
Abstract
Purpose of Review
Transplant recipients are at risk for cytomegalovirus (CMV) infection and associated morbidity and mortality. We summarize recently introduced or currently investigated modalities for prevention and treatment of CMV infection in hematopoietic cell (HCT) and solid organ transplant (SOT) recipients.
Recent Findings
Letermovir was recently approved for CMV prevention in HCT recipients. Data from real world studies support its role to improve outcomes in this population. Letermovir is currently under investigation for broader patient populations and indications. Maribavir is in late stages of development for CMV treatment and may provide a safer alternative to currently available anti-CMV drugs. Promising CMV vaccine candidates and adoptive cell therapy approaches are under evaluation. CMV immune monitoring assays are predicted to play a more central role in our clinical decision making.
Summary
In recent years, major advances have been made in CMV prevention and treatment in transplant recipients. Rigorous research is ongoing and is anticipated to further impact our ability to improve outcomes in this population.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Cytomegalovirus (CMV) infection is the most significant viral infection in hematopoietic cell and solid organ transplant recipients and is associated with increased mortality [1,2,3,4]. In addition to the direct impact of CMV end-organ disease (EOD), CMV is associated with increased incidence of opportunistic infections, graft-versus-host disease (GVHD) in hematopoietic cell transplant (HCT) recipients [5], allograft loss in solid organ transplant (SOT) recipients [6], and immune tolerance in liver transplantation [7].
A major recent advance in the field is the FDA approval of letermovir (Prevymis™) for CMV prevention in HCT recipients in November 2017 [8]. In the therapeutic area, two phase 3 studies of Maribavir for treatment of CMV are more than half accrued. In the diagnostic area, several assays measuring CMV cell mediated immunity are available as an adjunct tool to guide clinical decisions [9]. Progress has also been made in the standardization of the quantitation of CMV viral load [10], and the acceptance of CMV viral load as a surrogate endpoint by the FDA is a milestone for the clinical development of future drugs for the treatment or prevention of CMV [11].
In this review, we summarize these recent advances, their clinical implications, and potential future directions.
Prophylaxis
Universal post-transplant prophylaxis with valganciclovir or ganciclovir ranging from 3 to 12 months is widely adopted for high-risk SOT recipients [12] and has demonstrated a significant reduction in the risk of CMV disease and of all-cause mortality [13]. A meta-analysis comparing prophylaxis with preemptive therapy in SOT demonstrated that prophylaxis and preemptive strategies were both effective in reducing the incidence of CMV disease; however, no direct comparison could be made [14]. In a recent multi center randomized control study in donor seropositive/recipient seronegative liver transplant recipients, patients treated preemptively had significantly less CMV disease compared to those receiving prophylactic valganciclovir [15]. In the recently published American Transplant Society guidelines for CMV management in SOT recipient, both prophylaxis and preemptive therapy are given similar grade of recommendation in various scenarios [16].
Studies demonstrating the negative impact of CMV infection on survival after HCT in the era of preemptive therapy [1, 3] provide supportive evidence that prophylaxis should be the preferred strategy in HCT. However, the toxicities of DNA polymerase inhibitors ganciclovir, valganciclovir, foscarnet, and cidofovir preclude their use as prophylaxis in HCT. Ganciclovir and valganciclovir are associated with myelosuppression [17] while foscarnet and cidofovir with nephrotoxicity and electrolyte imbalance [18, 19]. In a randomized trial in HCT, ganciclovir prophylaxis for the first 100 days failed to show a survival benefit and was associated with substantial neutropenia [20].
Over the last decade, three anti-CMV antivirals (maribavir, brincidofovir, and letermovir) have been evaluated for CMV prevention in HCT. Maribavir, an inhibitor of UL97/threonine kinase, failed to demonstrated a benefit over placebo at a dose of 100 mg BID in phase 3 trials in HCT [21] and liver transplant recipients [22]. Brincidofovir (CMX001), an orally bioavailable conjugated nucleotide analog of cidofovir also failed to show an advantage over placebo through week 24 post-HCT and was associated with unacceptable gastrointestinal toxicity [23]. Consequently, further development of brincidofovir for CMV prophylaxis or treatment was terminated.
A major advance in CMV prevention has been the approval of letermovir in November 2017. Letermovir is a first in class, highly potent, CMV-specific terminase enzyme inhibitor which inhibits CMV replication by binding to components of the terminase complex (UL51, UL56, or both) [24]. Since there is no human analogue of the CMV terminase complex, no human toxicity is predicted. In a phase 3 randomized, double blind placebo-controlled trial of CMV-seropositive HCT recipients, letermovir prophylaxis significantly reduced the risk of clinically significant CMV infection defined as initiation of preemptive therapy for viremia or CMV end-organ disease (37.5% in letermovir arm versus 60.6% in placebo arm, p < 0.001).All-cause mortality at week 24 was lower in letermovir recipients (10.2%) versus placebo (15.9%, p < 0.03). At week 48, a persistent numerical survival advantage was found for letermovir recipients (20.9%) compared to placebo recipients (25.5%) though the difference was not significant. Letermovir was not associated with myelosuppression, making it feasible to start prior to neutrophil engraftment. Side effects were mild and included mainly vomiting, edema, and mild cardiac arrhythmias [25]. In a post-hoc analysis, letermovir recipients who developed clinically significant CMV infection had improved survival compared to placebo recipients [26].
