
Abstract
Appropriate reference range of thyroid-stimulating hormone (TSH) is important to interpreting the results of thyroid functional tests. However, the reference range and sociodemographic characteristics of TSH based on large-scale studies are yet to be declared in rural China. To clarify reference range and sociodemographic characteristics of TSH in reproductive age of women from rural China. A nationwide population-based study was conducted as The National Free Preconception Health Examination Project (NFPHEP). Nearly 400,000 (n = 392,659) of Chinese rural women aged 15–55 years were randomly recruited. Predetermined strict exclusion criteria made a number of 359,895 as the reference population. Serum TSH was evaluated with enzyme-linked immunosorbent assay (ELISA). The reference range of TSH on overall and reference population was 0.39–5.20 and 0.39–5.13 uIU/ml (2.5th–97.5th percentiles), respectively. In the reference population, the range (2.5th to 97.5th percentile) of serum TSH in different age groups was 0.40–5.03 uIU/ml, 0.39–5.15 uIU/ml, 0.37–6.10 uIU/ml, and 0.44–7.03 uIU/ml, respectively. The mean TSH value in women aged 26–35 years was 2.26 uIU/ml, significantly lower than those aged 36–45 (p < 0.001). The mean TSH values for eastern, central, and western regions were 2.28 uIU/ml, 2.29 uIU/ml, and 2.24 uIU/ml respectively. The mean of serum TSH concentration was significantly higher in central region than that in western region (p ≤ 0.001). The TSH value 0.39–5.13 uIU/ml (2.5th–97.5th percentiles) was derived as a reference range of reproductive age women from rural China. We use the TSH ranges from reference population to diagnose hyperthyrotropinemia or hypothyroidism in different areas in China. The reference ranges for eastern, central, and western regions were 0.33–5.61 uIU/ml, 0.40–5.04 uIU/ml, and 0.40–4.98 uIU/ml (2.5th–97.5th percentiles) respectively. The value of serum TSH was associated with age, living region, smoking, drinking, educational level, and interpersonal tension, as well as life and economic pressure, but irrelevant to ethnicity or occupation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Thyroid hormone is one of the most important hormones to ensure fetal normal growth and development. In the first 11 weeks of gestation, fetuses cannot produce thyroid hormone by themselves, so they still depend on maternal thyroid hormone. Pregnant women with hypothyroidism may exert a significantly negative impact on their children, especially during early pregnancy [1,2,3,4]. Understanding the thyroid function status of childbearing age women is vital for giving birth to healthy babies. The clinical definition of thyroid dysfunction derived from the reference ranges of TSH and thyroid hormones. Subclinical hypothyroidism or subclinical hyperthyroidism is defined as abnormally increased or decreased serum TSH level, respectively, with a normal serum-free thyroxine (fT4) level. The diagnosis of thyroid dysfunction, especially subclinical dysfunction, is heavily affected by the validity of the TSH reference range. However, the optimal reference value of serum TSH and clinical significance of subclinical thyroid dysfunction are still controversial [5]. In addition, it is difficult for the childbearing women to detect subclinical hypothyroidism in the early stage of pregnancy. The prevalence of subclinical hypothyroidism has been reported to vary from 3 to 12%, and that of subclinical hyperthyroidism to vary from 1 to 6% [6, 7]. Therefore, the National Academy of Clinical Biochemistry (NACB) suggested that the serum TSH reference range should be established in rigorously screened normal euthyroid volunteers without evidence of thyroid diseases [8].
There were several reference intervals derived from thyroid functional tests have been published [9,10,11]. Previously, the incidence and prevalence of hypothyroidism or hyperthyroidism of Chinese women have been reported by several studies [12,13,14]. However, a large nationwide epidemiological study evaluating the reference range of serum TSH has never been implemented in rural Chinese women of reproductive age. Therefore, the diagnosis and treatment of thyroid diseases in reproductive age women remain great challenges to physicians, especially in rural China. We aimed to perform a large-scale population-based study to assess the value of serum TSH in women aged 15–55 years, in order to provide valuable information on patterns of thyroid function in rural China. We also aimed to establish a universal reference range of serum TSH levels on different age groups of women in rural China based on the survey data obtained from the NFPHEP (2010 to 2012).
