
Abstract
Rabbits are widely used for the study of atherosclerosis; however, the lack of a unified and quantitative analysis of atheroma limits data interpretation and comparisons between laboratories. In this study, we applied a simple quantitative method, referred to as the oil red O (ORO) dye-eluting method, for analysis of atherosclerotic plaques in freshly isolated aortas. It employs ORO staining of the plaques followed by elution of the dye that is subjected to quantitative measurement. Atherosclerosis was induced in rabbits by feeding a 1% (w/w) high cholesterol diet for 4 or 12 weeks. Thoracic aortas were isolated and sufficiently stained by ORO. These dyes were easily and completely extracted by 100% ethanol and quantified by spectrophotometric measurement at 510 nm. A series of cross-sectional slices at 100-µm intervals were counterstained by elastic van Gieson. It was found that there was a highly positive correlation between the dye concentration and the amount of plaque tissue, determined as volume of plaques (regression coefficient r2: 0.8792, p < 0.001). The color equivalence of the dye content was expressed as µg/mm2 of intimal aorta area to allow direct comparisons among aortas. The color equivalences of ORO content in rabbits fed 12 weeks were almost 5.0 times higher than those fed 4 weeks. Thus, this ORO dye-eluting method is useful for quantification of atherosclerotic plaques in aortas in rabbits, as well as other animal models.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The rabbit model of atherosclerosis is widely used for the study of this disease condition because the lipoprotein metabolism of rabbits is more closely aligned to that of human than to that of rodents [1]. Cholesterol-fed rabbit model has provided the first experimental evidence for “lipid hypothesis” as well as “inflammatory hypothesis” of atherosclerosis [2, 3]. Arterial plaque development in rabbits displays a close similarity to the spontaneously arising atherosclerotic lesion pathology in humans [4]. Therefore, the rabbit model remains one of the preclinical models mainly used not only for basic research, but also for the development of therapeutics [5].
Atherosclerosis is characterized by an increasing retention of lipoprotein in the arterial intima at predilection sites such as aortic arch and thoracic aorta. Large plaques may occlude the vessel lumen and are prone to rupture and thrombosis [6]. Therapies aiming at directly reducing the size of atherosclerotic plaques and opening the luminal stenosis have become a focused approach. In this context, a highly quantitative assessment of atherosclerotic plaques is also in a great demand in preclinical models.
There are several methods to determine and characterize atherosclerotic plaques. One is to use a sequential sectioning of the aorta to determine the cross-sectional lesion area in mice [7, 8]. The aorta was sectioned between the heart and arch aorta at an interval of 64 µm with a total of 64 slices. This method can obtain information about microscopic lesion area, but is labor-intensive and time-consuming. In addition, it cannot generate morphometric data. Another method employs oil red O (ORO), an inert, oil-soluble bis-azo dye, to stain the neutral lipids constituting the fundamental components of atherosclerotic lesions [9]. This method has been commonly used for visualizing the irregular morphology of atherosclerotic plaques in the inner surface [8, 10] of the aorta. In this process, the aorta is opened longitudinally and stained with ORO. Morphological images are captured by a stereoscopic microscope. The quantitative analysis of atherosclerotic lesions en face is expressed as the percentage of lesion area [11]. However, this two-dimensional staining method has been proven to be effective only for the analysis of the presence of atherosclerotic plaques because it can only reflect the surface area, and it cannot distinguish a light lipid deposition from a heavy deposition when the en face surface lesion areas are similar. A quantitative assessment of aortic lesions was also attempted in previous studies [12, 13]. This procedure extracted ORO stained in the lesions followed by quantitative measurement of the ORO extracted from the tissue by spectrophotometry. This procedure was developed in rats [12] and mice [13]. It has not been applied to rabbit model of atherosclerosis. Moreover, more detailed validation of this procedure for measurement of aortic lesions in comparison with the en face has not been provided.
