
Abstract
The incidence of oropharyngeal squamous cell carcinoma (OPSCC) is on the rise. This is largely due to the rapid increase in HPV positive OPSCC, which has been shown to confer a survival advantage. HPV negative OPSCC, however, has a more aggressive tumor biology and is a challenge to treat with standard current therapies. Chemoradiation has demonstrated poor locoregional control in HPV negative OPSCC, and open surgeries are associated with high morbidity. Transoral robotic surgery (TORS) has been proposed as an option to both intensify treatment and decrease surgical morbidity for patients with HPV negative OPSCC. TORS can be utilized as a primary treatment or in persistent, recurrent, or second primary OPSCC. There is emerging data showing improved functional outcomes with TORS versus open surgery or chemoradiation. Unfortunately, there have been no randomized trials comparing TORS to chemoradiation in HPV negative OPSCC. This article will review utility of TORS for HPV negative OPSCC.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The incidence of oropharyngeal squamous cell carcinoma (OPSCC) is increasing in the USA at an alarming rate. There will be an estimated 16,420 new cases of OPSCC with an estimated 3080 deaths in 2016 [1]. Historically, squamous cell carcinoma of the upper aerodigestive tract was caused by exposure to tobacco and alcohol. The increased incidence of OPSCC is despite a decline in prevalence of tobacco use in the USA and is due to the epidemic increase in incidence of HPV positive OPSCC [2]. HPV was estimated to account for 16 % of OPSCC in the early 1980s while most recent studies suggest a prevalence of HPV positivity in >60 % of newly diagnosed OPSCC [3, 4]. HPV positive OPSCC has unique risk factors, tumor biology, and clinical characteristics when compared to HPV negative OPSCC [5–8]. Several studies have shown that HPV positivity confers a survival advantage and is the single strongest prognostic factor for OPSCC [6, 7, 9, 10].
Patients with HPV negative OPSCC have different demographics, tumor biology, and survival outcomes than patients with HPV positive OPSCC. To begin, patients diagnosed with HPV negative OPSCC tend to be older [6, 11]. HPV negative OPSCC is epidemiologically similar to the “traditional” type of squamous cell carcinoma of the upper aerodigestive tract in which long-term tobacco and alcohol exposure leads to development of malignancy [11]. HPV negative OPSCC also tends to present with higher tumor (T) classification compared to HPV positive OPSCC [7]. Similar to other epithelial carcinomas of the upper aerodigestive tract, HPV negative OPSCC typically harbor p53 mutations and stain weakly for p16 [8, 11].
Despite the relative decreased incidence of HPV negative OPSCC when compared to HPV positive OPSCC, treating patients with HPV negative disease remains a significant clinical challenge because the prognosis for patients with HPV negative OPSCC remains poor. A secondary analysis of RTOG 0129 confirmed a clinically meaningful increased risk of progression or death after adjusting for demographics, T class, nodal (N) class, and smoking for patients with HPV negative OPSCC when compared to HPV positive OPSCC [6]. In this study, patients with HPV negative OPSCC had a 25 % reduction in overall survival (OS) at 3 years (57 vs. 82 %) when compared to patients with HPV positive OPSCC [6]. A secondary analysis of the TAX 324 trial, including 111 patients with locally advanced OPSCC revealed increased mortality in HPV negative OPSCC compared to HPV positive OPSCC [7]. The overall poorer prognosis of HPV negative OPSCC is despite a trend toward treatment intensification in this patient population [7, 12, 13].
Historically, advanced-stage OPSCC was treated with open surgical resection, reconstruction, and postoperative radiotherapy [14, 15]. These open approaches to the oropharynx required mandibulotomy or pharyngotomy, resulting in significant morbidity and functional impairments to speech, swallowing, and breathing [16]. With the landmark publication of the Veterans Affairs Laryngeal Cancer Study Group trial in 1991, there has been an increased trend toward nonsurgical therapies to treat other head and neck sites, most notably OPSCC [17]. In 2002, a meta-analysis of patients with OPSCC found similar survival outcomes for patients treated with surgery and postoperative radiotherapy versus primary radiotherapy with salvage neck dissection [14]. In this same study, there was a significant difference in severe and fatal complications between these two cohorts favoring primary radiotherapy [14]. Subsequent studies showed comparable control rates as well as similar functional outcomes between primary surgery and radiotherapy for OPSCC [18, 19]. With the emergence of intensified “organ preservation” nonsurgical therapies, particularly concurrent chemoradiation, there was an increase treatment-related toxicities including mucositis, xerostomia, loss of taste, tissue fibrosis, stricture, osteoradionecrosis, neuropathy, and fatigue [20–22].
