
Abstract
While the primary manifestation of rheumatoid arthritis (RA) is articular disease, extra-articular disease may also occur. In particular, pulmonary disease is a frequent extra-articular manifestation of seropositive RA and a leading cause of morbidity and mortality in this population. This review will highlight studies published in the last several years and will, in particular, discuss the relationship of antibodies to citrullinated protein/peptide antigens (ACPA) and lung disease in patients with RA. We will also review the data regarding the potential role of the lung and generation of RA-related autoantibodies in a period of disease development termed “preclinical RA.” Finally, we will discuss the role of ACPA and other Abs in non-RA pulmonary diseases and discuss a research agenda for next steps in the understanding and management of the lung in RA.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Rheumatoid arthritis (RA) is a systemic autoimmune disease that affects approximately 0.5 to 1 % of the population globally. The disease is characterized in the majority of patients by elevations of circulating RA-related autoantibodies namely rheumatoid factor (RF) and antibodies to citrullinated protein/peptide antigens (ACPA) that can be characterized by the commercially available antibodies to cyclic citrullinated antigen (anti-CCP) assays [1]. If one or both of these autoantibodies are present, a patient is deemed to have “seropositive” RA, although a subset of patients (∼20 %) do not have detectable RF or ACPA [2, 3].
While the primary manifestation of RA is articular disease, extra-articular disease may also occur. In particular, pulmonary disease is a frequent extra-articular manifestation of seropositive RA and a leading cause of morbidity and mortality in this population [4, 5]. This review will highlight studies published in the last several years and will, in particular, discuss the relationship of ACPA and lung disease in patients with RA that is classifiable by existing criteria such as the 1987 and 2010 criteria [6, 7] or determined to be RA by treating clinicians. This disease status will be referred to herein as “established RA.” We will also review the data regarding the potential role of the lung and generation of RA-related autoantibodies in a period of disease development termed “preclinical RA”; while the specific nomenclature for this phase of RA is in development [8], we define it herein as the presence of circulating RA-related autoantibodies in absence of clinically apparent synovitis. Finally, we will discuss the role of ACPA and other Abs in non-RA pulmonary diseases. Of note, we will discuss the roles of both RF and ACPA; however, because less controversy surrounds the role of RF in RA-related lung disease, an association first described in the 1970s, we will primarily focus on ACPA [9].
Lung Involvement in Established RA
Among patients with established RA, the prevalence of lung involvement varies by type of lung disease, diagnostic method used to ascertain lung disease, and individual factors, including smoking history and RA disease duration [9]. Some studies suggest that up to 80 % of subjects with RA may have some form of lung disease; however, in the majority of those subjects, the disease may not be clinically identified [10].
RA-related pulmonary complications are diverse (Table 1) and can involve the airways in disease processes such as cricoarytenoid disease and bronchiolitis. In addition, there is parenchymal disease that can be collectively termed “interstitial lung disease” (ILD) and manifested by alveolar processes such as organizing pneumonia (OP), non-specific interstitial pneumonitis (NSIP), and usual interstitial pneumonia (UIP), all of which can have varying degrees of fibrosis. Furthermore, lung nodules may be present, as well as pleural-pericardial disease and pulmonary vascular disease including venous thromboembolism [5, 9, 11].
Of these diseases, perhaps, the most feared in RA are those classified as ILD and, in particular, the UIP form of ILD that is associated with significant fibrosis and poor prognosis with current therapies [12, 13]. Interestingly, however, a recent publication by Sparks and colleagues noted in a study based on database review that obstructive lung disease was a leading cause of death in RA [14•]. Since this was a study based on diagnostic codes, the specific underlying lung pathology was not known; however, this finding along with findings from older work raises the issue that non-ILD-related obstructive lung disease in RA may also be an important comorbidity [14•, 15•, 16].
Of note, there is some controversy as to what the term “ILD” encompasses in RA-related lung disease; however, for this review, we will use that term to refer to parenchymal disease including OP, NSIP, and UIP; when possible, diseases such as airway disease and pleural disease will be discussed separately.
Risk Factors for Lung Disease in Established RA: Focus on ACPA
Numerous risk factors for lung disease in RA have been identified including smoking, exposure to environmental factors such as occupational dust, male gender, duration of RA, disease activity in RA, seropositivity for RF, infections, and medication toxicity (e.g., methotrexate) [17–20•]. However, over the past several years, several studies have found particular associations between circulating ACPA and increased RA disease activity and joint erosions, as well as extra-articular involvement and, in particular, various forms of lung disease [3, 17, 21–23•].
ACPA and Airways Disease in RA
Airways disease (AD) in RA patients has also been linked to RA-related autoantibodies [22•, 24, 25]. A study by Mori and colleagues evaluated high-resolution computed tomography (CT) scans of 356 Japanese RA patients with AD, ILD, or no lung condition. These authors found a strong association of high elevations RF titers (RF ≥100 IU/ml, RR 3.0, p = 0.02) and anti-CCP2 (anti-CCP2 ≥90 U/ml, RR 3.8, p = 0.005) with AD, which included patterns of bronchiectasis (BR), bronchiolitis or both. However, while the anti-CCP2 level seemed to discriminate type of lung involvement, the rate of anti-CCP2 positivity was high in the overall cohort and did not differ significantly among the three groups (88.4 % no lung disease vs. 90 % in AD vs. 100 % in ILD) [22•].
Another study examined a unique cohort of arthritis patients with coexisting BR, a well-recognized association with RA [25, 26]. They described higher rates of seropositivity for anti-CCP2 (89 vs. 46 %) and RF (79 vs. 52 %) as well as increased very high values for RF (defined by >130 U/ml) and anti-CCP2 (defined by >340 U/ml) in RA-BR subjects compared to RA patients without BR. As previously described [27], smoking prevalence was low in their RA-BR subjects, which supports a potentially different trigger for ACPA generation in this subset of RA patients, such as infection [25]. Interestingly, an association with RA-related autoantibodies has also been described in idiopathic BR and cystic fibrosis (CF) subjects in the absence of inflammatory arthritis (IA) [28, 29]. The fact that BR symptoms precede joint disease in the majority of RA-BR patients strengthens the hypothesis of airway inflammation in RA development [30], especially among never smokers [26, 27]. This will be discussed more in the “The Lung in Preclinical RA.” section
ACPA and ILD in RA
RA-ILD, most commonly UIP and NSIP, has been linked to RA-related autoantibodies in multiple studies. ACPA may be pathogenic in the development of lung disease and influence the extent of radiographic damage and abnormalities on pulmonary function testing (PFT) [18•, 20•]. A 2014 case-control study by Kelly and colleagues found higher rates of ACPA positivity (94 vs. 55 %, p = 0.006) and median ACPA titers (median 180 vs. 78, p = 0.02) in RA-ILD subjects compared to RA controls, an association which persisted after adjusting for smoking [17].
