
Abstract
Purpose of Review
Chronic headache sufferers are estimated to be around 3% of the population. These patients have a high disease burden. When prophylactic treatments have low efficacy and tolerability, patients are in need of alternative therapeutic strategies and options.
Recent Findings
In the last decade, a number of neuromodulation procedures have been introduced as treatment of chronic intractable headache patients when pharmacological treatments fail or are not well tolerated. Neurostimulation of peripheral and central nervous system has been carried out, and now, various non-invasive and invasive stimulation devices are available. Non-invasive neurostimulation options include vagus nerve stimulation, supraorbital stimulation and single-pulse transcranial magnetic stimulation; invasive procedures include occipital nerve stimulation, sphenopalatine ganglion stimulation and hypothalamic deep brain stimulation. In many cases, results supporting their use derive from open-label series and small controlled trial studies. Lack of adequate placebo hampers adequate randomized controlled trials.
Summary
In this paper, we give an overview on the main neurostimulation procedures in terms of results and putative mechanism of cation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Headaches with a chronic course affect about 3% of the population [1]. In the majority of cases, patients with chronic headache referred to specialized headache centres suffer from chronic migraine or cluster headache [2].
Medical treatments improve these conditions in a large proportion of these patients, but still, a minority is refractory to or cannot tolerate pharmacological treatments.
In the last decade, a number of neuromodulation procedures have been employed in the attempt to improve chronic headache patients when pharmacological treatments fail [3]. Both peripheral and central neural structures have been targeted [4]. This paper offers an overview of main neurostimulation procedures employed to treat intractable chronic headaches.
Neuromodulation has the potential to modulate central and/or peripheral pain pathways using electrical or magnetic impulses and is aimed to produce changes in the pain system so to reduce pain levels. Targets for neurostimulation in headache currently include non-invasive stimulation as vagus nerve stimulation, superficial cortical stimulation produced by transcranial magnetic stimulation, supraorbital nerve stimulation and more invasive stimulation procedures as occipital nerve stimulation (ONS), sphenopalatine ganglion (SPG) stimulation and posterior hypothalamus stimulation (Table 1). All of these procedures have the potential to modulate brain phenomena thought to be responsible for attack generation, i.e. cortical spreading depression or brainstem activation (Fig. 1).

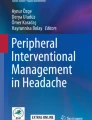
Anatomy of head pain and autonomic phenomena in neurovascular headaches: trigeminal autonomic cephalalgias (TACs) and migraine. The pain in neurovascular headaches is likely to come from activation of the trigeminovascular system while autonomic craniofacial phenomena (mainly in TACs) are from parasympathetic activation. Contemporary activation of trigeminovascular and cranial parasympathetic systems are thought to be part of a brainstem reflex, the trigemino-parasympathetic reflex. A number of brain structures are probably involved in the modulation of trigemino-parasympathetic reflex. Abbreviations: TG trigeminal ganglion, TCC trigeminocervical complex, SPG sphenopalatine ganglion; Hypothalamic nuclei: PH posterior, SON supra-optic, VMH ventromedial, PVN paraventricular hypothalamic nuclei, LH lateral, DMH dorsomedial, PON pre-optic, PAG periaqueductal grey, LC locus coeruleus, NRM nucleus raphe magnus. Ascending nociceptive signals, from to the TCC to higher brain structures (light blue neurons). Reflex connection from the TCC, via the superior salivatory nucleus (SuS), provides an autonomic projection to the cranial vasculature (grey neurons). Greater petrosal nerve (green neuron). The facial (seventh cranial) nerve (purple neuron). Descending projections from PH, PVN and LH thought to modulate trigeminovascular nociceptive transmission in the TCC (red neurons). Descending projections to the SuS (orange neurons). Modified with permission from: Akerman S and Goadsby PJ, Headache 2015 Jan;55(1):197–203
Non-invasive Neurostimulation
Vagus Nerve Stimulation
The vagus nerve is a mixed motor and sensory nerve crucial for a number of vital functions. Its projections include brain centres involved in pain regulation. The vagus nerve brings important information to the trigeminal nucleus caudalis (TNC) involved in head pain modulation, and it was initially suggested that vagus nerve stimulation (VNS) could directly inhibit nociceptive information there [5] (Fig. 1). This effect could be the consequence of reduced concentration of glutamate in the TNC produced by VNS, and reduced concentration of glutamate in the TNC might reverse central sensitisation in chronic headaches favouring clinical improvement [6]. The vagus nerve in the neck conveys visceral information to various brain areas involved in migraine pathophysiology in addition to TNC. In neuroimaging studies, chronic VNS inhibited activity in the thalamus, the locus coeruleus, the nucleus tractus solitarius, the dorsal pons and the limbic system [7]. VNS also induced a delay in the establishment of visual habituation [8] further suggesting its use to restore the dysfunctional visual cortex in migraine [9].
