
Abstract
Purpose of Review
Individuals with attention-deficit hyperactivity disorder (ADHD) may be unusually sensitive to screen media technology (SMT), from television to mobile devices. Although an association between ADHD and SMT use has been confirmed, its importance is uncertain partly due to variability in the way SMT has been conceptualized and measured. Here, we identify distinct, quantifiable dimensions of SMT use and review possible links to ADHD to facilitate more precise, reproducible investigation.
Recent Findings
Display characteristics, media multitasking, device notifications, SMT addiction, and media content all may uniquely impact the ADHD phenotype. Each can be investigated with a digital health approach and counteracted with device-based interventions. Novel digital therapeutics for ADHD demonstrate that specific forms of SMT can also have positive effects.
Summary
Further study should quantify how distinct dimensions of SMT use relate to ADHD. SMT devices themselves can serve as a self-monitoring study platform and deliver digital interventions.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The average US adult now spends over 9 h per day using screen media technology (SMT) [1] due largely to rising mobile device use [2, 3], which has surpassed television viewing among younger adults [1, 4]. For the typical American, “screen time” now occupies a majority of waking life: our screens are not just for entertainment but also for work and communication and are deeply integrated in our personal, social, family, and professional activities. In a recent conceptual article, Dr. Adam Gazzaley noted that “every way we interact with our environment, as well as with each other and ourselves, has been radically transformed by technology” [5]. It is natural, then, to be concerned about the effects these technologies may be having on our well-being, and on our minds—particularly the developing minds of children and adolescents, whose media use patterns have shifted most dramatically [1].
Scientific and popular articles have questioned the impact of SMT on mental health, pointing to increasing rates of depression and suicide among adolescents in parallel with growing device use [6•]. Although a statistically significant association between SMT use and well-being has been established, the size of the effect is small, and thus its importance has been debated [6•, 7•, 8]. There has also been growing concern that technology may be affecting our cognition [5, 9], including our ability to control and sustain attention, fueled partly by the rise in diagnosis rates of attention-deficit hyperactivity disorder (ADHD) that has taken place over the past 10 years [10].
ADHD, a neurodevelopmental disorder characterized by deficits in attentional and behavioral control, represents a key, sentinel phenotype that might alert us to the negative impacts of SMT. Due to the nature of the condition, individuals with ADHD may be unusually sensitive to cognitive effects associated with SMT use, whether positive or negative. While the causes of the rise in ADHD diagnosis rates are certainly multifactorial [11], media use has long been suspected as a contributing factor [12•]. Despite a surge of interest in this topic seen in the scientific literature, evidence for the effect of SMT on attention and other aspects of cognitive functioning has thus far been mixed and inconclusive [13••].
Purpose of Review
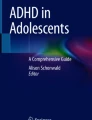
We propose a paradigm for conceptualizing and studying the impact of SMT on ADHD and other neurocognitive phenotypes, one focused on isolating the effects of five distinct, quantifiable dimensions of SMT use (see Fig. 1). These include dimensions unique to newer devices that might be examined by leveraging the devices themselves as the primary study platform.

Overview of distinct dimensions of screen media technology use that may impact the ADHD phenotype
We begin by highlighting the challenges of studying SMT, including sources of variability and imprecision that have contributed to the conflicting and inconclusive findings in the literature. We then describe each dimension of SMT use and summarize (a) what is known about its relationship to ADHD, and (b) how it has been, or might be, explored with a digital health study design. In choosing this organizational principle, we hope to encourage further study examining these dimensions individually, leading to interventions designed to counteract specific, hazardous forms of SMT use. Finally, we touch on the emerging field of digital therapeutics, which seeks to develop SMT-based interventions to treat impairments related to ADHD and other dimensions of cognitive and psychosocial functioning. Throughout, current technologies are emphasized not only as a potential hazard but also as a flexible platform for studying that hazard and delivering digital interventions.
Challenges of Studying SMT
In this section, we identify several challenges inherent in measuring and studying the effects of SMT on ADHD and other phenotypes, then suggest how the field might move forward.
Defining and Measuring Screen Time
An association between well-being and SMT use has been confirmed in large-scale, observational datasets [6•, 7•] and by meta-analysis [8], but effect sizes are small, with SMT use explaining < 1% of the variance in depression and related outcomes [6•, 7•, 8]. Although the statistical findings of these studies have been consistent, interpretations have varied widely. For example, one study emphasized that “new media screen time should be understood as an important modern risk factor for depression and suicide” [6•], whereas another came to the opposite conclusion, stating that “effects of technology might be statistically significant but so minimal that they hold little practical value” [7•].
A similar debate is taking place in the ADHD literature. A recent, 2-year longitudinal study of high school students in Los Angeles County found that higher self-reported digital media use was associated with increased odds of self-reported inattentive and hyperactive-impulsive symptoms at follow-up [14••]. This result corroborated and extended previously identified cross-sectional associations [15], but with a small effect size based entirely on self-report [14••, 16]. Echoing this uncertainty, a recent review found “contradictory and inconclusive” evidence for the impact of SMT on our attentional processes, working memory, and reward seeking [13••]. Findings connecting SMT use to ADHD-related symptoms have been sufficiently robust to prompt valid concern [17•, 18], but too imprecise to provide insight or a way forward short of curbing all device use.
Inconsistency in the methods used to quantify SMT use is partly to blame. With the exception of a limited number of laboratory studies [12•, 19, 20••], assessment of SMT use has relied on ad hoc questionnaires that vary widely in their structure and the breakdown of SMT-related activities. For example, one study asks about the frequency of 14 SMT-related activities spanning multiple devices [14••], whereas another asks about the total duration of only 5 activities [21]. Several validated questionnaires [22, 23] have been used [21, 24•] but have become somewhat outdated with the rapid changes in SMT use patterns that have taken place. Only recently has mobile device use been assessed [25], with studies as few as 5 years ago not including them [26, 27]. Some investigations have explored the differential impact of distinct activities accessed through a single device [19], whereas others have grouped activities and devices together to explore the effect of SMT as a whole [24•]. While it is important to study the full range of SMT use, our understanding of its impact on ADHD has been limited by imprecision and variability in the way SMT has been conceptualized and measured.