Due to the toxicities associated with concurrent chemoradiation, there are now numerous ongoing trials investigating treatment de-intensification protocols for the treatment of HPV positive OPSCC [23–26]. Patients with HPV negative OPSCC, because of the more aggressive tumor biology and poorer prognosis, are excluded from these protocols and often require more intensive therapy [6–8, 27]. There has been relatively less interest in investigating HPV negative OPSCC despite the poorer outcomes. In fact, the only trial specifically designed for HPV negative OPSCC, RTOG 1221, a randomized controlled trial of chemoradiation versus surgery followed by chemoradiation, was halted for failure to accrue. This paper will discuss the potential application of transoral robotic surgery (TORS) in the treatment of HPV negative OPSCC.
TORS
Advances in surgical technology have permitted transoral access to the upper aerodigestive tract limiting morbidity associated with traditional, open surgical resection. TORS, using the da Vinci Surgical System (Intuitive Surgical, Inc., Sunnyvale, California), was first approved by the United States Food and Drug Administration (FDA) for use in benign and selected malignancies of the head and neck in 2009, and has since become a recognized first-line treatment option in the management of OPSCC. The Flex Robotic System (MedRobotics, Raynham, MA) is also now cleared by the FDA for TORS. The potential benefits of TORS compared to open surgical approaches in the treatment of OPSCC revolve around the improvement of visualization and access. Specialized retractors and the high-resolution, three-dimensional view of the surgical field provided by a robotic system aid the surgeon during resection. Furthermore, TORS does not rely on direct line of sight access instead utilizing flexible or angled telescopes. This allows en-bloc resection of OPSCC to be performed safely without the morbidity associated with mandibulotomy or pharyngotomy.
Current Indications for TORS in Management of OPSCC
The role of TORS in the management of OPSCC has yet to be fully defined, including in HPV negative OPSCC. TORS is currently utilized for early T class (T1–T2) OPSCC with the goal of avoiding or deintesifying adjuvant treatment in HPV positive OPSCC [16]. Functional outcomes after TORS for T1–2 patients with OPSCC have been promising with low gastrostomy tube dependence at 6 and 12 months and improved dysphagia scores at 1 year [28, 29]. The potential functional benefits of TORS, however, may be lost in patients with large volume tumors due to the challenges of maintaining functionality with a large surgical defect and expected adjuvant therapy. Patients with HPV negative OPSCC are more likely to present with large volume primary disease that is less amenable to minimal access surgery. Patient selection for TORS is based on both tumor and patient characteristics. Bone invasion, carotid artery encasement, and fixation of tumor to the prevertebral musculature are contraindications to TORS. Adequate exposure is of paramount importance in selecting candidates for TORS. This includes oral compliance, neck flexibility, mandibular arch width, presence of mandibular tori, and tongue size [30].
Outcomes for TORS in HPV Negative OPSCC
There is little data investigating the role of TORS specifically for HPV negative OPSCC, and it remains unclear whether surgery should play a role in intensifying treatment for this patient population. Past strategies of accelerated fractionation radiation with or without chemotherapy and induction chemotherapy have revealed disappointing results [7, 27, 31]. TORS potentially offers a surgical option to intensify treatment for HPV negative OPSCC patients with low volume primary disease. This treatment strategy, however, remains formally untested.
RTOG 1221, was developed as a randomized phase II, two-arm trial was designed to compare survival outcomes in patients with T1-2, N1-2b HPV negative OPSCC. The experimental arm was to receive transoral surgery (TORS or transoral laser microsurgery (TLM)) for the primary tumor with concomitant neck dissection. Adjuvant intensity modulated radiation therapy (IMRT) (54–60 Gy) with or without concurrent chemotherapy was planned depending on margin status, extracapsular extension, lymphovascular or perineural invasion. The control arm treatment consisted of IMRT (70 Gy) with concurrent chemotherapy [32]. Unfortunately, this trial was terminated due to lack of accrual. The failure of RTOG 1221 to accrue suggests that physicians and patients may be unwilling to be randomized between surgical and non-surgical approaches. It is unlikely that a randomized trial will be promoted again in the foreseeable future.