Subjects and Methods
Study Population
The data set was derived from the NFPHEP. This project was launched by the National Health and Family Planning Commission and Ministry of Finance in China, aiming to provide free health examination for rural married couples who planned to have babies. This study was a nationwide population-based data survey of the rural Chinese who were aged from 15 to 55 years living in 28 provinces of China mainland. Sample collection was performed from 1 January 2010 to 31 December 2012. Couples who planned to have a baby were randomly enrolled by local community staff and signed information consent. Free medical examination and counseling service were provided by well-trained local medical workers. Files were then recorded in a web-based electronic data collection system and sent to the NFPHEP office. The detailed protocol, organization, and implementation of this project were documented elsewhere [15, 16]. Missing data and the extreme values (e.g., TSH > 1000 uIU/ml) were excluded from the subsequent statistical analyses. Thus, the overall population included 392,659 women, while the reference population included 359,895 women.
Study Design
For overall population, a standard questionnaire was used to collect the basic information on age, education level, occupation, ethnicity, residence address, medical history, drug history, family history, life pressure, economic pressure, and interpersonal tension. The overall population was defined as subjects that underwent thyroid function tests in the NFPHEP with a TSH value of ≤ 1000 uIU/ml. The reference population was defined as subjects without thyroid-related diseases or any other diseases that can cause changes in TSH levels, having any family diseases history, or taking any medications. Life pressure, economic pressure, and interpersonal tension were defined as socio-psychological factors which depend on participants’ own feeling.
According to age distribution, the reference population was categorized into various age groups (15–25, 26–35, 36–45, and 46–55). As to residential addresses, participants from 28 provinces were divided into three regions: eastern region (including Beijing, Fujian, Guangdong, Jiangsu, Liaoning, Shandong, and Zhejiang), central region (including Anhui, Hainan, Hebei, Heilongjiang, Henan, Hubei, Hunan, Jiangxi, Jilin, and Shanxi), and western region (including Chongqing, Gansu, Guangxi, Guizhou, Inner Mongolia, Ningxia, Qinghai, Shaanxi, Sichuan, Yunnan, and Xinjiang).
Serum Analysis
In order to evaluate serum TSH, approximately 5 ml of peripheral blood from each participate was collected. Within 30 min after separating the serum, the sample was transferred to the testing facility. Collected specimens were analyzed by ELISA kits within 24 h after collection. The ELISA kits with the same reference intervals, approved by the China Food and Drug Administration, were chosen by the local laboratories.
Statistical Analysis
Big data set seems to follow the law of large numbers and the central limit theorem. So the whole sampled big data is normal distribution. The reference range of TSH was expressed with the 2.5th and 97.5th percentiles, as described previously [17,18,19,20]. Student’s t test and one-way ANOVA test were applied to compare two or multiple groups, with respect to continuous and discrete variables. Comparisons of sub-data sets among different age and region groups were completed by using one-way ANOVA tests. Statistical analysis was performed using SPSS software (IBM SPSS Statistics, version 20.0; SPSS, Inc., Chicago, IL). A p value of < 0.05 was considered statistically significant.
Results
Baseline Characteristics of the Subjects
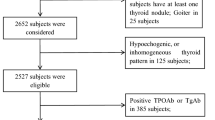
Strict inclusion and exclusion criteria were applied to this study. Step 1, we excluded the subjects with a TSH value > 1000 uIU/ml, so the overall population aged 15–55 years who underwent thyroid function tests in the NFPHEP (from 2010 to 2012) included 392,659 subjects. Step 2, we excluded 14,036 subjects with thyroid-related diseases or any other diseases that can cause changes in TSH levels. Step 3, we excluded 5413 subjects with any family disease history. Step 4, we excluded 13,315 subjects taking any medications. Finally, the reference population comprised of 359,895 subjects (Fig. 1).

