacco types in the Kazakhstani Adult Population in 2021: A cross-sectional study. International Journal of Environmental Research Public Health. https://doi.org/10.3390/ijerph20021509
Glushkova, N., Turdaliyeva, B., Kulzhanov, M., Karibayeva, I. K., Kamaliev, M., Smailova, D., et al. (2023). Examining disparities in cardiovascular disease prevention strategies and incidence rates between urban and rural populations: Insights from Kazakhstan. Science and Reports, 13(1), 20917. https://doi.org/10.1038/s41598-023-47899-8
Berkinbayev, S., Rysuly, M., Mussayev, A., Blum, K., Baitasova, N., Mussagaliyeva, A., et al. (2014). Apolipoprotein Gene Polymorphisms (APOB, APOC111, APOE) in the Development of Coronary Heart Disease in Ethnic Groups of Kazakhstan. J Genet Syndr Gene Ther., 5(2), 216. https://doi.org/10.4172/2157-7412.100021610.4172/2157-7412.1000216
Sikhayeva, N., Talzhanov, Y., Iskakova, A., Dzharmukhanov, J., Nugmanova, R., Zholdybaeva, E., et al. (2018). Type 2 diabetes mellitus: Distribution of genetic markers in Kazakh population. Clinical Interventions in Aging, 13, 377–388. https://doi.org/10.2147/CIA.S156044
Zhou, L., Li, N. F., Wang, X. L., Zhang, D. L., Wang, J., Ouyang, W. J., et al. (2005). Distributer characteristics of angiotensiongen (AGT) gene T17M polymorphism in Kazakans of Xinjiang. Yi Xue Fen Zi Sheng Wu Xue Za Zhi, 2, 162–165.
Gruzdeva, A. A. (2020). Clinical and pharmacological aspects of enhancing the treatment outcomes in patients with cardiovascular conditions. Yaroslavl State Medical University. [in Russian].
Dosenko, V. E., Zagoriy, V. Y., Lutay, Y. M., Parkhomenko, A. N., & Moibenko, A. A. (2006). Allelic polymorphism in the promoter (T–>C), but not in exon 7 (G–>T) or the variable number tandem repeat in intron 4, of the endothelial nitric oxide synthase gene is positively associated with acute coronary syndrome in the Ukrainian population. Experimental and Clinical Cardiology, 11(1), 11–13.
Semenova, Y., Pivina, L., Manatova, A., Bjørklund, G., Glushkova, N., Belikhina, T., et al. (2019). Mental distress in the rural Kazakhstani population exposed and non-exposed to radiation from the Semipalatinsk Nuclear Test Site. Journal of Environmental Radioactivity, 203, 39–47. https://doi.org/10.1016/j.jenvrad.2019.02.013
Strianese, O., Rizzo, F., Ciccarelli, M., Galasso, G., D’Agostino, Y., Salvati, A., et al. (2020). Precision and personalized medicine: how genomic approach improves the management of cardiovascular and neurodegenerative disease. Genes (Basel). https://doi.org/10.3390/genes11070747
Funding
The present study’s data were collected as part of the scientific project titled "Development of science-based technologies to minimize ecological risk and prevent adverse health effects" (Reg.-N 012RK01090), funded by the Ministry of Health, Kazakhstan.
Author information
Authors and Affiliations
Contributions
The contributions of GB, LP, and YS met the following three requirements: (a) significant contributions to the conception and design, acquisition of data, or analysis and interpretation of data; (b) drafting or revising the article for intellectual content; and (c) final approval of the published article.
Corresponding author
Ethics declarations
Competing interest
The authors declare no competing interests.
Ethical Approval
Before the initiation of the study, all participants provided informed consent, demonstrating their voluntary participation and comprehension of the study's objectives and procedures. The present study protocol underwent a thorough review and received approval from the Ethics Committee of Semey Medical University under Protocol No. 6 on April 27th, 2017.
Additional information
Handling Editor: Mahua Choudhury
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Bjørklund, G., Pivina, L. & Semenova, Y. Genetic Polymorphisms in Cardiovascular Disease: Effects Across Three Generations Exposed to Radiation from the Semipalatinsk Nuclear Test Site. Cardiovasc Toxicol 24, 870–878 (2024). https://doi.org/10.1007/s12012-024-09885-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12012-024-09885-y