Limitations of Available Study Designs
The vast majority of findings linking SMT to ADHD have been derived from cross-sectional studies, leading to uncertainty about cause versus effect. Results from large-scale, longitudinal studies provide stronger evidence that SMT use may contribute to ADHD-related symptoms, but conclusions remain tentative due to possible unmeasured confounders [14••, 28]. Because SMT is so ubiquitous, identifying large groups of participants who differ only in their SMT use is challenging at best, and finding participants with no exposure is near-impossible [13••].
These concerns could, in principle, be addressed with a randomized study design. Unfortunately, randomizing participants to SMT conditions for a suitable time period is impractical precisely because SMT is so deeply integrated in daily life. Indeed, a recent “24-h challenge” study found it difficult to identify participants willing to constrain their device use for a single day [29]. When randomized controlled trials have been conducted, they have been restricted to time-limited experimental conditions and their immediate effects. For example, several studies have examined the effect of television program pacing on subsequent symptoms of attention and hyperactivity [12•]. However, these short-term designs do not shed light on the longer-term neurocognitive impact of SMT use that has been hypothesized.
Rapidly changing SMT use patterns also strain the slow pace of scientific research. In addition to previously noted challenges in measuring use, rapid changes in SMT adoption may lead the composition of specific groups (e.g., video gamers) to differ systematically between studies.
Replacement Effects
In addition to the direct effects of SMT use on ADHD, a number of studies have emphasized the importance of replacement effects, wherein time using SMT might otherwise be spent engaging in activities with positive impact on ADHD-related symptoms and impairment. For example, both television watching and cell phone use have been linked to poorer cardiovascular health and reduced physical activity [30, 31], thereby reducing the potential benefit of physical activity on ADHD-related symptoms [32].
Importantly, SMT use has been found to reduce sleep in individuals with ADHD, which may in turn contribute to ADHD-related symptoms [21]. Nighttime SMT use has been associated with reduced sleep in older children and adolescents with ADHD [24•], and the mere presence of a television in the bedroom may have a small effect on average sleep duration [27]. However, media use has also been connected to additional sleep problems beyond sleep duration, such as increased sleep onset latency [24•], suggesting that nighttime media use may have a physiological impact on sleep that goes beyond a simple replacement effect. This is later discussed in more detail.
Replacement effects are not a dimension of SMT use itself, and therefore are not included among the quantifiable dimensions we have identified. However, understanding how these effects may mediate the relationship between SMT and ADHD is critical and might be investigated with digital health study designs that quantify sleep and physical activity in addition to SMT use.
Toward Quantifiable SMT Metrics
In light of these challenges, a recent commentary emphasized the need to “go beyond self-report” with apps that record detailed patterns of device use [28]. This approach leverages a key advantage of current technologies, namely that they are capable of self-monitoring. Instead of relying on coarse measures such as total screen time, device-based study platforms can quantify app use and timing, multitasking patterns, and the number and timing of notifications [33]. These observational data might be paired with outcomes of interest to test specific hypotheses that, if validated, would naturally lead to device modifications or non-digital interventions designed to counteract any negative effects identified. For example, if high notification frequency were conclusively linked to increased symptoms of inattention, an intervention might include scheduled periods when the device is placed in “do not disturb” mode (device-based implementation) or left in another room (non-device-based implementation). Intervention effectiveness could then be evaluated using a traditional trial or a range of small-scale, quasi-experimental digital health study designs [34].
Hazards of SMT Use and Options for Mitigating Impact
Having described challenges in studying the effects of SMT on ADHD, we now propose five dimensions of SMT use that might be better isolated going forward to promote a more precise, actionable program of research.
Screen Characteristics
Screen size, brightness, color profile, and other characteristics vary between devices and display technologies (e.g., LCD, OLED) and may pose health risks independent of specific SMT content or activities. For example, prolonged screen viewing is known to cause visual fatigue, with some evidence suggesting that over 50% of the adult US population is affected by symptoms such as blurred vision, eye irritation, or headache [35]. Screen flicker (i.e., oscillating brightness) also has established biological effects [36], but these are less of a concern with current high-frequency, LED-illuminated displays [37].
In ADHD, the negative impact of nighttime media use may be exacerbated by the bright artificial light emitted by SMT, which increases arousal and suppresses melatonin production [38, 39]. In a crossover study comparing nighttime use of an e-reader to a printed book, e-reader use was associated with increased sleep onset latency, reduced evening melatonin secretion, and reduced next-morning alertness [40]. Newer, LED-based technologies may have greatest impact due to their higher blue-light activity, which suppresses melatonin production and shifts the circadian cycle more effectively than other parts of the spectrum [41, 42]. Compared to red-enriched light, exposure to a blue-enriched light environment reduces reaction time variability and increases sleep onset latency [43].
These effects are particularly concerning among adolescents given the critical importance of sleep on adolescent neural development [44] and high nighttime SMT use in this group [24•]. Some evidence has suggested that effects of light on melatonin suppression may be stronger in early adolescence [45], and nighttime media use has been linked to reduced, poor sleep in adolescents with ADHD [24•].
Device-based interventions include f.lux [46] and Apple’s Night Shift, which appear to reduce melatonin suppression by limiting brightness and blue light in the evening hours [47,48,49], but were not found to impact sleep onset latency or sleep quality [50]. Alternatively, external filters can reduce screen brightness and/or blue light. In one study, blue-light-reducing eyewear reduced sleep latency and melatonin suppression, but results may have been confounded by unintended effects of the eyewear on vision sharpness [51]. A second study found that combining a blue-light filter with the removal of personally relevant social media content improved sleep quality, whereas either intervention alone did not [52]. However, these interventions have not yet been tested in ADHD or other populations particularly vulnerable to the effects of SMT.
Media Multitasking
In their seminal 2009 paper, Ophir et al. examined the relationship between self-reported media multitasking, defined as using several forms of SMT at once, and experimental tasks measuring cognitive control. Paradoxically, participants who multitasked more often seemed to be poorer at it: they were slower to classify a stimulus after a task-switching condition than other participants. Further, the heavy multitasking group performed worse on a working memory task in the presence of distracting, irrelevant stimuli, suggesting that participants’ multitasking behaviors were driven not by an ability to effectively multitask but an inability to attend to a single task when distractions are present [53]. This in turn underscored a possible relationship to inattention, distractibility, and ADHD.
