
Abstract
The purpose of this study was to analyze the existing studies and to investigate the relationship between the risk of colorectal cancer (CRC) and intakes of four individual dietary elements calcium (Ca), iron (Fe), magnesium (Mg), and potassium (K). All relevant articles in both Chinese and English were searched and collected from PubMed, Web of Science, and Chinese National Knowledge Infrastructure databases up to December 17, 2017. There were 29 eligible literatures selected for further meta-analysis, including 14 cohort studies and 15 case-control studies. The meta-analysis of cohort studies indicated that the high intakes of dietary Ca and Mg were negatively associated with the risk of CRC, as the hazard ratios (HR) were 0.76 (95% confidence interval (CI) 0.72, 0.80) and 0.80 (95% CI 0.73, 0.87), respectively. Nevertheless, high intake of dietary heme Fe was positively correlated to the incidence of colon cancer (HR = 1.01, 95% CI 0.82, 1.19) and rectal cancer (HR = 1.04, 95% CI 0.67, 1.42). A meta-analysis of case-control studies indicated that high intakes of dietary Ca, Mg, and K were negatively related with the occurrence of CRC, because the odds ratios (OR) were 0.36 (95% CI 0.32, 0.40), 0.80 (95% CI 0.63, 0.98) and 0.97 (95% CI 0.74, 1.21), respectively. However, high Fe intake from diet was positively correlated with the rising increasing of CRC (OR = 1.04, 95% CI 0.91, 1.18). More research is needed to indicate the risk relationship between element intake and CRC.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Colorectal cancer (CRC) is the third most common cancer around the world. Dietary and lifestyle factors play an important role in the etiology of CRC; a healthy diet and lifestyle can prevent a large number of CRC incidences and morbidities [1,2,3]. Generally, the dietary food sources are quite different from various geographical areas; the intake of macro and trace elements from diet varies accordingly among humans [4]. With the progress of economics and the change of environment, excessive amounts of mineral elements are found in food or drinking water. Although elements are indispensable to the human body, excessive, inadequate, or unbalanced elements can lead to different levels of physical abnormality or disease [5, 6]. In the past 20 years, the importance of trace elements has been widely recognized, and it is of great significance for biological monitoring of trace element concentration in various media such as blood or urine [7]. In patients with CRC, the cancer tissues and non-cancerous tissues showed significant differences in the concentration of trace elements, suggesting that these elements might play a vital role in the development of cancer [8]. However, to the best of our knowledge, very few analyses have focused on the relationship between different element intake levels and risk of CRC, although several studies reached inconsistent results [9, 10].
All the macroelements such as calcium (Ca), magnesium (Mg), and potassium (K), as well as trace element iron (Fe) can be obtained through diet or supplements [11]. Ca is a vital element in health and maintenance of growth and mature bones, and dietary Ca intake from fruits and vegetables has been reported to inversely relate to the risk of CRC [12,13,14]. Fe is an essential dietary element. Fe deficiency and heme Fe deficiency anemia are global health problems. However, the ability of Fe to cycle between oxidized and reduced forms also renders it capable of contributing to free radical formation, which may have deleterious effects, including promutagenic effects that can potentate tumor formation [15]. Additionally, previous epidemiological data besides showed a suggestive association between dietary heme Fe and risk of colon cancer [16]. Mg is crucial for every cell, and low concentration of Mg increases the risk of various diseases [17]. Mg plays a key role in maintenance of gastrointestinal and hormonal functions; there is convincing evidence that intake of garlic and Mg may significantly protect against developing CRC [14]. K is a nutrient that easily deficient for human health because it is usually not present in foods or is commonly eaten as a dietary supplement [18]. A high intake of dietary K is a statistically significant protective factor in females and males for CRC [9]. Since the effect of element intakes from diet associated with CRC has been widely concerned in recent years, the controversy results have continued to confuse physicians and patients alike. Therefore, the purpose of this study was to explore the relationship between the high intake of these four elements (Ca, Fe, Mg, and K, respectively) and the incidence of CRC through a meta-analysis of cohort and case-control studies.
