
Abstract
Leishmaniasis is a protozoal disease declared as an endemic in areas suffering from severe malnutrition and poverty. The factors associated with poverty like low income, ecological factors, and malnutrition cause disruption in immunity and host defense increasing risk of infection. Altered resistance to infection and host susceptibility are associated with low micronutrient levels in undernourished patients. Malnutrition has been recognized as a poor predictive marker for leishmaniasis, in particular the deficiency of trace elements like zinc, iron, and vitamin A, B, C, D which has a prominent function in the regulation of innate and adaptive immunity, cell proliferation, human physiology, etc. Malnourishment can exacerbate host sensitivity and pathophysiologic intensity to infection in variety of ways, whereas infection can enhance underlying poor nutrition or enhance host vulnerability and sandfly's urge to attack specific hosts. The intensity of leishmaniasis can be influenced by body mass and micronutrient availability in the blood. Vitamin D, C, zinc, and iron are proved effective in inhibiting the growth of leishmaniasis in both amastigote or promastigote forms, either directly or by acting as precursor for a pathway which inhibits the parasite growth. This article elucidates a new perception to the crucial role of micronutrients and their probable role in the therapeutic outcomes of leishmaniasis. Since there is requirement of novel drugs to fight drug resistance and relapse of leishmaniasis, this article may pave way to understand the importance of micronutrients and their role in therapeutic outcomes of leishmaniasis.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Leishmaniasis is caused by a group of leishmania parasites, it is further transmitted to humans through infected phlebotomine sand fly. The subtropical and tropical environments are hubs where the sand flies carrying parasite are developed [1]. [2] There are combinedly three different manifestations of leishmaniasis; visceral leishmaniasis, post-kala-azar dermal leishmaniasis, or cutaneous leishmaniasis; and mucocutaneous leishmaniasis. Visceral leishmaniasis being the deadliest among all the other manifestations accounts for majority of deaths. Due to its restricted reach and occurrence in isolated areas, the infection may go unnoticed from the official sources along with many other topical diseases. Untreated, visceral leishmaniasis (VL) may lead to death; however, the huge number of deaths are due to untreated leishmaniasis [3]. Micronutrients on the other hand are inorganic trace minerals and organic vitamins that are only required in limited amounts but are essential for physiological functions. Micronutrients play a vital role in metabolism, as cofactors in gene transcription, tissue function, and regulation of body’s defense system [4]. Low serum levels of micronutrients may be observed in individuals due to malnutrition, poverty, effect of inflammation, and response of the body to physiological stress. Furthermore, certain factors such as smoking, alcohol consumption, family size, and comorbidities like human immunodeficiency virus infections affect serum iron, zinc, vitamin A, and vitamin D levels. The assessment of micronutrient levels in patients with infection is crucial considering factors such as disease severity, medication use, nutritional status, and other medical interventions are depend on them [5]. Deficiency of iron causes microcytic anemia with impaired immune and endocrine function. Adequate zinc levels are required for immune function and deficiency of which may cause diarrhea and acute respiratory infections [6]. According to WHO, around 14 billion individuals are obese and around 462 million adults are underweight. National family health survey-5 of 2019–21 states that in India where leishmaniasis is declared endemic, around 18.7% of the women and 16.2% of men have BMI less than 18.5 kg/m2, around 67.1% of the children are anemic and 35.5% of children are stunted [7, 8]. Few clinical studies have elucidated the correlations between low serum micronutrient levels in patients with visceral leishmaniasis and their effect on the treatment outcomes. [9] Malnutrition not only increases the host's vulnerability to leishmaniasis infection, but it also influences the intensity of disease, manifesting as a range of physical abnormalities, many of whom involved etiologic pathways in both malnutrition and overnutrition. The abnormalities such as reduced development and growth in adolescents; abnormal metabolism; chronic inflammation; and abnormal nutritional absorption. [10]Considering the knowledge gap in this area this article sheds a new light into the importance of micronutrients and trace elements and their role in immunology, patient outcomes, physiology of leishmaniasis. This article further paves a way to conduct robust research by exploring novel possibilities to cover the research gaps and address challenges like the resistance and relapse of the infection, in undernourished patients. Furthermore, this article may help in developing evidence-based strategies related to malnutrition and trace elements, which may be implemented in eradication program of Leishmaniasis.
Materials and Methods
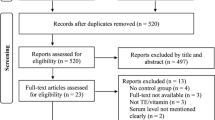
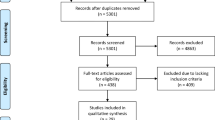
This narrative review was carried out by retrieving literature using the vocables such as vitamins, micronutrients, malnutrition, immunity, leishmaniasis in the bibliographic databases such Scopus, PubMed, and Google Scholar. The language filters were used as criteria for opting literature, and publications in English were considered. In vitro and in vivo studies, review literature, systematic review, and meta-analysis, were included. Unpublished, fragmentary, or only partially available data, as well as literature in several languages, were omitted. The majority of the material included in this narrative is of recent times, but earlier material as far up to 1968 is also included if it was relevant and required. There was no financial assistance from any organizations, and all of the literature is available for free download.
The Effect of Malnutrition in Leishmaniasis
Leishmaniasis is a vector-borne infection that has infected animals and humans for centuries. In pathogen defense, the nutritional condition of the host is highly critical as it holds a key role in regulation of human immune system. Asymptomatic infections and perhaps even serious diseases are caused by the disorganization of the human defense system as a result of malnutrition. Seroprevalence is still the most common way to correlate nutrition to Leishmania infection or any other infection and sensitivity in living organism habitats. Recent studies have shown correlations with malnutrition and the infection of leishmaniasis, risk of mortality, and morbidity of the disease. In southern Ethiopia, there was a 5.8% increased risk of getting infected with leishmaniasis in population with body mass index < 18. The same was noticed in northwest Ethiopia and other regions with threefold increased chance of getting infected with visceral leishmaniasis [10, 11]. Malnourishment can exacerbate host sensitivity and pathophysiologic intensity to infection in a variety of ways, whereas infection can enhance underlying poor nutrition or enhance host vulnerability. The sensitivity and intensity of leishmaniasis can be influenced by body mass and micronutrient availability in the blood. Nutrition influences not just the host's vulnerability, but also the sandfly's urge to attack specific hosts. Nutritional stress, in addition to host defensive mechanisms, has a significant impact on host-seeking behavior and vector competency, particularly during larval growth. The nutritional status of the parasite's host and sandfly vector could possibly have an impact on its growth [12].
The variables that determine the leishmaniasis susceptibility and advancement are vaguely explored, although some information implies that malnourishment is one of the major risk factors for the onset of leishmaniasis in children. According to epidemiological studies, malnourished hosts have a higher incidence of Visceral leishmaniasis [13] and a ninefold greater incidence of VL was observed in children with Protein-energy malnutrition varies from moderate to severe degree. [14] Malnutrition has been established as a potential cause in both children and adults developing serious illnesses and dying from VL. [15] Visceral leishmaniasis triggered by malnutrition is more prevalent in displaced and impoverished communities. [16]
The nutritional health of the host may be harmed by the intestinal parasite's increasing energy needs or by particular behaviors including commensal bacteria like Ascaris lumbricoides obstructing the absorbing layer of the mucosa, continuing the loss of blood from schistosomiasis [17]. Intestinal parasitosis tends to predispose certain patients to the emergence of persistent VL by suppressing cell-mediated immune responses. [18] Among VL patients, intestinal parasite infestation was reported to be substantially related with chronic malnutrition. Individuals with Visceral Leishmaniasis with more than one intestinal parasitic infections were threefold more likely to be seriously malnourished than those who didn't. Malnutrition caused by intestinal parasitosis can be caused by the parasite's own dietary demands, mature worms limiting the mucosa's absorbing surface, and continuing blood loss from hookworm infections and/or schistosomiasis. [14]
At molecular and cellular levels, the mechanistic association among malnutrition and the progression of VL is rarely discussed. A detailed understanding of those systems could open up new avenues for dietary prophylaxis and therapeutic management. Furthermore, the risk of being infected with various diseases associated with malnutrition, comprehending the interaction of micronutrients and their immune function is of particular relevance. Earlier research findings have used an animal model of starvation to replicate the developmental characteristics of humans’ weanling nutrition, [19] Early diffusion of Leishmania donovani (after three days of infection) to the visceral organs (liver and spleen) may be accelerated due to malnutrition caused by loss barrier function of the lymph node. The role of lymph nodes as a barrier to pathogenic spread is based on the pathogen's entrapment via phagocytes (primarily dendritic cells and macrophages). The pathogen's movement is limited through the node due to the exclusion size qualities of nodal anatomy [20, 21]. The innate and adaptive immune reaction development that destroys the parasite is then facilitated by this barrier functioning. The principle of lymph node barrier function has received a lot of attention in the domain of tumor metastasis control, but it has received less attention in the field of infectious disorders[22] The nutrition status may be considered to analyze the risk of infection in the endemic areas and develop public policies and strategies to restrict the disease in endemic areas.