While male gender has classically been associated with RA-ILD [19•, 31], a recent study highlighted a similar link between ACPA and ILD in an all-female RA cohort, finding that 100 % of RA-ILD subjects were ACPA positive compared to 64 % of RA controls (p < 0.01). Additionally, this study showed that anti-CCP2 titers correlated with severity of ground glass score (p = 0.02) and fibrosis (p < 0.01) after adjustment for age and DAS-28. Anti-CCP2 levels also correlated with respiratory symptoms, 6-min walk test, and forced vital capacity [18•].
In contrast, a retrospective study in 2008 analyzed 18 subjects with RA and ILD or follicular bronchiolitis and 36 RA subjects with no lung disease and found no significant difference in the frequency or level of anti-CCP2 between the two RA groups or between the ILD and bronchiolitis subgroups [23•]. This negative finding may have resulted from a small sample size or higher rates of seropositivity (88.9 %) in the RA-only group than typically reported in the literature, which may have masked any true difference in anti-CCP2 between subjects with and without lung disease. Additionally, only RA-ILD subjects with biopsy-proven lung disease were included in this study, and it is unclear what evaluation that the control group underwent to exclude subclinical lung disease, which may be present in asymptomatic RA patients [32].
There have been other studies that did not identify an association between ACPA and RA-ILD [22•, 33], leading to controversy regarding the association of ACPA and RA-ILD. In further exploration of this issue, Zhu and colleagues performed a meta-analysis to analyze the association of ACPA positivity and RA lung disease [34]. They reviewed eight case-control studies from 2008 to 2013 and included 243 RA patients with lung disease and 1442 RA controls. The authors reported a significant association between ACPA positivity and increased risk of RA lung disease (pooled OR 2.62, p < 0.01), an association that was more pronounced in Caucasians (OR 3.45) and the subgroup with RA-ILD or idiopathic pulmonary fibrosis (IPF) (OR 4.68); however, similar findings were not observed among Asians. While limited by heterogeneity and quality of studies, owing to choice of RA controls, unaccounted for confounding factors or small sample size, this meta-analysis validated a link between ACPA positivity and lung involvement in established RA.
Using ACPA to Predict RA-Related Lung Disease
Recently, research has focused on the interplay of ACPA and other clinical markers to predict lung involvement in RA [19•]. Restrepo and colleagues divided a cohort of 779 RA patients, of which 8.8 % had clinically diagnosed ILD, into development and validation groups in order to derive a clinical index that could identify RA patients at risk for RA-ILD. A stepwise logistic regression model assigned weighted points to significant variables, including male gender, rising erythrocyte sedimentation rate (ESR), presence of rales, and anti-CCP categorized by increasing strata. A score of 5 or higher (out of a maximum of 10), which provided modest sensitivity (43–75 %) and good specificity (88–89 %), would require patients to undergo additional testing [19•].
In further support of ACPA testing to identify RA-related lung disease, using a bead-based multiplex array, Giles and colleagues similarly found higher levels of specific ACPAs in patients diagnosed with RA-ILD based on CT imaging compared to RA controls. Moreover, the severity of lung disease by imaging and PFTs correlated with an expanded ACPA repertoire, defined by the authors as seven or greater high-level ACPAs [20•].
Certainly, better accuracy is needed before a risk assessment tool is widely adopted by clinicians, but the above findings support the importance of including assessment of ACPA levels in assessment for RA-ILD. Of particular interest is that in both the Restrepo and Giles studies, the association of anti-CCP titers and RA-ILD followed a dose-response pattern, which, in the Restrepo study, was less apparent for RF and ESR [19•]. Together with the observations that epitope spreading also occurs prior to the onset of joint inflammation [35], these studies support a mechanistic role of ACPA not only in the articular manifestations of RA but also in the development of lung disease [19•, 20•]. The possible direct pathogenic mechanisms behind these findings are explored in more detail in the next section.
Potential Mechanisms of Development of RA-Related Lung Disease
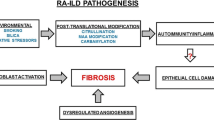
The pathophysiology of RA-related lung disease is poorly understood, but it likely mirrors the current paradigm of understanding of development of ACPA-positive articular RA that involves gene-environment interactions, protein citrullination, impaired tolerance, and eventually the development of circulating ACPA as well as other autoantibody/immune systems (e.g., RF) [36].
Following this, one study found that RA-ILD was associated with smoking only in the presence of HLA-DRB1 shared epitope (SE) [19•], an interaction that has similarly been observed for smoking, SE status, and anti-CCP for susceptibility to RA [37]. Accordingly, exposure to cigarette smoke in a SE-positive individual increases risk for RA but may also predispose to RA-ILD by means of increased local expression of factors that may drive local antigen production, such as increased citrullination mediated by increased enzymatic activity by PAD2 and PAD4 [24, 38]. Supporting this, Giles and colleagues showed a strong association with circulating anti-PAD3/4 cross-reactive Abs and RA-ILD by CT scan, particularly among smokers [39]. This newly discovered cross-reactive anti-PAD3 Ab appears to stimulate PAD4 activity by increasing its sensitivity to extra-cellular calcium and allowing unregulated citrullination of self-proteins, which in turn could disrupt the normal interaction of extracellular matrix with lymphocytes and fibroblasts in the joints or lungs [40, 41].
Increased citrullination of lung proteins, however, is not exclusive to ACPA-positive smokers and has been observed in non-smokers [42]. This implies that other inhaled factors such as silica, coal dust or air pollution, or microbial factors may interact with genes to generate ACPA or other RA-related immune factors [43, 44]. In particular, irritants are known to activate innate immune cells through pattern recognition molecules and alter the lung microbiome [43], which may activate a pro-inflammatory cascade and lead to the tissue damage observed in ILD and IPF [45, 46].