In the present study, we used 1% (w/w) high cholesterol-fed rabbits as an animal model and applied the ORO dye-eluting method to quantitatively analyze the plaques formed in relation to their severity, along with a validation of the procedure by its comparison with a labor-intensive measurement of a series of cross-sections of the lesions. This was a combined procedure, conducted by (1) using ORO dye to bind the lipids and stain the inner surface of atheroma plaques for detailed morphologic examination en face, and (2) quantitatively measuring the ORO contents eluted by 100% ethanol with a spectrophotometer at 510 nm. The same aorta sample was subsequently subjected to a series of cross-sectioning at 100-µm intervals and stained by elastic van Gieson (EVG) to determine the total volume of plaques. The ORO contents measured from the elution were proven to be highly positively correlated to the total volume of atherosclerotic plaques. Thus, this simple ORO colorimetric procedure is applicable for quantitative analysis of atherosclerosis in freshly isolated aortas from rabbits.
Materials and Methods
Animals
Male New Zealand white rabbits at age 10 weeks with initial weight about 2.0 kg were housed individually in metal cages. They were kept in rooms maintained at a 12-h/12-h light/dark cycle as well as constant temperature (22 ± 2 °C) and humidity (50 ± 5%). Rabbits were acclimatized to the laboratory conditions for 1 week. In the first part of the experimentation, ten rabbits were enrolled and assigned into two groups: a control group that received a standard chow diet ad libitum for 12 weeks (n = 5), and a high cholesterol diet (HCD) group that received standard chow diet supplemented with 1% (w/w) cholesterol (Genview, FL, USA) for 12 weeks (n = 5). Cholesterol crystals were dissolved in peroxide-free diethylether, mixed with the diet, and allowed to dry before feeding. Descending thoracic aorta sample between the first intercostal branch and second intercostal branch was collected and used to define the specificity of ORO-binding atheromatous plaques and the sufficiency of extracting from the plaques. In the second part of experimentation, ten rabbits were divided equally into two groups: HCD for 4 weeks (n = 5) or 12 weeks (n = 5). Descending thoracic aorta between the second intercostal branch and third intercostal branch was collected and used for determine the percentage of surface lesion area, color equivalences, and plaque volumes. Different segments of aortas, including descending thoracic aorta between the first intercostal branch and second intercostal branch, and any segment of abdominal aorta, were collected for analyzing the relationship between the volume of plaque lesions and ORO contents bonded to those plaques, or surface lesion area. This experiment was aimed to verify the reliability of the dye-eluting method and determine the color equivalence of thoracic aorta in the two groups. All animal protocols were approved by the Institutional Animal Care and Use Committee at Sichuan University West China Hospital, following the guidelines of the US National Institutes of Health.
Perfusion Process and Microdissection of Intima
After termination of the experiment, rabbits were anaesthetized with sodium pentobarbital solution (1.5 ml/kg intravenously) and were placed in a supine position. The perfusion process was designed by slightly modifying the method of Rutherford [14]. An inguinal incision was made to access the aorta for insertion of a cannula connected to a perfusion apparatus. Rabbits were then perfused with isotonic saline from left ventricle with a 50-ml syringe needle at a rate of 100 ml/minute/kg body weight. When the run-off liquid was clear, the aortas were isolated, then cleaned of muscle, adherent fat, and fascia. Approximately, 1-cm length of descending thoracic aorta between the first intercostal branch and second intercostal branch was taken. The aorta was longitudinally opened along the ventral midline to avoid destroying the integrity of the plaques, and then stained by ORO as described below.
ORO Stain Solution
The ORO stain solution was prepared as described previously [8]. In brief, a 5% solution (w/v) of ORO (Sigma-Aldrich, MO, USA, M.W. 408.495) in 2-propanol (Chengdu Kelong Reagents Ltd., Chengdu, CHN) was prepared by heating the reagents to 56 °C for 1 h followed by filtration through 0.2-µm filter paper at room temperature. A working solution was prepared by diluting the stock solution with deionised water (1:1). Before use, it was passed through 0.2-µm filter paper again.