In our center, adoption of letermovir prophylaxis has drastically reduced the need for preemptive therapy for CMV even in high-risk patients such as recipients of cord blood or T cell depleted allografts. Patients on letermovir require the addition of acyclovir for prevention of herpes simplex virus and Varicella zoster virus. Letermovir is an inducer of cytochrome P450 (CYP)3A, and an inhibitor of CYP2C8 and organic anion transporting polypeptide (OATP)1B and therefore increases the levels of calcineurin inhibitors (CNI) [27]. Dose modification is established for patients receiving cyclosporin A. In our clinical experience, the increase in CNI levels is mild and compensated for by adjusting doses of CNI based on levels, which is the standard of care.
Emergence of resistance during letermovir prophylaxis was rare in the phase 3 study and mapped on codons 231 to 369 of the UL56 gene [28]. The mutation C325Y has been reported in clinical isolates [29]. These mutations are not associated with cross-resistance to other CMV-antivirals. Genotypic assays for detection of letermovir resistance have become available, and continued vigilance is required to assess the frequency and circumstances under which resistance emerges in the real-world setting.
In the phase 3 study, patients that developed CMV infection after discontinuing letermovir had baseline risk factors such as HLA-mismatched donor, umbilical cord blood or T cell-depleted allograft or graft versus host disease (GVHD) requiring immunosuppression [30] providing supportive evidence that prolonged prophylaxis may be beneficial for these patients. A randomized study is currently accruing to evaluate the benefit of letermovir prophylaxis for 3 versus 6 months in high-risk patients (NCT03930615). Letermovir prophylaxis is also currently being evaluated in other populations including a phase 2 open label study in pediatric HCT (NCT03940586), and a phase 3 randomized study with valganciclovir as comparator in kidney transplant recipients (NCT03443869).
Another potential use of letermovir is in secondary prophylaxis for patients that require CMV suppression after completing preemptive therapy. A small observational study of 35 high-risk patients showed promising results [31]. We are currently conducting a single-center phase 2 study of letermovir as secondary prophylaxis at our institution.
Vaccines
While vaccination is an attractive strategy in transplantation, patients who will benefit most from vaccines are those that are least likely to respond to vaccines (for example recipients of T cell depleted HCT or those with GVHD and immune suppression). Protective immunity may differ between HCT and SOT recipients. Neutralizing antibodies prevent cell to cell CMV transmission and thus, are important in prevention of primary infection and are likely important for CMV protection in donor seropositive/recipient seronegative SOT recipients. The CMV envelope glycoprotein gB plays a role in host cell entry, cell to-cell virus transmission, and fusion of infected cells [32]. In liver and kidney transplant recipients, a gB targeted vaccine showed similar rates of viremia compared to placebo but increased anti-gB levels which were correlated with decreased duration of viremia and shortened treatment duration [33]. The protective effect elicited by the gB vaccine may not be dependent solely on neutralizing antibodies [34].
In HCT, CMV-specific T cells are required for protective immunity [35]. While the exact target repertoire is not well defined, presence of EI- and pp65- specific T cells correlates with protection [36].
The ASP0113, a bivalent plasmid-DNA vaccine composed of two plasmids encoding pp65 and gB failed to show a benefit over placebo in HCT or SOT recipients [37] and has not been developed further.
The CMV PepVax is a chimeric peptid-based vaccine composed of covalently linked pp65 and the helper T cell epitope P2 (from tetanus toxin), adjuvanted with PF03512676 (a Toll-like receptor 9 agonist). In a phase 1b randomized trial of CMV-seropositive HCT recipients, the vaccine was safe and well tolerated and achieved virologic endpoints and relapse-free survival [38]. A larger phase 2 placebo-controlled trial of PepVax in HCT is ongoing (NCT02396134).
The Triplex CMV vaccine is based on a modified vaccinia Ankara (MVA) vector encoding three full-length highly recognized CMV antigens: pp65, IE1-exon4, and IE2-exon5. Safety and tolerability was demonstrated in healthy adults [39] and clinical trials are ongoing in HCT recipients and donors.
The HB-101 vaccine is based on a recombinant lymphocytic choriomeningitis virus (rLCMV) vector expressing pp65 and a truncated isoform of gB. A randomized, placebo-controlled phase 2 trial in donor seropositive/recipient seronegative kidney transplant candidates is currently ongoing (NCT03629080). Ongoing vaccine studies are summarized on Table 1.