Furthermore, ectopic lymphoid tissue in subjects with RA-related lung disease supports a hypothesis of local immune dysregulation [47–49]. In particular, Rangel-Moreno and colleagues examined lung biopsies of patients with established RA as well as primary Sjögren’s syndrome (pSS), IPF, and hypersensitivity pneumonitis who had chronic lung disease and found larger and more organized lymphoid areas in the pSS and RA subjects. Interestingly, ectopic lymphoid tissue correlated with local RA-related Ab production, defined as adjacent plasma cells that stained specifically for RF or bound citrullinated proteins [49]. A 2015 study by Reynisdottir and colleagues also found significantly more lymphoid aggregates and germinal centers (GCs) in bronchial tissue from early, untreated RA subjects without lung disease compared to ACPA-negative RA subjects and healthy controls. The lung GCs also had features suggestive of local ACPA production, including plasma cells, mature B cells, and reactivity with citrullinated but not native enolase peptide [50]. Supporting this, in our own work that has been published in abstract form, we examined lung tissue from 10 subjects with RA-ILD and 65 non-RA subjects with ILD or emphysema and found a strong association of lung GCs with anti-CCP3.1 positivity (OR 4.1, 95 % CI 1.2, 14.4, p = 0.03), independent of age and RA status [51].
In aggregate, these studies suggest that lung GCs may initiate or perpetuate the immune response, leading to RA and/or RA-related lung disease in susceptible individuals. The possibility of this process occurring in the lung during preclinical RA will be discussed further.
Novel Biomarkers for RA-Related Lung Disease
While ACPA appears to be predictive of RA-ILD, pulmonary disease remains an underrecognized complication of RA, and newer pathways of evaluation including biomarkers are needed to detect lung involvement. Exploring this, Harlow and colleagues used an approach called “reverse immunophenotyping,” which employs mass spectrometric sequencing of protein immunoprecipitants; two new citrullinated targets, Hsp90α and Hsp90β, have been identified in RA-ILD [52]. When compared to sera from patients with RA without ILD, mixed connective tissue disease (MCTD), and IPF, reactivity by ELISA to citrullinated Hsp90 antigens was highly specific (>95 %) for RA-ILD. Moreover, these novel Abs were detected in bronchoalveolar lavage fluid in two of five patients with available samples, and their presence was not always consistent with serum findings. This observation points to local autoantibody production in the lungs, which has also been reported by Willis and colleagues for ACPA in the sputum of at-risk and early RA subjects [53]. While longitudinal studies are needed to confirm the significance of anti-citrullinated Hsp90 antibodies in RA-ILD in terms of both identifying disease and understanding the pathophysiology of disease development, it is plausible that citrullination of this ubiquitous protein may disrupt its function in protein folding, innate immune signaling, and tissue remodeling, triggering RA-ILD in a susceptible host [52].
The Lung in Preclinical RA
It is well known that RA-related Abs, including ACPA, RF, anti-PAD, and the newly described anti-carbamylated protein (anti-CarP) antibodies, circulate approximately 3 to 5 years prior to the appearance of clinically apparent IA that characterizes articular RA [54–57]. This period of autoimmunity in absence of and preceding arthritis has been termed preclinical RA, and its presence strongly supports that autoimmunity in RA starts at an extra-articular location. In addition, when coupled with emerging data that IgA-related autoimmunity (and, in particular, ACPA responses) may be a dominant feature in early RA development [58], these findings suggest that the initiation of RA-related autoimmunity occurs at a mucosal site [59].
While there are multiple mucosal sites that may be where RA initiates (e.g., oral mucosa, gut), to date, the lung has arguably been the most studied in preclinical RA. This focus on the lung has been based on a combination of factors including known risk factors for RA that primarily involve the lung (e.g., smoking) as well as a long knowledge that, in some cases, lung disease in RA precedes the appearance of articular disease [36, 60, 61]. In addition, the known immunologic mechanisms within the lung (e.g., iBALT) as discussed previously have been shown to be a site of generation of RA-related autoimmunity in established RA [49], making the lungs a prime site to investigate as a site of initiation of RA-related autoimmunity in the preclinical period of RA development.
In particular, inflammatory changes in the airways have been identified in early RA and subjects who are at risk for future RA based on serum elevations of RA-related autoantibodies in absence of synovitis [30, 62]. Specifically, Demoruelle and colleagues identified airway abnormalities suggestive of inflammation on high-resolution CT more often in seropositive at-risk subjects (76 %) compared to seronegative controls (33 %, p = 0.005) [30]. Furthermore, two of the seropositive at-risk subjects with lung abnormalities developed IA 13 months following the study, a finding that has also been described in case series of patients with ILD who, at presentation, were seropositive for RA-related autoantibodies without IA [30, 60, 63]. Specifically, Fischer and colleagues have identified a number of patients who presented with clinically apparent lung disease and were additionally serum ACPA positive in absence of IA [63]. In these subjects, AD was the predominant finding and characterized by obstructive PFT findings, airway inflammation on imaging, and lymphoplasmacytic infiltrates around the airways on histology [63]; in addition, several subjects developed classifiable articular RA during follow-up. Furthermore, while not a study of preclinical RA per se, Wischler and colleagues evaluated patients with newly diagnosed RA (median of 7 months) and found that AD was the predominant lung finding and correlated with ACPA positivity [62].
Sputum Studies Demonstrating Lung Generation of RA-Related Autoantibodies
While the presence of AD in preclinical and early established RA as described previously suggests that this particular site in the lung may be involved in RA development, identifying the airways as a site of generation of RA-related autoimmunity would serve to further support the role of the lung in RA development. Exploring this and following on their work identifying airway inflammation in subjects at risk for future RA, Demoruelle and colleagues [53] found elevated RA-related autoantibodies in the sputum of at-risk and early RA subjects (<12-month duration) compared to healthy controls. Specifically, 39 % of at-risk seronegative subjects had at least one sputum RA-related autoantibody present, followed by 65 % of at-risk seropositive subjects and 86 % of early RA subjects. This study also used ratio comparisons (Ab to total Ig levels) in sputum and serum samples to provide quantitative evidence for local generation of Abs in the lung. For all measured Abs, at-risk subjects had higher ratios of Abs to total Ig in sputum compared to serum, supporting a hypothesis of local Ab production rather than translocation from serum. Of note, these authors also pointed out that the IgA isotype, the chief mucosal antibody isotype, is important in RA pathogenesis, as there was a higher frequency of anti-CCP3.1 (IgG/IgA) reactivity in the sputum compared to other assays that measured only IgG reactivity within the seronegative at-risk group [53].