Transcutaneous vagus nerve stimulation can be applied to the neck thanks to a handheld device, the gammaCore.
Migraine
Acute treatment of migraine with gammaCore has been tried: in one open-label study, 80 attacks of 27 migraine patients were treated: 22% of moderate-to-severe attacks were pain free 2 h after treatment [10].
In a controlled study performed on 59 patients, gammaCore was investigated as preventative treatment for chronic migraine. After 2 months, active treatment did not produce significant reduction of headache days: −1.9 days with gammaCore vs 0.20 sham (p = 0.124) [11]. Ongoing open-label experience suggests better performance of gammaCore, but further controlled studies are needed.
Cluster Headache
In a prospective, open-label, randomised study including 97 patients VNS as adjunctive prophylactic was compared to with standard of care (SoC) [12]. A 2-week baseline phase was followed by a 4-week randomized phase (SoC plus non-invasive VNS (nVNS) vs control) and a 4-week extension phase (SoC plus nVNS). The primary end point was the reduction in the mean number of cluster headache (CH) attacks per week. Significantly higher ≥50% response rates were observed with SoC plus nVNS (40%) vs controls (8.3%). No serious adverse events were observed.
An open-label study on 19 CH patients showed that the device, used as acute treatment, reduced attacks duration in 47% of cases: 11 vs 75 min (mean duration before using gammaCore) [13].
Even if evidence for using gammaCore as an acute treatment in CH needs further investigation, it might be considered for patients suffering multiple CH attacks daily, when there are contraindications to triptans or acute therapies for CH do not produce improvement.
Adverse effects are mild and usually transient including hoarseness and voice change, irritation of skin, muscle discomfort and paraesthesia.
Transcranial Magnetic Stimulation
Migraine aura is attributed to cortical spreading depression (CSD) that is a wave of depolarisation of neural membranes originating from a hyperexcitable cortex of and activation of meningeal nociceptors [10]. CSD is also able to induce activation in the trigeminal system [14]. In addition, an abnormal cortical processing is observed in migraine between attacks characterized by a normal-to-low amplitude response to stimuli, followed by potentiation, i.e. an amplitude increase during prolonged stimulation, while the opposite, habituation, i.e. amplitude decrease, is observed in normal subjects [9]. Taken together, these information indicate that brain cortical activity is a potential target for migraine treatment. Transcranial magnetic stimulation (TMS) and transcranial direct current stimulation (tDCS) have the ability to modulate the underlying cerebral cortex. The principle behind transcranial magnetic stimulation is that a brief single magnetic pulse to the scalp produces electrical fields in the underlying cortex thought to provoke neurotransmitter release capable to interfere with CSD as well with other migraine-related cortical phenomena leading a hyperexcitable cortex [14]. It has been shown that single-pulse transcranial magnetic stimulation inhibits cortical spreading depression [15]. Hence, single-pulse transcranial magnetic stimulation could both terminate the aura phase and reduce the headache while repetitive transcranial magnetic stimulation may reduce cortical neuronal excitability, reverse central sensitisation and improve headache frequency (Fig. 1).
A rechargeable handheld device, the SpringTMS device, delivers a single pulse of magnetic stimulation to the occipital regions of the head and has been tested as treatment in migraine.