There are numerous retrospective studies reporting on oncologic outcomes after TORS, primarily for HPV positive OPSCC [33–36]. Early stage HPV positive OPSCC treated using TORS with adjuvant therapies applied based on pathologic staging yields an overall survival rate of 95 % [37]. To date, there are no large studies of HPV negative patients treated with TORS, with few studies reporting survival analysis based on HPV status [33, 36]. In one retrospective study, Cohen et al. reported on 13 patients with HPV negative OPSCC who underwent primary TORS and staged neck dissection. Adjuvant IMRT with or without concurrent cisplatin-based chemotherapy was given based on pathologic characteristics including margin status, extracapsular spread, and nodal burden. Eleven of the 13 patients had T1 or 2 tumors. Four patients had N0, seven patients had N1, and two patients had N2b nodal disease. Six patients received adjuvant concurrent chemoradiation, two received radiation alone, and five received no adjuvant therapy. After a mean follow up of 23 months, no patients had local recurrence, and one patient had both local and distant recurrence. There was no significant difference in disease-free survival between the HPV positive and HPV negative cohort in this study [33]. Moore et al. performed a retrospective review of a TORS database and found 66 patients treated for OPSCC with at least 2 years of follow up. Eighteen patients were HPV negative, and their 3 year disease-specific and recurrence-free survival was 89 and 83 %, respectively. Compared to HPV positive patients, there was no significant survival difference [34]. Most recently, De Almeida et al. reported a multi-institutional retrospective review of 364 patients with OPSCC, of which 70 were HPV negative. This study found no significant overall or disease-specific survival difference based on HPV or p16 status. This study representing the largest reported series of HPV negative OPSCC treated with TORS found favorable survival in HPV negative patients with 92 and 94 % 2-year locoregional control and overall survival, respectively [36]. Table 1 summarizes the results of TORS for HPV negative OPSCC.
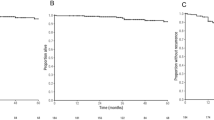
There are no randomized trials comparing primary surgical strategies to non-surgical strategies regardless of HPV status. Prospective non-surgical trials that included both HPV positive and negative patients report an overall survival range of 31 to 74 % at 3 years and progression-free survival range of 29 to 72 % for HPV negative OPSCC (Table 2). It is difficult to compare surgical with non-surgical studies for OPSCC. Surgical studies suggest improved survival for HPV negative OPSCC. However, the surgical study population is very small. Most importantly, the surgical studies include lower stage disease (Tables 1 and 2). So, the limitations of the available data are clear. Given the distinct tumor biology between HPV positive and HPV negative OPSCC, it is imperative that future trials segregate these populations. Multicenter studies will be required to learn more about the impact of TORS on HPV negative OPSCC.
Compared to traditional open surgical techniques for OPSCC, TORS provides better functional outcomes. Tracheotomy rates with traditional open surgical techniques approaches 100 %. With a transoral approach, there is a significant reduction of tracheotomy rates (0–2 %), shorter time to decannulation when a tracheotomy is placed, and shorter hospitalization time [34, 38, 39,]. Swallowing function is also improved with transoral approaches when compared to traditional open surgery for OPSCC. Outcomes data comparing transoral primary surgical and non-surgical approaches to OPSCC shows significantly improved swallowing function in patients treated with primary surgery with the majority of patients reporting “normal” swallowing at 1-year follow up [29]. Gastrostomy tube dependence is reported to range from 15 to 25 % for primary RT and increase to 18.1 to 63 % following CRT [39]. Rates of permanent gastrostomy tube after TORS is significantly lower ranging from 2 to 9 % in larger studies [28, 30, 34, 40–43]. Therefore, TORS may be a good option to improve functional outcomes even in selected HPV negative patients with OPSCC.
TORS for Salvage Surgery
In appropriately selected cases, TORS for resection of recurrent, persistent, or second primary OPSCC reveals acceptable oncologic outcomes. Patients with HPV negative OPSCC have higher local failure rates than those with HPV positive tumors [6, 7, 9, 10]. These patients are often not eligible for therapeutic re-irradiation. Regardless of HPV status, salvage surgery remains the best oncologic option in the setting of recurrence after radiation or chemoradiation.