Further supporting a role for mucosal generation of RA-related autoimmunity, previously, IgA-ACPA in the serum has been shown to be highly specific for preclinical and early RA, as well as linked to smoking [58, 64]. Additionally, circulating IgA anti-CCP and IgA RF isotypes were significantly associated with mucosal inflammation among non-RA subjects with CF and indicated worse pulmonary function and more frequent disease exacerbations [29].
Mechanisms by Which RA-Related Autoimmunity May Begin at a Mucosal Surface and Then Initiate Articular Disease
As discussed previously, if RA-related autoimmunity initially develops locally in the lung, then in order to develop clinically apparent articular RA, the autoimmunity must ultimately reach the joint [65]. There are several mechanisms by which this process may occur, including cells or autoantibodies targeting antigens that are shared between sites, development of new joint-specific autoimmune responses due to epitope spreading, and circulating immune complexes driving articular disease. Furthermore, given that it has been shown in established articular RA that RA-related autoantibodies are generated within the joints [66], it is important to understand the process by which the generation of those autoantibodies in the joint is triggered after autoimmunity initially was generated at another site.
Investigating this, albeit in established early RA and not preclinical RA, Ytterberg and colleagues used mass spectrometry to prove that shared citrullinated peptides existed between bronchial tissue from early, untreated RA subjects (n = 6; 67 % anti-CCP2 positive) and synovial tissue from long-standing RA subjects (n = 7; 71 % anti-CCP2 positive). In particular, five similar citrullinated targets were identified between the two tissues, most frequently two citrullinated-vimentin (cit-vim) peptides: cit-vim 446–466 and cit-vim 440–445. Additionally, serum Ab formation against cit-vim 435–455 was measured in 14 % of RA subjects (p < 0.05 compared to healthy controls), and Ab to cit-vim peptide was associated with anti-CCP2 and SE alleles, but not smoking among RA subjects [65]. While this study supports a direct link between lung and synovium targets in RA, it is likely that other mucosal sites, such as the gingiva or gut, are also involved in the generation of RA-related autoimmunity and such research efforts are ongoing [29, 59, 67].
Autoantibodies in Patients with Lung Disease in Absence of Articular RA
As described previously, individuals who have been identified with lung disease and ACPA positivity in the absence of IA may represent a preclinical RA state [60, 63]. Alternatively, this subgroup may be a distinct autoimmune phenotype, where lung disease is either the only or major feature of a connective tissue disease (CTD), and otherwise, definitive criteria for a CTD are not met [68].
Until recently, there was lack of consensus over terminology to identify this heterogeneous group of patients; however, an international task force has put forward the term “interstitial pneumonia with autoimmune features” (IPAF) to characterize this subgroup, along with validated criteria from three domains: (1) a clinical domain with extra-thoracic features; (2) a morphological domain based on imaging, PFTs, or histopathology; and (3) a serologic domain of Abs, including high titer RF (≥2× upper limit of normal) and anti-CCP [68, 69].
In the case of IPAF, ACPA elevations may signify a localized immune response that will never progress to clinically-apparent tissue injury outside the lung, although the possibility exists that autoimmune responses are generated at an unknown clinically silent location outside of the lung, yet targeting the lung for disease.
More study is needed to confirm if the presence of ACPA in IPAF patients may indicate a better prognosis than idiopathic conditions and alter treatment choices [69]. Nevertheless, subjects with IPAF should be followed longitudinally for the development of synovitis, as a high-titer anti-CCP may signal the onset of impending RA [60, 63].
Autoantibodies and the Lung in Other Autoimmune Diseases
Relationships between autoantibodies and lung diseases in other autoimmune diseases have been well described and further support that the lung has a pathophysiologic relationship with autoimmunity. In particular, anti-histidyl transfer RNA synthetase (anti-Jo1) autoantibody is well described in a subset of patients with idiopathic inflammatory myositis (IIM) especially with the anti-synthetase syndrome that is defined by ILD in the setting of Raynaud’s phenomenon, mechanic’s hands, non-erosive arthritis, and constitutional symptoms [70]. Levine and colleagues found that autoimmunity in anti-Jo1 myositis may start in the lung after confirming that Jo1 antigen expression is upregulated and altered in the lung [71]. Moreover, the majority of subjects with anti-Jo1 myositis develop ILD, supporting a pathogenic role of this Ab in myositis-related lung disease [70]. Furthermore, several studies suggest a strong relationship between anti-Sjogren's Syndrome related antigen A (anti-SSA) and lung disease including a retrospective study by Ferreira and colleagues, who examined 162 CTD patients, excluding systemic sclerosis, and found a higher frequency of ILD in the anti-SSA autoantibody-positive group compared to autoantibody-negative patients (71.4 vs. 16.7 %, p = 0.018), although the relationship between anti-SSA and RA-related lung disease was not examined [72]. In addition, Yazisiz and colleagues reported a higher frequency of autoantibodies including anti-Ro, La, ANA, and RF in the subset of pSS patients with lung disease [73].
Conclusions and Future Directions
Lung disease is a frequent complication of established RA and, based on the most up-to-date literature, appears to be intimately associated with ACPA positivity. In addition, there is an emerging understanding that lung-related processes, and in particular airway inflammation, may play an important role in the initiation of RA-related autoimmunity even prior to the development of IA. Of particular interest to the field is that if the earliest processes that drive the development of RA are understood, it could lead to novel treatment approach for lung disease in established RA or preventive approaches to lung disease or ultimately even the prevention of articular disease.
However, in order to reach these goals of improved treatments or disease prevention, several aspects of lung disease need further attention (Table 2). In particular, we need clear and homogenous nomenclature to define types of lung disease that may be present in RA. For example, clearly defining what is meant by AD and parenchymal fibrosis will be important in homogenizing research findings. Furthermore, understanding the natural history of lung disease in RA is important to understanding the pathophysiology of disease. For example, given AD appears to be common in early established RA, as described in Fig. 1, does lung involvement somehow evolve from isolated AD to parenchymal disease over the course of RA, and could the pathophysiologic processes related to disease at each of these sites be different?

