
Abstract
The definitive treatment for symptomatic large volume (>80 mL) benign prostatic hyperplasia (BPH) is simple prostatectomy (SP). This can be performed by utilizing a retropubic, suprapubic, or a combined approach. The latter two approaches allow for the management of concomitant bladder diverticulum or stones through the same incision. Each approach affords unique technical strengths and weaknesses that must be considered in light of patient characteristics and concomitant pathology. SP allows for removal of the entire prostatic adenoma while obviating some of the neurovascular and continence issues that can arise from radical prostatectomy. Concerns with SP include its relatively high perioperative morbidity, notably bleeding. Therefore, there is increasing interest in less invasive options, including enucleation procedures and minimally invasive SP. This review presents an update regarding trends and outcomes of SP, as well as the effectiveness and popularity of alternative treatments.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Benign prostatic hyperplasia (BPH) affects a large proportion of aging men. Transurethral resection of prostate and, more recently, endoscopic laser techniques have generally been utilized for patients who are refractory to or intolerant of medical therapies. In patients with very large prostates, open SP was the conventional approach for complete enucleation of the adenoma. Despite its clear effectiveness, there is considerable perioperative morbidity [1••]. Other procedures including laser enucleation and minimally invasive simple prostatectomy have recently gained popularity. These procedures aim to provide an alternative that maintains effectiveness but decreases the perioperative morbidity of SP [2]. In this article, the epidemiology of SP will be discussed along with a brief review of techniques, outcomes, and alternative approaches for men with symptomatic BPH and a large prostate (>80 g).
Epidemiology and Trends
BPH is a histologic diagnosis that refers to proliferation of smooth muscle and epithelial cells in the transition zone of the prostate [3, 4]. As the prostate grows, it causes obstruction from both increased tissue mass and smooth muscle tone, narrowing the lumen of the prostatic urethra [5]. It is a common condition in the aging male. Previous studies have suggested that clinically symptomatic BPH affects one-third of men in their sixties and about half of men over 80 years old [6]. As the population ages, greater numbers of men will be expected to develop lower urinary tract symptoms secondary to BPH. A large epidemiological study assessing 1071 participants showed that BPH and prostate volume correlates with increasing age [7]. Given the prevalence of BPH, many medical treatments have emerged and have been incorporated into guidelines that can be applied by primary care physicians and specialists alike [8].
Despite continued advances in medical therapies over the last few decades, a significant number of men are refractory to medical treatments or intolerant of side effects. The landmark CombAT trial was one of the largest studies assessing the effects of maximal medical therapy. It demonstrated improved efficacy from combining alpha blockers and 5 alpha reductase inhibitors over monotherapy with either agent for patients with prostates >30 g [9]. However, subsequent analysis reported significant clinical progression and symptom deterioration seen in all three treatment arms over time [10]. Many men with significantly larger prostates may not even experience comparable initial improvements in outcomes. Progression of BPH and need for further therapies are another concerns about medical therapies. The MTOPS study assessed 3047 men and the effect of combination therapy with doxazosin and finasteride [11]. In total, 2–3 % of men experience acute urinary retention, urinary tract infections, or require eventual surgical therapy. Side effects of medical management have also been well documented. The MTOPS study also demonstrated that up to 27 % of men had stopped doxazosin and 24 % of men had stopped finasteride by the end of the study. The most frequent side effects were erectile dysfunction, dizziness, and postural hypotension. Some men are unwilling to consider the option of lifelong medical therapy, especially in light of this side effect profile. For this reason, many patients seek surgical treatment for BPH as primary therapy, while others proceed to surgery after medication failure or intolerance.
American Urological Association (AUA) and European Association of Urology (EAU) guidelines both strongly recommend surgical treatment for BPH in select conditions, including refractory urinary retention, renal insufficiency, bladder stones, recurrent urinary tract infections, and refractory hematuria [12, 13]. AUA guidelines specifically state that “open prostatectomy is an appropriate and effective treatment alternative for men with moderate to severe LUTS (lower urinary tract symptoms) and/or who are significantly bothered by symptoms.” Other factors must be taken into account, including anatomy, surgeon experience, and a review of the benefits versus the risk of complications. Many also consider a large obstructing median lobe and large prostate volumes using a cutoff >80 or >100 g to be stronger indications for surgical treatments. AUA guidelines do not specifically recommend routine transrectal ultrasound measurement of prostate volume, although some experts utilize this to guide management decisions or surgical planning.