As expected, the overall prognosis in the salvage setting is generally poor. A study of 246 patients with HPV positive OPSCC treated with traditional open salvage surgery demonstrated a 55 % recurrence rate and the overall 5-year survival of 32 % [44]. Disease-free interval >1 year and initial early stage disease were significant prognostic factors in this study. White et al. reported on 64 patients who underwent TORS for salvage of recurrent OPSCC matched by TNM classification to 64 patients who underwent open salvage surgery. The TORS cohort had a significantly lower incidence of tracheostomy use (14 vs. 50, p < .001), feeding tube use (23 vs. 48, p < .001), shorter hospital stay, decreased operative time, and a significant decrease in incidence of positive margins (6 vs. 19, p = .007). The 2-year recurrence-free survival rate was also significantly higher in the TORS compared to open group (74 vs. 43 %, p = .01). Unfortunately, there was no mention of HPV status in this study [45••].
The use of TORS in the salvage setting is considerably more challenging than in treatment-naïve patients. To begin, patients with recurrent, persistent, or second primary OPSCC are often malnourished. This can dramatically impair wound healing after TORS, where the surgical defect is expected to heal by secondary intention. In addition, the risk of complications after TORS is significantly increased in patients who have been previously radiated. The risk of bleeding after TORS, for example, has been shown to be increased after salvage surgery (10.3 %) compared to primary surgery (6.8 %) [46]. These patients are also at substantially increased risk of requiring a tracheostomy and/or gastrostomy tube after TORS. For these reasons, complex reconstruction may be useful in patients undergoing TORS for recurrent, persistent, or second primary OPSCC. Reconstruction after TORS, including microvascular-free tissue transfer, has been shown to be feasible with acceptable functional outcomes [47]. Microvascular-free tissue transfer is especially useful after TORS salvage surgery when the carotid artery is left exposed and or for large defects. Small (T1) recurrent, persistent, or second primary OPSCC requiring TORS are usually acceptable for treatment without microvascular reconstruction (Fig. 1). However, larger (>T1) cancers requiring salvage TORS will frequently require microvascular reconstruction (Fig. 2). Reconstruction is particularly important in these cases as re-irradiation may be beneficial depending on pathology to improve locoregional control. It is important to understand that TORS and open approaches are not mutually exclusive. Depending on the extent of disease and need for microvascular reconstruction, TORS for salvage surgery may require a hybrid approach utilizing both TORS and open techniques. In these cases, TORS is utilized primarily to assist in clearing pharyngeal margins and deeper pharyngeal dissection while avoiding mandibulotomy. Additional transoral and transcervical dissection can be used to complete the resection and to deliver the specimen through the neck. Such TORS-assisted approaches are most often used for salvage procedures that require microvascular reconstruction (Fig. 3). Inset of a microvascular flap can also be aided by use of a robotic device. This approach has been shown to be feasible and safe [48].

Axial image from positron emission tomography (PET)/computed tomography (CT) of recurrent T1 human papillomavirus (HPV) negative squamous cell carcinoma of the right base of tongue after concurrent chemoradiation. This small-volume cancer was amenable to treatment using transoral robotic surgery (TORS) without reconstruction

Axial image from contrast-enhanced computed tomography (CT) of recurrent T2 human papillomavirus (HPV) negative squamous cell carcinoma of the right base of tongue after concurrent chemoradiation. This more deeply infiltrative cancer was treated using a hybrid transoral robotic surgery (TORS)/open approach with simultaneous microvascular reconstruction

Axial image from contrast-enhanced computed tomography (CT) after salvage transoral robotic (TORS) assisted surgery with simultaneous microvascular reconstruction for recurrent human papillomavirus (HPV) negative squamous cell carcinoma of the right base of tongue
Discussion
With the increasing incidence of HPV positive OPSCC, there is great interest in improved treatment strategies for OPSCC. Most of these are designed as de-intensification protocols. The aim of de-intensified strategies is to maintain excellent oncologic outcomes while potentially avoiding late toxicities and improving long-term functional outcomes, in a group of patients whose overall survival is excellent regardless of the treatment [23–26, 49, 50•]. HPV negative OPSCC patients, however, still compromise a significant proportion of the OPSCC patients who fail treatment. Contemporary treatment strategies, namely concurrent chemoradiation, provide relatively poor locoregional control and overall survival in HPV negative OPSCC [6, 7, 27]. So it is reasonable to consider TORS, when feasible, as part of a treatment intensification strategy in HPV negative OPSCC. It is important to recognize the very different tumor biology and different treatment objectives with respect to TORS between HPV positive and negative tumors.