Materials and Methods
Search Strategy
This study was conducted according to Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines [19].PubMed, Web of Science, and Chinese National Knowledge Infrastructure (CNKI) databases were queried by using the following keywords, and all articles in both Chinese and English were collected from the inception date to December 17, 2017.
English retrieval strategy of PubMed and Web of Science databases are (1) colorectal cancer OR colon cancer OR rectal cancer OR rectum cancer OR colon and rectum cancer OR colorectal carcinoma OR colon carcinoma OR Colon rectum carcinoma OR carcinoma of colon and rectum OR CRC; (2) trace element OR microelement OR calcium OR Fe OR iron OR magnesium OR potassium OR kalium; and (3) (1) AND (2).
Chinese retrieval strategy of CNKI database are (1) trace element OR calcium OR Fe OR magnesium OR potassium; (2) colorectal cancer; and (3) (1) AND (2).
Study Selection
The initial selection of articles was based on titles and abstract to exclude studies unrelated to element intake and CRC. The collection of relevant data was extracted from the eligible studies according to the criteria listed below. (1) The study was a cohort or case-control; (2) results of the study included at least one dietary element in a person’s daily intake; (3) the outcome of interest was colorectal; (4) the hazard ratio (HR) estimates or odds ratio (OR) in case-control studies with corresponding 95% confidence interval (CI) were provided; and (5) potential confounders, including age, sex, BMI, and total energy intake and other factors should be adjusted.
Exclusion criteria included the following: (1) similar objective results in the same study or in the same institution at different times; (2) research has some problems, such as design defects and poor quality and smaller sample size (n < 200), and the data of the study is not complete; (3) the full text can neither be obtained from the database nor by contacting the author; (4) the statistical method had an error that cannot be modified and measurement data cannot provide the effect size; and (5) review articles.
Data Extraction and Quality Assessment
Data extraction from included studies was carefully performed by three independent authors to ensure the accuracy of the extracted information. The following data were extracted from each included eligible study using a standardized report form: the first author and the publishing time, follow years and time period, area, sex, age, the number of cases and participants, assessment method, the comparison of elemental intake, the HR or of CRC and the corresponding 95% CI, and covariate adjusted in each study. We extracted the value of the intake, and the corresponding 95% CI in the highest categories (tertile quartile or quintile) measured versus after HR or adjustment. HR is the ratio of the hazard rates corresponding with the conditions described by two levels of an explanatory variable. HR = P/(1 − P); P = HR/(1 + HR) [20]. OR refers to the number to the case group and the ratio with the exposure number divided by exposure to toll and the number of non exposed than in the control group, in epidemiological studies is a commonly used indicator of case-control study [21].
We employed Newcastle-Ottawa Scale (NOS) to assess the quality of all included studies [22]. The NOS used two different tools for the case–control and cohort studies, and consist of three parameters of quality: selection (0–4 points), comparability (0–2 points), and outcome (0–3 points) [23].NOS Scores ranged from 0 to 9, and we defined studies of high quality as those that scored 6–9 [24]. Discrepancy in quality assessment was discussed and resolved by the two reviewers. The literature with a score greater than 5 was included in our analysis [25].
Statistical Analysis
Subgroup analysis, heterogeneity testing, and publication bias assessment were performed according to the PRISMA checklist [19]. We used software Stata version 12.0 to analyze the data. All statistical tests were two-sided, and a P value < 0.05 was considered statistically significant.
The heterogeneity between studies was evaluated using the chi squared-based Q statistic and I2 statistic. If a P value for the Q statistic > 0.05 and I2 < 50%, there was a low heterogeneity in the included studies, and the results of fixed effect model were selected [26, 27]; if a P value for the Q statistic < 0.05 and I2 > 50%, there was evidence of substantial heterogeneity in the included studies, and then the random effect model would be chosen.
In addition, potential publication bias was investigated by the use of Begg’s funnel plots and Egger’s regression asymmetry test. When the measuring tool is the same, the effect size would further be used for analysis of data. On the contrary, if different measurement tools were used, we switched to standardized effect size. All analyses were performed with the 95% CI. When necessary, sensitivity analysis was performed to test the stability of the results.