While the armamentarium of medications for treatment of BPH and associated LUTS has not changed dramatically in recent years, the breadth of surgical techniques available for the treatment of very large prostates has grown. Meanwhile, the popularity of SP has declined, despite open SP being considered a standard treatment for men with large prostates. When assessing rates of open SP to manage BPH worldwide, careful consideration must be given to differing practice patterns in varying countries. Studies assessing the management for BPH in the USA in the 1990s found that both open and endoscopic surgical management decreased by half from 1990 to 1995 [14, 15]. They surmised that this was due to the emergence of medical therapy at this time. By 1985, with the advent of transurethral resection of prostate, only 5 % of BPH cases were managed by open SP in the USA, and by the late 1990s, open SP accounted for less than 3 % of surgeries for BPH [16, 17].
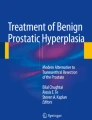
More recently, in a study using the National Inpatient Sample, the use of SP in the USA decreased from 2002 to 2012 by roughly 145 cases/year (Fig. 1) [1••]. A separate study reported that the overall frequency of simple prostatectomies in the USA decreased from 3157 cases in 1998 to 2227 cases in 2010 [18]. Interestingly, over a similar time period in New York State, transurethral resection of the prostate (TURP) also decreased, while remaining the most common surgery for BPH [19]. Lowrance et al. also examined trends in the use of endoscopic surgical management, including TURP and laser vaporization or enucleation. Reviewing case logs of urologists applying for certification or recertification from the American Board of Urology, they found that TURPs comprised 89 % of BPH endoscopic procedures in 2004. However, this percentage fell to 56 % by 2010, which corresponded with an increase in endoscopic laser procedures [20••]. Coinciding with decreases in open SP and TURP, there has been a surge in both minimally invasive SP and endoscopic laser technologies, as these techniques have become more widespread and popular [1••, 19].

Simple prostatectomy cases (open and MIS) performed in the USA over time. Trend line (β = −145 cases/year, 95 % CI [−220 to −69], R 2 = 0.68, p = .002). Percentages above the bars represent the rate of MIS used each year ([1••] with permission)
Outcomes
Simple prostatectomy may be more effective than conventional TURP in relieving bladder outlet obstruction in men with very large prostates [12]. It is also often preferred in the setting of concomitant bladder stone or diverticulum given the ability to extract stones or perform a diverticulectomy through the same incision.
Large multi-center series have reported their outcomes of open SP. In a European series of 1804 open prostatectomies, early complications were relatively common, with severe bleeding occurring in 11.6 % of procedures and sepsis in 8.6 % of patients [21]. Repeat interventions were required in 3.6 % of cases. A separate prospective multi-center study by Gratzke et al. reported on 902 patients who underwent open SP [22]. The overall complication rate was 17.3 %, with bleeding in 7.5 % and urinary tract infections in 5.1 % of patients. Functional outcomes were also assessed. Urinary peak flow rates increased significantly from 10.6 ± 6.4 mL/s to 23.1 ± 10.5 mL/s (p < 0.0001) with similar improvements of post-void residual volumes. Other large studies have shown that increased bleeding is associated with larger prostate size and that overall reoperation rates are low [16, 23].