Treatment
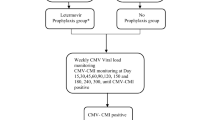
Preemptive therapy (PET) has been the most common approach to CMV management in HCT and has effectively reduced rates of CMV end-organ disease and associated mortality [40, 41]. CMV viral load thresholds for initiation of PET are not well established; however, most centers use a risk-adapted approach where PET is initiated at lower viral loads for high-risk patients (mismatched donors or receipt of T cell depleting agents). Although currently available antivirals are effective for CMV treatment, safer alternatives are needed.
Maribavir is currently in clinical trials for CMV treatment. Maribavir, a CMV selective inhibitor of UL97 threonine kinase, interferes with viral synthesis, packaging, and egress of virions from the nucleus [42]. Maribavir has an excellent oral bioavailability and is not associated with myelosuppression or nephrotoxicity [43]. Two recently completed studies of maribavir (dosing from 400 to 1200 mg BID) have shown promising results for treatment of CMV in HCT and SOT. For preemptive treatment, maribavir had comparable efficacy with valganciclovir. Twenty-two percent (22/98) of those in the maribavir arm versus 18% (5/28) in the valganciclovir arm developed CMV recurrence. There were more GI adverse events (23%) and dysgeusia (40%) in the maribavir arm compared with valganciclovir (10–15% and 3%, respectively). In contrast, neutropenia was less common in the maribavir (5%) versus valganciclovir arm (18%) [44]. A phase 3 study in HCT recipients is currently ongoing (NCT02927067).
Treatment of resistant CMV
The terms “resistant” or “refractory” CMV infection are used in clinical practice for infections that fail to respond to commercially available antivirals. CMV anti-viral resistance ranges from 1 to14% in certain high-risk HCT recipients [45]. Similar rates have been reported in SOT recipients [46]. Mortality rates are high in patients with resistant CMV [47, 48]. Recently, consensus definitions of resistant and refractory CMV were established [49]. In most patients with ganciclovir resistance, mutations are present on the UL97 kinase clustered at codons 460, 520, and 590 to 607 [50]. CMV that is ganciclovir resistant due to mutations in UL97 remains susceptible to foscarnet and cidofovir. Viral UL54 DNA polymerase gene mutations can confer cross-resistance to the traditional CMV polymerase inhibitors ganciclovir, foscarnet, and cidofovir. UL54 mutations cluster in certain functional domains resulting in distinct resistance phenotypes [50]. In general, mutations conferring ganciclovir and cidofovir cross-resistance map to the exonuclease and thumb domains and do not confer foscarnet cross resistance [51]. In contrast, foscarnet resistance mutations tend to cluster in different structure domains, typically confer 3–5-fold increase in IC50 and may confer a low-grade ganciclovir ± cidofovir cross-resistance [50].
In a phase 2 study, maribavir showed promising results for treatment of resistant or refractory (R/R) CMV in HCT or SOT recipients. Overall, 67% of patients with R/R CMV achieved virologic suppression within 6 weeks of treatment. Of these, 35% had a recurrent CMV infection. UL97 mutations conferring maribavir resistance were found in a substantial proportion of patients who developed recurrence while on maribavir. Recurrence was more common in patients with continued immunosuppression underscoring the importance of immune recovery for long-term protection from CMV [52]. A phase 3 study comparing maribavir to the best available treatment in transplant recipients with R/R CMV is approximately 70% accrued at this time (NCT02931539).
The clinical experience with letermovir for treatment is limited. Small proof of concept studies and case reports has shown a virologic effect [53, 54]. A low genetic barrier to resistance was observed in vitro [28] raising concerns about emergence of resistance in a setting of high-grade viral replication. Case series of HCT and SOT recipients with refractory CMV, using variable doses and duration of letermovir, showed mixed virologic and clinical responses and emergence of resistance [55, 56]. A study of letermovir treatment for patients experiencing refractory or resistant CMV infection or disease with concurrent organ dysfunction is ongoing (NCT03728426).
Adoptive Cytotoxic T Cells (CTL) Immune Therapy
Lack of CMV-specific T cells is a risk factor for CMV disease [57], and restoration of CMV T cell immunity correlated with protection against CMV disease [58]. Multiple studies have provided proof of concept that adoptive cell therapy can restore CMV immunity using a variety of cellular products, for different indications (prophylaxis vs. preemptive therapy vs. treatment of CMV disease) in diverse HCT types. The lack of appropriate control groups in these studies preclude comparisons and limit the applicability in the clinical setting. In addition, logistic hurdles and cost of cellular therapy are considerable [59,60,61]. Ongoing clinical trials are summarized in Table 1.