Results
Study Characteristics
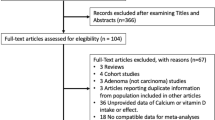
According to the retrieval strategy, there was a total of 29 eligible studies [28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56] selected in this meta-analysis, including a total of 14 cohort studies [28,29,30,31,32,33,34,35,36,37,38,39,40,41] and 15 case-control studies [42,43,44,45,46,47,48,49,50,51,52,53,54,55,56] (Fig. 1). We reported some characteristics of the included studies, such as the first author and the publishing time, follow years and time period, area, sex, age, the number of cases and participants, assessment method, and the comparison of elemental intake from each study between the highest categories (tertile, quartile, or quintile) and the lowest category. The characteristics of these studies were summarized in Tables 1 and 2.

Flowchart of the study selection process
Of the 14 cohort studies, researches focused on Ca, heme Fe, and Mg intakes which had 8, 2, and 6 studies, respectively. Of the 15 case-control studies, researches with respect to Ca, Fe, Mg, and K intakes contained 11, 9, 3, and 2 studies, respectively. Among them, 26 of the 29 studies included were published after 2000. Confounding variables in these studies (age, sex, body mass index, total energy intake, and other factors) were adjusted. We also evaluated the quality of 29 studies, as shown in Tables 1 and 2, both greater than 5, indicating that all these studies were of high quality.
Meta-Analyses of Cohort Studies
When all cohort studies were pooled, the obtained HR represented the risk of CRC. The HR of dietary Ca intake was 0.76 (95% CI 0.72, 0.80), the HR of dietary Mg intake was 0.80 (95% CI 0.73, 0.87), and the HR of dietary heme Fe intake was 1.00 (95% CI 0.87, 1.14) (Fig. 2). All these results demonstrated that dietary Ca and Mg intakes were negatively correlated to the risk of colorectal, colon, and rectal cancer in the subgroup meta-analysis of the study designed. Similarly, the risk of colon cancer was negatively correlated (HR = 0.99, 95% CI 0.77, 1.21) with dietary heme Fe intake (Fig. 2). However, the risk of CRC and rectal cancer in the subgroup meta-analysis was positively correlated with dietary heme Fe, as the HR was 1.01 (95% CI 0.82, 1.19) and 1.04 (95% CI 0.67, 1.42), respectively (Fig. 2). Our meta-analysis showed that higher dietary Ca and Mg intakes seemed to have a protective effect for CRC. Higher heme Fe intake appeared to be a risk factor for colorectal and rectal cancer and might have a protective effect for colon cancer.

Pooled random-effects HR (95% CI) of CRC risk comparing with the highest category of element intake from diet
Meta-Analyses of Case-Control Studies
Consistent with the cohort study, higher Ca and Mg intakes in case-control studies were still considered to be protective for CRC. The pooled OR for dietary Ca and Mg intakes were 0.36 (95% CI 0.32, 0.40) and 0.80 (95% CI 0.63, 0.98), respectively (Fig. 3). In addition, the OR of CRC of dietary K and Fe intakes were 0.97 (95% CI 0.74, 1.21) and 1.04 (95% CI 0.91, 1.18), respectively (Fig. 3). Analysis of case-control studies found that dietary high K intake might reduce the incidence of CRC, while high Fe intake from diet increased the risk of CRC.

Pooled random-effects OR (95% CI) of CRC risk comparing with the highest category of element intake from diet
Heterogeneity and Publication Bias
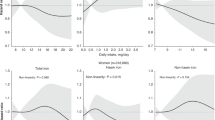
By comparing the different element intakes and risk of CRC, the differences in dietary Ca intake in the case control showed that there were significant heterogeneity in 11 studies (P < 0.01, I2 = 87.9%). According to the quality assessment of the studies and the availability of the full text, heterogeneity may be affected by these factors: sample size and age. By using a dependent variable of subgroup analysis and meta-regression, it showed that single or multiple covariates could explain the heterogeneity.