There exists no prospective randomized data to help define the role of TORS in HPV negative OPSCC. Studies that include both HPV positive and HPV negative OPSCC patients have shown that TORS offers excellent disease control and survival in early stage disease [37] and compares well to definitive concurrent chemoradiation for the management of advanced stage disease [33–35, 40]. Furthermore, the functional outcomes of TORS are superior to both open surgical procedures and concurrent chemoradiation in regards to tracheotomy rates and gastrostomy tube dependency [28, 30, 34, 40–42, 51]. Of course, the majority of the patients studied after TORS for OPSCC were HPV positive. So, it is difficult to extrapolate the promising oncologic and functional outcomes to HPV negative OPSCC. TORS may be a reasonable option for a patient with early T class HPV negative OPSCC to potentially obtain the benefits from a reduction in postoperative radiation dose and potential avoidance of chemotherapy. More likely, TORS can be used as a less invasive technique for treatment intensification in untreated HPV negative OPSCC patients.
The role of TORS is also important in the setting of recurrent, persistent, or second primary HPV negative OPSCC. HPV negative OPSCC is more likely to develop progressive disease or local recurrence [6, 7, 9, 52]. Re-irradiation with or without chemotherapy therapy can be performed in the salvage setting but is seldom preferred given the increased toxicity and overall dim prognosis [53]. Compared to open salvage surgery, TORS been shown to provide a greater incidence of negative margins and improved recurrence-free survival in the salvage setting [45••]. Treatment intensification utilizing TORS following induction chemotherapy and selective adjuvant re-irradiation can allow for a “triple modality” intensified therapy for this disease.
The optimal strategy for intensifying treatment in HPV negative OPSCC has yet to be defined. However, given the relatively poor survival for these patients, novel treatment strategies are warranted. Future directions may involve induction approaches that include targeted biologic therapies and or immune-modulated drugs [54]. Neo-adjuvant therapy with novel agents before TORS in window-of-opportunity trials may also offer an opportunity to deepen our understanding of HPV negative OPSCC.
Conclusion
The prognosis of patients with HPV negative OPSCC remains relatively poor, and few current treatment strategies are directed toward this group of high-risk patients. HPV negative OPSCC demonstrates a more aggressive tumor biology and remains a significant therapeutic challenge. TORS compares favorably to traditional open surgical techniques for OPSCC that are morbid. Contemporary non-surgical therapies have relatively poor locoregional control and survival in HPV negative OPSCC. So, there remains an unmet clinical need for innovative approaches in HPV negative OPSCC. In highly selected cases of HPV negative OPSCC, TORS may be an option to help better tailor therapy based on pathologic staging. TORS should also be considered as primary treatment for recurrent, persistent, or second primary HPV negative OPSCC. Treatment intensification in this group of patients may involve a combination of treatment modalities. To date, robust clinical data are lacking for the use of TORS in HPV negative OPSCC, and the role of TORS in this setting remains an area of active investigation.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Siegel R, Miller K, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;66(1):7–30.
Nguyen K, Marshall L, Hu S, Neff L. State-specific prevalence of current cigarette smoking and smokeless tobacco use among adults aged ≥18 years—United States, 2011-2013. MMWR Morb Mortal Wkly Rep. 2015;64(19):532–6.
Benson E, Li R, Eisele D, Fakhry C. The clinical impact of HPV tumor status upon head and neck squamous cell carcinomas. Oral Oncol. 2014;55:565–74.
Chaturvedi AK, Engels EA, Pfeiffer RM, et al. Human papillomavirus and rising oropharyngeal cancer incidence in the United States. J Clin Oncol. 2011;29:4294–301.
Chaturvedi AK, Engels EA, Anderson WF, Gillison ML. Incidence trends for human papillomavirus-related and -unrelated oral squamous cell carcinomas in the united states. J Clin Oncol. 2008;26(4):612–9.
