
Abstract
Parkinson’s disease (PD) is a chronic progressive neurodegenerative and multidimensional disease that involves a range of disabling motor and nonmotor symptoms. These symptoms can have a major impact on the quality of life of PD patients. The focus of this article is to stress the importance of the interdisciplinary team intervention approach in the treatment of patients with PD. The team approach uses experts in PD from different health care professions, including a neurologist, a nurse, a speech and language therapist, a physiotherapist, a social worker, a psychiatrist, an occupational therapist, a sexologist, and a dietician. The major aim of the team and of teamwork is to provide professional care in all motor and nonmotor aspects of PD throughout the course of the disease. There are different models of multidisciplinary teams: inpatient facility, community rehabilitation facility, and synchronized multiprofessional treatment in the community. The Tel Aviv Sourasky Medical Center model of interdisciplinary care was designed to create a coordinated multidisciplinary team in the Movement Disorders Unit. The role of each team member and their professional objective are described. Their collaboration is by design a promotion of a team goal for maintaining and enhancing the quality of life of PD patients and their families.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
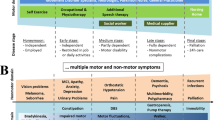
One of the most significant milestones achieved in recent years in the field of Parkinson’s disease (PD) has been the recognition that it is a multisystem disease affecting the entire brain, spinal cord, and autonomic nervous system [1, 2]. The transition from being considered a disease solely affecting the nigrostriatal dopaminergic system to one that also affects nondopaminergic systems has created increasing awareness of pathological aspects unrelated to motor functions [3]. Many studies that have appeared over the past decade have highlighted the impact that nonmotor features of PD have on the quality of life of PD patients and their families [4]. Gait, balance, falls, and, to a lesser degree, tremor have been recognized as being important motor features affecting quality of life. Moreover, depression, anxiety, sleep disturbances, autonomic dysfunctions (constipation, urinary incontinence, and erectile dysfunction), pain, visual problems, and cognitive decline play a major role affecting not only PD patients, but also their families [5–7]. Notably, PD is a chronic progressive disease, and issues that are of major significance in its early stages, such as work-related problems, public image, and shame, as well as uncertainty about the diagnosis and the future, may all play a significant role especially in the more advanced stages. As the disease progresses, the fight to maintain independence and safe mobility, the struggle with polypharmacy and the side effects of medications, the decline in cognition, and the emergence of sleep disturbances and significant autonomic disturbances or pain become more prominent [8, 9]. The therapeutic targets of minimizing symptoms and maintaining as normal a lifestyle as possible in the early stages of PD are typically replaced by designing a palliative approach for providing support and guidance, in recognition of the reality that most symptoms cannot be cured and that acceptance is part of the fight for independence. Palliative care is provided in order to maintain the best possible quality of life on the part of both the patient and the family. The spouse/caregiver is also a major partner throughout the course of the disease, in terms of coping with the patient’s depression, anxiety, and sleep disturbances, and sharing the marital difficulties, sexual disturbances, and social and financial restrictions. The caregiver plays a major role in the patient’s quality of life and degree of independence, and should be offered special professional attention [10•, 11•].
History of Multidisciplinary Care in Parkinson’s Disease
The concept of a multidisciplinary team approach to the care of families of PD patients evolved from a greater understanding of the complexity of PD, its multifaceted nature, the switch from providing symptomatic care to palliative care, and the recognition of the essential role of the spouse/caregiver in the management of the disease [12]. The first description of a team approach to the care of people with PD was published by Carlson-Davis in an occupational therapy journal in 1977. This was followed in 1981 by the controlled trial by Gibbered et al. [13] on the role of physiotherapy and occupational therapy in PD. Over the next 30 years, a few studies have been published on the role of the multiprofessional team in a PD treatment center setting [14, 15•]. A recent study by van der Marck et al. scientifically validated this approach in a nonrandomized controlled trial on integrated multidisciplinary care for PD. Publications on this subject have highlighted the concept that a team is needed to deal with all aspects of the disease throughout its course. The team should include a nurse, a psychologist, a speech and language therapist, a psychiatrist, a physiotherapist, an occupational therapist, a sexologist, a dietitian and, when indicated, an expert in sleep disturbances, an orthopedic surgeon, and a physiologist with special expertise in respiration [16•]. Few medical systems can afford to make all of these professionals available to all patients at all times, nor is it essential that they do so. Rather, the type of intervention and the team members needed to conduct it can be tailored to the specific needs of an individual patient and the patient’s family. Such a personalized approach, however, requires coordination and lines of communication between all team members under the direction of a team leader. Ideally, the team leader should be a neurologist with expertise in PD care and one who will be readily available to the patients, their families, and the other team members.