Begg’s funnel plots suggested the absence of asymmetry, we did not find any statistically significant publication bias in other groups. The funnel plots are shown in Figs. 4 and 5. It was confirmed that rectal cancer, colon cancer, and CRC was associated with the intakes of four elements through Egger regression asymmetrical test, respectively (all P > 0.05). Results of the Begg’s test of the cohort study showed that the P values of Ca, heme Fe, and Mg were 0.428, 0.754, and 0.127, respectively. Results of the Begg’s test in the case-control study indicated that the P values of Ca, Fe, Mg, and K were 0.592, 0.913, 0.296, and 1.000, respectively.

Begg’s funnel plot (with pseudo 95% CI) of all cohort studies in the meta-analysis

Begg’s funnel plot (with pseudo 95% CI) of all case-control studies in the meta-analysis
Discussion
To investigate the relationship between the risk of CRC and dietary intakes of individual Ca, Fe, Mg, and K elements, we conducted a meta-analysis containing 29 studies. We extracted HR or OR and corresponding 95% CI of each element in the included cohort and case-control studies, and further conducted subgroup analyses.
Most of the studies in this meta-analysis used the food frequency questionnaire (FFQ) to assess the extent of exposure. The FFQ is a dietary assessment tool widely used for epidemiological studies to study the relationship between dietary intake and disease or risk factors since the early 1990s [57]. In our meta-analysis, all cohort studies on the relationship between high intakes of Fe and the risk of CRC were all calculated as dietary intake of heme Fe. Dietary total Fe is present in food, and the most important form is heme Fe [58]. Heme Fe is mainly found in animal liver, animal blood, and red meat, which can be absorbed directly. Previous research have claimed that red meat consumption can replenish the Fe; however, the high consumption of red meat or its products, is not good for health, which will increase the risk of noncommunicable diseases, including cancer, type 2 diabetes, and cardiovascular diseases [59]. The meta-analysis of included cohort studies showed that the high heme Fe intake form diet was positively correlated to the incidence of CRC and rectal cancer, suggesting that high intake of dietary heme Fe might increase the risk of CRC and rectal cancer. In the meta-analysis of case-control studies, daily high Fe intake form diet was positively correlated with CRC morbidity, suggesting that excessive intake of dietary Fe might increase the risk of CRC.
Healthy lifestyle recommendations may improve dietary Mg intake and play an independent role in improving certain metabolites [60]. Our meta-analysis indicates that dietary intakes of Ca, Mg, and K may be protective factors for CRC, and high intake of them from diet may reduce the risk of CRC. Fe and heme Fe may be risk factors, and increased dietary intake may increase the risk of CRC. Previous meta-analyses have shown that higher dietary Mg intake appears to exhibit protective effects on cancer, especially CRC and female cancer [61,62,63]. Based on the literature we included, we found the highest category intake values for these four elements, and the intakes of Ca, Fe, Mg, K in the highest categories (tertile, quartile, or quintile) were greater than 505.77 mg/day, 12.9 mg/day, 319 mg/day, and 3424 mg/day, respectively (Tables 1 and 2). The adequate intake of Ca for people ages between 31–50 is 1000 mg/day, and ages between 50–70 is 1200 mg/day [64]. The recommended dietary allowance (RDAs) for Fe is 8 mg/day for men ages between 31–70 and for women over 50, and 18 mg/day for women ages between 31–50 [65]. RDAs for Mg are 420 mg/day for men ages between 31–70, which is 320 mg/day for women [64]. An adequate intake of K is 4700 mg/day [66]. Promoting a healthy human diet based on RDAs at these ages may play a vital role in preventing CRC.
This meta-analysis also has several limitations. First, as a meta-analysis of epidemiological studies, it does not allow for uniform confusion in all studies. For example, differences in follow-up time may skew the results from included studies. Second, because of the inability to accurately assess dietary K intake, our study only conducted a meta-analysis of two case-control studies. More studies are needed to confirm the relationship between the risk of CRC and high intake of dietary K. Finally, since we only extracted the HR or, the corresponding 95% of the element intake and the corresponding risk of CRC in the study could also lead to the deviation from the meta-analysis results.