Leishmaniasis and Micronutrients
Globally, extreme malnutrition is by far the most common trigger of immunodeficiency. Severe protein-calorie malnutrition affects the immune system's humoral and cellular arms, altering and reducing immunological-competent cell proliferation and activity, cytokine release, and antigen detection capacities [23, 24]. Micronutrients and minerals only needed in small quantities but are critical for healthy physiological functions. Many essential metabolic enzymes need them as cofactors. They improve immune system function and control gene transcription [4, 25]. Obesity, and diet-related chronic illnesses are all linked to the lack of vitamins and minerals. Malnutrition, in any of its manifestations, refers to excesses, shortages, or disparities in host’s energy or nutrient intake, and includes undernutrition in a wide sense. Infection and malnutrition have always had a complicated relationship, for centuries, nutrition and infection have interacted in individuals, with malnutrition raising susceptibility to infectious pathogens and aggravating their pathogenicity [26].
In past years, the link between leishmaniasis and cancer has been emphasized in both animal models and humans. The effects of VL and micronutrient deprivation are not restricted to infected individuals and their families; they also have an influence on a country's socioeconomic growth [27, 28]. Patients with leishmaniasis had low levels of micronutrients in their blood. The anti-leishmaniasis medication raises serum iodine and selenium levels significantly, but not serum iron, zinc, vitamin A, or vitamin D levels. Micronutrient levels in the blood have an important impact on the treatment of visceral leishmaniasis [9]. Apart from nutritional sustenance for visceral leishmaniasis patients throughout treatment, an aid organization in southern Sudan called Medicine-Sans-Frontiers has stressed the benefits of high-calorie nutrient supplementation and vitamin supplementation (vitamins C and A, as well as multivitamins) for many years. [28]
Cell-mediated immunity reduction is correlated with serum levels of iron, zinc, vitamin A, and other micronutrients. Vitamin A can play multiple roles in immune response modulation throughout VL infection, according to research conducted in an endemic area of northeast Brazil. Children with exposure to the antigens of Leishmania had shown increase in Treg and monocyte interlukin-10 expression and immunoregulatory responses. [29] Poor nutritional conditions which are considered as malnutrition may further lead to Cutaneous leishmaniasis infection [30]. A vast number of micronutrients regulate both innate and adaptive immunity, and possess pivotal roles in disease diagnosis, progression, and treatment outcome (Table 1). These micronutrients can be used as dietary prophylaxis to improve treatment efficacy and improve overall quality of life.
Micronutrient-Induced Immunity in Leishmaniasis
The human body endures enormous infections on daily basis, the biological system is highly and precisely regulated, integrated with the system of tissues and molecules that shields the recipient against contagious and harmful pathogens. The body uses two basic protective pathways to identify and neutralize harmful entities such as innate immunity and acquired/ active immunity. [31, 32] Many studies have shown that dietary deficit is linked to poor immunological functioning, including phagocyte activity, cell-mediated defense, antibody creation, and cytokine generation. The immune system dysfunction is caused by a lack of critical fatty acids, trace minerals such as calcium, sodium, iron, and vitamin A [33], B, C [34], D[35], E, etc. in addition to protein deprivation.
Immune cells rely on biological cell membrane fluidity for multiple defensive tasks. Lipid peroxidation clearly impairs membrane fluidity, which has a negative impact on immunological activities. Antioxidants are critically vital for proper functioning of defense system [31]. In an in vitro model of corneal endothelial cells, the lipid peroxidation was inhibited by a combination of vitamins C and E tocopherol /ascorbic acid, or a single intake of vitamin A /retinoic acid. Furthermore, anti-oxidative vitamin C supplement intake dramatically reduces the formation of oxidative damage induced by free radicals [36]. Oxidative stress and increased damage to DNA have been found in individuals with cutaneous leishmaniasis, as well as the individual's defense strategy of producing reactive oxygen species (ROS) and reactive nitrogen species (NOS) may augment the leishmanicidal potential in individuals with CL. These metabolites, on the other hand, not only destroy the pathogen, but also induce oxidative damage in cells which are not infected [37]. The importance of these micronutrients has been emphasized in various other infectious diseases such as COVID-19. [38] The conclusive evidence suggests that the deprived immune function due to the deficiency of micronutrients may also further affect patient outcomes in terms of treatment efficacy, disease progression, etc.
Vitamin A
Vitamin A is an integral micronutrient which was first identified nearly a century ago by McCollum and Davis who claimed in 1913 showing feeding rats an ether preparation from egg yolk or butter, but not lard or olive oil, over many months started to regain development in rats [39]. Vitamin A plays both stimulating and regulatory functions in both the nonspecific/innate and specific/adaptive immunity, allowing to improvise immune functions and offer better protection to hostile infections (Fig. 1) [39, 40].

Effect of Micronutrient vitamin A in leishmaniasis. Vitamin A absorption is decreased in Visceral leishmaniasis patients which causes deficiency, further leads to visceral leishmaniasis progression, non-healing clinical patterns, increased regulation of inflammatory cytokines
Vitamin A has a prominent function in physiological, immunological balance in human body. Deficiency of vitamin A was linked to increased production of IL-10, [41, 42] and mainly targets to disrupt Th1 memory cellular immune response, additionally, IL-10 producing Th2 are also affected [43]. A study elucidated that in monocytes isolated from healthy individuals, Tretinoin (all-trans retinoic acid) spiked IL-10 and transforming growth factor in regulatory T-cells and also IL-10 in monocytes. Whereas in case of leishmania antigens with all-trans retinoic acid on administration prevented escalated regulation of IL-10 and soluble Leishmania antigen (SLA) stimulus by cells isolated with Visceral Leishmaniasis patients. This shows the dual characteristics of vitamin A in the regulation of immune response and decreased regulation of interleukin-10 expression in monocytes and Treg cells during visceral leishmaniasis [44].
The vitamin A deficiency mainly disrupts T helper type 1 (Th1) cell immune response, Furthermore, elevated arginase production in malnourished mice's monocytes and macrophages has been attributed to a more favorable setting for Leishmania development; similarly, low serum vitamin A levels and micronutrients in children with VL compared to their non-infected counterparts. In the efficient leishmaniasis management and chronicity prevention, immunological pathways play a vital role. Due to the divergence of immune response against T cells because of the decreased levels of vitamin A this has led to deficiency state in the body resulting in non-healing clinical pattern [45]. Immunity tends to be improved by intake of nutrients [46, 47]. A closer relationship of immune response to medication treatment has been observed to have enhanced treatment and reduced ailment [48]. As a result, if taken in conjunction as adjuvant therapy, effect of medication therapy might eventually be improved [49]. The key role of vitamin A in patient outcomes, such as disease severity and disease progression needs more exploration to elucidate the importance of the micronutrient in leishmaniasis.
Vitamin B
The discovery of riboflavin(vitamin B2) as a yellow colored pigment present in milk was done by Blyth in 1872[50] but it was not until 1930 that the vitamin property of this pigment was established [51]. Vitamin B 2 (riboflavin) is an essential micronutrient with well-versed pharmacokinetic and toxicological outlines [52,53,54]. Riboflavin can quickly cross lipid membranes and intercalate with nucleic acids without being specific. Along with the degradation of guanine residues and the production of ROS, riboflavin induces alteration in the nucleic acid found in pathogens and white blood cells when exposed to light. The pathogen nucleic acids in the blood samples going through this process are not able to duplicate due to photochemical processes [55]. Unlike microorganisms, blood does not contain nucleic acid in any of the materials that are useful for transfusion. Inactivation of bacterial, viral extracellular, and intracellular pathogens in concentrates of platelets has been achieved using this process [56,57,58,59]. Folate (vitamin B9) is essential for the synthesis of nucleic acids and proteins. T lymphocyte proliferation in response to mitogen activation and the proportion of circulating T lymphocytes were both reduced in deficiency states [45]. In 2011, Gazanion and colleagues published a report on the effects of combination therapy on Leishmaniasis. They discovered that nicotinamide, also known as vitamin B9, had anti-leishmania effects [60]. Hemophagocytic syndrome, triggered by the aggregation of benign hemophagocytic histiocytes in the bone marrow, has been identified rarely in association with Visceral leishmaniasis and pseudomonas septicemia, irrespective of the fact that Leishmania bodies may be detected by liver biopsy [61]. Dysplasia of hematopoietic cells which is caused due to deficiencies of vitamin B12 and folate may cause some dysplastic anomalies, in addition to hemophagocytosis [62]. Vitamin B needs further animal and epidemiological research to establish its key role in this disease.