Model of the potential role of the lung in RA-related autoimmunity. In this model, rheumatoid arthritis (RA)-related autoimmunity may be initially generated in the lung and be primarily related to airway inflammation. Over time, this autoimmunity systemic (B) eventually targets the joints (C), leading to the characteristic articular disease of RA. In addition, evolving autoimmunity in the lung, joints, or elsewhere may lead to progression of lung disease and, perhaps, the development of specific types of lung disease (e.g., parenchymal or airways)
In addition, the role of the lung in the generation of autoimmunity, and in particular ACPA generation and relationship to genetic and environmental factors, needs further study. For example, the complex interplay of genetic, environmental (e.g., smoking, microbiome) factors at a mucosal surface needs exploration. In addition, it is not clear if the earliest breaks in tolerance in early RA at mucosal surfaces are solely ACPA related. A study by Quirk and colleagues found that patients with BR in absence of RA demonstrated autoantibody responses to non-citrullinated antigens, while in RA, citrullinated responses were dominant [74]. This could indicate that the earliest mucosal-related autoimmune responses are to non-citrullinated antigens, and identifying these responses could provide critical insights into the earliest breaks in tolerance in RA. Moreover, processes in the lung are unlikely to explain RA development in every individual, so other candidate mucosal sites (e.g., periodontium) should be evaluated for the development of RA. Furthermore, studies of SLE, pSS, IIM and even diseases associated with anti-neutrophil cytoplasmic antibodies should help to broaden the understanding of a potential role of the lung and other mucosal sites in the generation of autoimmunity. In addition, findings from other types of lung disease may shed light on pathophysiologic processes of lung disease in RA, as well as potential treatments. For example, approaches that have identified associations of specific genetic factors such as MUC5b polymorphisms with IPF may be relevant in RA [75], and the pharmacologic agents now approved for the treatment of IPF may warrant exploration in RA-related lung disease [76].
Finally, while much work in RA has thus far focused on autoantibody response and using antigens (and, in particular, citrullinated antigens), widespread use of advanced laboratory techniques including identification of broader antigen reactivity, the relationship between ACPA and other autoantibodies (e.g., RF), and improving techniques to study cellular processes such as specific T and B cell reactivity to antigens are needed to identify new processes and biomarkers that are superior or complementary to ACPA in order to better predict, diagnose, and guide treatment of RA lung involvement.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
Demoruelle MK, Parish MC, Derber LA, Kolfenbach JR, Hughes-Austin JM, Weisman MH, et al. Performance of anti-cyclic citrullinated peptide assays differs in subjects at increased risk of rheumatoid arthritis and subjects with established disease. Arthritis Rheum. 2013;65(9):2243–52. doi:10.1002/art.38017.
Spector TD. Rheumatoid arthritis. Rheum Dis Clin N Am. 1990;16(3):513–37.
Turesson C, Jacobsson LT, Sturfelt G, Matteson EL, Mathsson L, Ronnelid J. Rheumatoid factor and antibodies to cyclic citrullinated peptides are associated with severe extra-articular manifestations in rheumatoid arthritis. Ann Rheum Dis. 2007;66(1):59–64. doi:10.1136/ard.2006.054445.
Nannini C, Ryu JH, Matteson EL. Lung disease in rheumatoid arthritis. Curr Opin Rheumatol. 2008;20(3):340–6. doi:10.1097/BOR.0b013e3282f798ed.
Ascherman DP. Interstitial lung disease in rheumatoid arthritis. Curr Rheumatol Rep. 2010;12(5):363–9. doi:10.1007/s11926-010-0116-z.
Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, Cooper NS, et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988;31(3):315–24.
Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham 3rd CO, et al. 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010;62(9):2569–81. doi:10.1002/art.27584.
Gerlag DM, Raza K, van Baarsen LG, Brouwer E, Buckley CD, Burmester GR, et al. EULAR recommendations for terminology and research in individuals at risk of rheumatoid arthritis: report from the Study Group for Risk Factors for Rheumatoid Arthritis. Ann Rheum Dis. 2012;71(5):638–41. doi:10.1136/annrheumdis-2011-200990.
Chatzidionisyou A, Catrina AI. The lung in rheumatoid arthritis, cause or consequence? Curr Opin Rheumatol. 2016;28(1):76–82. doi:10.1097/BOR.0000000000000238.
Gabbay E, Tarala R, Will R, Carroll G, Adler B, Cameron D, et al. Interstitial lung disease in recent onset rheumatoid arthritis. Am J Respir Crit Care Med. 1997;156(2 Pt 1):528–35. doi:10.1164/ajrccm.156.2.9609016.
van den Oever IA, Sattar N, Nurmohamed MT. Thromboembolic and cardiovascular risk in rheumatoid arthritis: role of the haemostatic system. Ann Rheum Dis. 2014;73(6):954–7. doi:10.1136/annrheumdis-2013-204767.
Iqbal K, Kelly C. Treatment of rheumatoid arthritis-associated interstitial lung disease: a perspective review. Ther Adv Musculoskelet Dis. 2015;7(6):247–67. doi:10.1177/1759720x15612250.
Tsuchiya Y, Takayanagi N, Sugiura H, Miyahara Y, Tokunaga D, Kawabata Y, et al. Lung diseases directly associated with rheumatoid arthritis and their relationship to outcome. Eur Respir J. 2011;37(6):1411–7. doi:10.1183/09031936.00019210.
Sparks JA, Chang SC, Liao KP, Lu B, Fine AR, Solomon DH, et al. Rheumatoid arthritis and mortality among women during 36 years of prospective follow-up: results from the Nurses’ Health Study. Arthritis Care Res (Hoboken). 2016;68(6):753–62. doi:10.1002/acr.22752. Identifies that lung disease is a leading cause of mortality in RA. Furthermore, identifies that obstructive lung disease rather than ILD may be important in mortality.
Nannini C, Medina-Velasquez YF, Achenbach SJ, Crowson CS, Ryu JH, Vassallo R, et al. Incidence and mortality of obstructive lung disease in rheumatoid arthritis: a population-based study. Arthritis Care Res (Hoboken). 2013;65(8):1243–50. doi:10.1002/acr.21986. Describes the prevalence and incidence of lung disease in RA.
Sparks JA, Chang SC, Karlson EW. Reply. Arthritis Care Res (Hoboken). 2016;68(8):1211–2. doi:10.1002/acr.22838.