Acute Treatment of Migraine With and Without Aura
Single-pulse transcranial magnetic stimulation has been tried as acute treatment of migraine with aura in a randomised, double-blind, parallel-group, sham-controlled trial in 164 patients. Patients reported a pain-free response rate significantly higher in those with active vs sham treatment at both 2 h (39 vs 22%) and 24 h (29 vs 16%) [16].
In an open-label postmarketing survey, data on 190 out of 426 migraine with and without aura patients were obtained after a 3-month follow-up using SpringTMS as acute treatment [17]. Sixty-two percent reported some reduction in migraine pain and 59% some reduction in attack duration.
Preventative Treatment of Migraine and Cluster Headache
Unfortunately, no controlled study supports the use of SpringTMS in the migraine or cluster headache prevention.
In general, the limited evidence available suggest using SpringTMS as acute treatment of migraine with and without aura in patients overusing acute medications or when acute drugs do not work.
Supraorbital Nerve Stimulation
The supraorbital nerve is a branch of the first division of the trigeminal nerve and its stimulation has the potential to interfere with the trigeminal pain pathway and to inhibit activated trigeminovascular system (Fig. 1). Nociceptive fibres coming from the somatic portion of the ophthalmic nerve and Aδ and C fibres of the trigeminovascular system from meninges thought to be responsible for migraine pain converge onto the trigeminal nucleus caudalis (TNC). The convergence of somatic and visceral stimuli in the TNC suggests the therapeutic potential that the neuromodulation of somatic branches of the ophthalmic division of the trigeminal nerve may have on trigeminal nociceptors in the TNC and on migraine pain mechanisms.
An external transcutaneous supraorbital nerve stimulator, the Cefaly device, has been developed for headache treatment. In a pilot study on 10 migraine patients, the device employed for acute migraine treatment produced pain freedom in only 13% of attacks [18]. In a manufacturer-sponsored sham-controlled trial, including 67 subjects with episodic migraine, the Cefaly device has been tested as preventive treatment. After a 1-month run-in period, the Cefaly or sham device was used for 3 months. Migraine days were reduced by 29.7% (from 6.94 to 4.88 days; p = 0.023) in the active group, while in the sham group, the reduction was 4.9% (from 6.54 to 6.22 days) [19]. Some patients reported paraesthesia, worsening of pre-existing headache, and drowsiness, but generally, the adverse events reported using the Cefaly device appear mild and transient [20].
The exact mechanism of action of supraorbital nerve stimulation in migraine is not unknown. Supraorbital nerve stimulation produced sedative effect in healthy volunteers [21] suggesting this stimulation has the potential to interfere with central nervous system activity. Supraorbital nerve stimulation could modify activation threshold within the trigeminovascular system both peripherally and centrally by winding down the trigeminal pain pathway.
Invasive Neurostimulation
Occipital Nerve Stimulation
The occipital nerves are a target for neuromodulation due to the anatomical overlap between the trigeminal and cervical afferents in the trigeminocervical complex (TCC). As for the anatomy of nociceptive trigeminal fibres from ophthalmic nerve branches, painful information from cervical territories are conveyed to second order neurons of the TCC [22] (Fig. 1). The TCC is a relay system for head and cervical pain travelling to higher brain centres as thalamus, hypothalamus and pain matrix areas. ONS could act by modulating antinociceptive activity in the TCC and then remodelling neural activity in brain areas of the pain matrix [22] (Fig. 1). In chronic cluster headache, patients receiving occipital nerve stimulation fluorodeoxyglucose positron emission tomography imaging showed normalised metabolism in several areas of the pain matrix after neurostimulation [23] while the ipsilateral posterior hypothalamus, the so-called cluster generator, continued to maintain hyperactive. Patients undergoing occipital nerve stimulation for chronic migraine showed a similar pattern that is pain relief but persistent hyperactivity of the dorsalrostral pons, the so-called migraine generator [24]. Taken together, these findings suggest that occipital nerve stimulation may act via a non-specific modulation on descending pain control systems enhancing activity of antinociceptive pathways instead of acting on headache generators.