Ang KK, Harris J, Wheeler R, Weber R, Rosenthal DI, Nguyen-Tan PF, et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N Engl J Med. 2010;363(1):24–35.
Posner MR, Lorch JH, Goloubeva O, Tan M, Schumaker LM, Sarlis NJ, et al. Survival and human papillomavirus in oropharynx cancer in TAX 324: a subset analysis from an international phase III trial. Ann Oncol. 2011;22(5):1071–7.
Gillison ML, Koch WM, Capone RB, et al. Evidence for a causal association between human papillomavirus and a subset of head and neck cancers. J Natl Cancer Inst. 2000;92:709–20.
Rischin D, Young RJ, Fisher R, Fox SB, Le QT, Peters LJ, et al. Prognostic significance of p16INK4A and human papillomavirus in patients with oropharyngeal cancer treated on TROG 02.02 phase III trial. J Clin Oncol. 2010;28(27):4142–8.
Fakhry C, Westra WH, Li S, Cmelak A, Ridge JA, Pinto H, et al. Improved survival of patients with human papillomavirus-positive head and neck squamous cell carcinoma in a prospective clinical trial. J Natl Cancer Inst. 2008;100(4):261–9.
Pytynia KB, Dahlstrom KR, Sturgis EM. Epidemiology of HPV-associated oropharyngeal cancer. Oral Oncol. 2014;50(5):380–6.
Brizel DM, Albers ME, Fisher SR, et al. Hyperfractionated irradiation with or without concurrent chemotherapy for locally advanced head and neck cancer. NEJM. 1998;338:1798–804.
Rosenthal D, Harari P, Giralt J, et al. Association of Human Papillomavirus and p16 Status with Outcomes in the IMCL-9815 Phase III Registration Trial for Patients with Locoregionally Advanced Oropharyngeal
Parsons JT, Mendenhall WM, Stringer SP, et al. Squamous cell carcinoma of the oropharynx: surgery, radiation therapy, or both. Cancer. 2002;94:2967–80.
Parsons JT, Mendenhall WM, Million RR, Stringer SP, Cassisi NJ. The management of primary cancers of the oropharynx: combined treatment or irradiation alone? Semin Radiat Oncol. 1992;2:142–8.
Brickman D, Gross ND. Robotic approaches to the pharynx: tonsil cancer. Otolaryngol Clin North Am. 2014;47(3):359–72.
[No authors listed]. Induction chemotherapy plus radiation compared with surgery plus radiation in patients with advanced laryngeal cancer. The Department of Veterans Affairs Laryngeal Cancer Study Group. N Engl J Med. 1991;324:1685–1690.
Diaz-Molina JP, Rodrigo JP, Alvarez-Marcos C, et al. Functional and oncological results of nonsurgical vs surgical treatment in squamous cell carcinomas of the oropharynx. Acta Otorrinolaringol Esp. 2012;63:348–54.
Lyer N, Tan D, Tan V, et al. Randomized trial comparing surgery and adjuvant radiotherapy versus concurrent chemoradiotherapy in patients with advanced, nonmetastatic squamous cell carcinoma of the head and neck: 10-year update and subset analysis. Cancer. 2015;121:1599–607.
Prestwich RJ, Kancherla K, Oksuz DC, et al. A single centre experience with sequential and concomitant chemoradiotherapy in locally advanced stage IV tonsillar cancer. Radiat Oncol. 2010;5:121.
Greven KM, White DR, Browne JD, Williams III DW, McGuirt Sr WF, D’Agostino Jr RB. Swallowing dysfunction is a common sequelae after chemoradiation for oropharynx carcinoma. Am J Clin Oncol. 2008;31:209–12.
Goepfert R, Yom S, Ryan W, Cheung S. Development of a chemoradiation therapy toxicity staging system for oropharyngeal carcinoma. Laryngoscope. 2015;125:869–76.
Chera B, Amdur R, Tepper J, et al. Phase 2 trial of de-intensified chemoradiation therapy for favorable-risk human papillomavirus-associated oropharyngeal squamous cell carcinoma. Int J Radiat Oncol Biol Phys. 2015;93(5):976–85.
Owadally W, Hurt C, Timmins H. PATHOS: a phase II/III trial of risk-stratified, reduced intensity adjuvant treatment in patients undergoing transoral surgery for Human papillomavirus (HPV) positive oropharyngeal cancer. BMC Cancer. 2015;15:602.