Recruitment and participation of the study subjects
Serum TSH Concentrations in Total Population and Reference Population
In overall population, the mean value of serum TSH was 2.28 uIU/ml, with a range (2.5th to 97.5th percentile) of 0.39–5.20 uIU/ml. In the reference population, the mean value of serum TSH was 2.27 uIU/ml, with a range of 0.39–5.13 uIU/ml (2.5th to 97.5th percentile). The reference population was categorized into four age groups (15–25, 26–35, 36–45, and 46–55 years old). The mean TSH values were increased with age ascending. The range (2.5th to 97.5th percentile) of serum TSH in different age groups was 0.40–5.03 uIU/ml, 0.39–5.15 uIU/ml, 0.37–6.10uIU/ml, and 0.44–7.03 uIU/ml, respectively. One-way ANOVA was applied to compare the variation among different age groups. In the reference population, the mean TSH value in women aged 26–35 years was 2.26 uIU/ml, significantly lower than those aged 36–45 (p < 0.001). No significant difference was observed between 15–25 and 26–35 age groups (p = 0.520) or between 36–45 and 46–55age groups (p = 0.138) (Table 1). We found that most of the subjects were distributed within the range of 1.01 to 2.0 with the same trend in two groups (Fig. 2). The mean value of TSH in overall population was higher than that in the reference population, divided by age groups (Fig. 3).

Mean of serum TSH distribution in total and reference population

Mean of serum TSH in total and reference population of different age groups
Serum TSH Concentrations in Three Regions
The reference population was categorized into three region groups (eastern region, central region, and western region). In the eastern region population, the mean value of serum TSH was 2.28 uIU/ml, with a range (2.5th to 97.5th percentile) of 0.33–5.61 uIU/ml. In the central region population, the mean value of serum TSH was 2.29 uIU/ml, with a range (2.5th to 97.5th percentile) of 0.4–5.04 uIU/ml. In the western region population, the mean value of serum TSH was 2.24 uIU/ml, with a range (2.5th and 97.5th percentile) of 0.4–4.98 uIU/ml. The medians of serum TSH levels were all the same in all subgroups, 1.99 uIU/ml (Table 2). One-way ANOVA was performed to compare the TSH levels among three region groups. Serum TSH concentration was significantly higher in central region than that in western region (p ≤ 0.001, Table 2), while there was no difference between eastern and central region (Table 2).
Sociodemographic Characteristics of Participants
In the reference population, 359,895 women were assessed. Each participant was documented in detail on ethnicity, occupation, education level, smoking, alcohol intake, life pressure, economic pressure, and interpersonal tension. As shown in Table 3, 70.2% of the subjects only graduated from junior middle school. Most of them were Han ethnicity (95.4%), farmers (79.3%), non-smokers (99.1%), non-drinkers (95.7%), without life pressure (80.3%), without economic pressure (80.2%), or without interpersonal tension (89.0%). Serum TSH was significantly higher among women who were smoking, drinking, and uneducated (p < 0.0001) (Table 3). The mean value of TSH was positively correlated with life/economic pressure and interpersonal tension (p < 0.0001) (Table 3 and Fig. 4). There was no significant difference in TSH distribution by ethnicity or occupation, as indicated by one-way ANOVA or Student’s t test (Table 3).

Mean of serum TSH among different levels of life pressure, economic pressure, and interpersonal tension groups in reference population
Discussion
This population-based epidemiologic study on TSH levels of 359,895 women from rural China was the first attempt, as far as we know. We compare the levels of serum TSH in the reference population to several other studies. The results were different among Asian, European, and American countries. For instance, Korea National Health and Nutrition Examination Survey (KNHANES) (2013 to 2015) reported the 2.5th and 97.5th percentile of serum TSH as 0.6 and 7.21 uIU/ml, respectively, in the reference population of female [21]. In Finland, the Health 2000 Survey reported the 2.5th and 97.5th percentile as 0.39 and 3.22 uIU/ml, respectively [22]. In the USA, National Health and Nutrition Examination Survey (NHANES III) (1988 to 1994) reported the 2.5th and 97.5th percentile as 0.41 and 4.09 uIU/ml, respectively [17]. In our study, the corresponding value of the reference population was 0.39–5.13 uIU/ml. Comparing with the above three studies, the difference might stem from sampling bias and non-sampling bias, such as screening strategies, laboratory assays, and immunoassay methods, as described previously [18, 22,23,24].