A certain efficacy in the prevention of chronic migraine and trigeminal autonomic cephalalgias (TACs-chronic cluster headache, hemicrania continua and short-lasting unilateral neuralgiform headache attacks) has been demonstrated [3]. As a whole, patients suffering from chronic cluster headache have a response rate of about 60–70% [3, 25] and less than 50% for chronic migraine [26•].
Long-term ONS efficacy has been evaluated only in open-label studies.
Migraine
ONS efficacy in the prophylaxis of chronic migraine has been investigated in randomized controlled trials with conflicting results. Pooled data from a recent meta-analysis study conducted on three separate randomized controlled trials (RCTs) on ONS efficacy showed that ONS was associated with a mean reduction of 2.59 migraine days per month after 3 months compared with sham controls [26•].
In a randomised-controlled study on 61 subjects adjustable stimulation (28 patients), preset stimulation (16 patients) and medical management (17 patients) were compared [27]. Responders (a 50% reduction in monthly headache days or a less than three-point reduction in pain scores) rate 39% in the adjustable group, 6% in the preset group and 0% in the medical group.
In another randomized study, active stimulation was compared to sham stimulation in a population of 125 chronic migraine patients but, after 3 months, no difference was observed [28].
The largest RCT exploring ONS efficacy in chronic migraine was performed on 157 patients [29]. The active harm showed a significantly higher reduction of headache days vs the sham group (27 vs 15%). Similarly, the percentage of patients with at least a 30% reduction of headache pain scores was higher in the active group (38 vs 19%). However, when comparing the percentage of subjects achieving a >50% reduction in daily pain scores, there was no difference in the two groups (17 vs 14%); in chronic pain, a 30% improvement is considered a clinically relevant achievement.
Chronic Cluster Headache
There is only one ongoing controlled trials investigating ONS efficacy in chronic cluster headache. A number of open-label studies with long-term follow-up seem to support ONS efficacy. Data from 126 ONS treated patients from ten studies shows an average efficacy 67% reduction of attack frequency [3, 25].
Guidelines from the European Headache Society indicated when to propose the use of invasive neurostimulation procedures including ONS [28]. In general, ONS must be used in patients suffering highly medically refractory cluster headaches who have not responded to all other treatments. The same applies also to other invasive neurostimulation procedures [30••]. Less clear is its indication to treat intractable chronic migraine. A multidisciplinary team specialized in headache has to properly follow the patients before considering any kind of surgery. Special consideration has to be paid before implanting ONS in patients that may require future MRI scanning as multiple sclerosis and other brain conditions because implanted patients cannot have MRI scans.
Occipital nerve stimulation has no indication as treatment for acute migraine or cluster headache [30••].
Sphenopalatine Ganglion Stimulation
The sphenopalatine ganglion (SPG) lies in the pterygopalatine fossa and contains sympathetic and parasympathetic neurons as well as sensory neurons from the second trigeminal branch. Its nervous structures are connected with systems involved in neurovascular headache pathophysiology as the trigeminal system (responsible of head pain) and the superior salivatory nucleus (SSN) (responsible of cranial parasympathetic phenomena) [31] particularly in cluster headache [31] (Fig. 1). The parasympathetic fibres from the SPG innervate vessels and mucous membranes of the face and paranasal sinuses as well as meningeal vessels and release neurotransmitters activating trigeminal nociceptors that in turn send pain impulses to second-order neurons in the TNC (Fig. 1). TNC and SSN are connected in the brainstem, and this circuit is responsible of the contemporary appearance of pain and cranial autonomic phenomena: the trigemino-parasympathetic reflex [32]. Recent studies have shown that certain SPG stimulation pattern can improve acute CH [33] while other patterns of stimulation can trigger CH attacks [34] thus confirming the relevance of SPG in the pathophysiology of neurovascular headaches and prompting new studies with this procedure.
Chronic Cluster Headache
In a multicentre trial on 28 patients using implanted SPG stimulator, the active group showed a significantly higher number of improved cluster attacks at 15 min (67% active vs 7% sham) [33].