PD is a chronic, progressive disease which can affect an individual for decades. It can be characterized by the occurrence of multiple crises over those years. Although the full team can be expected to be recruited for assessment and care in an inpatient setting over a period of a few weeks, this kind of professional support is not realistic on an outpatient basis. A crisis intervention approach for treating patients in all stages of the disease is crucial in order to contend with all of these complex needs. Crises take all kinds of forms, from the need to quickly provide information about sudden events that may or may not be associated with the disease, to the processes involved in the patient’s life (e.g., getting a divorce, being fired from work, starting to experience falls, considering treatment with levodopa, deep brain stimulation, Duodopa or apomorphine pumps, facing cognitive decline with psychosis, debating about institutionalization or end-of-life dilemmas). This wide range of potential events necessitates the availability of a pool of well-trained multiprofessionals from which the team leader and team coordinator can recruit those needed for dealing with the specific crisis at a particular time [17].
Different Models of a Multidisciplinary Team
Inpatient Facility
Many countries have hospitals that contain a neurological rehabilitation center in which PD patients can be admitted for a number of weeks at the time of a crisis or on a yearly basis. The multidisciplinary team is part of the institution: it evaluates each new PD patient and develops a personalized intervention program. The patient is treated daily and evaluated weekly, and the staff members meet regularly to share information and opinions and plan the next step. This short intervention may be followed by a community-based interventional program. Scheduled yearly hospitalizations in rehabilitation inpatient centers are becoming fewer owing to financial constraints. Inpatient rehabilitation facilities have been becoming increasingly available only after major deterioration into a parkinsonian crisis secondary to causes such as a stroke, major surgery, severe pneumonia, and falls and associated fracture, as well as acute confusion or psychosis [18].
Community Rehabilitation Facility
Community-based rehabilitation centers frequently treat PD patients during weekly or twice-weekly sessions for a total of eight to 12 sessions, often according to the patient’s ability to pay. A new patient is usually referred for a specific problem, such as falls, speech disturbances, and cognitive issues. Even though the patient had been referred for a specific problem, many of these centers provide a multidisciplinary assessment and design a personalized multimodality therapeutic intervention. A patient may initially be given individual therapy and then be referred for group therapy. Such groups are becoming more popular because they are more affordable. Group therapy can focus exclusively on motor issues (led by a physiotherapist), on cognition issues (led by an occupational therapist), on activities of daily living (led by an occupational therapist), or on speech and communication issues (led by a speech and language therapist). Groups on dynamic and psychosocial issues for spouses/caregivers and patients are usually led by social workers or psychologists. The multimodality approach also allows there to be two or three leaders for a single group in order to provide answers to different but related issues at the same sessions. For example, the combination of a nurse and a social worker can provide the most appropriate answers for medical and social issues, whereas psychologists and speech and language therapists can be most effective in dealing with issues concerning communication. Thus, group therapy has been gaining increasing attention as an efficient and effective means of long-term therapy [19, 20].
Synchronized Multiprofessional Treatment in the Community
The multidisciplinary team approach has recently been moved to the community setting. Patients are treated at home or in a community clinic on a regular basis by physiotherapists, occupational therapists, speech and language therapists, psychologists, and other professionals. The treatment is administered individually, but all the therapists involved can communicate and consult electronically, and can regularly share information. The case manager serves as the coordinator of this process and is responsible for the assessment of the patient's performance. Such team work requires a high level of motivation on the part of all the team members [21].