Smaller series have allowed for a more granular assessment of specific outcomes. An Italian series of 50 patients examined sexual activity after open SP, finding that there were improvements in sexual function measured by mean International Index of Erectile Function (IIEF-5) scores [24]. They found a greater improvement in erectile function in younger patients. A prospective randomized trial of open SP versus plasmakinetic enucleation of the prostate assessed 6-year outcomes of 77 patients who underwent open SP [25•]. This study showed that mean IIEF-5 scores did not change over time. Furthermore, improvements in Qmax at 1 year were durable up to 6 years (mean Qmax 24.0 ± 6.2 versus 26.8 ± 7.9, respectively). They noted a 42.5 % rate of short-term complications, most commonly transient incontinence (13.75 %) and urinary tract infection (11.25 %), while the rate of medium to long-term complications including urethral stricture (1.25 %) and bladder neck contracture (5 %) were much lower. Kuntz et al. found similar results in a prospective randomized trial comparing open SP versus holmium laser enucleation of the prostate [26]. With 5-year follow-up, they demonstrated that 6.6 % of patients developed bladder neck contracture while 1.7 % developed urethral stricture. Finally, a Greek series assessing 232 patients with 5-year follow-up also showed a 3.3 % bladder neck contracture rate at a mean of 10 months, as well as a 0.6 % urethral stricture rate, and 3.9 % reoperation rate [17].
Studies utilizing national administrative databases, such as the National Inpatient Sample (NIS), have also reported perioperative complication rates after SP. Bleeding complications were estimated to occur between 21–24 % [1••, 18]. Pariser et al. reported that bladder diverticulectomy was performed in 5 % of patients and cystolithotomy in 17 % in patients undergoing SP in the USA. On multivariable analysis, patients were at increased risk of complications if they were African American, older, or had more baseline comorbidities. Interestingly, performance of cystolithotomy was independently associated with decreased risk of complications (Table 1). Removal of stones would seem to confer some protective benefit during SP. However, this may have reflected the study’s inability to control for prostate size; patients with smaller prostates and bladder stones may be preferentially offered SP. A previous study reported that high-grade perioperative complications after SP were more common for patients with a larger amount of resected tissue [27].
Emerging Alternatives to Conventional Open Simple Prostatectomy
In addition to conventional open SP or transurethral resection of the prostate, an array of additional techniques and modalities has been deployed in the effort to remove bladder outlet obstruction and allow for improved voiding. Autorino et al. reported a comprehensive summary of outcomes from studies including a variety of surgical techniques to treat bladder outlet obstruction in the setting of large prostates (Table 2) [28••]. We will review select emerging procedures below.
Enucleation Techniques
Holmium laser enucleation of prostate (HoLEP) or thulium laser enucleation of the prostate (ThuLEP) are efficacious options for very large glands, unlike TURP, laser ablation of prostate, and laser vaporization of the prostate. One might conceptualize enucleation techniques as the endoscopic equivalent of SP [31]. A randomized, prospective clinical trial comparing outcomes of HoLEP to SP demonstrated no significant differences in functional outcomes [26]. Specifically, AUA symptom score (3.0 for both, p = 0.98), Qmax (24.4 mL/s for both, p = 0.97), post-void residual measurements (11 mL for HoLEP versus 5 mL for SP), and rates of reoperation (5 % for HoLEP versus 6.7 % for SP) were similar at five-year follow-up. However, HoLEP was superior to SP in terms of perioperative morbidity (15 versus 26.7 %), mean hemoglobin loss (1.9 versus 2.8 g/dL), catheterization time (30 versus 194 h), and length of hospital stay (70 versus 250 h), p < 0.0001. Due to improved convalescence, HoLEP is associated with significant cost savings compared to SP; one study showed mean perioperative costs for HoLEP were approximately 33 % less than those for SP [32].
The thulium laser has also been examined for enucleation procedures. Gross et al. reported on 1080 patients who underwent ThuLEP. Significant improvements were seen in voiding parameters. Given the learning curve of this procedure, there was a significant decrease over time in the complication rate when cases were divided into chronological quintiles [33•].
Despite the equivalent efficacy, safety, and lower cost of HoLEP, this technique has been slow to overtake SP as the preferred treatment for very large glands (>80–100 g). Much of this has been attributed to a significant learning curve associated with HoLEP, with studies suggesting a requisite 20–50 cases to gain acceptable efficiency [34, 35].