In a subsequent study, 33 patients were enrolled in a 24-month open-label follow-up study. A total of 5956 attacks (180.5 ± 344.8, range 2–1581 per patient) were evaluated: 45% (n = 15) of patients were acute responders (acute effectiveness in ≥50% of attacks) [35]. A ≥50% reduction in attack frequency vs baseline was observed in 33% (n = 11) of patients.
An expert consensus [36] suggested that SPG neurostimulation can be considered as an acute treatment in strictly unilateral CH patients and should be implanted when all available medical treatments have failed. Its efficacy as prophylaxis needs a more in-depth investigation.
Hypothalamic Deep Brain Stimulation
Activation of the posterior hypothalamic area has been reported during cluster headache attacks as well as other TACs [37,38,39]. It was thought that activation there could be inhibited by high-frequency stimulation of that area applying the same principle used to treat tremor in Parkinson’s disease [40].
The first stimulation of this brain area was performed in 2001 on cluster headache patients [41]. So far, the procedure has been conducted in more than 90 chronic cluster headache patients with an overall response rate of about 66% [42, 43].
There has been discussion on how to name the activated brain area in CH patients [44], and a recent paper argued that the site of implantation is the ventral tegmental area rather than the posterior hypothalamus [43].
Selection criteria for deep brain stimulation (DBS) have been published [28]. The procedure must be reserved to severe intractable chronic CH not responding also to less invasive procedure as ONS and has to be performed in highly specialized centres with a multidisciplinary team; mental, cognitive, affective and emotional status assessment in these patients has to be considered before proposing DBS [30••].
Chronic Cluster Headache
There is only one randomised placebo-controlled trial of 11 patients treated with deep brain stimulation in chronic cluster headache: the main limitation is that the double-blind observation period was of only 1-month duration [45]. In fact, efficacy takes weeks to months to take place in these patients [42, 43]. It is of interest that deep brain stimulation is not effective in the acute treatment of CH [46].
Since continuous hypothalamic stimulation needs weeks to several months to improve CH, a complex mechanism of action is probable instead of a simple inhibition of the stimulated area.
Chronically stimulated CH patients show an increased ipsilateral cold pain threshold in V1 territories [47] indicating that hypothalamic stimulation has a modulatory effect on the antinociceptive system.
In hypothalamic stimulated patients, an increased blood flow in brain regions of the pain matrix is observed and it can be hypothesized that hypothalamic stimulation restore normal metabolism in these areas thus re-establishing a normal control on trigeminal pain circuits [48].
Hypothalamic stimulated CH patients have normal parasympathetic system activity [49] suggesting that the stimulation improve CH by restoring parasympathetic control in the SSN (Fig. 1).
DBS in CH patients activates the hypothalamus, the thalamus, the somatosensory cortex, the anterior cingulate, the ipsilateral trigeminal nucleus and the ganglion, and some of these structures are also active during acute cluster attacks [48]. Since DBS does not eliminate CH, it could act upon pain circuits involved in maintaining chronic cluster headache [50].
Conclusions
Intractable chronic headache syndromes challenge routine practice in specialized headache centres and have a high disease burden [1].
When migraine and cluster headache prophylactic treatments have low efficacy and tolerability, patients ask for new therapeutic strategies and options.
In the last years, a certain benefit from neurostimulation devices has been reported in a number of studies, mainly open-label studies, and only limited conclusions are allowed. Lack of adequate placebo and small number of studied patients indicate the increasing need of adequate randomized controlled trials (RCTs).
A main issue in such RCT is placebo. Many of used devices induce effects and sensations (as paraesthesia, abnormal sensations—warm/discomfort—twitching, etc.) that easily unblind patients. In this respect, a new approach is using electrical currents below the level hypothesized to produce improvement as sham stimulation [51]: the study is still ongoing; we are really interested for the future results.
Notwithstanding, costs for neurostimulation are high; it has been estimated that the saving due to the reduction in acute treatment (sumatriptan) consumption covers costs for both stimulators and patients’ management [52].
Clear guidelines have been published on patient selection and neurostimulation procedures: clinicians must attain to those and continue the discussion in the field [30••] to offer an up to dated and in-depth balanced view on neurostimulation approaches to the intractable chronic demanding headache sufferers.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Jensen R, Stovner LJ. Epidemiology and comorbidity of headache. Lancet Neurol. 2008;7:354–61.