Determination of ORO Dye’s Maximum Absorbance
Dilutions of ORO (1.5, 2.5, 15, 25 µM, respectively) were prepared with absolute ethyl alcohol (EtOH). A full-wavelength absorption spectrum was determined with a Synergy 2 microplate reader (Bio Tek Instruments, USA). The quartz colorimetric cuvettes were a matched set with 10-mm length.
Standard Concentration Curve
Serial dilutions of ORO working solution (from 1 to 50 µM) were prepared with 100% ethanol. The absorbances were recorded at the wavelength corresponding to the maximal absorbance of ORO. A regression line was derived using a computer program (Graph Pad Prism 6, USA).
Dye-Eluting Method Procedure
This method is a combined approach including ORO dye-staining and ORO dye-eluting procedures. The two procedures are described in detail as follows (Fig. 1).

Detailed procedures of the novel method. a Aorta sample was longitudinally opened along the ventral midline. Lesions were identified as yellowish, slightly raised irregular areas (arrowheads). b After staining by oil red O (ORO) for 1 h at 37 °C, the plaques became red (arrowheads). c Aorta was laid flat on a 3-mm thick wet, freshly cut section of potato and the inner surface of aorta was captured by a stereo microscope. d After staining by ORO, the aorta was put into 100% ethanol for 2 h at 37 °C to completely elute ORO dye. The color of plaques was faded (arrowheads). e The eluted solution which contained ORO was gently well-mixed. f The eluted color was read immediately in a quartz colorimetric cuvette by a microplate reader at 510 nm wavelength. g ORO content was obtained and the color equivalence of the dye was expressed as µg/mm2 of intimal aorta area and can be used to make comparisons between different samples
Step 1: ORO Dye-Staining Procedure
The longitudinal half of fresh aorta was fixed with 4% paraformaldehyde for 10 min. After being washed in deionised water three times, the aorta sample was stained in ORO working solution for 1 h at 37 °C. Subsequent to the staining, the aorta was immersed in 60% 2-propanol for 5 min, and then returned to deionised water [8]. After staining, adventitia was removed carefully. Preliminary studies showed that after being stained by ORO, the adventitia could be separated from intima and media working in physiological saline solution with ophthalmologic surgical instruments. After that, the intima was mounted in water, inner side up, and laid flat on a 3-mm thick wet, freshly cut section of potato. The images of the inner surface of aorta were captured with a Ziess digital camera mounted on a stereo microscope (SteREO Discovery V8, Ziess, GRE).
Step 2: ORO Dye-Eluting Procedure
After the dye-staining procedure, the aorta was placed in a tube filled with approximately 20–80 ml 100% ethanol at 37 °C for 2 h until the tissue was depleted of ORO dye completely. This solution was gently well-mixed, and then read immediately in a quartz colorimetric cuvette with a Synergy 2 microplate reader at ORO’s maximal absorbance. ORO content (µg) was calculated based on the concentration and volume of the EtOH. The color equivalence of the dye was expressed as µg/mm2 of intimal aorta area and can be used to make comparisons between different samples.
Direct Measurement of Atherosclerotic Lesions
In order to validate the dye-staining and dye-eluting method, the aorta was subsequently analyzed by applying serial sectional processing. The aorta was embedded longitudinally in paraffin wax and serially sliced with a microtome at 100-µm intervals. All specimens were cut into 3-µm-thick sections and stained by EVG. Images were captured with a Nikon DXM 1200/NIS-Elements mounted on a light microscope (Nikon Eclipse E600, Shanghai, CHN) and analyzed using Image Pro Plus 6 (IPP software, Houston, TX). The total volume of lesions in mm3 could be obtained as ∑[cross-sectional lesion area (mm2) × interval thickness (mm)]. Thus, the correlation between ORO contents bound to the plaques and the total volume of atherosclerotic lesions was revealed. Also, a regression line was derived using Graph Pad Prism 6.