Minimally Invasive Simple Prostatectomy
Minimally invasive approaches to SP have grown in popularity, with goals of achieving the effectiveness of SP while minimizing the known perioperative morbidity from the open approach. Mariano et al. described the first laparoscopic simple prostatectomy in 2002 [36]. Over time, robotic approaches for other urologic procedures have become ubiquitous. Increased dexterity and degrees of freedom of the Da Vinci (Intuitive Surgical Inc, Sunnyvale, CA) platform are some of the reasons robotic technology has gained popularity. Thus, some surgeons favor robotics over laparoscopy for SP. Several SP series have demonstrated the safety and efficacy of these minimally invasive approaches. The largest outcome analysis of the minimally invasive approach to simple prostatectomy is a multi-center series by Autorino et al. which examined 1330 minimally invasive simple prostatectomies between 2000 and 2014. Of these, 487 (36.6 %) were robotic and 843 (63.4 %) were pure laparoscopic [28••]. Median specimen weight was comparable between the two groups, 76 g in laparoscopic versus 75 g in robotic groups. Median operative time was 95 min for laparoscopic versus 154.5 min for the robotic approach, and median estimated blood loss was 280 mL for laparoscopic versus 200 mL for the robotic approach. In this series, they observed significant (p < 0.001) improvement in functional outcomes at 12-month follow-up. Postoperative Qmax and IPSS were 22 mL/s and 5 in the laparoscopic group versus 25 mL/s and 7 in the robotic group, respectively. Intraoperative complication rate was 2.2 %, and postoperative complication rate was 10.6 %, although most were low grade (Clavien 1–2). Moreover, their trifecta outcome (combination of IPSS <8, Qmax >15 mL/s, and no perioperative complications) did not significantly differ between the two approaches.
In a retrospective analysis, Pavan et al. compared outcomes of laparoscopic simple prostatectomy versus robotic-assisted simple prostatectomy at three teaching hospitals [37•]. They examined 319 patients undergoing SP, of which 189 were laparoscopic and 130 were robotic. The majority of the laparoscopic procedures occurred earlier in the series. After the introduction of the robotic approach at these institutions, robotic SP outnumbered pure laparoscopic SP by a factor greater than 4 to 1. This seems to mirror a trend in the field of urology overall, as robotic surgical systems become increasingly available and surgeon comfort and experience with robotic technology grows. In this series, the authors demonstrated a significant decrease in IPSS by 90 % in laparoscopic group and 64 % in the robotic group (p < 0.001). They also show improvements in Qmax by 100 % in laparoscopic and 142 % in robotic group (p = 0.03). Although the laparoscopic approach showed statistically significant greater functional improvement, the absolute difference in Qmax between laparoscopic and robotic groups was 2 mL/s, which is unlikely to be clinically significant. Similarly, while there were differences in IPSS between the two groups, the absolute values for median postoperative IPSS were in the mild range. There were no significant differences in median operative time (120 versus 150 min), estimated blood loss (250 versus 300 mL), and length of stay (5 versus 5 days) between laparoscopic and robotic approaches. The robotic approach was associated with a higher overall postoperative complication rate (17.7 versus 5.3 %), although the rate of major complications did not differ significantly (2.3 versus 2.1 %).
It is well known that early adopters of a new surgical approach meet skepticism from those who continue to use the conventional approach. Namely, does the newer technique allow clinically meaningful improvements in patient outcomes? Are there potentially increased costs and learning curves? The minimally invasive approach to simple prostatectomy is no exception. Several studies over the last decade aimed to address these questions, although there are no randomized studies to our knowledge. A study by Baumert et al. aimed to compare outcomes of patients who underwent laparoscopic SP compared to open SP by a single surgeon experienced in both techniques [38]. Data was gathered retrospectively for the open SP patients and prospectively for 30 consecutive laparoscopic SP patients. Operative time was longer in the laparoscopic group (115 ± 30 versus 54 ± 19 min), although it should be noted that these laparoscopic SPs were among the first performed by this surgeon. As such, operative times may have been affected by the learning curve. The laparoscopic group had less blood loss, shorter duration of catheterization, and decreased hospital stay. McCullough et al. presented a single institution series of 280 consecutive simple laparoscopic or open prostatectomies between 2003 and 2008 in patients who had previously failed medical therapy. Similar to the Baumert study, operative time in the laparoscopic group was approximately double that of the open group (95.1 ± 32.9 versus 54.7 ± 19.7 min, p < 0.0001). Estimated blood loss was not significantly different between the two groups. Catheterization time (5.2 ± 2.6 versus 6.4 ± 2.9 days, p = 0.001) and length of hospital stay (6.3 ± 1.9 versus 7.7 ± 2.4, p < 0.0001) were shorter in the laparoscopic group. There was no significant difference in incidence of hemorrhage between the two groups (28 % in laparoscopic and 29 % in open) [39]. Additional studies are needed to compare long-term urinary functional outcomes of minimally invasive compare to versus open approaches.