Vitamin C
Adequate vitamin C concentration in serum is required for robust, well-functioning mechanism of host defense. Vitamin C is known to improve immune functioning, tissue repair, wound healing, growth, and development of tissues. Vitamin C therapy of healthy individuals increased innate immune cell activity, lymphocyte proliferation, and chemotaxis in clinical investigations (Fig. 2) [63,64,65]. Dehydroascorbic acid is carried into erythrocytes, where it is converted via a GSH-dependent process into ascorbate. Vitamin C (ascorbic acid) is a potent antioxidant, which interacts quickly with an extensive range of oxidants, including relatively slow-reacting superoxide anion radical. [66] Vitamin C is one of the most potent reducing agents and free radical scavenger of oxygen-derived species like hydroxyl radical, singlet oxygen. [67] H2O2 is highly effective and acts as toxic to Leishmania donovani and Leishmania tropica species [68]. H2O2 inhibited the proliferation of promastigotes of Leishmania donovani by 94% and thymidine and uracil inclusion by 95 and 97%, accordingly, at a concentration of l0−4 and 10–3 M. The continuous production of H2O2 by glucose–glucose oxidase suppressed promastigote proliferation significantly. The growth-inhibitory effect was entirely eliminated when catalase was added. [69, 70] Several disorders have been linked to increased lipid peroxidation and lowered antioxidant defenses which causes imbalance in oxidant and antioxidant systems. This may further contribute to disease progression; lower levels of vitamin C and erythrocyte glutathione peroxidase enzyme were observed in active cutaneous leishmaniasis patients. However, lipid peroxidation and glutathione levels were increased compared to the control group[71] it was observed in canine animal model of visceral leishmaniasis that the antioxidants ceruloplasmin, glutathione, β-carotene, retinol, and ascorbic acid levels were decreased comparatively to control group further suggesting decrease in lipid peroxidation [72]. Vitamin C reflected leishmania inhibition when used as prophylactic treatment in hamster model. The animals were relatively resistant to subsequent Leishmania infection after receiving prophylactic vitamin C at various doses of 250, 100, and 50 mg/kg for 2 weeks, as in comparison to untreated controls, there was much reduced parasite burden. In The reduction in parasitic burden was observed in animal model treated with vitamin C as prophylaxis at 250 mg/kg [73].

Effect of Micronutrient vitamin C in leishmaniasis. Vitamin C inhibits disease progression by acting as antioxidant, by balancing oxidant and antioxidant levels, caused by increased lipid peroxidation & low anti-oxidant defense. Vitamin C also acts as prophylactic and decrease the parasitic burden in animal models. It further regulates free radicals which are toxic to leishmania species and cause inhibition
Role of Vitamin D
The innate and adaptive immunity in human body plays a crucial role in the disease management. Vitamin D is one such molecule which regulates both innate and adaptive immunity. [74] Vitamin D is also known as hormone of immunomodulation. 1,25-dihydroxyvitamin D, the active form of vitamin D, has been demonstrated in investigations to have immunological effects on several elements of the innate and adaptive immune systems, as well as endothelial membrane integrity. The link involving decreased serum 25-hydroxyvitamin D concentration and an enhanced probability of incurring a variety of immune-related disorders has been extensively debated for decades. [75] Sunlight exposure is one of the main sources of vitamin D, and it has a prominent effect in skin immune system. [76] Vitamin D3 also plays significant bit part in the brain function, by regulating cellular growth, cellular differentiation processes, neuroprotective and mood-stabilizing effects, and tissue proliferation [77].
Vitamin D induces the antimicrobial peptides which acts majorly by instigating immune defense against infectious agents [78], Calcitriol induced LL-37 binds with the promastigotes of leishmania resulting in killing of leishmania promastigotes. Calcitriol therapy can reduce the disease progression in leishmania Mexicana infested animal mice model. Vitamin D-induced cathelicidin expression, in GM-CSF polarized macrophages combination, aids in the limitation of Leishmania species in human macrophages (Fig. 3) [79]. Vitamin D regulates zinc homeostasis, by increasing the mRNA and protein expression of ZnT10 transporter. Vitamin D has a notable effect in controlling the development of dermal lesions in animal models of leishmaniasis where vitamin D deficient rats developed lesions. [80] A study supports the hypothesis that 1,25(OH)2D3 one of the active metabolites of vitamin D has an inhibiting effect on macrophage-mediated host defense. Subsequent research revealed that vitamin D receptor-knock out mice had a regular T helper cell type 1 (Th1) responsiveness to infection, as evidenced by appropriate IFN-release by CD4 + and CD8 + T cells, as a result, it was concluded that in vitamin D receptor-knock out mice, the lack of 1,25(OH)2D3-mediated suppression of macrophage microbicidal activity leads to greater resistance to Leishmania infection [81].

Effect of Micronutrient vitamin D in leishmaniasis. Vitamin D is a strong immunomodulator, which induces LL-37 an antimicrobial peptide, which causes restriction in leishmania growth, and cause death of promastigote form of leishmaniasis. Vitamin D treated mice were presented with decreased skin lesions. And deficiency of vitamin d effects the treatment out come and progression of visceral leishmaniasis. Vitamin D further inhibits IFN-γ mediated macrophages which further induces Arginase1 enzyme and decreases the NO resulting in decreased host defence in restricting Leishmania Major
Micronutrient levels in the blood have a substantial impact on the treatment of visceral leishmaniasis. The role of calcium signaling in epidermal stem cells, vitamin D, and progeny is necessary for normal re-epithelialization of wound in the epidermis. It was suggested that, by both β-catenin and adherents junction signaling, are promoted by vitamin D and calcium to facilitate re-epithelialization of wound [82]. An adjuvant therapy by utilizing micronutrients is highly in need to fight the drug-resistant leishmaniasis and it provides a new insight and novel perspective into eliminating leishmaniasis and avoiding another endemic in lower-income countries.
Even though major literature supports the key role of vitamin D in cell proliferation, body immunity, antiviral properties, etc. Some evidence suggests that vitamin D3 is detrimental for host. According to a canine animal model study, vitamin D level is neither seasonal nor risk predictor to transmit leishmaniasis in canines, but the vitamin D levels decrease along with beginning of the active clinical disease, indicating a function in control of parasite. [83] Vitamin D insufficiency was connected to the advancement of leishmaniasis in many ways. Moreover, there has been no link among the status of vitamin D and the cell immune response to Leishmania. [84] Despite the major role of vitamin D in tissue healing, however, it had no discernible effect on the parasite's viability in individuals with active leishmaniasis [85]. Nitrous oxide (NO) is widely considered as the primary antimicrobial compound used to inhibit Leishmania major through Interferon-γ activated macrophages in the animal model. It is generally known that NO functions as a bactericidal agent by producing reactive nitrogen species, which then alter organic molecules. [86] The IFN-γ-mediated activity of macrophages and their consequent improved ability to kill internalized parasites is an important mechanism for the host defense over Leishmania Major infection. [86, 87] The leishmanicidal activity of IFN-activated macrophage significantly inhibited by vitamin D3. Furthermore, the suppression of parasite inhibiting activity by vitamin D3 is significantly linked to a reduction in NO production from IFN-stimulated macrophages [81] Moreover, arginase1 is documented to promote Leishmania growth in macrophages, probably by producing polyamines, that are necessary for parasite proliferation [88]. In IFN-activated macrophages, sequential exposure to vitamin D3 induces the enzyme Arginase 1. Since this, reaction is impaired vitamin D receptor-KO macrophages, it could double the leishmanial activity in such cells. [81]
Zinc
Zinc is one of the essential trace elements, required in minute quantities for effective functioning of the immunological system. This element protects host cells from oxidative stress and inflammation [89] Many enzymes play a key role in cellular response to foreign infections based on the concentration of this trace metal for catalytic action. Zinc is required for B cells, T cell growth, and proliferation. The work of neutrophils, macrophages, is harmed by Zn deficiency. It also causes a mismatch between the TH1 and TH2 cells. Zinc deficiency causes stress and activates macrophages–monocytes, further leads to an upsurge in the development of inflammatory cytokines such as interleukin-1b, interleukin-6, IL-8, and tumor necrosis factor. Zinc deficiency, even at a low level, can affect clinical, biochemical, and immunological functions [90, 91].
Micronutrients such as calcium and zinc have played a major role in growth and maturation of B and T cells. Furthermore, it also results in an imbalance between the TH1 and TH2 cells. [90, 92, 93] Hence, calcium and zinc play a pivotal role in immune system. Given that vitamin D regulates zinc homeostasis, by increasing the mRNA and protein expression of Zinc transport 10 (ZnT10) transporter [94, 95]. Study on cutaneous leishmaniasis revealed low serum zinc concentration. Meglumine antimonate shows less treatment efficacy 60% when compared to zinc sulfate 83.9% in the period of six weeks [95, 96].