Histological Analysis
The paraffin-embedded aortas were cut into 3-µm-thick sections and deparaffinized. For microscopic evaluation of cross-sectional plaque area, EVG staining was performed. The staining process was performed as described previously [8, 15, 16]. For microscopic evaluation of the total collagen contents and cellular components of the lesions, deparaffinized sections were stained by sirius red (SR) [17] or immunohistochemically stained with mouse monoclonal primary antibody against rabbit α-smooth muscle actin (1:50; HHF-35; C34931, Enzo, NY, USA) and macrophages (1:400; CD68; M0633, Dako, Carpinteria, CA). The immunohistochemical procedures were described previously [18]. The second antibody was SignalStain® Boost IHC Detection Reagent (8125, CST, Danvers, MA). All sections were visualized with SignalStain® DAB Substrate Kit (8059S, CST, Danvers, MA).
Statistics
Data are presented for continuous variables as mean ± standard error of mean (SEM). The two groups were compared using Student’s t test. Two-tailed bivariate correlations were estimated with Pearson’s coefficient. All analyses were conducted using standard statistical software (SPSS 25.0, NY, USA). Differences are considered statistically significant at the p < 0.05 level. All figures were constructed using GraphPad Prism 6.0 Software (GraphPad Software, USA).
Results
Determination of ORO Dye’s Maximal Absorbance
Different concentrations of ORO solutions (1.5, 2.5, 15, 25 µM, respectively) all demonstrated the same maximal absorbance at 510 nm wavelength (Fig. 2a). Thus, a wavelength of 510 nm was used for all measurements.

Determination of ORO’s maximal absorbance and standard concentration curve. a Absorption spectra of ORO at concentration of 15 µM under full-wavelength condition were determined with a microplate reader. b The standard concentration curve showed a direct, linear, concentration-dependent increase in absorbance from 1.0 to 50 µM. c Absorption spectra of 100% ethanol under full-wavelength condition were determined with a microplate reader
Standard Curve of ORO Concentrations
The standard curve for ORO solutions at 510 nm wavelength is displayed in Fig. 2b. The curve shows a linear, concentration-dependent increase in absorbance from 1.0 to 50 µM (the regression coefficient r2 was 0.9997, p < 0.0001).
Specificity of ORO Binding to Atheromatous Plaques
En face aortas in the control group showed a rather light, flesh-colored intima. No ORO staining was observed near branch points in the normal aortas. However, aortas in the HCD group displayed intimal lesions of subendothelial, red, grape-like clusters, while the lesion-free areas were free of ORO (Fig. 3a). The lesions are preferentially located near branch points.

Elution of ORO specifically bonded to atheromatous plaques by 100% ethanol en face (a) or cross-sectional (b). a Aortas were longitudinally opened in the control group and HCD group. In the control group, no plaques were found near branch points (blue arrowheads). In the HCD groups, the lesions were preferentially located near branch points (yellow arrowheads). Images were captured at 10×; scale bar = 1000 µm. b Cross-sectional aortas from control group (the upper layer) and HCD group (the bottom layer) were compared. The aorta was folded back to back and formed a sandwich structure. The white dashed lines indicate the border of intima and media. After ORO-staining procedure, the intima was free of ORO (blue arrowheads) in control group, but the plaques in the HCD group had been stained sufficiently with ORO and turned to orange (yellow arrowheads). Images were captured at 20×; scale bar = 500 µm. ORO oil red O; HCD high cholesterol diet; I intima; M media
To further define whether ORO was specifically bound to fatty streaks in the freshly isolated aortas, and whether all plaques were completely stained with ORO, cross-sections of aortas from HCD group and control group were compared (Fig. 3b). The aorta was folded back to back and formed a sandwich structure. Before being stained, the intima from HCD group was thicker compared with control group under a stereomicroscope. There is no clear boundary between the intima and the media. During the dye-staining process, it was observed that the intima in the control group was free of ORO. However, in the HCD group, fatty streaks were mainly confined to the intima. Thus, intimal lesions from the HCD group were stained by ORO and became red (Fig. 3b). When the media was infiltrated by neutral lipids, the media would be colored.