Nguyen T, Zhang Q, Ang K. Randomized phase III trial to test accelerated versus standard fractionation in combination with concurrent cisplatin for head and neck carcinomas in the Radiation Therapy Oncology Group 0129 trial: long-term report of efficacy and toxicity. J Clin Oncol. 2014;32(34):3858–66.
Urban D, Corry J, Solomon B. Weekly cisplatin and radiotherapy for low risk, locoregionally advanced human papillomavirus-positive oropharyngeal squamous cell carcinoma. Head Neck. 2015. doi:10.1002/hed.24169.
Lassen P, Eriksen JG, Krogdahl A, Therkildsen MH, Ulhoi BP, Overgaard M, et al. The influence of HPV-associated p16-expression on accelerated fractionated radiotherapy in head and neck cancer: evaluation of the randomised DAHANCA 6&7 trial. Radiother Oncol. 2011;100(1):49–55.
Dziegielewski PT, Teknos TN, Durmus K, et al. Transoral robotic surgery for oropharyngeal cancer: long-term quality of life and functional outcomes. JAMA Otolaryngol Head Neck Surgery. 2013;139(11):1099–108.
Chen AM, Daly ME, Luu Q, et al. Comparison of functional outcomes and quality of life between transoral surgery and definitive chemoradiotherapy for oropharyngeal cancer. Head Neck. 2015;37:381–5.
Olsen SM, Moore EJ, Laborde RR, Garcia JJ, Janus JR, Price DL, et al. Transoral surgery alone for human-papillomavirus-associated oropharyngeal squamous cell carcinoma. Ear Nose Throat J. 2013;92(2):76–83.
Ang K, Zhang Q, Rosenthal D, et al. Randomized phase III trial of concurrent accelerated radiation plus cisplatin with or without cetuximab for Stage III to IV head and neck carcinoma: RTOG 0522. J Clin Oncol. 2014;32:2940–50.
Holsinger F, Thorstad W, Fontenla S, et al. Randomized phase II trial of transoral endoscopic head and neck surgery followed by risk-based IMRT and weekly cisplatin versus IMRT and weekly cisplatin for HPV negative oropharynx cancer RTOG 1221.
Cohen MA, Weinstein GS, OMalley BW, et al. Transoral robotic surgery and human papillomavirus status: oncologic results. Head Neck. 2011;33:573–80.
Moore EJ, Olsen SM, Laborde RR, et al. Long-term functional and oncologic results of transoral robotic surgery for oropharyngeal squamous cell carcinoma. Mayo Clin Proc. 2012;87:219–25.
Ford S, Brandwein-Gensler M, Carroll W, et al. Transoral robotic versus open surgicalapproaches to oropharyngeal squamous cell carcinoma by human papillomavirus status. Head Neck. 2014;151(4):606–11.
De Almeida J, Li R, Magnuson S, et al. Oncologic outcomes after transoral robotic surgery: a multi-institution study. JAMA Otolaryngol Head Neck Surg. 2015;141(12):1043–51.
Kelly K, Johnson-Obaseki S, Lumingu J. Oncologic, functional and surgical outcomes of primary transoral robotic surgery for early squamous cell cancer of the oropharynx: a systematic review. Oral Oncol. 2014;50:696–703.
Harari P, Harris J, Kies M, et al. Postoperative chemoradiotherapy and cetuximab for high-risk squamous cell carcinoma of the head and neck: radiation therapy oncology group RTOG-0234. J Clin Oncol. 2014;32:2486–95.
Al-Khudari S, Bendix S, Lindholm J, Simmerman E, Hall F, Ghanem T. Gastrostomy tube use after transoral robotic surgery for oropharyngeal cancer. ISRN Otolaryngol. 2013;2013:190364.
Weinstein GS, O’Malley Jr BW, Cohen MA, Quon H. TRansoral robotic surgery for advanced oropharyngeal carcinoma. Arch Otolaryngol Head Neck Surg. 2010;136(11):1079–85.
Hurtuk AM, Marcinow A, Agrawal A, Old M, Teknos TN, Ozer E. Quality-of-life outcomes in transoral robotic surgery. Otolaryngol Head Neck Surg. 2012;146(1):68–73.