The zinc ion possesses the capability to precipitate protein molecules. In vitro and in animal models, the Leishmania major and Leishmania tropica’s promastigotes and amastigotes were more susceptible to zinc sulfate. A 2% zinc sulfate cause growth inhibition in amastigotes form of leishmania species (Fig. 4) [97]. A controlled trial of cutaneous leishmaniasis patients the treatment showed the uppermost cure rate with 94–7% for zinc sulfate 2% solution injected intralesional, followed by 88–5% for sodium stibogluconate and 85% for hypertonic sodium chloride [98]. In individuals with visceral leishmaniasis, reduced Zn levels and elevated Mg levels can be linked to chronicity and severity of the disease. This result could indicate only more progressed phases of the infection or it could indicate a distinct prognostic factor [99].

Effect of Micronutrient trace element Zinc in leishmaniasis. Zinc sulphate was found to cause high cure rates in visceral leishmaniasis, and susceptible to both amastigote and promastigotes. Low zinc levels cause increase in progression and chronicity of leishmaniasis
Calcium
Calcium has a crucial function in the immune response's activation. Variations in the cytoplasmic excess calcium concentration Ca2 + are thought to be important for reactions as diverse as neutrophil bacterial death and lymphoid cell antibody production. Calcium is required for vascular contraction and vasodilation, muscular function, neuronal transmission, cellular communication, and hormone production in the systemic circulation, extracellular fluid, muscle, and other tissues. [100] Calcium signals are involved in cell regulation, gene transcription, and development effector actions in immune system. The involvement of immunoreceptors including the T, B cell receptors, and Fc receptors, costimulatory receptors, as well as chemokines causes a rise in intracellular calcium ions (Ca2)[101, 102] From mammals to parasites, Ca2 + has long been identified as an key messenger in all the eukaryotes. When Ca2 + homeostasis is disrupted in any cell, it typically has lethal consequences, resulting in cell death via apoptosis or necrosis. The expression of intracellular Ca2 + and the cytotoxic effect of new drugs that disrupt Ca2 + in the parasites may create new possibilities to develop newer drugs to treat leishmaniasis [103]. Miltefosine, an orally ingested alkyllysophospholipid with substantial anti-Leishmania action, is a significant step forward in leishmaniasis therapy. Miltefosine has recently been discovered to disrupt the intracellular Ca2 + homeostasis in parasite by causing a significant spike in [Ca2 +] by activating a plasma membrane Ca2 + receptor. Miltefosine and amiodarone were discovered to have synergistic effect on multiplication of the amastigotes developing within the macrophages, resulting in a parasitological cure of 90% in a murine model of leishmaniasis, as demonstrated by a polymerase chain reaction assay [104, 105]. When Ca2 + homeostasis is disrupted in any cell, it usually has deadly consequences, culminating in cell death via apoptosis or necrosis. The breakdown of Ca2 + homeostasis, which releases Ca2 + from the mitochondrion, is a mechanism of action, through which drug amiodarone was shown effective against leishmania Mexicana.[106, 107].[104] However, unlike amiodarone, miltefosine only increased [Ca2 +] in the presence of external Ca2 + , demonstrating that this drug does not cause Ca2 + to be released from intracellular compartments, other than through the stimulation of plasma membrane Ca2 + channel [106]. Hence, calcium plays a key role as micronutrient in the inhibition of growth of leishmania parasite and helps in the immunity of the host against the disease.
Iron
Iron is a vital nutrient in the physiology of human beings, since it holds a significant role in various biological pathways. The iron access and availability in the systemic circulation have a significant impact on pathogen development, iron deprivation, virulence by various methods is an essential element in the first-line protection against infection [108]. Iron's biological value stems from its capacity to switch among two states of oxidation, i.e., ferrous (Fe2 +) and ferric (Fe3 +),for a variety of biological activities, such as respiration and DNA replication, iron is an appropriate redox catalyst [109]. Iron is a critical nutrient for all species, notably pathogenic trypanosomiasis parasites, and serves as a component for numerous enzymes in many aspects of cellular metabolism. Some studies have established that cutaneous leishmaniasis patients are suffering from iron deficiency[110,111,112] Visceral Leishmaniasis induced disruptions in iron homeostasis have been linked to immunological dysfunction in studies. Increased hepcidin damaged the sole iron transporter ferroprotein, resulting in reduced iron regulation by transferrin-dependent and -independent channels in VL patients. As a result, the disruptions in homeostasis of iron play an important role in human leucocyte antigen-DR isotype (HLA-DR)mediated antigen presentation and innate armament by iNOS downregulation and changing IFN-, interleukin-6, and interleukin-10 profiles [113]. Iron is necessary as a component for Iron super oxide dismutase (Fe-SOD) antioxidant activity and as a precursor for the parasite's synthesis of cofactor Fe–S clusters. Sodium oxide dismutase was first discovered in Leishmania chagasi. Three superoxide dismutase (SOD) genes, SODA, SODB1, and SODB2, each of which has Fe-dependent SOD sequences preserved [114]. ROS equilibrium in the parasite is controlled by the amount of iron available. Unlike higher eukaryotes, which use separate metal intermediates for cytosolic and mitochondrial SODs, all SODs of Leishmania (FeSODA) and FeSODB1/B2) need iron as a component [115, 116]. The parasites are protected from free radicals generated by nitro prussiate and paraquat when SODa and SODb are overexpressed in Leishmania tropica.[108, 117] immunity to Leishmania major infection caused by a ‘iron load,’ with concurrent Th1 growth immune response of the type was thought to have increased T cell receptor-mediated T lymphocyte proliferation, NF-kB activation and a large proportion of interferon-positive CD4 + -T cells with enhanced capacity of splenic cells to present Leishmania major-derived peptides [118]. This was proved correct with further evidence of NF-kB signaling pathway modulation with in macrophages which was influenced by high amount of iron generated reactive oxygen species. [119] Iron overload reduces Leishmania proliferation by promoting the host's oxidative defense mechanism, most likely through an oxidative process that modulates the signaling cascade and produces parasite-harmful metabolites. Understanding of the role of iron and iron-containing heme uptake by Leishmania in parasite transformation and disease has been in light for past some time. Knowledge regarding the impact of iron on Leishmania is also a high concern subject that should be addressed in order to gain a better understanding of how reactive products affect the parasite's physiology in both iron replete and iron depleted conditions. Conclusively, iron has its crucial role in immune-modulation, cell differentiation, redox regulation.
Micronutrients as Dietary Prophylaxis in Leishmaniasis
The World Health Organization (WHO) considers leishmaniasis to be a prioritized disease for which novel therapies must be developed. Available drugs are not always completely effective; they require i.v administration and also have common and serious side effects. Miltefosine is the only oral drug that is effective against leishmaniasis; however, it has some drawbacks, including resistance, high cost, and non-availability in several endemic regions [120]. As a result, investigating therapeutic alternatives to develop an oral medicine could overcome most of these problems. It is shown that malnutrition prompts the progression of VL disease, and VL exacerbates micronutrient deficiencies. Malnutrition has been recognized as a poor predictive marker for leishmaniasis. Nevertheless, the impact of nutritional supplements in VL patients is unknown. Given that VL commonly disturb the individual’s livelihood in developing countries with limited availability to diets, adding extra nutrients to individuals getting VL therapies could improve their micronutrients status and therefore their well-being [2].