ORO Elution from Atheromatous Plaques
The amount of EtOH used to elute ORO bound to the plaques was determined by the extent of atherosclerosis which was evaluated by the en face ORO-staining method. When the freshly isolated aortas with plaques were destained in the EtOH, the color of the EtOH solution of ORO increased in intensity with time. After 2 h at 37 °C, the ORO was completely eluted by EtOH, which was easily judged by visual inspection of the colorless aorta after quantitative extraction of ORO (Fig. 3a, b).
After the entire process, the aorta was subjected to formalin fixation and paraffin embedding for further histologic and immunohistochemical analyses. The purpose of immunohistochemistry analysis was to prove that the detection of collagen or cellular components in the aorta was unaffected by the extraction. Immunohistochemistry analysis identified the cellular components, including smooth muscle cells and macrophages in the lesions (Fig. 4).

Histologic analysis of aortas following ORO dye-eluting process. Aortas from rabbits fed HCD for 12 weeks were re-stained by elastic van Gieson (EVG), or sirius red (SR), and immunohistochemically stained with HHF-35 antibody for rabbit smooth muscle cells (SMC) or RAM11 for macrophages (MØ). Each slice was captured at 400×; scale bar = 50 µm
Determination of the Color Equivalence of ORO
Solutions containing different concentrations of ORO were scanned and the relative maximal absorbances at 510 nm wavelength were determined by a Synergy 2 microplate reader. The corrected absorbance of ORO was obtained by subtracting 100% EtOH interference, although 100% EtOH has little interference with ORO at 510 nm wavelength (Fig. 2c). A color equivalence of ORO was expressed as ORO content per intimal area (µg/mm2) to allow direct comparisons among aortas. Representative EVG images of aortas from rabbits in control, HCD 4 weeks, and HCD 12 weeks groups are presented in Fig. 5a. The ORO-stained areas were 4.8 times higher in animals fed HCD for 12 weeks than those fed HCD for 4 weeks (Fig. 5b), while the color equivalences of dye were 5.0 times higher in animals fed HCD for 12 weeks than those fed HCD for 4 weeks (Fig. 5c). Serial cross-section measurements of the plaque volume by EVG staining were 5.1 times higher in HCD-fed rabbits at 12 weeks than those at 4 weeks (Fig. 5d).

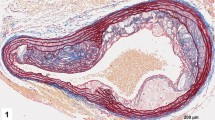
Determination of percentage of lesion area and color equivalences. a Representative EVG images of aortas from rabbits in control group, HCD 4 weeks group, and HCD 12 weeks group. Internal elastic lamina was stained in black (yellow arrowhead) and the plaque was formed in the intima (star). Images were captured at 200×; scale bar = 100 µm. b ORO-staining method showed that the percent of surface lesion area was 4.8 times higher in HCD-fed rabbits at 12 weeks of feeding than those fed HCD for 4 weeks. c ORO dye-eluting method showed that the color equivalences were almost 5.0 times higher in HCD-fed rabbits at 12 weeks of feeding than those fed HCD for 4 weeks. d. Serial cross-section measurements of the plaque volume by EVG staining were 5.1 times higher in HCD-fed rabbits at 12 weeks of feeding than those fed HCD for 4 weeks. Number in each group: control rabbits (n = 5), HCD-fed rabbits for 4 weeks (n = 5), or 12 weeks (n = 5). Data are expressed as mean ± SEM (*p < 0.05; **p < 0.001)
Validation of the Dye-Eluting Method
To validate that the amount of ORO bound to the plaques can quantitatively represent the volume of the plaques, the total volumes in mm3 of plaque lesions obtained by EVG were compared with the amount of ORO content. The aorta was serially sliced at 100-µm intervals, then each slice was stained by EVG to confirm the cross-sectional lesion area. The total volumes of plaque lesions in mm3 were obtained by ∑[cross-sectional lesion area (mm2) × interval thickness(mm)]. To reveal whether this method can be applied to different stages of atherosclerosis, early and advanced atherosclerotic descending thoracic or abdominal aortas (HCD for 4 or 12 weeks, respectively) were collected and analyzed as described previously. The results showed that for fatty streak plaques, the amount of ORO bound to the plaques has a strong positive correlation with the total volume of plaques in mm3, determined as described above (the regression coefficient r2 was 0.8792, p < 0.001) (Fig. 6a). A linear correlation curve was also constructed between the percent of surface lesion area and plaque volume. The regression coefficient r2 was 0.4311, p = 0.019 (Fig. 6b).