Kelly CA, Saravanan V, Nisar M, Arthanari S, Woodhead FA, Price-Forbes AN, et al. Rheumatoid arthritis-related interstitial lung disease: associations, prognostic factors and physiological and radiological characteristics—a large multicentre UK study. Rheumatology (Oxford). 2014;53(9):1676–82. doi:10.1093/rheumatology/keu165.
Rocha-Munoz AD, Ponce-Guarneros M, Gamez-Nava JI, Olivas-Flores EM, Mejia M, Juarez-Contreras P, et al. Anti-cyclic citrullinated peptide antibodies and severity of interstitial lung disease in women with rheumatoid arthritis. J Immunol Res. 2015;2015:151626. doi:10.1155/2015/151626. Review of the risk factors for RA-related ILD, including elevated ACPA.
Restrepo JF, del Rincon I, Battafarano DF, Haas RW, Doria M, Escalante A. Clinical and laboratory factors associated with interstitial lung disease in rheumatoid arthritis. Clin Rheumatol. 2015;34(9):1529–36. doi:10.1007/s10067-015-3025-8.
Giles JT, Danoff SK, Sokolove J, Wagner CA, Winchester R, Pappas DA, et al. Association of fine specificity and repertoire expansion of anticitrullinated peptide antibodies with rheumatoid arthritis associated interstitial lung disease. Ann Rheum Dis. 2014;73(8):1487–94. doi:10.1136/annrheumdis-2012-203160. Primary study identifying that expanded ACPA repertoire is related to ILD.
Vencovsky J, Machacek S, Sedova L, Kafkova J, Gatterova J, Pesakova V, et al. Autoantibodies can be prognostic markers of an erosive disease in early rheumatoid arthritis. Ann Rheum Dis. 2003;62(5):427–30.
Mori S, Koga Y, Sugimoto M. Different risk factors between interstitial lung disease and airway disease in rheumatoid arthritis. Respir Med. 2012;106(11):1591–9. doi:10.1016/j.rmed.2012.07.006. Primary study evaluating different types of lung disease in RA (airways and ILD) and separate risk factors for each of these manifestations.
Inui N, Enomoto N, Suda T, Kageyama Y, Watanabe H, Chida K. Anti-cyclic citrullinated peptide antibodies in lung diseases associated with rheumatoid arthritis. Clin Biochem. 2008;41(13):1074–7. doi:10.1016/j.clinbiochem.2008.06.014. Primary studying identifying that RA-related autoantibodies can be generated in the lung in individuals without classifiable RA.
Perry E, Kelly C, Eggleton P, De Soyza A, Hutchinson D. The lung in ACPA-positive rheumatoid arthritis: an initiating site of injury? Rheumatology (Oxford). 2014;53(11):1940–50. doi:10.1093/rheumatology/keu195.
Perry E, Eggleton P, De Soyza A, Hutchinson D, Kelly C. Increased disease activity, severity and autoantibody positivity in rheumatoid arthritis patients with co-existent bronchiectasis. International Journal of Rheumatic Diseases. 2015. doi:10.1111/1756-185x.12702
Walker WC. Pulmonary infections and rheumatoid arthritis. Q J Med. 1967;36(142):239–51.
Kaushik VV, Hutchinson D, Desmond J, Lynch MP, Dawson JK. Association between bronchiectasis and smoking in patients with rheumatoid arthritis. Ann Rheum Dis. 2004;63(8):1001–2. doi:10.1136/ard.2003.015123.
Perry E, Stenton C, Kelly C, Eggleton P, Hutchinson D, De Soyza A. RA autoantibodies as predictors of rheumatoid arthritis in non-cystic fibrosis bronchiectasis patients. Eur Respir J. 2014;44(4):1082–5. doi:10.1183/09031936.00064014.
Janssen KM, de Smit MJ, Brouwer E, de Kok FA, Kraan J, Altenburg J, et al. Rheumatoid arthritis-associated autoantibodies in non-rheumatoid arthritis patients with mucosal inflammation: a case-control study. Arthritis Res Ther. 2015;17:174. doi:10.1186/s13075-015-0690-6.
Demoruelle MK, Weisman MH, Simonian PL, Lynch DA, Sachs PB, Pedraza IF, et al. Brief report: airways abnormalities and rheumatoid arthritis-related autoantibodies in subjects without arthritis: early injury or initiating site of autoimmunity? Arthritis Rheum. 2012;64(6):1756–61. doi:10.1002/art.34344.
Turesson C, Jacobsson LT. Epidemiology of extra-articular manifestations in rheumatoid arthritis. Scand J Rheumatol. 2004;33(2):65–72.
Dawson JK, Fewins HE, Desmond J, Lynch MP, Graham DR. Fibrosing alveolitis in patients with rheumatoid arthritis as assessed by high resolution computed tomography, chest radiography, and pulmonary function tests. Thorax. 2001;56(8):622–7.
Skare TL, Nakano I, Escuissiato DL, Batistetti R, Rodrigues Tde O, Silva MB. Pulmonary changes on high-resolution computed tomography of patients with rheumatoid arthritis and their association with clinical, demographic, serological and therapeutic variables. Rev Bras Reumatol. 2011;51(4):325–30. 36-7.
Zhu J, Zhou Y, Chen X, Li J. A metaanalysis of the increased risk of rheumatoid arthritis-related pulmonary disease as a result of serum anticitrullinated protein antibody positivity. J Rheumatol. 2014;41(7):1282–9. doi:10.3899/jrheum.131341.
Sokolove J, Bromberg R, Deane KD, Lahey LJ, Derber LA, Chandra PE, et al. Autoantibody epitope spreading in the pre-clinical phase predicts progression to rheumatoid arthritis. PLoS One. 2012;7(5):e35296. doi:10.1371/journal.pone.0035296.
Klareskog L, Stolt P, Lundberg K, Kallberg H, Bengtsson C, Grunewald J, et al. A new model for an etiology of rheumatoid arthritis: smoking may trigger HLA-DR (shared epitope)-restricted immune reactions to autoantigens modified by citrullination. Arthritis Rheum. 2006;54(1):38–46. doi:10.1002/art.21575.
Kallberg H, Ding B, Padyukov L, Bengtsson C, Ronnelid J, Klareskog L, et al. Smoking is a major preventable risk factor for rheumatoid arthritis: estimations of risks after various exposures to cigarette smoke. Ann Rheum Dis. 2011;70(3):508–11. doi:10.1136/ard.2009.120899.