CMVpp65-specific donor-derived CTLs given for preemptive therapy along with antiviral therapy in high-risk haplo-identical HCT recipients reduced the risk of persistent and late CMV infection and improved 1-year overall survival compared to matched controls [62].
An alternative approach to donor-derived CTL is “third party” CTL generated from unrelated donors partially matched to the recipient. A bank of cellular products covering the most common HLA alleles could provide “off the shelf” cellular therapy.
In a small study from our center, 73.3% patients responded to third party CMV-CTL [63]. Unlike donor-derived CTL that may persist in the recipient for up to 10 years, third-party T cells do not achieve durable engraftment and are commonly detected only for about 90 days post administration. Thus, multiple infusions may be required to maintain therapeutic effect [64].
Studies of third party CTL with specificity against multiple viruses (EBV, CMV, adenovirus, HHV-6, and BK) have also showed safety and efficacy in small uncontrolled studies in HCT recipients [65] and several prospective multicenter trials are in progress.
The therapeutic use of CTLs has been less extensively studied in SOT recipients. CMV-specific T cell response is often attenuated due to immunosuppressive therapy, and the importance of CMV immune-reconstitution has been demonstrated in this population [66]. SOT recipients are not tolerant to donor-derived CTL [67]; nevertheless, successful treatment of resistant/refractory CMV infection in SOT recipients with CMV-specific CTLs has been demonstrated in case reports [68,69,70,71], and there is increasing interest in “off the shelf” CTLs using HLA-matched third-party banked cells for SOT.
Assessment of CMV Immune Reconstitution
Quantitative assessment of CMV Cell-mediated immunity (CMI) reconstitution may assist in risk stratification and enable an individualized approach for initiation or discontinuation of prophylaxis and preemptive therapy [9]. CMI assays in clinical trials are listed in Table 1.
The enzyme-linked immunosorbent spot (ELISPOT) assays quantify both CD4+ and CD8+ T cells producing IFN-γ in response to CMV by measuring IFN-γ as spot forming colony (SFC)/cells. Two ELISPOT assays (T-Track ® CMV Lophius Biosciences, Germany, and T-SPOT.CMV ®, Oxford Immunotec, UK) are currently marketed in Europe and used as a laboratory developed test (LDT) in the USA. Several recent studies in kidney transplant recipients support the clinical utility of ELISPOT assays at various time points. A positive CMI response 1 month following transplant was associated with protection against CMV reactivation [72], and a negative response has shown to predict the risk for CMV viremia at 3-month post-transplant [73, 74]. Pre-transplant evaluation of CMI using ELISPOT was highly predictive of post-transplant CMV outcomes in SOT recipients [75, 76].
In a prospective observational trial in HCT recipients, results of the ELISPOT assay correlated with clinically significant CMV infection [77].
The Quantiferon-CMV® assay (Qiagen Ltd) is a commercially available kit that uses enzyme-linked immunosorbent assay (ELISA) to detect IFN-γ secretion by CD8 T cells after peptide stimulation. It is simple and rapid and thus may be easily incorporated in clinical settings. Studies in SOT recipients support the utility of Quantiferon-CMV assay to predict risk for CMV disease [78, 79], assist in decision making for safe discontinuation of antiviral treatment [80], and optimize duration of prophylaxis in lung transplant recipients [81]. A study is ongoing to evaluate the utility of Quantiferon-CMV as a tool to guide administration of primary prophylaxis (NCT02784756).
Limitations of the IFN-γ-based assays include the difficulty to interpret the results in cases of negative mitogen controls representing T helper cell activity [82], but the utility of these assays in these cases merits further evaluation. IFN-γ-based assays cannot be performed in profoundly lymphopenic patients.
Intracellular cytokine staining (ICS) provides functional immunophenotyping and can detect multiple cytokines and cell surface markers and differentiate T cell phenotypes [83,84,85,86]. Until recently, ICS was only available in research setting. Currently an ICS-based assay is offered by Viracor (Eurofins, Lee’s Summit, MO, USA), and two clinical trials to evaluate its clinical use in SOT are ongoing (NCT03924219, NCT01558037).
In summary, a growing clinical experience to date supports the clinical utility of CMV monitoring immune assays as an adjunct tool in the management of CMV in transplantation. Controlled studies are critical for validation of these assays, establishing relevant cut offs and determining optimal frequency of monitoring and the type of assay best suited for each patient population.
Summary
It has taken a village of scientists, clinicians, and industry over 30 years to catch up with the “troll of transplantation”. The year 2019 is an exciting time for CMV. After more than two decades of no new anti-CMV antivirals, letermovir, a first in class, CMV-terminase inhibitor, was approved for CMV prevention in HCT recipients. Real-world data to date supports the efficacy of letermovir in preventing CMV infection without any new safety concerns. Letermovir provides us a powerful tool to assess the impact of CMV prevention on long-term outcomes such as survival beyond the duration of prophylaxis [26].