A study conducted in an endemic region of northeast Brazil discovered that vitamin A may play a dual function in immune response regulation during Visceral Leishmaniasis infection. The study found that when healthy children were subjected to Leishmania antigens, their immunoregulatory reactions as well as IL-10 expression in Treg or monocytes improved [28]. Several researches have revealed that zinc could contribute as a promising and potent anti-cutaneous leishmaniasis agent. In studies intended to investigate the efficacy of zinc sulfate in vitro or in vivo, it was indicated that it can be used as a therapy for or a prophylactic agent against Cutaneous Leishmaniasis. [121]
Discussion
Previous studies ascertain that the major concerns in endemic areas to restrict leishmaniasis are higher cost, injectables, and toxicity, resistance to drugs, malnutrition due to poverty, comorbid diseases, and the absence of effective vaccine. Micronutrients such as vitamins and trace elements are crucial to instigate immune defense against pathogens which cause infectious diseases. Less intake of micronutrients which leads to malnutrition further affects the disease progression, treatment efficacy, and relapse of leishmaniasis. There are no large sample size studies carried out to identify the hypovitaminosis A, B, C, D and trace elements such as calcium, zinc, and iron in leishmaniasis patients. Since these micronutrients play a major role in body innate and adaptive immunity which further reduces the risk of getting infection of leishmaniasis. There is lack knowledge, perception, and practices toward the usage of micronutrient supplementation, in the endemic areas of leishmaniasis. The molecules are proved to be effective in inhibiting the growth of both amastigotes and promastigote form of leishmaniasis through various cellular pathways. Vitamin D was suggested to be a probable agent to be used to treat drug resistance in dermal leishmaniasis to inhibit the growth through vitamin D receptor pathway. In similar way, vitamin C is a free radical scavenger of hydroxyl, singlet oxygen, etc. which inhibits the growth of leishmaniasis. Apart from vitamin D and vitamin C the other vitamin molecules are vaguely explored in the immunological studies to define the immunomodulatory pathways in leishmaniasis. The disease progression, treatment efficacy of current available drugs needs to be explored individually in relation to the serum micronutrient levels. Furthermore, the attitudes, practices, and knowledge toward the micronutrients in the population of endemic areas need to be addressed to fill the knowledge gap with community education to decrease the infection rate altogether. Conclusively, these micronutrients can be used as dietary prophylaxis for better treatment efficacy and to decrease the reinfection and relapse of leishmaniasis. More robust research is required in this area to cross the major obstacles to fight the disease. Some researchers have been looking into alternatives and novel agents that have leishmanicidal or anti-leishmanial properties for this reason. Some sort of vector control, such as reservoir population eradication, are the main strategies available. Modulating nutritional status or correcting malnutrition could likely lower disease aggravation and stop rate of infection in endemic areas. The epidemiological surveys for mapping of vitamin and trace element deficiency in leishmaniasis patients need to be done as part of eradication strategy. Secondly, using selected vitamins and trace elements as supportive therapy may need to be explored further with robust preclinical and clinical studies to fight resistance and reoccurrence of leishmaniasis in the endemic areas. This may further help in building public health strategies, and health policies in endemic areas to fight the disease.
References
Romano T-GE, Quintanilla-Cedillo M, Ruiz-Esmenjaud J (2017) Leishmaniasis: A review. F1000 Res 6(750):10.12688/f1000research.11120.1
Custodio E, López-Alcalde J, Herrero M, Bouza C, Jimenez C, Genannt Bonsmann SS, Mouratidou T, López-Cuadrado T, Benito A, Alvar J (2018) Nutritional supplements for patients being treated for active visceral leishmaniasis. Cochrane Database Syst Rev: 3. https://doi.org/10.1002/14651858.CD012261.pub2
Alvar J, Vélez ID, Bern C, Herrero M, Desjeux P, Cano J et al (2012) World Health Organization, WHO. Leishmaniasis control team. Leishmaniasis worldwide and global estimates of its incidence. PLoS One 7(5):e35671. https://doi.org/10.1371/journal.pone.0035671
Shenkin A (2006) Micronutrients in health and disease. Postgrad Med J 82(971):559–567. https://doi.org/10.1136/pgmj.2006.047670
Dao DT, Anez-Bustillos L, Cho BS, Li Z, Puder M, Gura KM (2017) Assessment of micronutrient status in critically ill children: challenges and opportunities. Nutrients. 9(11):1185. https://doi.org/10.3390/nu9111185
Bailey RL, West KP Jr, Black RE (2015) The epidemiology of global micronutrient deficiencies. Ann Nutr Metab 66(Suppl 2):22–33. https://doi.org/10.1159/000371618
National Family Health Survey-5 2019-2021, India Fact sheet. Mumbai: Ministry of health and family welfare; 2021 [cited 2021 07-05-2021]. Available from: http://rchiips.org/nfhs/NFHS-5_FCTS/India.pdf.
WHO. Malnutrition, fact sheet: WHO; 2021 [updated 9 June 2021]. Available from: https://www.who.int/news-room/fact-sheets/detail/malnutrition.
Feleke BE, Feleke TE (2020) Micronutrient levels and their effects on the prognosis of visceral leishmaniasis treatment, a prospective cohort study. BMC Infect Dis 20(1):1–9. https://doi.org/10.1186/s12879-020-05615-1
Ali A (1997) Visceral leishmaniasis in Southern Ethiopia II. Nutritional risk factors. Ethiop J Health Dev 11(2)
Bantie K, Tessema F, Massa D, Tafere Y (2014) Factors associated with visceral leishmaniasis infection in North Gondar Zone, Amhara Region, North West Ethiopia, case control study. Sci J Pub Health 2(6):560–568. https://doi.org/10.1016/j.nut.2019.110712
Nweze JA, Nweze EI, Onoja US (2020) Nutrition, malnutrition, and leishmaniasis. Nutrition 73:110712. https://doi.org/10.1016/j.nut.2019.110712
Malafaia G (2009) Protein-energy malnutrition as a risk factor for visceral leishmaniasis: a review. Parasite Immunol 31(10):587–596. https://doi.org/10.1111/j.1365-3024.2009.01117.x
Cerf B, Jones T, Badaro R, Sampaio D, Teixeira R, Johnson W Jr (1987) Malnutrition as a risk factor for severe visceral leishmaniasis. J Infect Dis 156(6):1030–1033
Collin S, Davidson R, Ritmeijer K, Keus K, Melaku Y, Kipngetich S, Davies C (2004) Conflict and kala-azar: determinants of adverse outcomes of kala-azar among patients in southern Sudan. Clin Infect Dis 38(5):612–619. https://doi.org/10.1086/381203
Seaman J, Mercer AJ, Sondorp E (1996) The epidemic of visceral leishmaniasis in Western Upper Nile, southern Sudan: course and impact from 1984 to 1994. Int J Epidemiol 25(4):862–871
Jardim-Botelho A, Brooker S, Geiger SM, Fleming F, Souza Lopes AC, Diemert DJ, Corrêa-Oliveira R, Bethony JM (2008) Age patterns in undernutrition and helminth infection in a rural area of Brazil: associations with ascariasis and hookworm. Trop Med Int Health 13(4):458–467. https://doi.org/10.1111/j.1365-3156.2008.02022.x
Pearson RD, de Queiroz SA (1996) Clinical spectrum of leishmaniasis. Clin Infect Dis 1:1–1
Anstead GM, Chandrasekar B, Zhao W, Yang JU, Perez LE, Melby PC (2001) Malnutrition alters the innate immune response and increases early visceralization following Leishmania donovani infection. Infect Immun 69(8):4709–4718. https://doi.org/10.1128/IAI.69.8.4709-4718.2001
Gray EE, Cyster JG (2012) Lymph node macrophages. J Innate Immun 4:424–436. https://doi.org/10.1159/000337007
Roozendaal R, Mebius RE, Kraal G (2008) The conduit system of the lymph node. Int Immunol 20(12):1483–1487. https://doi.org/10.1093/intimm/dxn110
Engzell U, Rubio C, Tjernberg B, Zajicek J (1968) The lymph node barrier against V×2 cancer cells before, during and after lymphography: A preliminary report of experiments on rabbits. Eur J Cancer 4(3):305–312. https://doi.org/10.1016/0014-2964(68)90056-X
Malekshah AF, Kimiagar M, Saadatian-Elahi M, Pourshams A, Nouraie M, Goglani G, Hoshiarrad A, Sadatsafavi M, Golestan B, Yoonesi A, Rakhshani N (2006) Validity and reliability of a new food frequency questionnaire compared to 24 h recalls and biochemical measurements: pilot phase of Golestan cohort study of esophageal cancer. Eur J Clin Nutr 60(8):971–977. https://doi.org/10.1038/sj.ejcn.1602407
Alam I, Almajwal AM, Alam W, Alam I, Ullah N, Abulmeaaty M, Razak S, Khan S, Pawelec G, Paracha PI (2019) The immune-nutrition interplay in aging–facts and controversies. Nutr Healthy Aging 5(2):73–95. https://doi.org/10.3233/NHA-170034
Beard J (2007) Recent evidence from human and animal studies regarding iron status and infant development. J Nutr 137(2):524S–530S. https://doi.org/10.1093/jn/137.2.524S
Vermund SH, Scott ME, Humphries DL (2021) Public health and clinical implications of nutrition-infection interactions. Nutr Infect Dis:459–481
Rashidi S, Fernández-Rubio C, Manzano-Román R, Mansouri R, Shafiei R, Ali-Hassanzadeh M, Barazesh A, Karimazar M, Hatam G, Nguewa P (2021) Potential therapeutic targets shared between leishmaniasis and cancer. Parasitology 148(6):655–671. https://doi.org/10.1017/S0031182021000160
Lima Maciel BL, Valverde JG, Rodrigues-Neto JF, Freire-Neto F, Keesen TS, Jeronimo SM (2014) Dual immune modulatory effect of vitamin A in human visceral leishmaniasis. PLoS One 9(9):e107564. https://doi.org/10.1371/journal.pone.0107564
Moore EM, Lockwood DN (2010) Treatment of visceral leishmaniasis. J Glob Infect Dis 2(2):151–158. https://doi.org/10.4103/0974-777X.62883
Bizri NA, Alam W, Khoury M, Musharrafieh U, Ghosn N, Berri A, Bizri AR (2021) The association between the syrian crisis and cutaneous leishmaniasis in Lebanon. Acta Parasitol 66(4):1240–1245. https://doi.org/10.1007/s11686-021-00395-3
Puertollano MA, Puertollano E, de Cienfuegos GÁ, de Pablo MA (2011) Dietary antioxidants: immunity and host defense. Curr Top Med Chem 11(14):1752–1766. https://doi.org/10.2174/156802611796235107
Grant M, Lamb C (2006) Systemic immunity. Curr Opin Plant Biol 9(4):414–420. https://doi.org/10.1016/j.pbi.2006.05.013
Semba RD (1998) The role of vitamin A and related retinoids in immune function. Nutr Rev 56(1 Pt 2):S38–S48. https://doi.org/10.1111/j.1753-4887.1998.tb01643.x
Carr AC, Maggini S (2017) Vitamin C and immune function. Nutrients 9(11):1211. https://doi.org/10.3390/nu9111211
Hewison M (2012) Vitamin D and immune function: an overview. Proc Nutr Soc 71(1):50–61. https://doi.org/10.1017/S0029665111001650
Serbecic N, Beutelspacher SC. 9 (2005) Anti-oxidative vitamins prevent lipid-peroxidation and apoptosis in corneal endothelial cells. Cell Tissue Res 320(3):465-475. https://doi.org/10.1007/s00441-004-1030-3.