Makrygiannakis D, Hermansson M, Ulfgren AK, Nicholas AP, Zendman AJ, Eklund A, et al. Smoking increases peptidylarginine deiminase 2 enzyme expression in human lungs and increases citrullination in BAL cells. Ann Rheum Dis. 2008;67(10):1488–92. doi:10.1136/ard.2007.075192.
Giles JT, Darrah E, Danoff S, Johnson C, Andrade F, Rosen A, et al. Association of cross-reactive antibodies targeting peptidyl-arginine deiminase 3 and 4 with rheumatoid arthritis-associated interstitial lung disease. PLoS One. 2014;9(6):e98794. doi:10.1371/journal.pone.0098794.
Darrah E, Giles JT, Ols ML, Bull HG, Andrade F, Rosen A. Erosive rheumatoid arthritis is associated with antibodies that activate PAD4 by increasing calcium sensitivity. Sci Transl Med. 2013;5(186):186ra65. doi:10.1126/scitranslmed.3005370.
Shelef MA, Bennin DA, Mosher DF, Huttenlocher A. Citrullination of fibronectin modulates synovial fibroblast behavior. Arthritis Res Ther. 2012;14(6):R240. doi:10.1186/ar4083.
Reynisdottir G, Karimi R, Joshua V, Olsen H, Hensvold AH, Harju A, et al. Structural changes and antibody enrichment in the lungs are early features of anti-citrullinated protein antibody-positive rheumatoid arthritis. Arthritis Rheumatol. 2014;66(1):31–9. doi:10.1002/art.38201.
Catrina AI, Ytterberg AJ, Reynisdottir G, Malmstrom V, Klareskog L. Lungs, joints and immunity against citrullinated proteins in rheumatoid arthritis. Nat Rev Rheumatol. 2014;10(11):645–53. doi:10.1038/nrrheum.2014.115.
Sparks JA, Karlson EW. The roles of cigarette smoking and the lung in the transitions between phases of preclinical rheumatoid arthritis. Curr Rheumatol Rep. 2016;18(3):15. doi:10.1007/s11926-016-0563-2.
Larsen JM, Steen-Jensen DB, Laursen JM, Sondergaard JN, Musavian HS, Butt TM, et al. Divergent pro-inflammatory profile of human dendritic cells in response to commensal and pathogenic bacteria associated with the airway microbiota. PLoS One. 2012;7(2):e31976. doi:10.1371/journal.pone.0031976.
Thannickal VJ, Toews GB, White ES, Lynch 3rd JP, Martinez FJ. Mechanisms of pulmonary fibrosis. Annu Rev Med. 2004;55:395–417. doi:10.1146/annurev.med.55.091902.103810.
Turesson C, Matteson EL, Colby TV, Vuk-Pavlovic Z, Vassallo R, Weyand CM, et al. Increased CD4+ T cell infiltrates in rheumatoid arthritis-associated interstitial pneumonitis compared with idiopathic interstitial pneumonitis. Arthritis Rheum. 2005;52(1):73–9. doi:10.1002/art.20765.
Atkins SR, Turesson C, Myers JL, Tazelaar HD, Ryu JH, Matteson EL, et al. Morphologic and quantitative assessment of CD20+ B cell infiltrates in rheumatoid arthritis-associated nonspecific interstitial pneumonia and usual interstitial pneumonia. Arthritis Rheum. 2006;54(2):635–41. doi:10.1002/art.21758.
Rangel-Moreno J, Hartson L, Navarro C, Gaxiola M, Selman M, Randall TD. Inducible bronchus-associated lymphoid tissue (iBALT) in patients with pulmonary complications of rheumatoid arthritis. J Clin Invest. 2006;116(12):3183–94. doi:10.1172/JCI28756.
Reynisdottir G, Olsen H, Joshua V, Engstrom M, Forsslund H, Karimi R et al. Signs of immune activation and local inflammation are present in the bronchial tissue of patients with untreated early rheumatoid arthritis. Ann Rheum Dis. 2015. doi:10.1136/annrheumdis-2015-208216
Brown LE DM, Parish MC, Feser ML, Sachs PB, Heinz DE, Cool CD, Deane KD. Ectopic lymphoid tissue in the lung is associated with serum rheumatoid arthritis-related autoantibodies even in absence of clinically apparent rheumatoid arthritis [Abstract 963]. Arthritis Rheumatol. 2015;67 (S10): abstract 963. doi: 10.1002/art.39448.
Harlow L, Rosas IO, Gochuico BR, Mikuls TR, Dellaripa PF, Oddis CV, et al. Identification of citrullinated hsp90 isoforms as novel autoantigens in rheumatoid arthritis-associated interstitial lung disease. Arthritis Rheum. 2013;65(4):869–79. doi:10.1002/art.37881.
Willis VC, Demoruelle MK, Derber LA, Chartier-Logan CJ, Parish MC, Pedraza IF, et al. Sputum autoantibodies in patients with established rheumatoid arthritis and subjects at risk of future clinically apparent disease. Arthritis Rheum. 2013;65(10):2545–54. doi:10.1002/art.38066.
Nielen MM, van Schaardenburg D, Reesink HW, van de Stadt RJ, van der Horst-Bruinsma IE, de Koning MH, et al. Specific autoantibodies precede the symptoms of rheumatoid arthritis: a study of serial measurements in blood donors. Arthritis Rheum. 2004;50(2):380–6. doi:10.1002/art.20018.
Shi J, van de Stadt LA, Levarht EW, Huizinga TW, Hamann D, van Schaardenburg D, et al. Anti-carbamylated protein (anti-CarP) antibodies precede the onset of rheumatoid arthritis. Ann Rheum Dis. 2014;73(4):780–3. doi:10.1136/annrheumdis-2013-204154.
Brusca SB, Abramson SB, Scher JU. Microbiome and mucosal inflammation as extra-articular triggers for rheumatoid arthritis and autoimmunity. Curr Opin Rheumatol. 2014;26(1):101–7. doi:10.1097/bor.0000000000000008.
Kolfenbach JR, Deane KD, Derber LA, O’Donnell CI, Gilliland WR, Edison JD, et al. Autoimmunity to peptidyl arginine deiminase type 4 precedes clinical onset of rheumatoid arthritis. Arthritis Rheum. 2010;62(9):2633–9. doi:10.1002/art.27570.