Linear correlations for ORO contents and the lesion volumes or the percentage of surface lesion areas and the plaque volumes. The regression coefficient r2 was 0.8792 in the linear curves of ORO bonded to plaques and plaque volumes (a), and was 0.4311 in the linear curves of percentage of surface lesion area and plaque volumes (b)
Discussion
Rabbits are sensitive to dietary cholesterol and develop severe hypercholesterolemia rapidly, resulting in aortic atherosclerosis. Because they share a similar lipid metabolism with humans, they are often used as an animal model for the study of pathogenesis of atherosclerosis [1]. The early and major locations of atherosclerotic plaques were found to be ascending thoracic aorta, aortic arch, and descending thoracic aorta in rabbits [1]. A method to assess the plaques in the rabbit thoracic aorta has been described by Koike et al. [19], using Sudan IV to evaluate the gross lesion area en face and EVG to determine the cross-sectional microscopic lesions. This procedure requires sectioning the rabbit’s thoracic aorta into several 1-cm interval segments for cross-sectional microscopic quantification. As the plaques were asymmetric and irregularly distributed in the aorta, it was difficult to generate precise quantitative information from these roughly dissected segments. Lin et al. [8] applied a method of serial cross-sectioning at 64-µm intervals to measure the aortic roots in apoE−/− mice. This method can avoid the bias mentioned above, but since a total of 64 sequential slices was made for a 4–5 mm length of aortic root, it is a labor-intensive and time-consuming method for medium-sized animals like rabbits.
Compared with the inaccuracy of the first method and the high labor-intensity of the second method mentioned previously, a simple ORO-staining and extraction procedure for quantitation of aortic lesions was developed previously in rats and mice [12, 13]. However, this procedure has not been applied in the rabbit model, and furthermore, this procedure was not fully validated. The study described here presents the application of the simple ORO-staining and extraction procedure for quantitation of atherosclerotic plaques in rabbits with a detailed validation. ORO, an azo dye similar to Sudan IV, has been widely used in assessing atherosclerotic plaques en face [20,21,22]. The key assumption of this method is that ORO can specifically and sufficiently bind to the plaques, as was validated by the results obtained in the present study. The en face ORO-staining procedure enables an identification of the location and extent of the atherosclerotic plaques in freshly isolated aortas [13, 21], but the en face ORO method cannot distinguish a light lipid infiltration from a heavy lipid deposition. It is of insufficient accuracy to evaluate the severity of atheroma plaques. After the ORO stain was eluted and measured by spectrophotometry, the ORO staining and measurement become more reliably quantitative.
The result presented here provides critical validation of this simple procedure for quantitation of atherosclerotic plaques. The spectrometric measurements of the ORO were compared with the serial cross-sectional measurements of the volume of plaques. Through this comparison, a high correlation between the simple measurement of ORO by spectrometry and the labor-intensive measurement of the volume was revealed. In addition, a meaningful measurement was presented as the color equivalence of ORO dye was corresponded to the severity of atherosclerosis, as indicated by a much higher readout in rabbits fed high cholesterol for 12 weeks than that for 4 weeks.