Kocyigit A, Keles H, Selek S, Guzel S, Celik H, Erel O (2005) Increased DNA damage and oxidative stress in patients with cutaneous leishmaniasis. Mutat Res 585(1-2):71–78. https://doi.org/10.1016/j.mrgentox.2005.04.012
Udaya Kumar V, Pavan G, Murti K, Kumar R, Dhingra S, Haque M, Ravichandiran V (2021) Rays of immunity: role of sunshine vitamin in management of COVID-19 infection and associated comorbidities. Clin Nutr ESPEN 46:21–32. https://doi.org/10.1016/j.clnesp.2021.09.727
Clagett-Dame M, Knutson D (2011) Vitamin A in reproduction and development. Nutrients 3(4):385–428. https://doi.org/10.3390/nu3040385
Tanumihardjo SA (2011) Vitamin A: biomarkers of nutrition for development. Am J Clin Nutr 94(2):658S–665S. https://doi.org/10.3945/ajcn.110.005777
Caldas A, Favali C, Aquino D, Vinhas V, van Weyenbergh J, Brodskyn C, Costa J, Barral-Netto M, Barral A (2005) Balance of IL-10 and interferon-gamma plasma levels in human visceral leishmaniasis: implications in the pathogenesis. BMC Infect Dis 5:113. https://doi.org/10.1186/1471-2334-5-113
Kenney RT, Sacks DL, Gam AA, Murray HW, Sundar S (1998) Splenic cytokine responses in Indian kala-azar before and after treatment. J Infect Dis 177(3):815–818. https://doi.org/10.1086/517817
Stephensen CB, Jiang X, Freytag T (2004) Vitamin A deficiency increases the in vivo development of IL-10-positive Th2 cells and decreases development of Th1 cells in mice. J Nutr 134(10):2660–2666. https://doi.org/10.1093/jn/134.10.2660
Bezerra IPDS, Oliveira-Silva G, Braga DSFS, de Mello MF, Pratti JES, Pereira JC, da Fonseca-Martins AM, Firmino-Cruz L, Maciel-Oliveira D, Ramos TD, Vale AM, Gomes DCO, Rossi-Bergmann B, de Matos Guedes HL (2019) Dietary vitamin D3 deficiency increases resistance to leishmania (leishmania) amazonensis infection in mice. Front Cell Infect Microbiol 9:88. https://doi.org/10.3389/fcimb.2019.00088
Mashayekhi Goyonlo V, Norouzy A, Nemati M, Layegh P, Akhlaghi S, Taheri AR, Kiafar B (2020) Nutritional intake and chronicity associated with the old world cutaneous leishmaniasis: role of vitamin A. Iran J Public Health 49(1):167–172
Kau AL, Ahern PP, Griffin NW, Goodman AL, Gordon JI (2011) Human nutrition, the gut microbiome and the immune system. Nature 474(7351):327–336. https://doi.org/10.1038/nature10213
Maggini S, Wintergerst ES, Beveridge S, Hornig DH (2007) Selected vitamins and trace elements support immune function by strengthening epithelial barriers and cellular and humoral immune responses. Br J Nutr 98(Suppl 1):S29–S35. https://doi.org/10.1017/S0007114507832971
Doenhoff MJ, Modha J, Lambertucci JR, McLaren DJ (1991) The immune dependence of chemotherapy. Parasitol Today 7(1):16–18. https://doi.org/10.1016/0169-4758(91)90079-4
Adinolfi LE, Bonventre PF, Vander Pas M, Eppstein DA (1985) Synergistic effect of glucantime and a liposome-encapsulated muramyl dipeptide analog in therapy of experimental visceral leishmaniasis. Infect Immun 48(2):409–416. https://doi.org/10.1128/iai.48.2.409-416.1985
Northrop-Clewes CA, Thurnham DI (2012) The discovery and characterization of riboflavin. Ann Nutr Metab 61(3):224–230. https://doi.org/10.1159/000343111
Mahan LK, Raymond JL (2016) Krause’s food & the nutrition care process-e-book. Elsevier Health Sciences
Joshi PC (1989) Ultraviolet radiation-induced photodegradation and 1O2, O2-. production by riboflavin, lumichrome and lumiflavin. Indian J Biochem Biophys 26(3):186–189
Zempleni J, Galloway JR, McCormick DB (1996) Pharmacokinetics of orally and intravenously administered riboflavin in healthy humans. Am J Clin Nutr 63(1):54–66. https://doi.org/10.1093/ajcn/63.1.54
Unna K, Greslin JG (1942) Studies on the toxicity and pharmacology of riboflavin. J Pharmacol Exp Ther 76(1):75–80
Meisel P, Kocher T (2005) Photodynamic therapy for periodontal diseases: state of the art. J Photochem Photobiol B 79(2):159–170. https://doi.org/10.1016/j.jphotobiol.2004.11.023
Redfearn DP, Trim GM, Skanes AC, Petrellis B, Krahn AD, Yee R, Klein GJ (2005) Esophageal temperature monitoring during radiofrequency ablation of atrial fibrillation. J Cardiovasc Electrophysiol 16(6):589–593. https://doi.org/10.1111/j.1540-8167.2005.40825.x
Picker SM, Steisel A, Gathof BS (2009) Cell integrity and mitochondrial function after Mirasol-PRT treatment for pathogen reduction of apheresis-derived platelets: Results of a three-arm in vitro study. Transfus Apher Sci 40(2):79–85. https://doi.org/10.1016/j.transci.2009.01.013
AuBuchon JP, Herschel L, Roger J, Taylor H, Whitley P, Li J, Edrich R, Goodrich RP (2005) Efficacy of apheresis platelets treated with riboflavin and ultraviolet light for pathogen reduction. Transfusion 45(8):1335–1341. https://doi.org/10.1111/j.1537-2995.2005.00202.x
Ruane PH, Edrich R, Gampp D, Keil SD, Leonard RL, Goodrich RP (2004) Photochemical inactivation of selected viruses and bacteria in platelet concentrates using riboflavin and light. Transfusion 44(6):877–885. https://doi.org/10.1111/j.1537-2995.2004.03355.x
Bafghi AF, Kianfar P, Moradi A, Dehghani A. Antileishmanial activity of 2-phenoxy nicotinic acid hydrazide sulfonamide against leishmania (L) major [MRHO/IR/75/ER] promastigotes: an in-vitro study
Sipahi T, Tavil B, Oksal A (2005) Visceral leishmaniasis and pseudomonas septicemia associated with hemophagocytic syndrome and myelodysplasia in a Turkish child. Turk J Pediatr 47(2):191–194
Hasle H, Kerndrup G, Jacobsen BB, Heegaard ED, Hornsleth A, Lillevang ST (1994) Chronic parvovirus infection mimicking myelodysplastic syndrome in a child with subclinical immunodeficiency. Am J Pediatr Hematol Oncol 16(4):329–333
Heuser G, Vojdani A (1997) Enhancement of natural killer cell activity and T and B cell function by buffered vitamin C in patients exposed to toxic chemicals: the role of protein kinase-C. Immunopharmacol Immunotoxicol 19(3):291–312. https://doi.org/10.3109/08923979709046977
Levy R, Shriker O, Porath A, Riesenberg K, Schlaeffer F (1997) Vitamin C for the treatment of recurrent furunculosis in patients with imparied neutrophil functions. J Infect Dis 173(6):1502–1505. https://doi.org/10.1093/infdis/173.6.1502
Mousavi S, Bereswill S, Heimesaat MM (2019) Immunomodulatory and antimicrobial effects of vitamin C. Eur J Microbiol Immunol (Bp) 9(3):73–79. https://doi.org/10.1556/1886.2019.00016
Iheanacho EN, Stocker R, Hunt NH (1993) Redox metabolism of vitamin C in blood of normal and malaria-infected mice. Biochimica et Biophysica Acta (BBA)-Molecular Basis of Disease 1182(1):15–21
Mahmoud MA (2021) Luteal phase Vitamin C supplementation on the outcome of in-vitro fertilization. Egypt J Fertil Steril 25(2):28–35
Murray HW (1981) Susceptibility of leishmania to oxygen intermediates and killing by normal macrophages. J Exp Med 153(5):1302–1315. https://doi.org/10.1084/jem.153.5.1302