Maribavir is in late stages of development for CMV treatment and may provide a safer alternative to DNA polymerase inhibitors for treatment of CMV. Promising CMV vaccine candidates and adoptive cell therapy approaches are under evaluation. The optimal way to incorporate cellular therapies in the era of letermovir remains open. CMV immune monitoring assays are predicted to play a more central role in our clinical decisions. The ultimate challenge will be to close the survival gap of disadvantaged CMV R/D serostatus in transplantation. While there will be challenges along the way, the outlook is clearly positive for CMV in transplantation.
References
Teira P, Battiwalla M, Ramanathan M, Barrett AJ, Ahn KW, Chen M, et al. Early cytomegalovirus reactivation remains associated with increased transplant-related mortality in the current era: a CIBMTR analysis. Blood. 2016;127(20):2427–38 [cited 2019 Jul 4]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/26884374.
Fisher RA. Cytomegalovirus infection and disease in the new era of immunosuppression following solid organ transplantation. Transpl Infect Dis. 2009;11(3):195–202. https://doi.org/10.1111/j.1399-3062.2009.00372.x.
Green ML, Leisenring W, Xie H, Mast TC, Cui Y, Sandmaier BM, et al. Cytomegalovirus viral load and mortality after haemopoietic stem cell transplantation in the era of pre-emptive therapy: a retrospective cohort study. Lancet Haematol. 2016;3(3):e119–27 [cited 2019 Jul 4]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/26947200.
Sagedal S, Hartmann A, Nordal KP, Osnes K, Leivestad T, Foss A, et al. Impact of early cytomegalovirus infection and disease on long-term recipient and kidney graft survival. Kidney Int. 2004;66(1):329–37 [cited 2019 Sep 3]. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0085253815500355.
Chan ST, Logan AC. The clinical impact of cytomegalovirus infection following allogeneic hematopoietic cell transplantation: why the quest for meaningful prophylaxis still matters. Blood Rev. 2017;31(3):173–83 [cited 2019 Jul 4]. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0268960X16300492.
Stern M, Hirsch H, Cusini A, van Delden C, Manuel O, Meylan P, et al. Cytomegalovirus serology and replication remain associated with solid organ graft rejection and graft loss in the era of prophylactic treatment. Transplantation. 2014;98(9):1013–8 [cited 2019 Jul 4]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/24837540.
Litjens NHR, van der Wagen L, Kuball J, Kwekkeboom J. Potential beneficial effects of cytomegalovirus infection after transplantation. Front Immunol. 2018;9:389 [cited 2019 Jul 4]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/29545802.
Merck Sharp & Dohme Corp. PREVYMIS™ (Letermovir) Prescribing Information. [cited 2019 Jul 9]. Available from: www.fda.gov/medwatch.
Yong MK, Lewin SR, Manuel O. Immune monitoring for CMV in transplantation. Curr Infect Dis Rep. 2018;20(4):4 [cited 2019 Jul 6]. Available from: http://springerlink.bibliotecabuap.elogim.com/10.1007/s11908-018-0610-4.
Preiksaitis JK, Hayden RT, Tong Y, Pang XL, Fryer JF, Heath AB, et al. Are we there yet? Impact of the first international standard for cytomegalovirus DNA on the harmonization of results reported on plasma samples. Clin Infect Dis. 2016;63(5):583–9 [cited 2019 Jul 9]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/27307504.
Food and Drug Administration (FDA), Center for Drug Evaluation and Research (CDER). Cytomegalovirus in Transplantation: Developing Drugs to Treat or Prevent Disease Guidance for Industry DRAFT GUIDANCE. 2018. [cited 2019 Jul 11]. Available from: https://www.fda.gov/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/default.htm.
Kotton CN, Kumar D, Caliendo AM, Huprikar S, Chou S, Danziger-Isakov L, et al. The third International Consensus Guidelines on the management of cytomegalovirus in solid-organ transplantation. Transplantation. 2018;102(6):900–31 [cited 2019 Jul 4]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/29596116.
Hodson EM, Ladhani M, Webster AC, Strippoli GF, Craig JC. Antiviral medications for preventing cytomegalovirus disease in solid organ transplant recipients. Cochrane Database Syst Rev. 2013. https://doi.org/10.1002/14651858.CD003774.pub4.
Owers DS, Webster AC, Strippoli GF, Kable K, Hodson EM. Pre-emptive treatment for cytomegalovirus viraemia to prevent cytomegalovirus disease in solid organ transplant recipients. Cochrane Database Syst Rev. 2013;(2):CD005133 [cited 2019 Jul 4]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/23450558.