Subsequent results strengthened this interpretation [54], including an fMRI study that connected multitasking behaviors to distractibility and differential activation of brain areas related to attentional control [55]. Multitasking behaviors and preference were found to be associated with symptoms of inattention and hyperactivity-impulsivity [56], making the connection to ADHD explicit, and heavier multitasking has also been linked to poorer achievement test scores [57]. The evidence seemed to point conclusively to an association between simultaneous use of multiple media streams and deficits in attentional and inhibitory control.
However, two recent studies failed to replicate the effects reported by Ophir et al. [58, 59], and recent reviews have drawn attention to conflicting findings [60, 61•]. Other researchers have observed non-monotonic relationships between executive functioning and media multitasking, suggesting that multitasking behaviors should be divided into more than two groups [62, 63]. When interpreting the evidence, it must be noted that technology and media use patterns changed dramatically in the time between Ophir and colleagues’ original study and more recent studies that failed to replicate it. Current SMT facilitates multitasking and encourages it through notifications; therefore, the composition of the heavy multitasking groups may have changed substantially between 2009 and 2018.
Device-based studies of multitasking have found that most participants use a large range of apps (> 50), and a substantial portion of app use is very brief (< 15 s) [64, 65•]; therefore, self-reported measures may not be sufficiently precise or detailed to adequately capture variability in current multitasking behaviors. Moreover, multitasking is heavily impacted by device notifications, discussed in the next section, which frequently elicit app-switching but have little impact on total device use [66]. Further study is needed to explore app-switching behaviors in the context of ADHD.
Although its impacts remain uncertain, several interventions to curb multitasking have been developed. Interventions have focused on awareness of multitasking behaviors, mindfulness, or device restrictions [67], any of which might be implemented using a device-based approach. Although positive effects on attention have been reported [68], a majority of interventions have been brief (i.e., occurring in a single session), and evidence supporting their effectiveness is inconclusive [67].
Digital Disruptions
Although device notifications initiated by e-mail, messaging, and other apps encourage multitasking behaviors [13••, 66], they also represent a distinct, modifiable hazard of SMT use that has been directly connected to symptoms of ADHD.
Disruptions from mobile phones impair performance on attention-related tasks by causing post-disruption commission errors [69], also called “resumption errors” [13••], which can be mitigated by a brief “resumption lag” to recover from the interruption [70]. However, individuals with deficits in attention may be more vulnerable to resumption errors, as they have established deficits in post-error slowing, an adaptive behavior similar to resumption lag that is thought to improve post-error performance [71].
Recently, notifications were directly linked to ADHD-related symptoms in a crossover study of 221 university students, who maximized and minimized notifications, respectively, in two different weeks. Notification levels self-reported at baseline were significantly associated with both inattention (r = 0.30) and hyperactivity (r = 0.31), and maximizing notifications led to a medium-sized increase in both types of symptoms. Perhaps most interestingly, mediation analysis revealed that participants with higher inattention scores reported greater reduction in productivity, environmental mastery, social connectedness, perceived choice, and meaning in life when notifications were maximized [72••].
Moreover, the negative impact of disruptions is not limited to times when they occur, but instead leads to a “checking habit” that persistently undermines productivity [73]. Indeed, the mere presence of a cell phone on a participant’s desk was found to reduce performance on complex cognitive tasks [74]. While the long-term impact is unknown, evidence suggests that individuals with ADHD, particularly those with prominent inattentive symptoms, are unusually sensitive to the negative effects of SMT-related disruptions.
Device-based strategies for managing notifications include “do not disturb” functions as well as e-mail and messaging apps that reduce alerts by filtering low-priority messages. Participants in a “24-h challenge” to eliminate notifications reported that they were more productive during the challenge period but also more anxious and lonely [29]. These negative symptoms may be more extreme in participants with ADHD, who have a greater need for social connection and assurance [75]. However, limiting social media use over a longer, 3-week period reduced loneliness and depression among college students [76], implying that the negative effects observed in the 24-h challenge may be short-lived. This underscores the importance of a longer trial window when exploring notification-related interventions in ADHD populations.
Availability and Addiction
Persistent, compulsive use of SMT—including social media, video games, and the internet—has been connected to impairment and therefore labeled as a form of behavioral addiction. This expanding view of addiction is reflected by the inclusion of gambling addiction in the 5th Edition of the Diagnostic and Statistical Manual [77]. Although SMT can have positive effects, excessive or compulsive use has negative effects on physical and psychosocial health, as observed in gaming addiction [78] and internet addiction [79]. Individuals with ADHD are at greater risk for several addictive behaviors, including smoking and illicit drug use [80], suggesting they may also be at greater risk for SMT-related addictions.
Recent studies have confirmed this hypothesis. In a cross-sectional study of 263 participants with online gaming addiction and 153 controls, the ADHD rating scale was the strongest predictor of gaming addiction among a range of demographic and psychosocial factors [81]. This finding has been reproduced and does not depend on the type of video game [82]. Similarly, ADHD symptoms were the best predictor of social media addiction in a large cross-sectional study of adults [83•] and have been linked to Facebook addiction in adolescents [84]. A moderate association between ADHD and internet addiction has been demonstrated by meta-analysis [85], and the link between addictions and ADHD is stronger than links between distinct forms of addiction [86]. As with other addictive behaviors, therefore, the ADHD phenotype is uniquely predisposed to addictive use of SMT.
Because SMTs have become so pervasive and integrated in daily life, SMT-related addictions may be particularly difficult to overcome. Unlike substance use, abstaining from SMT may not be feasible due to work or social obligations, which often require access to an internet-connected device. With a device always in reach, overcoming SMT addiction might be compared to quitting smoking while holding a lit cigarette, surrounded by smokers. Moreover, current technologies are deliberately designed to maximize engagement through habit-forming “features” such as infinite scroll [87] and intermittent reinforcement schedules known to lead to more persistent behaviors [88].