In summary, this meta-analysis suggests that higher or increased intakes of individual dietary Ca, Mg, and K may help to reduce the risk of CRC slightly, whereas higher or increased intakes of dietary heme Fe and Fe, respectively may increase the risk of CRC. Therefore, more prospective studies are needed in future meta-analyses to further demonstrate that four individual element (Ca, Fe, Mg, and K) intakes are risk factors of CRC, and more relevant health policy should be carried out to prevent that hazard effect.
References
Kushi LH, Doyle C, McCullough M, Rock CL, Demark-Wahnefried W, Bandera EV, Gapstur S, Patel AV, Andrews K, Gansler T, American Cancer Society 2010 Nutrition and Physical Activity Guidelines Advisory Committee (2012) American Cancer Society Guidelines on nutrition and physical activity for cancer prevention: reducing the risk of cancer with healthy food choices and physical activity. CA Cancer J Clin 62:30–67
Platz EA, Willett WC, Colditz GA, Rimm EB, Spiegelman D, Giovannucci E (2000) Proportion of colon cancer risk that might be preventable in a cohort of middle-aged US men. Cancer Causes Control 11:579–588
Mehta M, Shike M (2014) Diet and physical activity in the prevention of colorectal cancer. J Natl Compr Cancer Netw 12:1721–1726
Welch AA, Fransen H, Jenab M, Boutron-Ruault MC, Tumino R, Agnoli C et al (2009) Variation in intakes of calcium, phosphorus, magnesium, iron and potassium in 10 countries in the European prospective investigation into cancer and nutrition study. Eur J Clin Nutr 63:101–121
Zhuo L, Wang C, Lu L, Mengyun S, Wang L, Xin L et al (2018) The study on the correlation between six kinds of mineral elements and diabetes. Biol Trace Elem Res 183:226–232
He D, Wang Z, Chuying H, Xiping F, Dian C (2017) Serum selenium levels and cervical cancer: systematic review and meta-analysis. Biol Trace Elem Res 179:195–202
Nordberg M, Nordberg GF (2016) Trace element research-historical and future aspects. J Trace Elem Med Biol 38:46–52
Sohrabi M, Gholami A, Azar MH, Yaghoobi M, Shahi MM, Shirmardi S et al (2017) Trace element and heavy metal levels in colorectal cancer: comparison between cancerous and non-cancerous tissues. Biol Trace Elem Res 183:1–8
Kune GA, Kune S, Watson LF (1989) Dietary sodium and potassium intake and colorectal cancer risk. Nutr Cancer 12:351–359
Lei Q, Yong F (2013) Intakes of heme iron and zinc and colorectal cancer incidence: a meta-analysis of prospective studies. Cancer Causes Control 24:1175–1183
Dawczynski C, Schäfer U, Leiterer M, Jahreis G (2007) Nutritional and toxicological importance of macro, trace, and ultra-trace elements in algae food products. J Agric Food Chem 55:10470–10475
Wilczynski C, Camacho P (2014) Calcium use in the management of osteoporosis: continuing questions and controversies. Curr Osteoporos Rep 12:396–402
Cho E, Smith-Warner SA, Spiegelman D, Beeson WL, van den Brandt PA, Colditz GA, Folsom AR, Fraser GE, Freudenheim JL, Giovannucci E, Goldbohm RA, Graham S, Miller AB, Pietinen P, Potter JD, Rohan TE, Terry P, Toniolo P, Virtanen MJ, Willett WC, Wolk A, Wu K, Yaun SS, Zeleniuch-Jacquotte A, Hunter DJ (2004) Dairy foods, calcium, and colorectal cancer: a pooled analysis of 10 cohort studies. J Natl Cancer Inst 96:1015–1022
Hou N, Huo D, Dignam JJ (2013) Prevention of colorectal cancer and dietary management. Chin Clin Oncol 2:13
Manz DH, Blanchette NL, Paul BT, Torti FM, Tortiet SV (2016) Iron and cancer: recent insights. Ann N Y Acad Sci 1368:149–161