Moore EJ, Olsen KD, Kasperbauer JL. Transoral robotic surgery for oropharyngeal squamous cell carcinoma: a prospective study of feasibility and functional outcomes. Laryngoscope. 2009;119(11):2156–64.
Setton J, Lee N, Riaz N, et al. A multi-institution pooled analysis of gastrostomy tube dependence in patients with oropharyngeal cancer treated with definitive intensity-modulated radiotherapy. Cancer. 2015;121:294–301.
Agra I, Carvalho A, Ulbrich F, et al. Prognostic factors in salvage surgery for recurrent oral and oropharyngeal cancer. Head Neck. 2006;28:107–13.
White H, Ford S, Bush B. Salvage surgery for recurrent cancer of the oropharynx. JAMA Otolaryngol Head Neck Surg. 2013;139(8):773–8. Retrospective multi-institutional case control study of TNM matched patients groups comparing TORS vs traditional open approach. Patients who underwent TORS had significantly lower tracheostomy use, feeding tube use and shorter hospital stays and decreased incidence of positive marginsThe 2 year recurrence free survival rate was significantly higher in the TORS group.
Asher SA, White HN, Kejner AE, Rosenthal EL, Carroll WR, Magnuson JS. Hemorrhage after transoral robotic-assisted surgery. Otolaryngol Head Neck Surg. 2013;149(1):112–7.
de Almeida JR, Park RC, Villanueva NL, Miles BA, Teng MS, Genden EM. Reconstructive algorithm and classification system for transoral oropharyngeal defects. Head Neck. 2014;36(7):934–41. doi:10.1002/hed.23353.
Selber JC, Sarhane KA, Ibrahim AE, Holsinger FC. Transoral robotic reconstructive surgery. Semin Plast Surg. 2014;28(1):35–8. doi:10.1055/s-0034-1368166.
Weinstein GS, Quon H, O’Malley BW, Kim GG, Cohen MA. Selective neck dissection and deintensified postoperative radiation and chemotherapy for oropharyngeal cancer: a subset analysis of the university of pennsylvania transoral robotic surgery trial. Laryngoscope. 2010;120(9):1749–55.
Rosenthal D, Harari P, Giralt D, et al. Association of human papillomavirus and p16 status with outcomes in the IMCL-9815 phase iii registration trial for patients with locoregionally advanced oropharyngeal squamous cell carcinoma of the head and neck treated with radiotherapy With or Without Cetuximab. J Clin Oncol. 2015;33. Phase III Registration Trial of locoregionally advanced OPSCC. This study confirmed a survival for HPV positive patients and found that the addition of cetuximab to radiotherapy improved locoregional control, overall survival and progression free survival.
Williams CE, Kinshuck AJ, Derbyshire SG, et al. Transoral laser resection versus lip-split mandibulotomy in the management of oropharyngeal squamous cell carcinoma (OPSCC): a case match study. Eur Arch Otorhinolaryngol. 2014;271:367–72.
Worden FP, Kumar B, Lee JS, et al. Chemoselection as a strategy for organ preservation in advanced oropharyngeal cancer: response and survival positively associated with HPV 16 copy number. J Clin Oncol. 2008;26:3138–46.
Kharofa J, Choong N, Want D. Continuous-course reirradiation with concurrent carboplatin and paclitaxel for locally recurrent, nonmetastatic squamous cell carcinoma of the head-and-neck. Int J Radiat Oncol Biol Phys. 2012;83(2):690–5.
Dillon M, Harrington K. Human papillomavirus–negative pharyngeal cancer. J Clin Oncol. 2015;33:3251–61.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Ryan Sload declares that he has no conflict of interest.
Natalie Silver declares that she has no conflict of interest.
A. Basit Jawad declares that he has no conflict of interest.
Neil D. Gross has served as an unpaid scientific advisor for both MedRobotics and Intuitive Surgical, Inc.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Head and Neck Cancers
Rights and permissions
About this article

Cite this article
Sload, R., Silver, N., Jawad, B.A. et al. The Role of Transoral Robotic Surgery in the Management of HPV Negative Oropharyngeal Squamous Cell Carcinoma. Curr Oncol Rep 18, 53 (2016). https://doi.org/10.1007/s11912-016-0541-x
Published:
DOI: https://doi.org/10.1007/s11912-016-0541-x