To understand and combat SMT addiction, we can begin to identify frequent or repetitive use patterns associated with self-reported addiction and impairment [89]. Apps such as Moment [90] and Apple’s Screen Time are beginning to provide such data, and Moment has been used to identify patterns connected to depression and emotion regulation [91]. Development of research-oriented apps such as MyCap [92] may provide greater customization and data granularity needed to rigorously study the relationship between SMT addiction and ADHD.
Media Content
Video programming, games, internet and social media, and a range of other content can be accessed with any smartphone. Some content types have been studied for years (e.g., television programs), whereas others are unique to newer devices (e.g., augmented reality apps). Exposure to specific content, such as fast-paced and violent programming, has long been hypothesized to contribute to the development of ADHD-related symptoms and behaviors. In both cases, the balance of evidence has been inconclusive [12•, 17•], partly due to the ethical and practical limitations of studying the effects of SMT in children [20••].
However, a controlled, blinded study of “excessive sensory stimulation” in juvenile mice demonstrated that learning and memory were decreased, and risk-taking and motor activity were increased, in animals exposed nightly to simulated television viewing compared to control animals [20••]. Further, a recent study of 2- and 3-year old children found that an interactive, tablet-based app improved measures of both hot and cold executive functioning compared to non-interactive educational content, suggesting that interactivity may be a key factor [19]. These results highlight the importance, but also the difficulty, of investigating the effects of specific forms of media content.
With newer technologies, detailed app usage statistics can be used to approximate exposure to specific forms of content, such as social media or video programming [65•]. Given the shift toward mobile devices [3] and other smart technologies, device-based monitoring is an increasingly important alternative to older measures of exposure when studying the effects of media content on individuals with ADHD.
Digital Therapeutics—Beyond Counteracting Negative Effects
Amid concerns about the impact of SMT, a wave of FDA-regulated “digital therapeutics” has also emerged [93]. This new treatment category consists of apps and other software that incorporate evidence-based principles and might be prescribed to treat specific medical or psychiatric conditions following clinical trials. Their development rests on the assumption that SMT effects are not uniformly positive or negative but vary by content type and mode of interaction.
A trial of a digital therapeutic for ADHD, an app designed to improve attentional control and resistance to distractions, has demonstrated differential benefit on working memory and the Test of Variables of Attention (TOVA) among children with ADHD, including a high-severity group, compared to children without [94•]. This app, a game called Project: EVO, was based on an earlier app found to improve cognitive control in older adults [95], and it also appears to be effective in children with co-occurring ADHD and autism spectrum disorder [96]. Other digital therapeutics designed for ADHD include a “Decoder” game that improved visual attention in adult participants compared to a non-app-based control group [97], and a smartglasses intervention that improved ADHD symptoms in a small pilot study of children with autism spectrum disorder [98].
These results, while promising, should be interpreted with a degree of caution. A recent meta-analysis found that video game training has negligible effect on cognition in the general population, and studies have repeatedly demonstrated that learned cognitive skills tend to generalize poorly between domains [99]. Consistent with these general principles, Project: EVO was found to improve performance only in children with ADHD, and not control children with no psychiatric diagnoses [94•]. Continued study is needed to determine whether novel digital therapeutics can complement other device-based interventions to shift the net effects of SMT from negative to positive.
Conclusions
We have proposed a novel paradigm for conceptualizing and studying the effects of SMT despite varied, shifting usage patterns. Our review identified five distinct dimensions of SMT use whose effects might be isolated, for instance by leveraging SMT itself as a study platform. There is evidence that the ADHD phenotype may be unusually sensitive to each of these dimensions, but further study is needed to directly investigate potential effects and motivate interventions. Although some forms of SMT use appear to be hazardous, the emergence of effective digital therapeutics for ADHD implies that others are likely to be beneficial.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Nielsen. Time Flies: U.S. Adults now spend nearly half a day interacting with media [Internet]. neilsen.com. 2018 [cited 2019 Feb 24]. Available from: https://www.nielsen.com/us/en/insights/news/2018/time-flies-us-adults-now-spend-nearly-half-a-day-interacting-with-media.print.html. Accessed 28 Mar 2019.
Wurmser Y. Mobile time spent 2018 [Internet]. eMarketer. 2018 [cited 2019 Mar 17]. Available from: https://www.emarketer.com/content/mobile-time-spent-2018. Accessed 28 Mar 2019.
Khalaf S, Kesiraju L. U.S. Consumers time-spent on mobile crosses 5 hours a day [Internet]. Flurry Anal. Blog. 2017 [cited 2019 Mar 17]. Available from: https://flurrymobile.tumblr.com/post/157921590345/us-consumers-time-spent-on-mobile-crosses-5. Accessed 28 Mar 2019.
Khalaf S. Mobile to Television: We interrupt this broadcast (Again) [Internet]. Flurry Anal. Blog. [cited 2019 Mar 17]. Available from: https://flurrymobile.tumblr.com/post/115194107130/mobile-to-television-we-interrupt-this-broadcast. Accessed 28 Mar 2019.
Gazzaley A. The cognition crisis [Internet]. Medium. 2018 [cited 2019 Mar 17]. Available from: https://medium.com/s/futurehuman/the-cognition-crisis-a1482e889fcb. Accessed 28 Mar 2019.
• Twenge JM, Joiner TE, Rogers ML, Martin GN. Increases in depressive symptoms, suicide-related outcomes, and suicide rates among U.S. adolescents after 2010 and links to increased new media screen time. Clin Psychol Sci. 2018;6:3–17. Based on large, observational data from the United States, this article argues that there is an important connection between growing screen media technology use in adolescents and higher rates of mental health problems, incuding suicide.
• Orben A, Przybylski AK. The association between adolescent well-being and digital technology use. Nat Hum Behav [Internet]. Springer US; 2019;3(2):173. Available from: https://doi.org/10.1038/s41562-018-0506-1. Based on the same U.S. observational datasets as [6] and an additional dataset from the United Kingdom, this article argues that although a negative association between screen media technology and well-being does exist, it is small.
Stiglic N, Viner RM. Effects of screentime on the health and well-being of children and adolescents: a systematic review of reviews. BMJ Open. 2019;9(1):e023191.
Greenfield S. Screen Technologies [Internet]. 2019 [cited 2019 Mar 17]. Available from: http://www.susangreenfield.com/science/detail/screen-technologies/. Accessed 28 Mar 2019.