Bastide NM, Pierre FH, Corpet DE (2011) Heme iron from meat and risk of colorectal cancer: a meta-analysis and a review of the mechanisms involved. Cancer Prev Res 4:177–184
Vormann J (2016) Magnesium: nutrition and homoeostasis. AIMS Public Healt 3:329–340
Weaver CM (2013) Potassium and health. Adv Nutr 4:368–377
MoherD LA, Tetzlaff J, Altman DG (2010) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg 8:336–341
Spruance SL, Reid JE, Grace M, Samore M (2004) Hazard ratio in clinical trials. Antimicrob Agents Chemother 48:2787–2792
Cole SR, Chu H, Nie L, Schisterman EF (2009) Estimating the odds ratio when exposure has a limit of detection. Int J Epidemiol 38:1674–1680
Zeng X, Zhang Y, Kwong JS, Zhang C, Li S, Sun F et al (2015) (2015) the methodological quality assessment tools for preclinical and clinical studies, systematic review and meta-analysis, and clinical practice guideline: a systematic review. J Evid Based Med 8:2–10
Stang A (2010) Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol 25:603–605
Lo CK, Mertz D, Loeb M (2014) Newcastle-Ottawa scale: comparing reviewers’ to authors’ assessments. BMC Med Res Methodol 14:45
Qi D, Li J, Jiang M, Liu C, Hu Y, Li M, Su J, Que B, Ji W (2015) The relationship between promoter methylation of p16 gene and bladder cancer risk: a meta-analysis. Int J Clin Exp Med 8:20701–20711
DerSimonian R, Laird N (2015) Meta-analysis in clinical trials revisited. Contemp Clin Trials 45:139–145
Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, Moher D, Becker BJ, Sipe TA, Thacker SB (2000) Meta-analysis of observational studies in epidemiology: a proposal for reporting. JAMA 283:2008–2012
Tantamango-Bartley Y, Knutsen SF, Jaceldo-Siegl K, Fan J, Mashchak A, Fraser GE (2017) Independent associations of dairy and calcium intakes with colorectal cancers in the Adventist Health Study-2 cohort. Public Health Nutr 20:2577–2586
Gorczyca AM, He K, Xun P, Margolis KL, Wallace JP, Lane D, Thomson C, Ho GYF, Shikany JM, Luo J (2015) Association between magnesium intake and risk of colorectal cancer among postmenopausal women. Cancer Causes Control 26:1761–1769
Murphy N, Norat T, Ferrari P, Jenab M, Bueno-de-Mesquita B, Skeie G, Olsen A, Tjønneland A, Dahm CC, Overvad K, Boutron-Ruault MC, Clavel-Chapelon F, Nailler L, Kaaks R, Teucher B, Boeing H, Bergmann MM, Trichopoulou A, Lagiou P, Trichopoulos D, Palli D, Pala V, Tumino R, Vineis P, Panico S, Peeters PHM, Dik VK, Weiderpass E, Lund E, Garcia JRQ, Zamora-Ros R, Pérez MJS, Dorronsoro M, Navarro C, Ardanaz E, Manjer J, Almquist M, Johansson I, Palmqvist R, Khaw KT, Wareham N, Key TJ, Crowe FL, Fedirko V, Gunter MJ, Riboli E (2013) Consumption of dairy products and colorectal cancer in the European prospective investigation into cancer and nutrition (EPIC). PLoS One 8:e72715
Dai Q, Shu XO, Deng X, Xiang YB, Li H, Yang G, Shrubsole MJ, Ji B, Cai H, Chow WH, Gao YT, Zheng W (2013) Modifying effect of calcium/magnesium intake ratio and mortality: a population-based cohort study. BMJ Open 3:e002111
Hara A, Sasazuki S, Inoue M, Iwasaki M, Shimazu T, Sawada N, Yamaji T, Takachi R, Tsugane S, Japan Public Health Center–based Prospective Study Group (2012) Zinc and heme iron intakes and risk of colorectal cancer: a population-based prospective cohort study in Japan. Am J Clin Nutr 96:864–873
Zhang X, Giovannucci EL, Wu K, Smith-Warner SA, Fuchs CS, Pollak M, Willett WC, Ma J (2012) Magnesium intake, plasma C-peptide, and colorectal cancer incidence in US women: a 28-year follow-up study. Br J Cancer 106:1335–1341