Scher AI, Stewart WF, Liberman J, et al. Prevalence of frequent headache in a population sample. Headache. 1998;38:497–506.
Magis D, Schoenen J. Advances and challenges in neurostimulation for headaches. Lancet Neurol. 2012;11(8):708–19.
Jurgens T, Leone M. Neuromodulation in primary headaches—pearls and pitfalls. Cephalalgia. 2013;33(8):512–25.
Lambru G, Matharu MS. Peripheral neurostimulation in primary headaches. Neurol Sci. 2014;35 Suppl 1:77–81.
Beekwilder JP, Beems T. Overview of the clinical applications of vagus nerve stimulation. J Clin Neurophysiol. 2010;27:130–8.
Kraus T, Kiess O, Hösl K, et al. CNS BOLD fMRI effects of sham-controlled transcutaneous electrical nerve stimulation in the left outer auditory canal—a pilot study. Brain Stimul. 2013;6:798–804.
Martınez-Vargas D, Valdes-Cruz A, Magdaleno-Madrigal V, Almazan-Alvarado S, Fernandez-Mas R. Effects of electrical stimulation of the vagus nerve on the development of visual habituation in the cat. Behav Brain Res. 2009;205:45–9.
Coppola G, Di Lorenzo C, Schoenen J, Pierelli F. Habituation and sensitization in primary headaches. J Headache Pain. 2013;14:65.
Goadsby PJ, Grosberg BM, Mauskop A, Cady R, Simmons KA. Effect of noninvasive vagus nerve stimulation on acute migraine: an open-label pilot study. Cephalalgia. 2014;34:986–93.
Silberstein SD, Da Silva AN, Calhoun AH, Grosberg BM, Lipton RB, Cady RK, et al. Non-invasive vagus nerve stimulation for chronic migraine prevention in a prospective, randomized, sham-controlled pilot study (the EVENT Study): report from the double-blind phase. Headache. 2014;54:1426.
Gaul C, Diener H, Solbach K, Silver N, Straube A, Magis D, et al. EHMTI-0364. Non-invasive vagus nerve stimulation using gammacore® for prevention and acute treatment of chronic cluster headache: report from the randomized phase of the preva study. J Headache Pain. 2014;15 Suppl 1:I7.
Nesbitt AD, Marin JC, Tompkins E, Ruttledge MH, Goadsby PJ. Initial use of a novel noninvasive vagus nerve stimulator for cluster headache treatment. Neurology. 2015;84:1249–53.
Ferrari MD, Klever RR, Terwindt GM, Ayata C, van den Maagdenberg AM. Migraine pathophysiology: lessons from mouse models and human genetics. Lancet Neurol. 2015;14(1):65–80.
Lipton RB, Pearlman SH. Transcranial magnetic simulation in the treatment of migraine. Neurotherapeutics. 2010;7:204–12.
Lipton RB, Dodick DW, Silberstein SD, Saper JR, Aurora SK, Pearlman SH, et al. Single-pulse transcranial magnetic stimulation for acute treatment of migraine with aura: a randomised, double-blind, parallel-group, sham-controlled trial. Lancet Neurol. 2010;9:373–80.
Bhola R, Kinsella E, Giffin N, Lipscombe S, Ahmed F, Weatherall M, et al. Single-pulse transcranial magnetic stimulation (sTMS) for the acute treatment of migraine: evaluation of outcome data for the UK post market pilot program. J Headache Pain. 2015;16:535.
Gerardy PY, Fabry D, Fumal A, Schoenen J. A pilot study on supra-orbital surface electrotherapy in migraine. Cephalalgia. 2009;29:134.
Schoenen J, Vandersmissen B, Jeangette S, Herroelen L, Vandenheede M, Gérard P, et al. Migraine prevention with a supraorbital transcutaneous stimulator: a randomized controlled trial. Neurology. 2013;80:697–704.