Visser SN, Danielson ML, Bitsko RH, Holbrook JR, Kogan MD, Ghandour RM, et al. Trends in the parent-report of health care provider-diagnosed and medicated attention-deficit/hyperactivity disorder: United States, 2003–2011. J Am Acad Child Adolesc Psychiatry. 2014;53(1):34–46.
Davidovitch M, Koren G, Fund N, Shrem M, Porath A. Challenges in defining the rates of ADHD diagnosis and treatment: trends over the last decade. BMC Pediatr. 2017;17:1–9.
• Beyens I, Valkenburg PM, Piotrowski JT. Screen media use and ADHD-related behaviors: four decades of research. Proc Natl Acad Sci [Internet]. 2018;115:9875–81 Available from: http://www.pnas.org/lookup/doi/10.1073/pnas.1611611114. Accessed 28 Mar 2019. This article reviews evidence for the effects of specific media content on ADHD and describes possible underlying mechanisms.
•• Wilmer HH, Sherman LE, Chein JM. Smartphones and cognition: a review of research exploring the links between mobile technology habits and cognitive functioning. Front Psychol. 2017;8:1–16. This article comprehensively reviews evidence linking technology use to attention, memory and knowledge, and reward processing. It is an excellent reference on the potential cognitive effects of media multitasking.
•• Ra CK, Cho J, Stone MD, De La Cerda J, Goldenson NI, Moroney E, et al. Association of digital media use with subsequent symptoms of attention-deficit/hyperactivity disorder among adolescents. JAMA - J Am Med Assoc. 2018;320:255–63. This large longitudinal study found that higher self-reported digital media use was associated with increased odds of self-reported inattentive and hyperactive-impulsive symptoms at follow-up.
Montagni I, Guichard E, Kurth T. Association of screen time with self-perceived attention problems and hyperactivity levels in French students: a cross-sectional study. BMJ Open. 2016;6:1–8.
Sibley MH, Coxe SJ. Digital media use and ADHD symptoms. JAMA. 2018;320(24):2599.
• Nikkelen SWC, Valkenburg PM, Huizinga M, Bushman BJ. Media use and ADHD-related behaviors in children and adolescents: a meta-analysis. Dev Psychol. 2014;50:2228–41. This comprehensive meta-analysis demonstrates a significant but small effect of media content on ADHD and highlights conflicting results.
Suchert V, Hanewinkel R, Isensee B. Sedentary behavior and indicators of mental health in school-aged children and adolescents: a systematic review. Prev Med. 2015;76:48–57.
Huber B, Yeates M, Meyer D, Fleckhammer L, Kaufman J. The effects of screen media content on young children’s executive functioning. J Exp Child Psychol [Internet]. 2018;170:72–85 Available from: https://linkinghub.elsevier.com/retrieve/pii/S002209651730646X. Accessed 28 Mar 2019.
•• Christakis DA, Ramirez JSB, Ferguson SM, Ravinder S, Ramirez J-M. How early media exposure may affect cognitive function: a review of results from observations in humans and experiments in mice. Proc Natl Acad Sci [Internet]. 2018;115:9851–8 Available from: http://www.pnas.org/lookup/doi/10.1073/pnas.1711548115. Accessed 28 Mar 2019. This paper emphasizes the limitations of existing research on screen media in children and provides new, compelling evidence for its negative effects using a mouse model of "excessive sensory stimulation".
Thoma VK, Schulz-Zhecheva Y, Oser C, Fleischhaker C, Biscaldi M, Klein C. Media use, sleep quality, and ADHD symptoms in a community sample and a sample of ADHD patients aged 8 to 18 years. J Atten Disord. 2018. https://doi.org/10.1177/1087054718802014
Rey-López JP, Ruiz JR, Ortega FB, Verloigne M, Vicente-Rodriguez G, Gracia-Marco L, et al. Reliability and validity of a screen time-based sedentary behaviour questionnaire for adolescents: the HELENA study. Eur J Pub Health. 2012;22:373–7.
Calamaro CJ, Mason TBA, Ratcliffe SJ. Adolescents living the 24/7 lifestyle: effects of caffeine and technology on sleep duration and daytime functioning. Pediatr Int. 2009;123:e1005–10 Available from: http://journals.rcni.com/doi/10.7748/phc.20.3.14.s23. Accessed 28 Mar 2019.
• Becker SP, Lienesch JA. Night time media use in adolescents with ADHD: links to sleep problems and internalizing symptoms. Sleep Med. 2018;51:171–8. This study demonstrates the negative impact of nighttime screen media technology use on sleep as well as self-reported anxiety and depression in adolescents with ADHD.
Lissak G. Adverse physiological and psychological effects of screen time on children and adolescents: literature review and case study. Environ Res. Elsevier Inc. 2018;164:149–57.
Swing EL, Gentile DA, Anderson CA, Walsh DA. Television and video game exposure and the development of attention problems. Pediatrics. 2010;126:214–21.
Engelhardt CR, Mazurek MO, Sohl K. Media use and sleep among boys with autism spectrum disorder, ADHD, or typical development. Pediatrics. 2013;132:1081–9.
Radesky J. Digital media and symptoms of attention-deficit/hyperactivity disorder in adolescents. JAMA. 2018;320(3):237–9.
Pielot M, Rello L. Productive, anxious, lonely: 24 hours without push notifications. In Proceedings of the 19th International Conference on Human-Computer Interaction with Mobile Devices and Services. 2017 (p. 11). ACM.
Andersen RE, Crespo CJ, Bartlett SJ, Cheskin LJ, Pratt M. Relationship of physical activity and television watching with body weight and level of fatness among children: results from the Third National Health and Nutrition Examination Survey. JAMA. 1998;279(12):938–42.
Lepp A, Barkley JE, Sanders GJ, Rebold M, Gates P The relationship between cell phone use, physical and sedentary activity, and cardiorespiratory fitness in a sample of U.S. college students. Int J Behav Nutr Phys Act. 2013;10(1):79.
Berwid OG, Halperin JM. Emerging support for a role of exercise in attention-deficit/hyperactivity disorder intervention planning. Curr Psychiatry Rep. 2012;14(5):543–51.