Singh N, Winston D, Razonable RR, Lyon III GM, Silveira FP, Wagener M, et al. Preemptive therapy (PET) vs. prophylaxis for prevention of cytomegalovirus (CMV) disease in high-risk donor seropositive/recipient seronegative (D+R−) liver transplant recipients (LTR): A NIH-sponsored, randomized, controlled, multicenter trial. In: Open Forum Infectious Diseases. Idsa; 2018 [cited 2019 Sep 3]. p. S766–S766. Available from: https://idsa.confex.com/idsa/2018/webprogram/Paper74389.html.
Razonable RR, Humar A. Cytomegalovirus in solid organ transplant recipients—guidelines of the American Society of Transplantation Infectious Diseases Community of Practice. Clin Transplant. 2019:e13512 [cited 2019 Sep 3]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/30817026.
Kalil AC, Freifeld AG, Lyden ER, Stoner JA. Valganciclovir for cytomegalovirus prevention in solid organ transplant patients: an evidence-based reassessment of safety and efficacy. Chêne G, editor. PLoS One 2009;4(5):e5512. https://doi.org/10.1371/journal.pone.0005512.
Hirsch HH, Steiger J. Polyomavirus BK. Lancet Infect Dis. 2003;3(10):611–23 [cited 2019 Feb 20]. Available from: http://linkinghub.elsevier.com/retrieve/pii/S1473309903007709.
Bueno J, Ramil C, Green M. Current management strategies for the prevention and treatment of cytomegalovirus infection in pediatric transplant recipients. Pediatr Drugs. 2002;4(5):279–90 [cited 2019 Jul 4]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/11994033.
Goodrich JM, Bowden RA, Fisher L, Keller C, Schoch G, Meyers JD. Ganciclovir prophylaxis to prevent cytomegalovirus disease after allogeneic marrow transplant. Ann Intern Med. 1993;118(3):173 [cited 2019 Jul 11]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/8380242.
Marty FM, Ljungman P, Papanicolaou GA, Winston DJ, Chemaly RF, Strasfeld L, et al. Maribavir prophylaxis for prevention of cytomegalovirus disease in recipients of allogeneic stem-cell transplants: a phase 3, double-blind, placebo-controlled, randomised trial. Lancet Infect Dis. 2011;11(4):284–92 [cited 2019 Jul 5]. Available from: https://linkinghub.elsevier.com/retrieve/pii/S147330991170024X.
Winston DJ, Saliba F, Blumberg E, Abouljoud M, Garcia-Diaz JB, Goss JA, et al. Efficacy and safety of maribavir dosed at 100 mg orally twice daily for the prevention of cytomegalovirus disease in liver transplant recipients: a randomized, double-blind, multicenter controlled trial. Am J Transplant. 2012;12(11):3021–30. https://doi.org/10.1111/j.1600-6143.2012.04231.x.
Marty FM, Winston DJ, Chemaly RF, Mullane KM, Shore TB, Papanicolaou GA, et al. A randomized, double-blind, placebo-controlled phase 3 trial of oral brincidofovir for cytomegalovirus prophylaxis in allogeneic hematopoietic cell transplantation. Biol Blood Marrow Transplant. 2019;25(2):369–81 [cited 2019 Jul 5]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/30292744.
Lischka P, Hewlett G, Wunberg T, Baumeister J, Paulsen D, Goldner T, et al. In vitro and in vivo activities of the novel anticytomegalovirus compound AIC246. Antimicrob Agents Chemother. 2010;54(3):1290–7 [cited 2019 Jul 5]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/20047911.
Marty FM, Ljungman P, Chemaly RF, Maertens J, Dadwal SS, Duarte RF, et al. Letermovir prophylaxis for cytomegalovirus in hematopoietic-cell transplantation. N Engl J Med. 2017;377(25):2433–44 [cited 2019 Jul 5]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/29211658.
Ljungman P, Schmitt M, Marty FM, Maertens J, Chemaly RF, Kartsonis NA, et al. A mortality analysis of letermovir prophylaxis for cytomegalovirus (CMV) in CMV-seropositive recipients of allogeneic hematopoietic-cell transplantation. Clin Infect Dis. 2019; [cited 2019 Jul 5]; Available from: http://www.ncbi.nlm.nih.gov/pubmed/31179485.
Kropeit D, von Richter O, Stobernack H-P, Rübsamen-Schaeff H, Zimmermann H. Pharmacokinetics and safety of letermovir coadministered with cyclosporine A or tacrolimus in healthy subjects. Clin Pharmacol Drug Dev. 2018;7(1):9–21. https://doi.org/10.1002/cpdd.388.
Rapid CS. In Vitro evolution of human cytomegalovirus UL56 mutations that confer letermovir resistance. Antimicrob Agents Chemother. 2015;59(10):6588–93 [cited 2019 Jul 9]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/26259791.