Li K, Kaaks R, Linseisen J, Rohrmann S (2011) Dietary calcium and magnesium intake in relation to cancer incidence and mortality in a German prospective cohort (EPIC-Heidelberg). Cancer Causes Control 22:1375–1382
Ma E, Sasazuki S, Inoue M, Iwasaki M, Sawada N, Takachi R, Tsugane S, for the Japan Public Health Center-based Prospective Study Group (2010) High dietary intake of magnesium may decrease risk of colorectal cancer in Japanese men. J Nutr 140:779–785
Park Y, Leitzmann MF, Subar AF, Hollenbeck A, Schatzkin A (2009) Dairy food, calcium, and risk of cancer in the NIH-AARP diet and health study. Arch Intern Med 169:391–401
Ishihara J, Inoue M, Iwasaki M, Sasazuki S, Tsugane S (2008) Dietary calcium, vitamin D, and the risk of colorectal cancer. Am J Clin Nutr 88:1576–1583
Kabat GC, Miller AB, Jain M, Rohan TE (2007) A cohort study of dietary iron and heme iron intake and risk of colorectal cancer in women. Br J Cancer 97:118–122
Park SY, Murphy SP, Wilkens LR, Nomura AM, Henderson BE, Kolonel LN (2007) Calcium and vitamin D intake and risk of colorectal cancer: the multiethnic cohort study. Am J Epidemiol 165:784–793
Folsom AR, Hong CP (2006) Magnesium intake and reduced risk of colon cancer in a prospective study of women. Am J Epidemiol 163:232–235
Lin J, Zhang SM, Cook NR, Manson JE, Lee IM, Buring JE (2005) Intakes of calcium and vitamin D and risk of colorectal cancer in women. Am J Epidemiol 161:755–764
Han C, Shin A, Lee J, Lee J, Park JW, Oh JH, Kim J (2015) Dietary calcium intake and the risk of colorectal cancer: a case control study. BMC Cancer 15:966
Ruder EH, Berndt SI, Gilsing AM, Graubard BI, Burdett L, Hayes RB et al (2014) Dietary iron, iron homeostatic gene polymorphisms and the risk of advanced colorectal adenoma and cancer. Carcinogenesis 35:1276–1283
Galas A, Augustyniak M, Sochacka-Tatara E (2013) Does dietary calcium interact with dietary fiber against colorectal cancer? A case-control study in Central Europe. Nutr J 12:134
Ashmore JH, Lesko SM, Miller PE, Cross AJ, Muscat JE, Zhu J, Liao J, Harper G, Lazarus P, Hartman TJ (2013) Association of dietary and supplemental iron and colorectal cancer in a population-based study. Eur J Cancer Prev 22:506–511
Key TJ, Appleby PN, Masset G, Brunner EJ, Cade JE, Greenwood DC et al (2012) Vitamins, minerals, essential fatty acids and colorectal cancer risk in the United Kingdom Dietary Cohort Consortium. Int J Cancer 131:320–325
Sun Z, Zhu Y, Wang PP, Roebothan B, Zhao J, Zhao J, Dicks E, Cotterchio M, Buehler S, Campbell PT, McLaughlin J, Parfrey PS (2012) Reported intake of selected micronutrients and risk of colorectal cancer: results from a large population-based case-control study in Newfoundland, Labrador and Ontario, Canada. Anticancer Res 32:687–696
Jin X, Gao C, Jianhua D, Suping L, Yanting L, Haixia C et al (2011) The risk of dietary micronutrient intake and colorectal cancer. national cancer epidemiology and tumor etiology academic conference. China Cancer 10:731–734
van Lee L, Heyworth J, McNaughton S, Iacopetta B, Clayforth C, Fritschi L (2011) Selected dietary micronutrients and the risk of right- and left-sided colorectal cancers: a case-control study in Western Australia. Ann Epidemiol 21:170–177
Jenab M, Bueno-de-Mesquita HB, Ferrari P, van Duijnhoven FJ, Norat T, Pischon T et al (2010) Association between pre-diagnostic circulating vitamin D concentration and risk of colorectal cancer in European populations: a nested case-control study. BMJ 340:b5500