Interdisciplinary Team Approach in a Parkinson Disease Center—the Tel Aviv Model
Over the past 18 years, the Tel Aviv National Parkinson Foundation Center of Excellence has been operating as an outpatient, interdisciplinary center in a tertiary academic hospital. The concept underlying this model is that the three neurologists, all the therapists, and all the other team members conduct their work in the same facility and share the same secretarial services, including data access. Patients and families are seen by the neurologist every 1–6–months, as required, and are always seen by the Center of Excellence nurse at the same visit. Sessions with the social worker, speech and language therapist, psychiatrist, genetic counselor, sexologist, geriatrician, dietitian, occupational therapist, and other specialists are scheduled in advance. In addition, caregivers can receive individual counseling and support from the PD nurse, social worker, psychiatrist, or sexologist free of charge. The senior neurologist is the team leader, the PD nurse is the clinical coordinator, and the speech and language therapist is the team coordinator. The team meets formally once a week, but there is constant informal sharing of information. Special meetings are held when necessary. The center follows over 3,000 patients regularly and operates according to a crisis intervention model. The speech and language therapist see patients regularly in order to provide clear swallowing guidelines for the prevention of aspiration. There is a very active group therapy program which patients attend either once or twice a week to receive treatment for motor and mobility issues. The groups are open to all patients, mainly for physiotherapy and prevention of falls. The other groups meet once a week for eight to 12 sessions, and are usually led by a nurse, social worker, or speech and language therapist. The groups comprise eight to 12 participants, who are patients only, spouses/caregivers only, or patients and spouses/caregivers. The group for families of recently diagnosed patients is led by a neurologist together with a psychiatrist, a social worker, and a nurse [22•].
The Role of Each Team Member at the Tel Aviv Sourasky Medical Center Model of Interdisciplinary Care in the Movement Disorders Unit
The Tel Aviv Sourasky Medical Center model of interdisciplinary care in the Movement Disorders Unit was designed to create a coordinated multidisciplinary team. Three neurologists who are movement disorders specialists and a nurse specialist are employed full time in the unit. The additional specialists are part-time speech and language therapists, psychiatrists, a social worker, a sexologist, and a physiotherapist, each with their own professional objective, and working together toward the single main goal of maintaining and enhancing the quality of life of the PD patients and their families.
The role of the speech and language therapist is to educate and increase the awareness of the patients, caregivers, and other team members of the patients’ speech and swallowing disturbances. We are motivated by the belief that early referral will lead to early intervention, which may avoid communication difficulties and reduce aspiration pneumonia. In 2008, an evidence-based guideline for intervention by the speech and language therapist in PD was published [12]. It includes specific recommendations that can assist the speech and language therapist when working with PD patients. The fact that this therapist spends 3 days a week at our center and is personally involved in all of the center’s academic, clinical, and social activities has created a unique working environment with regard to awareness of and interventions for speech and swallowing difficulties.
Patients with depression, anxiety, or psychosis are frequently referred for evaluation and treatment to either the psychiatrist or the social worker, and sometimes to both. The psychiatrist evaluates the mental status of patients and, when indicated, recommends the provision of psychosocial support and cognitive behavior therapy, which may also involve family members and/or caregivers. The psychiatrist may prescribe medications and/or provide psychotherapy according to the patient’s needs and the type of crisis.
The social worker has a central role in the multidisciplinary team, helping patients and their families cope with the psychosocial ramifications of PD. The social worker helps patients and their families in recruiting community and personal resources to improve the quality of life of the patients and their families. The social worker’s expertise in helping to improve coping abilities and recruiting potential supportive resources is tailored to the needs of each individual and each family. The group therapy program is usually guided by the social worker together with another team member (the nurse, the speech and language therapist, the neurologist, or the psychiatrist).
People with PD and their partners experience a variety of sexual disturbances and difficulties during the course of the disease. The sexologist plays a critical role in promoting sexual health for the patients and in our outreach program, which provides information on sexual function and dysfunction and related issues to families with PD. Sexual counseling covers physical issues, marital aspects, and emotional difficulties, as well support in regard to ethnic, cultural, and religious issues. The overall goal of sex counseling is reestablishing sexual pleasure and satisfaction, intimacy, and open communication. The unit nurse or neurologist who sees the patient is most often the one who initiates the discussion about sexual issues and refers the patient to the sexologist, urologist, gynecologist, or psychologist/social worker when there is need for further consultation.
The benefits of physical activity for PD patients have been established by a growing body of empirical evidence that confirms our clinical experience of exercise having a positive impact on the well-being of patients. The role of the physical therapist is to prevent physical symptoms associated with PD and to provide treatment for existing ones in order to restore maximum movement, functional ability, and participation in activities of daily living. The therapeutic arsenal of physiotherapy for PD is outlined in an evidence-based guideline for clinical practice [23]. Our PD patients are involved in a number of physical therapy programs, including individual sessions, exercise groups and virtual reality interventions.
The unit also has access to “on-call specialists” from the medical center’s occupational therapy, pulmonary rehabilitation, gastroenterology, otolaryngology, dermatology, neuropsychology, and dietary services who are available for consultation when needed. We have established long-term associations with one or two specialists from each discipline in order to heighten their awareness of the unique problems in their specialties that are associated with PD.