Barra L, Scinocca M, Saunders S, Bhayana R, Rohekar S, Racape M, et al. Anti-citrullinated protein antibodies in unaffected first-degree relatives of rheumatoid arthritis patients. Arthritis Rheum. 2013;65(6):1439–47. doi:10.1002/art.37911.
Demoruelle MK, Deane KD, Holers VM. When and where does inflammation begin in rheumatoid arthritis? Curr Opin Rheumatol. 2014;26(1):64–71. doi:10.1097/BOR.0000000000000017.
Gizinski AM, Mascolo M, Loucks JL, Kervitsky A, Meehan RT, Brown KK, et al. Rheumatoid arthritis (RA)-specific autoantibodies in patients with interstitial lung disease and absence of clinically apparent articular RA. Clin Rheumatol. 2009;28(5):611–3. doi:10.1007/s10067-009-1128-9.
Mikuls TR, Payne JB, Deane KD, Thiele GM. Autoimmunity of the lung and oral mucosa in a multisystem inflammatory disease: the spark that lights the fire in rheumatoid arthritis? J Allergy Clin Immunol. 2016;137(1):28–34. doi:10.1016/j.jaci.2015.10.024.
Wilsher M, Voight L, Milne D, Teh M, Good N, Kolbe J, et al. Prevalence of airway and parenchymal abnormalities in newly diagnosed rheumatoid arthritis. Respir Med. 2012;106(10):1441–6. doi:10.1016/j.rmed.2012.06.020.
Fischer A, Solomon JJ, du Bois RM, Deane KD, Olson AL, Fernandez-Perez ER, et al. Lung disease with anti-CCP antibodies but not rheumatoid arthritis or connective tissue disease. Respir Med. 2012;106(7):1040–7. doi:10.1016/j.rmed.2012.03.006.
Svard A, Kastbom A, Reckner-Olsson A, Skogh T. Presence and utility of IgA-class antibodies to cyclic citrullinated peptides in early rheumatoid arthritis: the Swedish TIRA project. Arthritis Res Ther. 2008;10(4):R75. doi:10.1186/ar2449.
Ytterberg AJ, Joshua V, Reynisdottir G, Tarasova NK, Rutishauser D, Ossipova E, et al. Shared immunological targets in the lungs and joints of patients with rheumatoid arthritis: identification and validation. Ann Rheum Dis. 2015;74(9):1772–7. doi:10.1136/annrheumdis-2013-204912.
Ossipova E, Cerqueira CF, Reed E, Kharlamova N, Israelsson L, Holmdahl R, et al. Affinity purified anti-citrullinated protein/peptide antibodies target antigens expressed in the rheumatoid joint. Arthritis Res Ther. 2014;16(4):R167. doi:10.1186/ar4683.
Liu X, Zou Q, Zeng B, Fang Y, Wei H. Analysis of fecal Lactobacillus community structure in patients with early rheumatoid arthritis. Curr Microbiol. 2013;67(2):170–6. doi:10.1007/s00284-013-0338-1.
Fischer A, Antoniou KM, Brown KK, Cadranel J, Corte TJ, du Bois RM, et al. An official European Respiratory Society/American Thoracic Society research statement: interstitial pneumonia with autoimmune features. Eur Respir J. 2015;46(4):976–87. doi:10.1183/13993003.00150-2015.
Oldham JM, Adegunsoye A, Valenzi E, Lee C, Witt L, Chen L et al. Characterisation of patients with interstitial pneumonia with autoimmune features. Eur Respir J. 2016. doi:10.1183/13993003.01565-2015
Fathi M, Lundberg IE. Interstitial lung disease in polymyositis and dermatomyositis. Curr Opin Rheumatol. 2005;17(6):701–6.
Levine SM, Raben N, Xie D, Askin FB, Tuder R, Mullins M, et al. Novel conformation of histidyl-transfer RNA synthetase in the lung: the target tissue in Jo-1 autoantibody-associated myositis. Arthritis Rheum. 2007;56(8):2729–39. doi:10.1002/art.22790.
Ferreira JP, Almeida I, Marinho A, Cerveira C, Vasconcelos C. Anti-Ro52 antibodies and interstitial lung disease in connective tissue diseases excluding scleroderma. ISRN Rheumatol. 2012;2012:415272. doi:10.5402/2012/415272.
Yazisiz V, Arslan G, Ozbudak IH, Turker S, Erbasan F, Avci AB, et al. Lung involvement in patients with primary Sjogren’s syndrome: what are the predictors? Rheumatol Int. 2010;30(10):1317–24. doi:10.1007/s00296-009-1152-8.
Quirke AM, Perry E, Cartwright A, Kelly C, De Soyza A, Eggleton P, et al. Bronchiectasis is a model for chronic bacterial infection inducing autoimmunity in rheumatoid arthritis. Arthritis Rheumatol. 2015;67(9):2335–42. doi:10.1002/art.39226.
Yang IV, Fingerlin TE, Evans CM, Schwarz MI, Schwartz DA. MUC5B and idiopathic pulmonary fibrosis. Ann Am Thorac Soc. 2015;12 Suppl 2:S193–9. doi:10.1513/AnnalsATS.201503-110AW.
Adegunsoye A, Strek ME. Therapeutic approach to adult fibrotic lung diseases. Chest. 2016. doi:10.1016/j.chest.2016.07.027
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflicts of interest.
Human and Animal Rights and Informed Consent
All reported studies/experiments with human or animal subjects performed by the authors have been previously published and were in compliance with all applicable ethical standards (including the Helsinki Declaration and its amendments, institutional/national research committee standards, and international/national/institutional guidelines).
Financial Support and Grants
LBK and MKD were supported by the NIH grants (AR-07534, AR066712) and the Rheumatology Research & Education Foundation. In addition, LBK was supported in part by funding through a VA Accreditation Council for Graduate Medical Education Enhancement Award.
Additional information
This article is part of the Topical Collection on Rheumatoid Arthritis
Rights and permissions
About this article

Cite this article
Kelmenson, L.B., Demoruelle, M.K. & Deane, K.D. The Complex Role of the Lung in the Pathogenesis and Clinical Outcomes of Rheumatoid Arthritis. Curr Rheumatol Rep 18, 69 (2016). https://doi.org/10.1007/s11926-016-0618-4
Published:
DOI: https://doi.org/10.1007/s11926-016-0618-4