A further analysis also revealed that the ORO elution and spectrometric procedure are not only simple and time-saving, but also provide more accurate quantitative assessment of atherosclerotic lesions than the labor-consuming, serial cross-sectioning, and staining procedure of atherosclerotic plaques. As presented in the present study, the regression coefficient for the ORO procedure was 0.8792 (p < 0.001) but that for the percent of surface lesion area and plaque volume was 0.4311 (p = 0.019). This further defined the advantage of the simple ORO elution and spectrometric procedure over other existing procedures.
In conclusion, there are several advantages in this method: (1) the location of plaques, the extent of en face lesion areas, and the volume of plaques per intima can be measured in one aorta sample; (2) the whole staining and eluting procedure is rapid, requiring only 3 h; and (3) after the dye elution analysis, the aorta is available for further histopathological analyses. The detection of collagen or cellular components in the aorta was unaffected by the extraction.
Therefore, the method described here is suitable for the study of atherosclerosis in rabbit model. Due to the fact that ORO was bonded to neutral lipids, the method was designed to evaluate fatty streak lesions volumes. Fibroatheroma and fibrocalcific plaques have calcification or ulcers may not suitable for this method. This is an end-point measurement. Its combination with currently available molecular imaging probes can expand the analytic capacity for understanding the progression and severity of atherosclerosis in rabbit models. Thus, the method presented here will help to make further insights into atherosclerosis in a quantitative manner.
References
Fan, J., Kitajima, S., Watanabe, T., Xu, J., Zhang, J., Liu, E., & Chen, Y. E. (2015). Rabbit models for the study of human atherosclerosis: from pathophysiological mechanisms to translational medicine. Pharmacology & Therapeutics, 146, 104–119.
Steinberg, D. (2004). Thematic review series: the pathogenesis of atherosclerosis. An interpretive history of the cholesterol controversy: part I. Journal of Lipid Research, 45, 1583–1593.
Hansson, G. K., Seifert, P. S., Olsson, G., & Bondjers, G. (1991). Immunohistochemical detection of macrophages and T lymphocytes in atherosclerotic lesions of cholesterol-fed rabbits. Arteriosclerosis and Thrombosis: A Journal of Vascular Biology, 11, 745–750.
Hong, M. K., Vossoughi, J., Mintz, G. S., Kauffman, R. D., Hoyt, R. F. Jr., Cornhill, J. F., … Hoeg, J. M. (1997). Altered compliance and residual strain precede angiographically detectable early atherosclerosis in low-density lipoprotein receptor deficiency. Arteriosclerosis, Thrombosis, and Vascular Biology, 17, 2209–2217.
Wang, Y., Bai, L., Lin, Y., Chen, Y., Guan, H., Zhu, N., … Liu, E. (2015). Combined use of probucol and cilostazol with atorvastatin attenuates atherosclerosis in moderately hypercholesterolemic rabbits. Lipids in Health and Disease, 14, 82.
Bentzon, J. F., Otsuka, F., Virmani, R., & Falk, E. (2014). Mechanisms of plaque formation and rupture. Circulation Research, 114, 1852–1866.
Paigen, B., Morrow, A., Holmes, P. A., Mitchell, D., & Williams, R. A. (1987). Quantitative assessment of atherosclerotic lesions in mice. Atherosclerosis, 68, 231–240.
Lin, Y., Bai, L., Chen, Y., Zhu, N., Bai, Y., Li, Q., … Liu, E. (2015). Practical assessment of the quantification of atherosclerotic lesions in apoE(−)/(−) mice. Molecular Medicine Reports, 12, 5298–5306.
Weber, C., & Noels, H. (2011). Atherosclerosis: current pathogenesis and therapeutic options. Nature Medicine, 17, 1410–1422.
Littie, R. D. (1944). Various oil soluble dyes as fat stains in the supersaturated isopropanol technic. Stain Technology, 19, 55–58.
Zhang, C., Zheng, H., Yu, Q., Yang, P., Li, Y., Cheng, F., … Liu, E. (2010). A practical method for quantifying atherosclerotic lesions in rabbits. Journal of Comparative Pathology, 142, 122–128.