Cherrier L, Nasar A, Goodlet KJ, Nailor MD, Tokman S, Chou S. Emergence of letermovir resistance in a lung transplant recipient with ganciclovir-resistant cytomegalovirus infection. Am J Transplant. 2018;18(12):3060–4. https://doi.org/10.1111/ajt.15135.
Hodowanec A, Komatsu T, Singer M, Smith F, Valappil T, O’Rear JMJBD. Late Cmv Infection Following Letermovir Prophylaxis in Allogeneic Hematopoietic Stem Cell Transplant Recipients. In: American Transplant Congress, Seattle Washington, June 8, 2018 [Internet]. [cited 2019 Jul 10]. Available from: https://atcmeeting.org/abstracts.
Robin C, Ducastelle-Lepretre S, Thiebaut A, de la Tour RP, Ceballos P, Masure M, et al. Letermovir for prophylaxis of cytomegalovirus (CMV) infection or disease in allogeneic hct recipients: experience of secondary prophylaxis in the French compassionate program. Bone Marrow Transplant. 2019;54(S1):144–619 [cited 2019 Jul 9]. Available from: http://www.nature.com/articles/s41409-019-0559-4.
McVoy MA. Cytomegalovirus vaccines. Clin Infect Dis. 2013;57(suppl_4):S196–9 [cited 2019 Jul 5]. Available from: http://academic.oup.com/cid/article/57/suppl_4/S196/494333/Cytomegalovirus-Vaccines.
Griffiths PD, Stanton A, McCarrell E, Smith C, Osman M, Harber M, et al. Cytomegalovirus glycoprotein-B vaccine with MF59 adjuvant in transplant recipients: a phase 2 randomised placebo-controlled trial. Lancet. 2011;377(9773):1256–63 [cited 2019 Jul 5]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/21481708.
Baraniak I, Kropff B, Ambrose L, McIntosh M, McLean GR, Pichon S, et al. Protection from cytomegalovirus viremia following glycoprotein B vaccination is not dependent on neutralizing antibodies. Proc Natl Acad Sci U S A. 2018;115(24):6273–8 [cited 2019 Jul 5]. Available from: http://www.pnas.org/lookup/doi/10.1073/pnas.1800224115.
Smith L, Wloch M, Chaplin J, Gerber M, Rolland A, Smith LR, et al. Clinical development of a cytomegalovirus DNA vaccine: from product concept to pivotal phase 3 trial. Vaccines. 2013;1(4):398–414 [cited 2019 Jul 9]. Available from: http://www.mdpi.com/2076-393X/1/4/398.
Diamond DJ, La Rosa C, Chiuppesi F, Contreras H, Dadwal S, Wussow F, et al. A fifty-year odyssey: prospects for a cytomegalovirus vaccine in transplant and congenital infection. Expert Rev Vaccines. 2018;17(10):889–911 [cited 2019 Jul 5]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/30246580.
Ávila SG, Gaminde AI, Escamilla MS. EBMT Abstracts 2019 Infectious complications. 2019.
Nakamura R, La Rosa C, Longmate J, Drake J, Slape C, Zhou Q, et al. Viraemia, immunogenicity, and survival outcomes of cytomegalovirus chimeric epitope vaccine supplemented with PF03512676 (CMVPepVax) in allogeneic haemopoietic stem-cell transplantation: randomised phase 1b trial. Lancet Haematol. 2016;3(2):e87–98 [cited 2019 Jul 5]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/26853648.
La Rosa C, Longmate J, Martinez J, Zhou Q, Kaltcheva TI, Tsai W, et al. MVA vaccine encoding CMV antigens safely induces durable expansion of CMV-specific T cells in healthy adults. Blood. 2017;129(1):114–25 [cited 2019 Jul 5]. Available from: http://www.bloodjournal.org/lookup/doi/10.1182/blood-2016-07-729756.
Pollack M, Heugel J, Xie H, Leisenring W, Storek J, Young J-A, et al. An international comparison of current strategies to prevent herpesvirus and fungal infections in hematopoietic cell transplant recipients. Biol Blood Marrow Transplant. 2011;17(5):664–73 [cited 2019 Jul 4]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/20699126.
Boeckh M, Bowden RA, Gooley T, Myerson D, Corey L. Successful modification of a pp65 antigenemia-based early treatment strategy for prevention of cytomegalovirus disease in allogeneic marrow transplant recipients. Blood. 1999;93(5):1781–2 [cited 2019 Jul 4]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/10084817.
Biron KK, Harvey RJ, Chamberlain SC, Good SS, Smith AA, Davis MG, et al. Potent and selective inhibition of human cytomegalovirus replication by 1263W94, a benzimidazole L-riboside with a unique mode of action. Antimicrob Agents Chemother. 2002;46(8):2365–72 [cited 2019 Jul 5]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/12121906.