Montag C, Diefenbach S, Montag C, Diefenbach S. Towards homo digitalis: important research issues for psychology and the neurosciences at the dawn of the Internet of Things and the digital society. Sustainability. 2018;10(2):415.
Kumar S, Nilsen WJ, Abernethy A, Atienza A, Patrick K, Pavel M, et al. Mobile health technology evaluation: the mHealth evidence workshop. Am J Prev Med [Internet]. 2013;45:228–36. Available from: http://www.ncbi.nlm.nih.gov/pubmed/23867031. Accessed 28 Mar 2019.
Sheppard AL, Wolffsohn JS. Digital eye strain: prevalence, measurement and amelioration. BMJ Open Ophthalmol. 2018;3:e000146.
Wilkins A, Veitch J, Lehman B. LED lighting flicker and potential health concerns: IEEE standard PAR1789 update. In 2010 IEEE Energy Conversion Congress and Exposition. 2010 (pp. 171–178). IEEE.
Inger R, Bennie J, Davies TW, Gaston KJ. Potential biological and ecological effects of flickering artificial light. PLoS One. 2014;9:e98631.
Mclntyre IM, Norman TR, Burrows GD, Armstrong SM. Human melatonin suppression by light is intensity dependent. J Pineal Res. 1989;6:149–56.
Souman JL, Tinga AM, te Pas SF, van Ee R, Vlaskamp BNS. Acute alerting effects of light: a systematic literature review. Behav Brain Res [Internet]. 2018;337:228–39 Available from: https://linkinghub.elsevier.com/retrieve/pii/S0166432817311002. Accessed 28 Mar 2019.
Chang A-M, Aeschbach D, Duffy JF, Czeisler CA. Evening use of light-emitting eReaders negatively affects sleep, circadian timing, and next-morning alertness. Proc Natl Acad Sci. 2014;112:1232–7.
Tosini G, Ferguson I, Tsubota K. Effects of blue light on the circadian system and eye physiology. Mol Vis [Internet]. 2016;22:61–72 Available from: http://www.ncbi.nlm.nih.gov/pubmed/26900325. Accessed 28 Mar 2019.
Chellappa SL, Steiner R, Blattner P, Oelhafen P, Götz T, Cajochen C. Non-visual effects of light on melatonin, alertness and cognitive performance: can blue-enriched light keep us alert? PloS One. 2011;6(1):e16429.
Studer P, Brucker JM, Haag C, Van Doren J, Moll GH, Heinrich H, et al. Effects of blue- and red-enriched light on attention and sleep in typically developing adolescents. Physiol Behav. 2019;199:11–9.
Lunsford-Avery JR, Krystal AD, Kollins SH. Sleep disturbances in adolescents with ADHD: a systematic review and framework for future research. Clin Psychol Rev. 2016;50:159–74.
Crowley SJ, Cain SW, Burns AC, Acebo C, Carskadon MA. Increased sensitivity of the circadian system to light in early/mid-puberty. J Clin Endocrinol Metab. 2015;100:4067–73.
f.lux: software to make your life better [Internet]. [cited 2019 Mar 17]. Available from: https://justgetflux.com/. Accessed 28 Mar 2019.
Rahman SA, Hilaire MA, Lockley SW. The effects of spectral tuning of evening ambient light on melatonin suppression, alertness and sleep. Physiol Behav. 2017;177:221–9.
Heo JY, Kim K, Fava M, Mischoulon D, Papakostas GI, Kim MJ, et al. Effects of smartphone use with and without blue light at night in healthy adults: a randomized, double-blind, cross-over, placebo-controlled comparison. J Psychiatr Res. 2017;87:61–70.
Nagare R, Plitnick B, Figueiro MG. Does the iPad Night Shift mode reduce melatonin suppression? Light Res Technol. 2019;51(3):373–83.
Heath M, Sutherland C, Bartel K, Gradisar M, Williamson P, Lovato N, et al. Does one hour of bright or short-wavelength filtered tablet screenlight have a meaningful effect on adolescents’ pre-bedtime alertness, sleep, and daytime functioning? Chronobiol Int [Internet]. 2014;31:496–505 Available from: http://www.tandfonline.com/doi/full/10.3109/07420528.2013.872121. Accessed 28 Mar 2019.
Ayaki M, Yoshimura M, Nakano M, Maruyama Y, Negishi K, Tsubota K, et al. Protective effect of blue-light shield eyewear for adults against light pollution from self-luminous devices used at night. Chronobiol Int [Internet] Informa Healthcare. 2016;33:134–9. Available from. https://doi.org/10.3109/07420528.2015.1119158.
Bowler J, Bourke P. Facebook use and sleep quality: light interacts with socially induced alert. Br J Psychol. 2018;1–11. https://doi.org/10.1111/bjop.
Ophir E, Nass C, Wagner AD. Cognitive control in media multitaskers. Proc Natl Acad Sci [Internet]. 2009;106:15583–7 Available from: https://www.scientific.net/MSF.836-837.220. Accessed 28 Mar 2019.
Baumgartner SE, Weeda WD, van der Heijden LL, Huizinga M. The relationship between media multitasking and executive function in early adolescents. J Early Adolesc. 2014;34:1120–44.
Moisala M, Salmela V, Hietajärvi L, Salo E, Carlson S, Salonen O, et al. Media multitasking is associated with distractibility and increased prefrontal activity in adolescents and young adults. Neuroimage [Internet]. Elsevier Inc. 2016;134:113–21. https://doi.org/10.1016/j.neuroimage.2016.04.011.
Magen H. The relations between executive functions, media multitasking and polychronicity. Comput Human Behav [Internet] Elsevier Ltd. 2017;67:1–9. https://doi.org/10.1016/j.chb.2016.10.011.
Cain MS, Leonard JA, Gabrieli JDE, Finn AS. Media multitasking in adolescence. Psychon Bull Rev [Internet]. 2016;23:1932–41. Available from. https://doi.org/10.3758/s13423-016-1036-3.
Wiradhany W, Nieuwenstein MR. Cognitive control in media multitaskers: two replication studies and a meta-analysis. Attention Perception Psychophys. 2017;79:2620–41.