Conclusions
Simple prostatectomy is an effective treatment for relieving bladder outlet obstruction in the setting of a very large prostate or concomitant operative bladder pathology, such as stone or diverticulum. However, it is associated with considerable perioperative morbidity including bleeding complications. The overall utilization of SP has recently decreased given the advent of alternative surgical techniques. For patients with very large prostates, effective alternatives to the conventional open approach include minimally invasive (robotic or laparoscopic) approaches to SP or laser enucleation techniques, which have both been shown to be effective and yield decreased morbidity. However, there is a considerable learning curve associated with these modalities which precludes their rapid widespread adoption. Despite this, we expect that the surgical management of BPH will continue to evolve, as the development of new procedures and refinement of existing techniques yield better functional outcomes and decreased morbidity.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Pariser JJ, Pearce SM, Patel SG, Bales GT. National Trends of Simple Prostatectomy for Benign Prostatic Hyperplasia With an Analysis of Risk Factors for Adverse Perioperative Outcomes. Urology. 2015;86:721–5. This manuscript represents the largest national database study regarding trends in the use of SP with a multivariate analysis of risk factors for complications.
Jones P, Alzweri L, Rai BP, Somani BK, Bates C, Aboumarzouk OM. Holmium laser enucleation versus simple prostatectomy for treating large prostates: results of a systematic review and meta-analysis. Arab J Urol. 2016;14:50–8.
Lee C, Kozlowski JM, Grayhack JT. Etiology of benign prostatic hyperplasia. Urol Clin N Am. 1995;22:237–46.
Lee C, Kozlowski JM, Grayhack JT. Intrinsic and extrinsic factors controlling benign prostatic growth. Prostate. 1997;31:131–8.
Auffenberg GB, Helfand BT, McVary KT. Established medical therapy for benign prostatic hyperplasia. Urol Clin N Am. 2009;36:443–59.
McVary KT. BPH: epidemiology and comorbidities. Am J Manag Care. 2006;12:S122–8.
Wright EJ, Fang J, Metter EJ, Partin AW, Landis P, Chan DW, et al. Prostate specific antigen predicts the long-term risk of prostate enlargement: results from the Baltimore Longitudinal Study of Aging. J Urol. 2002;167:2484–7.
Blankstein U, Van Asseldonk B, Elterman DS. BPH update: medical versus interventional management. Can J Urol. 2016;23:10–5.
Roehrborn CG, Siami P, Barkin J, Damião R, Major-Walker K, Nandy I, et al. The effects of combination therapy with dutasteride and tamsulosin on clinical outcomes in men with symptomatic benign prostatic hyperplasia: 4-year results from the CombAT study. Eur Urol. 2010;57:123–31.
Roehrborn CG, Barkin J, Siami P, Tubaro A, Wilson TH, Morrill BB, et al. Clinical outcomes after combined therapy with dutasteride plus tamsulosin or either monotherapy in men with benign prostatic hyperplasia (BPH) by baseline characteristics: 4-year results from the randomized, double-blind Combination of Avodart and Tamsulosin (CombAT) trial. BJU Int. 2011;107:946–54.
McConnell JD, Roehrborn CG, Bautista OM, Andriole GL, Dixon CM, Kusek JW, et al. The long-term effect of doxazosin, finasteride, and combination therapy on the clinical progression of benign prostatic hyperplasia. N Engl J Med. 2003;349:2387–98.