Reiner NE, Kazura JW (1982) Oxidant-mediated damage of Leishmania donovani promastigotes. Infect Immun 36(3):1023–1027. https://doi.org/10.1128/iai.36.3.1023-1027.1982
Mehlotra RK (1996) Antioxidant defense mechanisms in parasitic protozoa. Crit Rev Microbiol 22(4):295–314. https://doi.org/10.3109/10408419609105484
Vural H, Aksoy N, Ozbilge H (2004) Alterations of oxidative-antioxidative status in human cutaneous leishmaniasis. Cell Biochem Funct 22(3):153–156. https://doi.org/10.1002/cbf.1066
Bildik A, Kargin F, Seyrek K, Pasa S, Ozensoy S (2004) Oxidative stress and non-enzymatic antioxidative status in dogs with visceral leishmaniasis. Res Vet Sci 77(1):63–66. https://doi.org/10.1016/j.rvsc.2004.01.005
Garg R, Singh N, Dube A (2004) Intake of nutrient supplements affects multiplication of leishmania donovani in hamsters. Parasitology 129(Pt 6):685–691. https://doi.org/10.1017/s0031182004006055
Hewison M (2011) Vitamin D and innate and adaptive immunity. Vitam Horm 86:23–62. https://doi.org/10.1016/B978-0-12-386960-9.00002-2
Charoenngam N, Holick MF (2020) Immunologic effects of vitamin D on human health and disease. Nutrients 12(7):2097. https://doi.org/10.3390/nu12072097
Amerio P, Carbone A, Auriemma M, Varrati S, Tulli A. (2009) UV induced skin immunosuppression. anti-inflammatory & anti-allergy agents in medicinal chemistry (Formerly current medicinal chemistry-anti-inflammatory and anti-allergy agents) 8(1):3-13.
Christiansen C, Rodbro P, Sjö O (1994) “Anticonvulsant action” of vitamin D in epileptic patients? A controlled pilot study. Br Med J 2(5913):258–259. https://doi.org/10.1136/bmj.2.5913.258
Ramos-Martínez E, Gutierrez-Kobeh L, Villaseñor-Cardoso MI (2015) The role of vitamin D in the control of Leishmania infection. Can J Physiol Pharmacol 93(5):369–376. https://doi.org/10.1139/cjpp-2014-0372
Crauwels P, Bank E, Walber B, Wenzel UA, Agerberth B, Chanyalew M, Abebe M, König R, Ritter U, Reiling N, van Zandbergen G (2019) Cathelicidin contributes to the restriction of leishmania in human host macrophages. Front Immunol 10:2697. https://doi.org/10.3389/fimmu.2019.02697
Whitcomb JP, Deagostino M, Ballentine M, Fu J, Tenniswood M, Welsh J, Cantorna M, McDowell MA (2012) The role of vitamin D and vitamin D receptor in immunity to leishmania major infection. J Parasitol Res 134645. https://doi.org/10.1155/2012/134645
Ehrchen J, Helming L, Varga G, Pasche B, Loser K, Gunzer M, Sunderkötter C, Sorg C, Roth J, Lengeling A (2007) Vitamin D receptor signaling contributes to susceptibility to infection with Leishmania major. FASEB J 21(12):3208–3218. https://doi.org/10.1096/fj.06-7261com
Oda Y, Bikle DD (2020) Vitamin D and calcium signaling in epidermal stem cells and their regeneration. World J Stem Cells 12(7):604–611. https://doi.org/10.4252/wjsc.v12.i7.604
Martori C, Velez R, Gállego M, Mesa I, Ferreira R, Alberola J, Rodríguez-Cortés A (2021) Vitamin d and leishmaniasis: neither seasonal nor risk factor in canine host but potential adjuvant treatment through cbd103 expression. PLoS Negl Trop Dis 15(8):e0009681. https://doi.org/10.1371/journal.pntd.0009681
Rodriguez-Cortes A, Martori C, Martinez-Florez A, Clop A, Amills M, Kubejko J, Llull J, Nadal JM, Alberola J (2017) Canine Leishmaniasis progression is associated with vitamin D deficiency. Sci Rep 7(1):3346. https://doi.org/10.1038/s41598-017-03662-4
Machado PA, Escrivani DO, Gomes DCO, Rossi-Bergmann B, Chaves SP, Coimbra ES, de Matos Guedes HL (2020) Vitamin D increases killing of intracellular Leishmania amazonensis in vitro independently of macrophage oxidative mechanisms. Parasitology 147(14):1792–1800. https://doi.org/10.1017/S0031182020001791
Murray HW, Nathan CF (1999) Macrophage microbicidal mechanisms in vivo: reactive nitrogen versus oxygen intermediates in the killing of intracellular visceral Leishmania donovani. J Exp Med 189(4):741–746. https://doi.org/10.1084/jem.189.4.741
Bogdan C (2001) Nitric oxide and the immune response. Nat Immunol 2(10):907–916. https://doi.org/10.1038/ni1001-907
Kropf P, Fuentes JM, Fähnrich E, Arpa L, Herath S, Weber V, Soler G, Celada A, Modolell M, Müller I (2005) Arginase and polyamine synthesis are key factors in the regulation of experimental leishmaniasis in vivo. FASEB J 19(8):1000–1002. https://doi.org/10.1096/fj.04-3416fje
Ferencík M, Ebringer L (2003) Modulatory effects of selenium and zinc on the immune system. Folia Microbiol (Praha) 48(3):417–426. https://doi.org/10.1007/BF02931378
Prasad AS (2007) Zinc: mechanisms of host defense. J Nutr 137(5):1345–1349. https://doi.org/10.1093/jn/137.5.1345
Van Weyenbergh J, Santana G, D’Oliveira A Jr, Santos AF Jr, Costa CH, Carvalho EM, Barral A, Barral-Netto M (2004) Zinc/copper imbalance reflects immune dysfunction in human leishmaniasis: an ex vivo and in vitro study. BMC Infect Dis 4:50. https://doi.org/10.1186/1471-2334-4-50
Zughaier SM, Lubberts E, Bener A (2020) Editorial: immune-modulatory effects of vitamin D. Front Immunol 11:596611. https://doi.org/10.3389/fimmu.2020.596611
Claro da Silva T, Hiller C, Gai Z, Kullak-Ublick GA (2016) Vitamin D3 transactivates the zinc and manganese transporter SLC30A10 via the vitamin D receptor. J Steroid Biochem Mol Biol 163:77–87. https://doi.org/10.1016/j.jsbmb.2016.04.006
Farzin L, Moassesi ME (2014) A comparison of serum selenium, zinc and copper level in visceral and cutaneous leishmaniasis. J Res Med Sci 19(4):355–357
Pourfallah F, Javadian S, Zamani Z, Saghiri R, Sadeghi S, Zarea B, Faiaz S, Mirkhani F, Fatemi N (2009) Evaluation of serum levels of zinc, copper, iron, and zinc/copper ratio in cutaneous leishmaniasis. Iran J Arthropod Borne Dis 3(2):7–11
Grossman P, Tiefenthaler-Gilmer U, Raysz A, Kesper U (2007) Mindfulness training as an intervention for fibromyalgia: evidence of postintervention and 3-year follow-up benefits in well-being. Psychother Psychosom 76(4):226–233. https://doi.org/10.1159/000101501
Najim RA, Sharquie KE, Farjou IB (1998) Zinc sulphate in the treatment of cutaneous leishmaniasis: an in vitro and animal study. Mem Inst Oswaldo Cruz 93(6):831–837. https://doi.org/10.1590/s0074-02761998000600025
Sharquie KE, Najim RA, Farjou IB (1997) A comparative controlled trial of intralesionally-administered zinc sulphate, hypertonic sodium chloride and pentavalent antimony compound against acute cutaneous leishmaniasis. Clin Exp Dermatol 22(4):169–173. https://doi.org/10.1111/j.1365-2230.1997.tb01054.x
Lal CS, Kumar S, Ranjan A, Rabidas VN, Verma N, Pandey K, Verma RB, Das S, Singh D, Das P (2013) Comparative analysis of serum zinc, copper, magnesium, calcium and iron level in acute and chronic patients of visceral leishmaniasis. J Trace Elem Med Biol 27(2):98–102. https://doi.org/10.1016/j.jtemb.2012.09.007
Benaim B, Garcia CR (2011) Targeting calcium homeostasis as the therapy of Chagas’ disease and leishmaniasis - a review. Trop Biomed 28(3):471–481