Seddon AL, Law AS, Adams AM, Simmons FR. Exploring the relationship between executive functions and self-reported media-multitasking in young adults. J Cogn Psychol. Taylor & Francis. 2018;30:728–42.
Van Der Schuur WA, Baumgartner SE, Sumter SR, Valkenburg PM. The consequences of media multitasking for youth: a review. Comput Human Behav [Internet] Elsevier Ltd. 2015;53:204–15. https://doi.org/10.1016/j.chb.2015.06.035.
• Uncapher MR, Wagner AD. Minds and brains of media multitaskers: current findings and future directions. Proc Natl Acad Sci. 2018;115:9889–96. This article comprehensively reviews evidence regarding the impact of media multitasking on cognitive functioning, from the original results of Ophir et al. [53] to more recent, conflicting findings.
Murphy K, McLauchlan S, Lee M. Is there a link between media-multitasking and the executive functions of filtering and response inhibition? Comput Human Behav [Internet]. Elsevier Ltd. 2017;75:667–77. https://doi.org/10.1016/j.chb.2017.06.001.
Cardoso-Leite P, Kludt R, Vignola G, Ma WJ, Green CS, Bavelier D. Technology consumption and cognitive control: contrasting action video game experience with media multitasking. Attention Perception Psychophys. 2016;78:218–41.
Ferreira D, Goncalves J, Kostakos V, Barkhuus L, Dey AK. Contextual experience sampling of mobile application micro-usage. In Proceedings of the 16th international conference on Human-computer interaction with mobile devices & services 2014 Sep23 (pp. 91–100). ACM.
• Morrison A, Xiong X, Higgs M, Bell M, Chalmers M. A Large-scale study of iPhone App launch behaviour. In Proceedings of the 2018 CHI Conference on Human Factors in Computing Systems 2018 Apr 21 (p. 344). ACM. This study provides detailed information on the app usage patterns of a large cohort of iPhone users, illustrating how device-based study designs can be used to precisely quantify screen media technology use, including in ADHD.
Sahami Shirazi A, Henze N, Dingler T, Pielot M, Weber D, Schmidt A. Large-scale assessment of mobile notifications. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems 2014 Apr 26 (pp. 3055–3064). ACM.
Parry DA, le Roux DB. Media multitasking and cognitive control: a systematic review of interventions. Comput Human Behav [Internet]. Elsevier. 2019;92:316–27. https://doi.org/10.1016/j.chb.2018.11.031.
Gorman TE, Green CS. Short-term mindfulness intervention reduces the negative attentional effects associated with heavy media multitasking. Sci Rep [Internet]. Nature Publishing Group. 2016;6:1–7. https://doi.org/10.1038/srep24542.
Stothart C, Mitchum A, Yehnert C. Journal of Experimental Psychology: human perception and performance the attentional cost of receiving a cell phone notification the attentional cost of receiving a cell phone notification. J Exp Psychol Hum Percept [Internet]. 2015;41:893–7. Available from. https://doi.org/10.1037/xhp0000100.
Brumby DP, Cox AL, Back J, Gould SJJ. Recovering from an interruption: investigating speed-accuracy trade-offs in task resumption behavior. J Exp Psychol Appl. 2013;19:95–107.
Shiels K, Tamm L, Epstein JN. Deficient post-error slowing in children with ADHD is limited to the inattentive subtype. J Int Neuropsychol Soc. 2012;18:612–7.
•• Kushlev K, Proulx J, Dunn EW. “Silence your phones”: smartphone notifications increase inattention and hyperactivity symptoms. In: Proc 2016 CHI Conf Hum Factors Comput Syst [Internet]. New York: ACM Press; 2016. p. 1011–20. [cited 2018 Mar 22];. Available from: http://dl.acm.org/citation.cfm?doid=2858036.2858359 Accessed 28 Mar 2019. This important study demonstrated not only that device notifications are associated with symptoms of ADHD, but also that those with higher ADHD symptoms are more negatively affected by the negative impacts of notifications, including on productivity.
Duke É, Montag C. Smartphone addiction, daily interruptions and self-reported productivity. Addict Behav Reports [Internet]. Elsevier. 2017;6:90–5. https://doi.org/10.1016/j.abrep.2017.07.002.
Thornton B, Faires A, Robbins M, Rollins E. The mere presence of a cell phone may be distracting implications for attention and task performance. Soc Psychol (Gott). 2014;45:479–88.
Kim JH. Psychological issues and problematic use of smartphone: ADHD’s moderating role in the associations among loneliness, need for social assurance, need for immediate connection, and problematic use of smartphone. Comput Human Behav [Internet]. Elsevier Ltd. 2018;80:390–8. https://doi.org/10.1016/j.chb.2017.11.025.
Hunt MG, Marx R, Lipson C, Young J. No more FOMO: limiting social media decreases loneliness and depression. J Soc Clin Psychol. 2018;37:751–68.
Potenza MN. Non-substance addictive behaviors in the context of DSM-5. Addict Behav [Internet]. 2014;39:1–2 Available from: https://linkinghub.elsevier.com/retrieve/pii/S0306460313002633. Accessed 28 Mar 2019.
Stavropoulos V, Adams BLM, Beard CL, Dumble E, Trawley S, Gomez R, et al. Associations between attention deficit hyperactivity and internet gaming disorder symptoms: is there consistency across types of symptoms, gender and countries? Addict Behav Reports [Internet]. Elsevier. 2019;9:100158. https://doi.org/10.1016/j.abrep.2018.100158.
Kuss DJ, Griffiths MD. Online social networking and addiction-a review of the psychological literature. Int J Environ Res Public Health. 2011;8:3528–52.
Lee SS, Humphreys KL, Flory K, Liu R, Glass K. Prospective association of childhood attention-deficit/hyperactivity disorder (ADHD) and substance use and abuse/dependence: a meta-analytic review. Clin Psychol Rev [Internet] Elsevier Ltd. 2011;31:328–41. https://doi.org/10.1016/j.cpr.2011.01.006.
Han DH, Chung U-S, Hyun GJ, Lee YS, Renshaw PF, Kang KD, et al. Risk factors associated with online game addiction: a hierarchical model. Comput Human Behav [Internet]. Elsevier Ltd. 2015;48:706–13. https://doi.org/10.1016/j.chb.2015.02.008.