In our study, the mean value of TSH was positively correlated with age. In several relevant literatures, the TSH value was significantly affected by age [17, 25,26,27,28,29]; however, this was not the case in other studies [18, 30, 31]. We suggest that age-specific reference limits should be used for thyroid function tests by the NACB guidelines [8].
Other factors, such as gender, thyroidauto-antibodies, iodine intake, and investigation methods [25, 32, 33], might have contributed to different levels of serum TSH in Chinese. However, limited by resource, this study did not evaluate the above factors. We evaluated the effects of resident areas on TSH levels, and found that the value of TSH was significantly higher in the central region than in the western region of China. This phenomenon could be due to different iodine intake or eating habits in the above regions. The iodine intake could contribute to differential distribution of serum TSH in rural China. Guan H et al. [34] showed “a urinary iodine-related increase of serum TSH levels in areas according to different levels of iodine intake.” They also found that “iodine nutrition was an important factor associated with TSH concentration, even in the rigorously selected reference population.” Rebagliato observed “an increased risk of TSH above 3.0 mIU/L in pregnant women who consumed 200 μg or more of iodine supplements daily compared with those who consumed less than 100 μg/d” [35]. Orito found “significant positive correlations between urinary iodine concentration and TSH” [36]. There may be two reasons for high TSH caused by an increased iodine intake. Firstly, Papanastasiou reported “a strong association of thyroid autoimmunity with increased serum TSH aggravated by high iodine intake has been reported due to increased iodination of thyroglobulin or direct stimulation of immune cells” [37]. Xiaoguang Shi reported that “thyroid autoimmunity might impair the thyroid sufficiently to raise TSH” [38]. Next, Li N’s animal study offers another explanation “the activity of deiodinase-II in the hypothalamus and pituitary was significantly inhibited by chronically increased iodine intake, which reduced T3 production in the hypothalamus and the pituitary and resulted in increased TSH production” [39]. Rosene reported the same results in amiodarone treated mice [40].
At the same time, we found that the value of TSH was significantly associated with smoking, drinking, education, life/economic pressure, or interpersonal tension. The increase in pressure or tension may result in an increase in TSH concentration. However, the effect of cigarette smoking on thyroid function is controversial. Several studies have reported that smokers have a lower prevalence of TPOAb [41] and a lower level of TSH [41, 42]. Another study has proposed that the effect of smoking on thyroid function differs according to iodine intake [42], which suggests that compounds from cigarettes interact with iodine in the thyroid gland.
Predetermined strict exclusion criteria had excluded 32,764 (8.34%) samples and left 359,895 subjects as the reference population. To some extent, the exclusion criteria were even stricter than NACB guidelines [8]. As the value of TSH might be affected by many diseases [43,44,45,46,47], it might be related to family history or medications. Meanwhile, we excluded extreme values of TSH (≥ 1000 uIU/ml), since the detection range of ELISA kits was 0–1000 uIU/ml. The extreme values may be caused by input mistakes or non-sampling errors.