Nunnari, J. J., Zand, T., Joris, I., & Majno, G. (1989). Quantitation of oil red O staining of the aorta in hypercholesterolemic rats. Experimental and Molecular Pathology, 51, 1–8.
Beattie, J. H., Duthie, S. J., Kwun, I. S., Ha, T. Y., & Gordon, M. J. (2009). Rapid quantification of aortic lesions in apoE(−/−) mice. Journal of Vascular Research, 46, 347–352.
Rutherford, C., Martin, W., Carrier, M., Anggard, E. E., & Ferns, G. A. (1997). Endogenously elicited antibodies to platelet derived growth factor-BB and platelet cytosolic protein inhibit aortic lesion development in the cholesterol-fed rabbit. International Journal of Experimental Pathology, 78, 21–32.
Yu, Q., Li, Y., Wang, Y., Zhao, S., Yang, P., Chen, Y., Fan, J., & Liu, E. (2012). C-reactive protein levels are associated with the progression of atherosclerotic lesions in rabbits. Histology and Histopathology, 27, 529–535.
Otto, C. M., Kuusisto, J., Reichenbach, D. D., Gown, A. M., & O’Brien, K. D. (1994). Characterization of the early lesion of ‘degenerative’ valvular aortic stenosis. Histological and immunohistochemical studies. Circulation, 90, 844–853.
Xie, C., Ma, B., Wang, N., & Wan, L. (2017). Comparison of serological assessments in the diagnosis of liver fibrosis in bile duct ligation mice. Experimental Biology and Medicine, 242, 1398–1404.
Xiao, Y., Nie, X., Han, P., Fu, H., & Kang, J., Y (2016). Decreased copper concentrations but increased lysyl oxidase activity in ischemic hearts of rhesus monkeys. Metallomics: Integrated Biometal Science, 8, 973–980.
Koike, T., Kitajima, S., Yu, Y., Nishijima, K., Zhang, J., Ozaki, Y., … Fan, J. (2009). Human C-reactive protein does not promote atherosclerosis in transgenic rabbits. Circulation, 120, 2088–2094.
Gao, B., Li, L., Zhu, P., Zhang, M., Hou, L., Sun, Y., … Gu, Y. (2015). Chronic administration of methamphetamine promotes atherosclerosis formation in ApoE−/− knockout mice fed normal diet. Atherosclerosis, 243, 268–277.
Hu, J. H., Touch, P., Zhang, J., Wei, H., Liu, S., Lund, I. K., Hoyer-Hansen, G., & Dichek, D. A. (2015). Reduction of mouse atherosclerosis by urokinase inhibition or with a limited-spectrum matrix metalloproteinase inhibitor. Cardiovascular Research, 105, 372–382.
Kamkar, M., Wei, L., Gaudet, C., Bugden, M., Petryk, J., Duan, Y., … Ruddy, T. D. (2016). Evaluation of Apoptosis with 99mTc-rhAnnexin V-128 and inflammation with 18F-FDG in a low-dose irradiation model of atherosclerosis in apolipoprotein E-deficient mice. Journal of Nuclear Medicine, 57, 1784–1791.
Acknowledgements
The authors wish to acknowledge Mr. Zhenghui Luo, Ms. Jingyao Zhang, and Ms. Shan Zhao for their technical assistance.
Author information
Authors and Affiliations
Contributions
All authors participated in conceive, design, and review of the manuscript; LJZ carried out the ORO, EVG, SR, and immunohistochemistry staining. LJZ, YX, and XM analyzed the data and interpreted the results; NW performed the sequential sectioning process; LJZ wrote the draft of the manuscript and YJK edited, revised, and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared that no competing interest exists.
Rights and permissions
About this article

Cite this article
Zhao, LJ., Xiao, Y., Meng, X. et al. Application of a Simple Quantitative Assessment of Atherosclerotic Lesions in Freshly Isolated Aortas from Rabbits. Cardiovasc Toxicol 18, 537–546 (2018). https://doi.org/10.1007/s12012-018-9465-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12012-018-9465-z