McVary KT, Roehrborn CG, Avins AL, Barry MJ, Bruskewitz RC, Donnell RF, et al. Update on AUA guideline on the management of benign prostatic hyperplasia. J Urol. 2011;185:1793–803.
Madersbacher S, Alivizatos G, Nordling J, Sanz CR, Emberton M, de la Rosette JJMCH. EAU 2004 guidelines on assessment, therapy and follow-up of men with lower urinary tract symptoms suggestive of benign prostatic obstruction (BPH guidelines). Eur Urol. 2004;46:547–54.
Gee WF, Holtgrewe HL, Albertsen PC, Litwin MS, Manyak MJ, O’Leary MP, et al. Practice trends in the diagnosis and management of benign prostatic hyperplasia in the United States. J Urol. 1995;154:205–6.
Bruskewitz R. Management of symptomatic BPH in the US: who is treated and how? Eur Urol. 1999;36 Suppl 3:7–13.
Roos NP, Wennberg JE, Malenka DJ, Fisher ES, McPherson K, Andersen TF, et al. Mortality and reoperation after open and transurethral resection of the prostate for benign prostatic hyperplasia. N Engl J Med. 1989;320:1120–4.
Varkarakis I, Kyriakakis Z, Delis A, Protogerou V, Deliveliotis C. Long-term results of open transvesical prostatectomy from a contemporary series of patients. Urology. 2004;64:306–10.
Parsons JK, Rangarajan SS, Palazzi K, Chang D. A national, comparative analysis of perioperative outcomes of open and minimally invasive simple prostatectomy. J Endourol. 2015;29:919–24.
Chughtai BI, Simma-Chiang V, Lee R, Isaacs A, Te AE, Kaplan SA, et al. Trends and utilization of laser prostatectomy in ambulatory surgical procedures for the treatment of benign prostatic hyperplasia in New York State (2000–2011). J Endourol. 2015;29:700–6.
Lowrance WT, Southwick A, Maschino AC, Sandhu JS. Contemporary practice patterns of endoscopic surgical management for benign prostatic hyperplasia among urologists in the United States. J Urol. 2013;189:1811–6. This study reports on the urologist-level practice patterns in the treatment of BPH. Notably, endoscopic laser procedures are gaining in popularity, especially with younger physicians.
Serretta V, Morgia G, Fondacaro L, Curto G. Lo bianco A, Pirritano D, et al. Open prostatectomy for benign prostatic enlargement in southern Europe in the late 1990s: a contemporary series of 1800 interventions. Urology. 2002;60:623–7.
Gratzke C, Schlenker B, Seitz M, Karl A, Hermanek P, Lack N, et al. Complications and early postoperative outcome after open prostatectomy in patients with benign prostatic enlargement: results of a prospective multicenter study. J Urol. 2007;177:1419–22.
Abrams PH, Shah PJ, Bryning K, Gaches CG, Ashken MH, Green NA. Blood loss during transurethral resection of the prostate. Anaesthesia. 1982;37:71–3.
Montesi L, Quaresima L, Tiroli M, Lacetera V, Cantoro U, Sbrollini G, et al. Improvement of lower urinary tract symptoms and sexual activity after open simple prostatectomy: prospective analysis of 50 cases. Arch Ital Urol Androl. 2014;86:353–5.
Chen S, Zhu L, Cai J, Zheng Z, Ge R, Wu M, et al. Plasmakinetic enucleation of the prostate compared with open prostatectomy for prostates larger than 100 grams: a randomized noninferiority controlled trial with long-term results at 6 years. Eur Urol. 2014;66:284–91. This was a randomized trial of plasmakinetic enucleation and open prostatectomy. The enucleation procedure demonstrated similar long-term voiding outcomes with improved perioperative morbidity.
Kuntz RM, Lehrich K, Ahyai SA. Holmium laser enucleation of the prostate versus open prostatectomy for prostates greater than 100 grams: 5-year follow-up results of a randomised clinical trial. Eur Urol. 2008;53:160–6.