Magis D, Sava S, d’Elia TS, Baschi R, Schoenen J. Safety and patients’ satisfaction of transcutaneous supraorbital neurostimulation (tSNS) with the Cefaly® device in headache treatment: a survey of 2,313 headache sufferers in the general population. J Headache Pain. 2013;14:95.
Piquet M, Balestra C, Sava SL, Schoenen J. Supraorbital transcutaneous neurostimulation has sedative effects in healthy subjects. BMC Neurol. 2011;11:135.
Goadsby PJ, Bartsch T. On the functional neuroanatomy of neck pain. Cephalalgia. 2008;28 Suppl 1:1–7.
Magis D, Bruno MA, Fumal A, Gérardy PY, Hustinx R, Laureys S, et al. Central modulation in cluster headache patients treated with occipital nerve stimulation: an FDG-PET study. BMC Neurol. 2011;11:25.
Matharu MS, Bartsch T, Ward N, Frackowiak RSJ, Weiner R, Goadsby PJ. Central neuromodulation in chronic migraine patients with suboccipital stimulators: a PET study. Brain. 2004;127(Pt 1):220–30.
Leone M, Proietti Cecchini A, Messina G, Franzini A. Long-term occipital nerve stimulation for drug-resistant chronic cluster headache. Cephalalgia. 2016
• Chen YF, Bramley G, Unwin G, Hanu-Cernat D, Dretzke J, Moore D, et al. Occipital nerve stimulation for chronic migraine–a systematic review and meta-analysis. PLoS ONE. 2015;10:e0116786. Balanced and comprehensive review of an important topic as occipital nerve stimulation for chronic migraine.
Saper JR, Dodick DW, Silberstein SD, McCarville S, Sun M, Goadsby PJ, et al. Occipital nerve stimulation for the treatment of intractable chronic migraine headache: ONSTIM feasibility study. Cephalalgia. 2011;31:271–85.
Lipton R, Goadsby PJ, Cady R, Aurora SK, Grosberg BM, Freitag FG, et al. PRISM study: occipital nerve stimulation for treatment-refractory migraine. Cephalalgia. 2009;29 Suppl 1:30.
Dodick DW, Silberstein SD, Reed KL, Deer TR, Slavin KV, Huh B, et al. Safety and efficacy of peripheral nerve stimulation of the occipital nerves for the management of chronic migraine: long-term results from a randomized, multicenter, double-blinded, controlled study. Cephalalgia. 2015;35(4):344–58.
•• Martelletti P, Jensen RH, Antal A, Arcioni R, Brighina F, de Tommaso M, et al. Neuromodulation of chronic headaches: position statement from the European Headache Federation. J Headache Pain. 2013;14:86. Patient selection for neurostimulation procedures is discussed in detail.
Jürgens T, May A. Role of sphenopalatine ganglion stimulation in cluster headache. Curr Pain Headache Rep. 2014;18:433. doi:10.1007/s11916-014-0433-4.
May A, Goadsby PJ. The trigeminovascular system in humans: pathophysiologic implications for primary headache syndromes of the neural influences on the cerebral circulation. J Cereb Blood Flow Metab. 1999;19:115–27.
Schoenen J, Jensen RH, Lanteri-Minet M, Láinez MJA, Gaul C, Goodman AM, et al. Stimulation of the sphenopalatine ganglion (SPG) for cluster headache treatment. Pathway CH-1: a randomized, sham-controlled study. Cephalalgia. 2013;33:816–30.
Schytz HW, Barløse M, Guo S, Selb J, Caparso A, Jensen R, et al. Experimental activation of the sphenopalatine ganglion provokes cluster-like attacks in humans. Cephalalgia. 2013;33(10):831–41.
Jürgens TP, Barloese M, May A, Láinez JM, Schoenen J, Gaul C et al. Long-term effectiveness of sphenopalatine ganglion stimulation for cluster headache. Cephalalgia. 2016
Jürgens TP, Schoenen J, Rostgaard J, Hillerup S, Láinez MJA, Assaf AT, et al. Stimulation of the sphenopalatine ganglion in intractable cluster headache: expert consensus on patient selection and standards of care. Cephalalgia. 2014;34:1100–10.