Our study has the following limitations, which should be improved in future studies. Firstly, the NFPHEP study targeted only on the couples who were planning to have babies in rural China. The values of TSH in single women or in the couples who were not planning to have babies in rural China could be underestimated or ignored. Meanwhile, married women who were preparing to have babies deliberately avoided smoking and drinking, so women who were smoking and drinking in the reference population were very few, only accounting for 0.9 and 4.3%, respectively. Therefore, this population may not be representative for ordinary population. In the future, we plan to recruit unmarried women to our ongoing study. Secondly, more detailed histories and physical examination findings should be collected, such as iodine intake which has been considered as an important factor associated with TSH concentration in previous studies [34]. However, in a large-scale survey, it is hard for the researchers to collect the histories completely and sufficiently. Thirdly, restricted by the funds and human resources, the serum levels of TgAb and TPOAb were not measured. As a result, we could not follow all the stringent criteria of the NACB guidelines [8]. TPOAb-positivity had a substantial effect on the TSH upper limit in some studies [18, 22, 27], yet in other studies, the effect was nonexistent or less pronounced [19, 48]. It was reported that the effect of TPOAb-positivity was apparent only among women [49]. TPOAb presented a high sensitivity for screening for thyroid related diseases [22]. Therefore, TgAb and TPOAb should be investigated in our future studies, which deserves more efforts to set up a reliable, accurate, and reproducible reference range of TSH, especially for Chinese population. Finally, there were many influential factors in ELISA measurement. Samples, reagents and operating factors all influence the test results, especially the difficulty in standardization of manual operation was one of the limiting factors in present study.
In conclusion, we collected and analyzed the TSH data and sociodemographic characteristics of 359,895 women of reproductive age in rural China. We obtained that the normal TSH reference range for them was 0.39–5.13 uIU/ml (2.5th–97.5th percentiles). We suggest that people from different regions should have different reference ranges of TSH to diagnose hyperthyrotropinemia or hypothyroidism. The reference ranges for eastern, central, and western regions were 0.33–5.61 uIU/ml, 0.40–5.04 uIU/ml and 0.40–4.98 uIU/ml (2.5th–97.5th percentiles) respectively.
Abbreviations
- TSH:
-
Thyroid-stimulating hormone
- fT4:
-
Free thyroxine
- TPOAb:
-
Thyroid peroxidase antibody
- TgAb:
-
Thyroglobulin antibody
- NFPHEP:
-
National Free Preconception Health Examination Project
- ELISA:
-
Enzyme-linked immunosorbent assay
- NACB:
-
National Academy of Clinical Biochemistry
References
Utiger RD (1999) Maternal hypothyroidism and fetal development [J]. N Engl J Med 341(8):601–602
de Escobar GM, Ares S, Berbel P, Obregón MJ, del Rey FE (2008) The changing role of maternal thyroid hormone in fetal brain development [J]. Semin Perinatol 32(6):380–386
Haddow JE, McClain MR, Palomaki GE et al (2011) Thyroperoxidase and thyroglobulin antibodies in early pregnancy and placental abruption [J]. Obstet Gynecol 117(2 Pt 1):287–292
Nazarpour S, Tehrani FR, Simbar M et al (2015) Thyroid dysfunction and pregnancy outcomes [J]. Iran J Reprod Med 13(7):387–396
Biondi B, Cooper DS (2008) The clinical significance of subclinical thyroid dysfunction [J]. Endocr Rev 29(1):76–131
Kim YA, Park YJ (2014) Prevalence and risk factors of subclinical thyroid disease [J]. Endocrinol Metab 29(1):20–29