Elshal AM, El-Nahas AR, Barakat TS, Elsaadany MM, El-Hefnawy AS. Transvesical open prostatectomy for benign prostatic hyperplasia in the era of minimally invasive surgery: perioperative outcomes of a contemporary series. Arab J Urol. 2013;11:362–8.
Autorino R, Zargar H, Mariano MB, Sanchez-Salas R, Sotelo RJ, Chlosta PL, et al. Perioperative Outcomes of robotic and laparoscopic simple prostatectomy: a European-American multi-institutional analysis. Eur Urol. 2015;68:86–94. This is a very large multi-institutional study regarding the perioperative outcomes of minimally invasive simple prostatectomy. They demonstrate good outcomes of the procedure across multiple centers.
Humphreys M, Miller N, Handa S, Terry C, Munch L, Lingeman J. Holmium laser enucleation of the prostate—outcomes independent of prostate size? J Urol. 2008;180:2431–5.
Geavlete B, Stanescu F, Iacoboaie C, Geavlete P. Bipolar plasma enucleation of the prostate vs open prostatectomy in large benign prostatic hyperplasia cases—a medium term, prospective, randomized comparison. BJU Int. 2013;111:793–803.
Sivarajan G, Borofsky MS, Shah O, Lingeman JE, Lepor H. The Role of Minimally Invasive Surgical Techniques in the Management of Large-gland Benign Prostatic Hypertrophy. Rev Urol. 2015;17:140–9.
Salonia A, Suardi N, Naspro R, Mazzoccoli B, Zanni G, Gallina A, et al. Holmium laser enucleation versus open prostatectomy for benign prostatic hyperplasia: an inpatient cost analysis. Urology. 2006;68:302–6.
Gross AJ, Netsch C, Knipper S, Hölzel J, Bach T. Complications and early postoperative outcome in 1080 patients after thulium vapoenucleation of the prostate: results at a single institution. Eur Urol. 2013;63:859–67. This is a very large study (n = 1080) regarding thulium laser vapoenucleation of the prostate and perioperative outcomes with improvements in complication rates seen throughout their experience.
El-Hakim A, Elhilali MM. Holmium laser enucleation of the prostate can be taught: the first learning experience. BJU Int. 2002;90:863–9.
Shah HN, Mahajan AP, Sodha HS, Hegde S, Mohile PD, Bansal MB. Prospective evaluation of the learning curve for holmium laser enucleation of the prostate. J Urol. 2007;177:1468–74.
Mariano MB, Graziottin TM, Tefilli MV. Laparoscopic prostatectomy with vascular control for benign prostatic hyperplasia. J Urol. 2002;167:2528–9.
Pavan N, Zargar H, Sanchez-Salas R, Castillo O, Celia A, Gallo G, et al. Robot-assisted versus standard laparoscopy for simple prostatectomy: multicenter comparative outcomes. Urology. 2016 (in press). This is a comparative analysis of robotic and laparoscopic simple prostatectomy across multiple centers. Both procedures were safe approaches to treat BPH in very large glands.
Baumert H, Ballaro A, Dugardin F, Kaisary AV. Laparoscopic versus open simple prostatectomy: a comparative study. J Urol. 2006;175:1691–4.
McCullough TC, Heldwein FL, Soon SJ, Galiano M, Barret E, Cathelineau X, et al. Laparoscopic versus open simple prostatectomy: an evaluation of morbidity. J Endourol. 2009;23:129–33.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Joseph J. Pariser, Vignesh T. Packiam, Melanie A. Adamsky, and Gregory T. Bales each declare no potential conflicts of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Benign Prostatic Hyperplasia
Rights and permissions
About this article

Cite this article
Pariser, J.J., Packiam, V.T., Adamsky, M.A. et al. Trends in Simple Prostatectomy for Benign Prostatic Hyperplasia. Curr Urol Rep 17, 57 (2016). https://doi.org/10.1007/s11934-016-0610-6
Published:
DOI: https://doi.org/10.1007/s11934-016-0610-6