The Neurologist’s Perspective
Clinical management of the modern family with PD has become much more challenging from the physician’s perspective. The development and introduction of new technologies and medications has been accompanied by unprecedented involvement of the patients and their families in the planning and execution of overall care. Family members are much more knowledgeable, and they express their opinions and preferences at every step during the course of the disease. Modern care has therefore become a combined effort on the part of the interdisciplinary team, the patient's family and friends, and other consultants. For example, patients are looking for minimal medication-based therapy and are equally open to nonpharmacologic approaches. The focus on the patient's quality of life has been steadily increasing since the 1990s, as has the awareness and acceptance of palliative care approaches. Furthermore, families are aware of the accessibility of our multiprofessional team and frequently ask for referrals to those experts. These changes require a very different approach from the neurologist’s perspective. The neurologist must assume the position of a team member who understands and accepts the limitations of his or her knowledge in other specialty fields and must be welcoming of the participation of other team members (i.e., allied health professionals) in decision-making processes that are best for patient treatment. In addition, neurologists need to undergo a considerable shift in thinking in order to accept the option of a palliative approach in place of classical practice. Such a transition is not easy, and is one that requires the learning of new approaches by all involved, especially the neurologist, who is expected to take the leading role in these efforts. In addition to leadership skills, the neurologist must be able to develop strategies for treating PD families, and must be able to choose the team members who need to be involved in the ongoing care of that specific family. The modern PD expert must be very knowledgeable not only in the usual skills of history taking, medical management, and long-term care, but must also have a basic understanding of all aspects of the disease in order to invite the appropriate specialists to take part in the treatment as well. All neurologists in the interdisciplinary team need to shift from “diagnosis-centered” to “patient-centered” medicine. Our experience based on 18 years of working as a multidisciplinary team focused on outpatient management of PD shows that it is possible even for neurologists who have not previously had formal experience or education in sharing the provision of medical care to adopt modern approaches. We believe that accepting the professionalism of the other team members and their unique added value to the care of the PD family represents the most important step for the success of teamwork in PD centers such as ours.
The Team Members’ Interactions
The main scheduled interactions between all team members occur during:
-
1.
Twice monthly meetings to discuss potential patients who have been referred for deep brain stimulation (DBS) or those who underwent DBS and are a challenge to treat. Such meetings are chaired by the neurosurgeon, but all the unit members who are involved in the care of those patients are invited to attend. We have come to appreciate the valuable contributions of all team members to the discussion and the development of an individualized strategy for each patient.
-
2.
Twice monthly scientific update meetings involving the clinicians in the team as well as all researchers and students associated with the unit.
-
3.
A once-monthly Basal Ganglia Club, where a presentation is given by a staff member or an invited speaker on selected topics related to movement disorders.
-
4.
Twice monthly staff meetings to discuss current clinical problems as well as organizational issues.
-
5.
Weekly meeting for updating relevant team members on patients who have special problems requiring special attention or intervention.
In addition to the above, there are informal daily interactions between team members, often devoted to sharing personal and professional impressions of the various patients and their treatment. The nurse specialist is in the center of those interactions during the patient’s visit to the neurologist. She ensures that the patient’s main problems are identified and discussed with the patient, the patient’s caregiver, and the patient’s physician and nurse, and that a plan of action is agreed. It is the nurse’s role to schedule the appointments with the various specialists and to follow-up on those consults. The nurse also serves as a link between the patient/family and the specialist. When necessary, the specialist discusses the patient’s problem with other relevant team members, and the patient may be referred to other specialist services. The unit director (neurologist) and the PD nurse are informed by team members who become aware of a patient in crisis. Team members relevant to the specific problem are informed, and a meeting or a teleconference is held, and an immediate intervention is planned.
The philosophy of our interdisciplinary team is to combine our individual strengths in order to provide the greatest benefit to our patients (Fig. 1).

The interdisciplinary team interactions. MD medical doctor, psych psychiatrist, psycho psychologist, RN registered nurse, social social worker, speech/swallow speech and swallowing therapist
In parallel to the medical care, we also provide emotional support to our PD patients and their families throughout the course of the disease. Every stage requires its own interventional approach for emotional aspects. We believe that interpersonal interactions by one-on-one sessions or group therapy are superior to written materials and to Web-based information. The unit provides emotional support for patients and caregivers in three main forms:
-
1.