Boekholdt SM, Titan SM, Wiersinga WM, Chatterjee K, Basart DCG, Luben R, Wareham NJ, Khaw KT (2010) Initial thyroid status and cardiovascular risk factors: the EPIC-Norfolk prospective population study [J]. Clin Endocrinol 72(3):404–410
Baloch Z, Carayon P, Conte-Devolx B, Demers LM, Feldt-Rasmussen U, Henry JF, LiVosli V, Niccoli-Sire P, John R, Ruf J, Smyth PP, Spencer CA, Stockigt JR, Guidelines Committee, National Academy of Clinical Biochemistry (2003) Laboratory medicine practice guidelines. Laboratory support for the diagnosis and monitoring of thyroid disease [J]. Thyroid 13(1):3–126
Iwaku K, Noh JY, Minagawa A, Kosuga Y, Suzuki M, Sekiya K, Matsumoto M, Ohye H, Kunii Y, Yoshihara A, Watanabe N, Mukasa K, Ito K, Ito K (2013) Determination of pediatric reference levels of FT3, FT4 and TSH measured with ECLusys kits [J]. Endocr J 60(6):799–804
Loh TP, Sethi SK, Metz MP (2015) Paediatric reference interval and biological variation trends of thyrotropin (TSH) and free thyroxine (T4) in an Asian population [J]. J Clin Pathol 68(8):642–647
Zhang X, Yao B, Li C, Mao J, Wang W, Xie X, Teng X, Han C, Zhou W, Li C, Xu B, Bi L, Meng T, du J, Zhang S, Gao Z, Yang L, Fan C, Teng W, Shan Z (2016) Reference intervals of thyroid function during pregnancy: self-sequential longitudinal study versus cross-sectional study [J]. Thyroid 26(12):1786–1793
Liu J, Yu X, Meng X et al (2017) Development of gestation-specific reference intervals for thyroid hormones in normal pregnant Northeast Chinese women: what is the rational division of gestation stages for establishing reference intervals for pregnancy women?[J]. Clin Biochem 50(6):309–317
Liu H, Shan Z, Li C, Mao J, Xie X, Wang W, Fan C, Wang H, Zhang H, Han C, Wang X, Liu X, Fan Y, Bao S, Teng W (2014) Maternal subclinical hypothyroidism, thyroid autoimmunity, and the risk of miscarriage: a prospective cohort study [J]. Thyroid 24(11):1642–1649
Han C, Li C, Mao J et al (2015) High body mass index is an Indicator of maternal hypothyroidism, hypothyroxinemia, and thyroid-peroxidase antibody positivity during early pregnancy [J]. Biomed Res Int 2015(3):1–7
Sun L, Wang Q, Shen H, Liu M, Ma X, Ye H, Liu X, Pan H, du Z, Zhang Y, Yan D, Wang Y, Pan Y, Zhang S (2015) Evaluation and trend analysis of prepregnancy nutrition in Chinese women of reproductive age during 2010–2012 [J]. Zhonghua Yi Xue Za Zhi 95(3):181–186
Wang QM, Zhang M, Zhang SK et al (2015) Establishment of quality assurance system of the national free preconception health care project in China in Chinese [J]. Zhonghua Yi Xue Za Zhi 95:166–168
Hollowell JG, Staehling NW, Flanders WD, Hannon WH, Gunter EW, Spencer CA, Braverman LE (2002) Serum TSH, T(4), and thyroid antibodies in the United States population (1988 to 1994): National Health and nutrition examination survey (NHANES III) [J]. J Clin Endocrinol Metab 87(2):489–499
Schalin-Jäntti C, Tanner P, Välimäki MJ, Hämäläinen E (2011) Serum TSH reference interval in healthy Finnish adults using the Abbott Architect 2000i Analyzer [J]. Scand J Clin Lab Invest 71(4):344–349
Kratzsch J, Fiedler GM, Leichtle A, Brügel M, Buchbinder S, Otto L, Sabri O, Matthes G, Thiery J (2005) New reference intervals for thyrotropin and thyroid hormones based on National Academy of Clinical Biochemistry criteria and regular ultrasonography of the thyroid [J]. Clin Chem 51(8):1480–1486
Bjoro T, Holmen J, Krüger O et al (2000) Prevalence of thyroid disease, thyroid dysfunction and thyroid peroxidase antibodies in a large, unselected population. The health study of Nord-Trondelag (HUNT)[J]. Eur J Endocrinol 143(5):639–647