Mathews CL, Morrell HE, Molle JE. Video game addiction, ADHD symptomatology, and video game reinforcement. Am J Drug Alcohol Abuse. 2019;45(1):67–76.
• Andreassen CS, Billieux J, Griffiths MD, Kuss DJ, Demetrovics Z, Mazzoni E, et al. The relationship between addictive use of social media and video games and symptoms of psychiatric disorders: a large-scale cross-sectional study. Psychol Addict Behav [Internet]. 2016;30:252–62 Available from: http://doi.apa.org/getdoi.cfm?doi=10.1037/adb0000160. Accessed 28 Mar 2019. In this large, cross-sectional study, ADHD symptoms were found to be the strongest predictor of social media addiction.
Settanni M, Marengo D, Fabris MA, Longobardi C. The interplay between ADHD symptoms and time perspective in addictive social media use: a study on adolescent Facebook users. Child Youth Serv Rev [Internet]. Elsevier. 2018;89:165–70. https://doi.org/10.1016/j.childyouth.2018.04.031.
Wang B-Q, Yao N-Q, Zhou X, Liu J, Lv ZT. The association between attention deficit/hyperactivity disorder and internet addiction: a systematic review and meta-analysis. BMC Psychiatry BMC Psychiatry. 2017;17:1–12.
Metin O, Saracli O, Atasoy N, Senormanci O, Cakir Kardes V, Ozan Acikgoz H, et al. Association of internet addiction in high school students with ADHD and tobacco/alcohol use. Dusunen Adam J Psychiatry Neurol Sci [Internet]. 2015;28:204–12 Available from: http://www.dusunenadamdergisi.org/ing/Articledetails.aspx?MkID=1069. Accessed 28 Mar 2019.
Andersson H Social media apps are “deliberately” addictive to users. BBC News [Internet]. 2018 Jul 4 [cited 2019 Mar 17]; Available from: https://www.bbc.com/news/technology-44640959. Accessed 28 Mar 2019.
Horsley RR, Osborne M, Norman C, Wells T. High-frequency gamblers show increased resistance to extinction following partial reinforcement. Behav Brain Res [Internet]. Elsevier B.V. 2012;229:438–42. https://doi.org/10.1016/j.bbr.2012.01.024.
Liu CH, Lin SH, Pan YC, Lin YH. Smartphone gaming and frequent use pattern associated with smartphone addiction. Med (United States). 2016;95:1–4.
Moment – Less phone. More life. [Internet]. [cited 2019 Mar 17]. Available from: https://inthemoment.io/. Accessed 28 Mar 2019.
Elhai JD, Tiamiyu MF, Weeks JW, Levine JC, Picard KJ, Hall BJ. Depression and emotion regulation predict objective smartphone use measured over one week. Pers Individ Dif [Internet]. Elsevier Ltd. 2018;133:21–8. https://doi.org/10.1016/j.paid.2017.04.051.
MyCap [Internet]. [cited 2019 Mar 17]. Available from: https://projectmycap.org/. Accessed 28 Mar 2019.
Waltz E. Pear approval signals FDA readiness for digital treatments. Nat Biotechnol [Internet]. Nature Publishing Group. 2018;36:481–2. https://doi.org/10.1038/nbt0618-481.
• Davis NO, Bower J, Kollins SH. Proof-of-concept study of an at-home, engaging, digital intervention for pediatric ADHD. PLoS One. 2018;13:1–19. This study demonstrated benefits of a digital therapeutic video game on working memory and the Test of Variables of Attention (TOVA) in children with ADHD, suggesting that specific forms of screen media technology use can have positive effects.
Anguera JA, Boccanfuso J, Rintoul JL, Al-Hashimi O, Faraji F, Janowich J, et al. Video game training enhances cognitive control in older adults. Nature [Internet]. Nature Publishing Group. 2013;501:97–101. https://doi.org/10.1038/nature12486.
Yerys BE, Bertollo JR, Kenworthy L, Dawson G, Marco EJ, Schultz RT, et al. Brief report: pilot study of a novel interactive digital treatment to improve cognitive control in children with autism spectrum disorder and co-occurring ADHD symptoms. J Autism Dev Disord. 2019;49(4):1727–37.
Savulich G, Thorp E, Piercy T, Peterson KA, Pickard JD, Sahakian BJ. Improvements in attention following cognitive training with the novel “decoder” game on an iPad. Front Behav Neurosci [Internet]. 2019;13:1–8 Available from: https://www.frontiersin.org/article/10.3389/fnbeh.2019.00002/full. Accessed 28 Mar 2019.
Vahabzadeh A, Keshav NU, Salisbury JP, Sahin NT. Improvement of attention-deficit/hyperactivity disorder symptoms in school-aged children, adolescents, and young adults with autism via a digital smartglasses-based socioemotional coaching aid: short-term, uncontrolled pilot study. J Med Internet Res. 2018;20:1–13.
Sala G, Tatlidil KS, Gobet F. Video game training does not enhance cognitive ability: a comprehensive meta-analytic investigation. Psychol Bull [Internet]. 2018;144:111–39 Available from: http://doi.apa.org/getdoi.cfm?doi=10.1037/bul0000139. Accessed 28 Mar 2019.
Funding
This work was partly supported by the C. Keith Conners Fellowship in Digital Health founded by a donation from Multi-Health Systems, Inc.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Matthew M. Engelhard declares no potential conflicts of interest.
Scott H. Kollins reports grants and personal fees from Akili Interactive, Arbor Pharmaceuticals, Bose, Otsuka Pharmaceuticals, Rhodes, Shire Pharmaceuticals, and Tris Pharmaceuticals.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Attention-Deficit Disorder
Rights and permissions
About this article

Cite this article
Engelhard, M.M., Kollins, S.H. The Many Channels of Screen Media Technology in ADHD: a Paradigm for Quantifying Distinct Risks and Potential Benefits. Curr Psychiatry Rep 21, 90 (2019). https://doi.org/10.1007/s11920-019-1077-1
Published:
DOI: https://doi.org/10.1007/s11920-019-1077-1