Long-term intervention groups: physical therapy and prevention of falls, art therapy, dance and movement therapy, and caregiver support. These groups usually meet once a week during the year, and patients may join them whenever they choose.
-
2.
Short-term intervention groups: speech therapy, virtual reality treatment while walking on the treadmill, patient support, and caregiver support. These groups have a well-defined agenda and a fixed number of participants, who have been accepted for the groups after an initial individual intake. These groups meet once a week for 5–8 weeks, and are usually led by two specialists (e.g., a nurse and a social worker, a speech and language therapist and a social worker, etc.).
-
3.
Follow-up maintenance group meetings are held once a month for people who previously participated in any of the short-term intervention groups. There are individual one-on-one meetings of the patient or the patient’s caregivers with the nurse, social worker, psychologist, psychiatrist, sexologist, occupational therapist, or physiotherapist. This kind of individual support is usually given for a limited time, frequently as part of crisis intervention or for dealing with a specific problem. Examples of triggers for focused one-on-one intervention are frequent falls, marital problems, sexual difficulties, initiation of Duodopa treatment, referral for DBS, paranoid psychosis, and institutionalization.
Conclusion
A multiprofessional team approach is the modern and preferred way to provide multimodality intervention for a disease that causes both motor and nonmotor disturbances, when a symptomatic approach is slowly replaced by palliative care. Teamwork requires a leader, and mutual respect among its members. Whereas professionalism together with open and continuous exchange of information leads to better outcomes, the multimodality approach is based on the acceptance of the concept that interdisciplinary teamwork can provide better and more comprehensive care, which, in the long run, leads to a better quality of life for our PD patients and their families.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
Lee AJ, Hardy J, Revesz T. Parkinson’s disease. Lancet. 2009;373(9680):2055–66.
Valkovic P, Abrahamova D, Hlavacka F, Benetin J. Static posturography and infraclinical postural instability in early-stage Parkinson’s disease. Mov Disord. 2009;24:1713–4.
Chaudhuri KR, Martinez-Martin P, Schapira AH, et al. International multicenter pilot study of the first comprehensive self-completed nonmotor symptoms questionnaire for Parkinson’s disease: the NMSQuest study. Mov Disord. 2006;21:916–23.
Barone P, Antonini A, Colosimo C, et al. The PRIAMO study: a multicenter assessment of nonmotor symptoms and their impact on quality of life in Parkinson’s disease. Mov Disord. 2009;24:1641–9.
Karlsen KH, Tandberg E, Arsland D, Larsen JP. Health related quality of life in Parkinson’s disease: a prospective longitudinal study. J Neurol Neurosurg Psychiatry. 2000;69:584–9.
Forsaa EB, Larsen JP, Wentzel-Larsen T, et al. Predictors and course of health-related quality of life in Parkinson’s disease. Mov Disord. 2008;23:1420–7.
Roland KP, Jenkins ME, Johnson AM. An exploration of the burden experienced by spousal caregivers of individuals with Parkinson’s disease. Mov Disord. 2010;25:189–93.
Poewe W, Mahlknecht P. The clinical progression of Parkinson’s disease. Parkinsonism Relat Disord. 2009;15 Suppl 4:S28–32.
Sinforiani E, Zangaglia R, Manni R, Cristina S, Marchioni E, Nappi G, et al. REM sleep behavior disorder, hallucinations, and cognitive impairment in Parkinson’s disease. Mov Disord. 2006;21:462–6.
Adams D, Richfield E, Johnson M, Jones E, Campbell C. A specialist palliative care service for Parkinson’s disease: review of end of life outcomes. BMJ Support Palliat Care. 2014;4 Suppl 1:A107. This article introduces the concept of palliative care in PD, which is relatively new and very important for the intervention program in advanced PD.
Rodríguez-Violante M, Camacho-Ordoñez A, Cervantes-Arriaga A, González-Latapí P, Velázquez-Osuna S. Factors associated with the quality of life of subjects with Parkinson’s disease and burden on their caregivers. Neurologia. 2014. doi:10.1016/j.nrl.2014.01.008. This article develops the concept of the involvement of caregivers in the treatment of PD patients and its relation to the quality of life.
Kalf H, Sturkenboom I, Thijssen M, de Swart B, Bloem B, Munneke M. Pursuing best practice in multidisciplinary care. EPPN J. 2008;14:12–5.