Kim WG, Kim WB, Woo G, Kim H, Cho Y, Kim TY, Kim SW, Shin MH, Park JW, Park HL, Oh K, Chung JH (2017) Thyroid stimulating hormone reference range and prevalence of thyroid dysfunction in the Korean population: Korea National Health and nutrition examination survey 2013 to 2015[J]. Endocrinol Metab 32(1):106–114
Lang VL, Niiranen TJ, Mi J et al (2014) Thyroid-stimulating hormone reference range and factors affecting it in a nationwide random sample [J]. Clin Chem Lab Med 52(12):1807–1813
Waise A, Price HC (2009) The upper limit of the reference range for thyroid-stimulating hormone should not be confused with a cut-off to define subclinical hypothyroidism [J]. Ann Clin Biochem 46(Pt 2):93–98
Spencer CA, Takeuchi M, Kazarosyan M, MacKenzie F, Beckett GJ, Wilkinson E (1995) Interlaboratory/intermethod differences in functional sensitivity of immunometric assays of thyrotropin (TSH) and impact on reliability of measurement of subnormal concentrations of TSH [J]. Clin Chem 41(3):367–374
Surks MI, Boucai L (2010) Age- and race-based serum thyrotropin reference limits [J]. J Clin Endocrinol Metab 95(2):496–502
Surks MI, Hollowell JG (2007) Age-specific distribution of serum thyrotropin and antithyroid antibodies in the U.S. population: implications for the prevalence of subclinical hypothyroidism [J]. J Clin Endocrinol Metab 92(12):4575–4582
Friishansen L, Hilsted L (2008) Reference intervals for thyreotropin and thyroid hormones for healthy adults based on the NOBIDA material and determined using a modular E170 [J]. Clin Chem Lab Med 46(9):1305–1312
Atzmon G, Barzilai N, Hollowell JG, Surks MI, Gabriely I (2009) Extreme longevity is associated with increased serum thyrotropin [J]. J Clin Endocrinol Metab 94(4):1251–1254
Takeda K, Mishiba M, Sugiura H et al (2009) Evaluated reference intervals for serum free thyroxine and thyrotropin using the conventional outliner rejection test without regard to presence of thyroid antibodies and prevalence of thyroid dysfunction in Japanese subjects [J]. Endocr J 56(9):1059–1066
O'Leary PC, Feddema PH, Michelangeli VP, Leedman PJ, Chew GT, Knuiman M, Kaye J, Walsh JP (2006) Investigations of thyroid hormones and antibodies based on a community health survey: the Busselton thyroid study [J]. Clin Endocrinol 64(1):97–104
Hoogendoorn EH, Hermus AR, Vegt FD et al (2006) Thyroid function and prevalence of anti-thyroperoxidase antibodies in a population with borderline sufficient iodine intake: influences of age and sex [J]. Clin Chem 52(1):104–111
Gannagéyared M, Balech N, Farah V et al (2017) Pediatric TSH reference intervals and prevalence of high thyroid antibodies in the Lebanese population [J]. Int J Endocrinol 2017(3):1–6
Cho NH, Choi HS, Kim KW, Kim HL, Lee SY, Choi SH, Lim S, Park YJ, Park DJ, Jang HC, Cho BY (2010) Interaction between cigarette smoking and iodine intake and their impact on thyroid function [J]. Clin Endocrinol 73(2):264–270
Guan H, Shan Z, Teng X, Li Y, Teng D, Jin Y, Yu X, Fan C, Chong W, Yang F, Dai H, Yu Y, Li J, Chen Y, Zhao D, Shi X, Hu F, Mao J, Gu X, Yang R, Chen W, Tong Y, Wang W, Gao T, Li C, Teng W (2008) Influence of iodine on the reference interval of TSH and the optimal interval of TSH: results of a follow-up study in areas with different iodine intakes [J]. Clin Endocrinol 69(1):136–141
Rebagliato M, Murcia M, Espada M, Álvarez-Pedrerol M, Bolúmar F, Vioque J, Basterrechea M, Blarduni E, Ramón R, Guxens M, Foradada CM, Ballester F, Ibarluzea J, Sunyer J (2010) Iodine intake and maternal thyroid function during pregnancy [J]. Epidemiology 21(1):62–69
Orito Y, Oku H, Kubota S, Amino N, Shimogaki K, Hata M, Manki K, Tanaka Y, Sugino S, Ueta M, Kawakita K, Nunotani T, Tatsumi N, Ichihara K, Miyauchi A, Miyake M (2009) Thyroid function in early pregnancy in Japanese healthy women: relation to urinary iodine excretion, emesis, and fetal and child development [J]. J Clin Endocrinol Metab 94(5):1683–1688