May A, Bahra A, Buchel C, Frackowiak RS, Goadsby PJ. Hypothalamic activation in cluster headache attacks. Lancet. 1998;352:275–8.
May A, Bahra A, Buchel C, Turner R, Goadsby PJ. Functional MRI in spontaneous attacks of SUNCT: short-lasting neuralgiform headache with conjunctival injection and tearing. Ann Neurol. 1999;46:791–3.
Matharu MS, Cohen AS, Frackowiak RSJ, Goadsby PJ. Posterior hypothalamic activation in paroxysmal hemicrania. Ann Neurol. 2006;59:535–45.
Benabid AL, Chabardes S, Mitrofanis J, Pollak P. Deep brain stimulation of the subthalamic nucleus for the treatment of Parkinson’s disease. Lancet Neurol. 2009;8(1):67–81.
Leone M, Franzini A, Bussone G. Stereotactic stimulation of posterior hypothalamic gray matter for intractable cluster headache. NEJM. 2001;345(19):1428–9.
Leone M, Proietti Cecchini A. Deep brain stimulation in headache. Cephalalgia. 2015
Akram H, Miller S, Lagrata S, Hyam J, Jahanshahi M, Hariz M, et al. Ventral tegmental area deep brain stimulation for refractory chronic cluster headache. Neurology. 2016;86(18):1676–82.
Fontaine D, Lanteri-Minet M, Ouchchane L, Lazorthes Y, Mertens P, Blond S, et al. Anatomical location of effective deep brain stimulation electrodes in chronic cluster headache. Brain. 2010;133(Pt 4):1214–23.
Fontaine D, Lazorthes Y, Mertens P, Blond S, Géraud G, Fabre N, et al. Safety and efficacy of deep brain stimulation in refractory cluster headache: a randomized placebo-controlled double-blind trial followed by a 1-year open extension. J Headache Pain. 2010;11:23–31.
Leone M, Franzini A, Broggi G, Mea E, Proietti Cecchini A, Bussone G. Acute hypothalamic stimulation and ongoing cluster headache attacks. Neurology. 2006;67(10):1844–5.
Jürgens T, Leone M, Proietti-Cecchini A, Busch V, Mea E, Bussone G, et al. Hypothalamic deep-brain stimulation modulates thermal sensitivity and pain thresholds in cluster headache. Pain. 2009;146(1–2):84–90.
May A, Leone M, Boecker H, Sprenger T, Juergens T, Bussone G, et al. Hypothalamic deep brain stimulation in positron emission tomography. J Neurosci. 2006;26(13):3589–93.
Cortelli P, Guaraldi P, Leone M, Pierangeli G, Barletta G, Grimaldi D, et al. Effect of deep brain stimulation of the posterior hypothalamic area on the cardiovascular system in chronic cluster headache patients. Eur J Neurol. 2007;14:1008–15.
Leone M, Franzini A, Proietti Cecchini A, Bussone G. Success, failure and putative mechanisms in hypothalamic stimulation for drug resistant chronic cluster headache. Pain. 2013;154(1):89–94.
Wilbrink LA, Teernstra OP, Haan J, van Zwet EW, Evers SM, Spincemaille GH, et al. Occipital nerve stimulation in medically intractable, chronic cluster headache. The ICON study: rationale and protocol of a randomised trial. Cephalalgia. 2013;33(15):1238–47.
Leone M, Franzini A, Proietti Cecchini A, Mea E, Broggi G, Bussone G. Costs of hypothalamic stimulation in chronic drug-resistant cluster headache: preliminary data. Neurol Sci. 2009;30 Suppl 1:S43–7.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Massimo Leone and Alberto Proietti Cecchini declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Neuromodulation
Rights and permissions
About this article

Cite this article
Leone, M., Cecchini, A.P. Central and Peripheral Neural Targets for Neurostimulation of Chronic Headaches. Curr Pain Headache Rep 21, 16 (2017). https://doi.org/10.1007/s11916-017-0616-x
Published:
DOI: https://doi.org/10.1007/s11916-017-0616-x