Cross AJ, Gunter MJ, Wood RJ, Pietinen P, Taylor PR, Virtamo J, Albanes D, Sinha R (2006) Iron and colorectal cancer risk in the alpha-tocopherol, beta-carotene cancer prevention study. Int J Cancer 118:3147–3152
Kesse E, Boutron-Ruault MC, Norat T, Riboli E, Clavel-Chapelon F (2005) Dietary calcium, phosphorus, vitamin D, dairy products and the risk of colorectal adenoma and cancer among French women of the E3N-EPIC prospective study. Int J Cancer 117:137–144
Levi F, Pasche C, Lucchini F, La Vecchia C (2000) Selected micronutrients and colorectal cancer. A case-control study from the canton of Vaud, Switzerland. Eur J Cancer 36:2115–2119
Kato I, Dnistrian AM, Schwartz M, Toniolo P, Koenig K, Shore RE, Zeleniuch-Jacquotte A, Akhmedkhanov A, Riboli E (1999) Iron intake, body iron stores and colorectal cancer risk in women: a nested case-control study. Int J Cancer 80:693–698
De Stefani E, Mendilaharsu M, Deneo-Pellegrini H, Ronco A (1997) Influence of dietary levels of fat, cholesterol, and calcium on colorectal cancer. Nutr Cancer 29:83–89
Boutron MC, Faivre J, Marteau P, Couillault C, Senesse P, Quipourt V (1996) Calcium, phosphorus, vitamin D, dairy products and colorectal carcinogenesis: a French case-control study. Br J Cancer 74:145–151
Pérez RC, Aranceta J, Salvador G, Varela-Moreiras G (2015) Food frequency questionnaires. Nutr Hosp 31:49–56
Carpenter CE, Mahoney AW (1992) Contributions of heme and nonheme iron to human nutrition. Crit Rev Food Sci Nutr 31:333–367
Czerwonka M, Tokarz A (2017) Iron in red meat-friend or foe. Meat Sci 123:157–165
Bo S, Milanesio N, Schiavone C, Villois P, Durazzo M, Gentile L, Cassader M, Cavallo-Perin P (2011) Magnesium and trace element intake after a lifestyle intervention. Nutrition 27:108–110
Ko HJ, Youn CH, Kim HM, Cho YJ, Lee GH, Lee WK (2014) Dietary magnesium intake and risk of cancer: a meta-analysis of epidemiologic studies. Nutr Cancer 66:915–923
Wark PA, Lau R, Norat T, Kampman E (2012) Magnesium intake and colorectal tumor risk: a case-control study and meta-analysis. Am J Clin Nutr 96:622–631
Chen GC, Pang Z, Liu QF (2012) Magnesium intake and risk of colorectal cancer: a meta-analysis of prospective studies. Eur J Clin Nutr 66:1182–1186
Food and Nutrition Board, Institute of Medicine (1997) Dietary reference intakes for calcium, phosphorus, magnesium, vitamin D, and fluoride. National Academies Press, Washington, DC
Food and Nutrition Board, Institute of Medicine (2001) Dietary reference intakes for vitamin a, vitamin K, arsenic, boron, chromium, copper, iodine, Iron, manganese, molybdenum, nickel, silicon, vanadium, and zinc. National Academies Press, Washington, DC
Food and Nutrition Board, Institute of Medicine Sodium and chloride (2005) Dietary reference intakes for water, potassium, sodium, chloride, and sulfate. National Academies Press, Washington, DC
Funding
This study was supported by the Fundamental Research Funds for the Central Universities (No. 2042017kf0031), Natural Science Foundation of Hubei Province (No. 2018CFB131), and the National Natural Science Foundation of China (No. 81773471).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Rights and permissions
About this article

Cite this article
Meng, Y., Sun, J., Yu, J. et al. Dietary Intakes of Calcium, Iron, Magnesium, and Potassium Elements and the Risk of Colorectal Cancer: a Meta-Analysis. Biol Trace Elem Res 189, 325–335 (2019). https://doi.org/10.1007/s12011-018-1474-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12011-018-1474-z