Papanastasiou L, Vatalas IA, Koutras DA, Mastorakos G (2007) Thyroid autoimmunity in the current iodine environment [J]. Thyroid 17(8):729–739
Shi X, Han C, Li C, Mao J, Wang W, Xie X, Li C, Xu B, Meng T, du J, Zhang S, Gao Z, Zhang X, Fan C, Shan Z, Teng W (2015) Optimal and safe upper limits of iodine intake for early pregnancy in iodine-sufficient regions: a cross-sectional study of 7,190 pregnant women in China [J]. J Clin Endocrinol Metab 100(4):1630–1638
Li N, Jiang Y, Shan Z, Teng W (2012) Prolonged high iodine intake is associated with inhibition of type 2 deiodinase activity in pituitary and elevation of serum thyrotropin levels [J]. Br J Nutr 107(5):674–682
Rosene ML, Wittmann G, Arrojo eDR et al (2010) Inhibition of the type 2 iodothyronine deiodinase underlies the elevated plasma TSH associated with amiodarone treatment [J]. Endocrinology 151(12):5961–5970
Belin RM, Astor BC, Powe NR, Ladenson PW (2004) Smoke exposure is associated with a lower prevalence of serum thyroid autoantibodies and thyrotropin concentration elevation and a higher prevalence of mild thyrotropin concentration suppression in the third National Health and Nutrition Examination Survey (NHANES III) [J]. J Clin Endocrinol Metab 89(12):6077–6086
Vejbjerg P, Knudsen N, Perrild H, Carlé A, Laurberg P, Pedersen IB, Rasmussen LB, Ovesen L, Jørgensen T (2008) The impact of smoking on thyroid volume and function in relation to a shift towards iodine sufficiency [J]. Eur J Epidemiol 23(6):423–429
Souza LL, Guedes EP, Teixeira PF et al (2016) Serum TSH levels are associated with cardiovascular risk factors in overweight and obese adolescents [J]. J Pediatr 92(5):532–538
Fu J, Yang A, Zhao J, Zhu Y, Gu Y, Xu Y, Chen D (2017) The relationship between iron level and thyroid function during the first trimester of pregnancy: a cross-sectional study in Wuxi, China [J]. J Trace Elem Med Biol 43:148–152
Rondeau G, Rutamucero N, Messier V, Burlacu L, Prud'homme D, Mircescu H, Rabasa-Lhoret R (2010) Reference range thyroid-stimulating hormone is associated with physical activity energy expenditure in overweight and obese postmenopausal women: a Montreal-Ottawa new emerging team study [J]. Metab Clin Exp 59(11):1597–1602
Nie X, Chen Y, Chen Y, Chen C, Han B, Li Q, Zhu C, Xia F, Zhai H, Wang N, Lu Y (2017) Lead and cadmium exposure, higher thyroid antibodies and thyroid dysfunction in Chinese women [J]. Environ Pollut 230:320–328
Ndrepepa G, Braun S, Mayer K, Cassese S, Fusaro M, Byrne RA, Hoppmann P, Schunkert H, Laugwitz KL, Kastrati A (2015) Prognostic value of thyroid-stimulating hormone within reference range in patients with coronary artery disease [J]. Metab Clin Exp 64(10):1308–1315
Chan AOK, Iu YP, Shek CC (2011) The reference interval of thyroid-stimulating hormone in Hong Kong Chinese [J]. J Clin Pathol 64(5):433–466
Eskelinen S, Suominen P, Vahlberg T, Löppönen M, Isoaho R, Kivelä SL, Irjala K (2005) The effect of thyroid antibody positivity on reference intervals for thyroid stimulating hormone (TSH) and free thyroxine (FT4) in an aged population [J]. Clin Chem Lab Med 43(12):1380–1385
Funding
This work was supported by the Chinese Association of Maternal and Child Health Studies (AMCHS-2014-03) and National Key R&D Plan (2016YFC1000702).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no competing interests.
Rights and permissions
About this article

Cite this article
Su, Q., Zhang, S., Hu, M. et al. Reference Range and Sociodemographic Characteristics of TSH among Reproductive Age Women in Rural China. Biol Trace Elem Res 189, 336–343 (2019). https://doi.org/10.1007/s12011-018-1480-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12011-018-1480-1