Serrano-Martín X, Payares G, De Lucca M, Martinez JC, Mendoza-León A, Benaim G (2009) Amiodarone and miltefosine act synergistically against Leishmania mexicana and can induce parasitological cure in a murine model of cutaneous leishmaniasis. Antimicrob Agents Chemother 53(12):5108–5113. https://doi.org/10.1128/AAC.00505-09
Croft SL, Engel J (2006) Miltefosine-discovery of the antileishmanial activity of phospholipid derivatives. Trans R Soc Trop Med Hyg 100(Suppl 1):S4–S8. https://doi.org/10.1016/j.trstmh.2006.03.009
Grinstein S, Klip A (1989) Calcium homeostasis and the activation of calcium channels in cells of the immune system. Bull N Y Acad Med 65(1):69–79
Feske S (2007) Calcium signalling in lymphocyte activation and disease. Nat Rev Immunol 7(9):690–702. https://doi.org/10.1038/nri2152
Oh-hora M, Rao A (2008) Calcium signaling in lymphocytes. Curr Opin Immunol 20(3):250–258. https://doi.org/10.1016/j.coi.2008.04.004
Serrano-Martín X, García-Marchan Y, Fernandez A, Rodriguez N, Rojas H, Visbal G, Benaim G (2009) Amiodarone destabilizes intracellular Ca2+ homeostasis and biosynthesis of sterols in Leishmania mexicana. Antimicrob Agents Chemother 4:1403–1410. https://doi.org/10.1128/AAC.01215-08
Kashif M, Manna PP, Akhter Y, Alaidarous M, Rub A (2017) Screening of novel inhibitors against Leishmania donovani calcium ion channel to fight Leishmaniasis. Infect Disord Drug Targets 17(2):120–129. https://doi.org/10.2174/1871526516666161230124513
Bonizzi G, Karin M (2004) The two NF-kappaB activation pathways and their role in innate and adaptive immunity. Trends Immunol 25(6):280–288. https://doi.org/10.1016/j.it.2004.03.008
Cassat JE, Skaar EP (2013) Iron in infection and immunity. Cell Host Microbe 13(5):509–519. https://doi.org/10.1016/j.chom.2013.04.010
Faryadi M, Mohebali M (2003) Alterations of serum zinc, copper and iron concentrations in patients with acute and chronic cutaneous leishmaniasis. Iran J Public Health 32(4):53–58
Azadbakht M, Davoodi A, Hosseinimehr SJ, Keighobadi M, Fakhar M, Valadan R, Faridnia R, Emami S, Azadbakht M, Bakhtiyari A (2020) Tropolone alkaloids from Colchicum kurdicum (Bornm.) Stef. (Colchicaceae) as the potent novel antileishmanial compounds; purification, structure elucidation, antileishmanial activities and molecular docking studies. Exp Parasitol 213(107902). https://doi.org/10.1016/j.exppara.2020.107902
Kocyigit A, Erel O, Gurel MS, Avci S, Aktepe N (1998) Alterations of serum selenium, zinc, copper, and iron concentrations and some related antioxidant enzyme activities in patients with cutaneous leishmaniasis. Biol Trace Elem Res 65(3):271–281. https://doi.org/10.1007/BF02789102
Singh B, Singh SS, Sundar S (2019) Hepcidin mediated iron homoeostasis as immune regulator in visceral leishmaniasis patients. Parasite Immunol 41(1):e12601. https://doi.org/10.1111/pim.12601
Taylor MC, Kelly JM (2010) Iron metabolism in trypanosomatids, and its crucial role in infection. Parasitology 137(6):899–917. https://doi.org/10.1017/S0031182009991880
Plewes KA, Barr SD, Gedamu L (2003) Iron superoxide dismutases targeted to the glycosomes of Leishmania chagasi are important for survival. Infect Immun 71(10):5910–5920. https://doi.org/10.1128/IAI.71.10.5910-5920.2003
Genetu A, Gadisa E, Aseffa A, Barr S, Lakew M, Jirata D, Kuru T, Kidane D, Hunegnaw M, Gedamu L (2006) L. Leishmania aethiopica: strain identification and characterization of superoxide dismutase-B genes. Exp Parasitol 113(4):221–226. https://doi.org/10.1016/j.exppara.2006.01.010
Le TH, Humair PF, Blair D, Agatsuma T, Littlewood DT, McManus DP (2001) Mitochondrial gene content, arrangement and composition compared in African and Asian schistosomes. Mol Biochem Parasitol 117(1):61–71. https://doi.org/10.1016/s0166-6851(01)00330-9
Zaidi A, Singh KP, Ali V (2017) Leishmania and its quest for iron: An update and overview. Mol Biochem Parasitol 211:15–25. https://doi.org/10.1016/j.molbiopara.2016.12.004
Bisti S, Soteriadou K (2006) Is the reactive oxygen species-dependent-NF-kappaB activation observed in iron-loaded BALB/c mice a key process preventing growth of leishmania major progeny and tissue-damage? Microbes Infect 8(6):1473–1482. https://doi.org/10.1016/j.micinf.2006.01.004
de Souza ML, Dos Santos WM, de Sousa ALMD, Ferraz LRM, da Costa LAG, Silva EO, Rolim Neto PJ (2022) Cutaneous leishmaniasis: new oral therapeutic approaches under development. Int J Dermatol. 61(1):89–98. https://doi.org/10.1111/ijd.15902
Iraji F, Vali A, Asilian A, Shahtalebi MA, Momeni AZ (2004) Comparison of intralesionally injected zinc sulfate with meglumine antimoniate in the treatment of acute cutaneous leishmaniasis. Dermatology 209(1):46–49. https://doi.org/10.1159/000078586
Diro E, Lynen L, Gebregziabiher B, Assefa A, Lakew W, Belew Z, Hailu A, Boelaert M, van Griensven J (2015) Clinical aspects of paediatric visceral leishmaniasis in North-west Ethiopia. Trop Med Int Health 20(1):8–16. https://doi.org/10.1111/tmi.12407
Sharquie KE, Najim RA, Farjou IB, Al-Timimi DJ (2001) Oral zinc sulphate in the treatment of acute cutaneous leishmaniasis. Clin Exp Dermatol 26(1):21–26. https://doi.org/10.1046/j.1365-2230.2001.00752.x
Mishra J, Carpenter S, Singh S (2010) Low serum zinc levels in an endemic area of visceral leishmaniasis in Bihar, India. Indian J Med Res 131:793–798
Lazarte CE, Alegre C, Rojas E, Granfeldt Y (2013) Nutritional status of patients with cutaneous leishmaniasis from a tropical area of Bolivia, and implications for zinc bioavailability. Food Nutr Sci 4(10A):49. https://doi.org/10.4236/fns.2013.410A009
Acknowledgements
The authors would like to express the gratitude toward the faculty of National Institute of Pharmaceutical Education and Research- Hajipur, Department of Pharmaceuticals, Ministry of Chemicals & Fertilizers, Government of India.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Author information
Authors and Affiliations
Contributions
V Udaya Kumar drafted the manuscript and designed pictographic representations. Ayush Sharma, Muhammed favas KT, and Priya Bisht assisted in manuscript preparation and finalization. V Udaya Kumar, Dr. Krishna Murti, and Dr. Sameer Dhingra conceptualized the topic. Dr. M Ramesh and Prof V Ravichandiran conducted the final review and editing for the manuscript. All the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics Approval
This is a narrative review article and does not require any ethical approval.
Competing Interests
The authors have no relevant financial and non-financial interests to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
kumar, V., KT, M.F., Sharma, A. et al. The Possible Role of Selected Vitamins and Minerals in the Therapeutic Outcomes of Leishmaniasis. Biol Trace Elem Res 201, 1672–1688 (2023). https://doi.org/10.1007/s12011-022-03311-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12011-022-03311-6