Gibberd FB, Page NG, Spencer KM, Kinnear E, Hawksworth JB. Controlled trial of physiotherapy and occupational therapy for Parkinson’s disease. Br Med J (Clin Res Ed). 1981;282(6271):1196.
van der Marck MA, Kalf JG, Sturkenboom IH, Nijkrake MJ, Munneke M, Bloem BR. Multidisciplinary care for patients with Parkinson’s disease. Parkinsonism Relat Disord. 2009;15 Suppl 3:S219–23.
Post B, van der Eijk M, Munneke M, Bloem BR. Multidisciplinary care for Parkinson’s disease: not if, but how! Pract Neurol. 2011;11(2):58–61. This article stresses the importance of the early involvement of multidisciplinary care in the course of PD.
van der Marck MA. The many faces of Parkinson ’s disease: towards a multifaceted approach? Doctoral thesis. Donders Institute, Radboud University Nijmegen. 2013. This thesis explains the effectiveness of the multimodal approach to the management of PD in accordance with the different clinical symptoms of the disease.
Dorsey ER, George BP, Leff B, Willis AW. The coming crisis: obtaining care for the growing burden of neurodegenerative conditions. Neurology. 2013;80(21):1989–96. doi:10.1212/WNL.0b013e318293e2ce.
Frazzitta G, Bertotti G, Riboldazzi G, Turla M, Uccellini D, Boveri N, et al. Effectiveness of intensive inpatient rehabilitation treatment on disease progression in parkinsonian patients: a randomized controlled trial with 1-year follow-up. Neurorehabil Neural Repair. 2012;26(2):144–50. doi:10.1177/1545968311416990.
Evans JR, Mason SL, Williams-Gray CH, Foltynie T, Brayne C, Robbins TW, et al. The natural history of treated Parkinson’s disease in an incident, community based cohort. J Neurol Neurosurg Psychiatry. 2011;82:1112–8.
Troeung L, Egan SJ, Gasson N. A waitlist-controlled trial of group cognitive behavioural therapy for depression and anxiety in Parkinson’s disease. BMC Psychiatr. 2014;14:19. doi:10.1186/1471-244X-14-19.
Keus SH, Oude Nijhuis LB, Nijkrake MJ, Bloem BR, Munneke M. Improving community healthcare for patients with Parkinson’s disease: the Dutch model. Parkinsons Dis. 2012. doi:10.1155/2012/543426.
Giladi N. Multidisciplinary team work can improve the care of families with Parkinson’s disease. Touch Medical Media. 2011. http://www.touchneurology.com/articles/multidisciplinary-team-work-can-improve-care-families-parkinson-s-disease. This article provides a brief review of the multiprofessional teamwork model of the Movement Disorders Unit at Tel Aviv Sourasky Medical Center.
Keus SH, Bloem BR, Hendriks EJ, Bredero‐Cohen AB, Munneke M. Evidence‐based analysis of physical therapy in Parkinson’s disease with recommendations for practice and research. Mov Disord. 2007;22(4):451–60.
Acknowledgments
The authors acknowledge the support of the National Parkinson Foundation Center of Excellence funding which supported the programs reviewed in this article.
Compliance with Ethics Guidelines
ᅟ
Conflict of Interest
Nir Giladi declares the receipt of fees for providing expert testimony for GlaxoSmithKline about impulse control disturbances in Parkinson’s disease, the receipt of grant money, paid to his institution, from the Michael J. Fox Foundation, the National Parkinson Foundation, the European Union Seventh Framework Programme, the Israel Science Foundation, and TEVA Innovative, and the receipt of honoraria from Teva-Lundbeck, Novartis, UCB, and MDS.
Yael Manor declares the receipt of travel expense reimbursement from the World Parkinson Congress (2013, Montreal, Canada).
Ariela Hilel declares the receipt of travel expense reimbursement from the World Parkinson Congress (2013, Montreal, Canada).
Tanya Gurevich declares the receipt of grants, paid to her institution, from the Michael J. Fox Foundation and the National Parkinson Foundation, as well as the receipt of travel expense reimbursement from the World Parkinson Congress in 2013 and the Movement Disorders Congress in 2013 and 2014.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is part of the Topical Collection on Movement Disorders
Rights and permissions
About this article

Cite this article
Giladi, N., Manor, Y., Hilel, A. et al. Interdisciplinary Teamwork for the Treatment of People with Parkinson’s Disease and Their Families. Curr Neurol Neurosci Rep 14, 493 (2014). https://doi.org/10.1007/s11910-014-0493-1
Published:
DOI: https://doi.org/10.1007/s11910-014-0493-1