Koszalka GW, Johnson NW, Good SS, Boyd L, Chamberlain SC, Townsend LB, et al. Preclinical and toxicology studies of 1263W94, a potent and selective inhibitor of human cytomegalovirus replication. Antimicrob Agents Chemother. 2002;46(8):2373–80 [cited 2019 Jul 5]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/12121907.
Maertens J, Cordonnier C, Jaksch P, Poiré X, Wu JJ, Wijatyk A, et al. Maribavir versus valganciclovir for preemptive treatment of cytomegalovirus (CMV) viremia: a randomized, dose-ranging, phase 2 study among hematopoietic stem cell transplant (SCT) and solid organ transplant (SOT) recipients. In Idsa; 2016. [cited 2019 Jul 5]. Available from: https://idsa.confex.com/idsa/2016/webprogram/Paper56176.html.
Shmueli E, Or R, Shapira MY, Resnick IB, Caplan O, Bdolah-Abram T, et al. High rate of cytomegalovirus drug resistance among patients receiving preemptive antiviral treatment after haploidentical stem cell transplantation. J Infect Dis. 2014;209(4):557–61 [cited 2019 Jul 4]. Available from: https://academic.oup.com/jid/article-lookup/doi/10.1093/infdis/jit475.
Van Leer Buter CC, de Voogd DWK, Blokzijl H, de Joode AAE, Berger SP, Verschuuren EAM, et al. Antiviral-resistant cytomegalovirus infections in solid organ transplantation in the Netherlands. J Antimicrob Chemother. 2019; [cited 2019 Jul 4]. Available from: https://academic.oup.com/jac/advance-article/doi/10.1093/jac/dkz196/5489804.
Minces LR, Nguyen MH, Mitsani D, Shields RK, Kwak EJ, Silveira FP, et al. Ganciclovir-resistant cytomegalovirus infections among lung transplant recipients are associated with poor outcomes despite treatment with foscarnet-containing regimens. Antimicrob Agents Chemother. 2014;58(1):128–35 [cited 2019 Jul 9]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/24145525.
Limaye AP. Ganciclovir-resistant cytomegalovirus in organ transplant recipients. Clin Infect Dis. 2002;35(7):866–72 [cited 2019 Jul 9]. Available from: https://academic.oup.com/cid/article-lookup/doi/10.1086/342385.
Chemaly RF, Chou S, Einsele H, Griffiths P, Avery R, Razonable RR, et al. Definitions of Resistant and refractory cytomegalovirus infection and disease in transplant recipients for use in clinical trials. Clin Infect Dis. 2019;68(8):1420–6 [cited 2019 Jul 9]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/30137245.
Chou S. Approach to drug-resistant cytomegalovirus in transplant recipients. Curr Opin Infect Dis. 2015;28(4):293–9 [cited 2019 Jul 9]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/26098499.
El Chaer F, Shah DP, Chemaly RF. How I treat resistant cytomegalovirus infection in hematopoietic cell transplantation recipients. Blood. 2016;128(23):2624–36 [cited 2019 Jul 9]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/27760756.
Papanicolaou GA, Silveira FP, Langston AA, Pereira MR, Avery RK, Uknis M, et al. Maribavir for refractory or resistant cytomegalovirus infections in hematopoietic-cell or solid-organ transplant recipients: a randomized, dose-ranging, double-blind, phase 2 study. Clin Infect Dis. 2019;68(8):1255–64 [cited 2019 Jul 5]. Available from: https://academic.oup.com/cid/article/68/8/1255/5133438.
Stoelben S, Arns W, Renders L, Hummel J, Mühlfeld A, Stangl M, et al. Preemptive treatment of cytomegalovirus infection in kidney transplant recipients with letermovir: results of a phase 2a study. Transpl Int. 2014;27(1):77–86. https://doi.org/10.1111/tri.12225.
Kaul DR, Stoelben S, Cober E, Ojo T, Sandusky E, Lischka P, et al. First report of successful treatment of multidrug-resistant cytomegalovirus disease with the novel anti-CMV compound AIC246. Am J Transplant. 2011;11(5):1079–84. https://doi.org/10.1111/j.1600-6143.2011.03530.x.
Phoompoung P, Ferreira VH, Tikkanen J, Husain S, Viswabandya A, Kumar D, et al. Letermovir as salvage therapy for CMV infection in transplant recipients. Transplantation. 2019;1. [cited 2019 Jul 5]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/31107821.
Turner N, Strand A, Grewal DS, Cox G, Arif S, Baker AW, et al. Use of letermovir as salvage therapy for drug-resistant cytomegalovirus retinitis. Antimicrob Agents Chemother. 2019;63(3). [cited 2019 Jul 5]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/30642941.
Li CR, Greenberg PD, Gilbert MJ, Goodrich JM, Riddell SR. Recovery of HLA-restricted cytomegalovirus (CMV)-specific T-cell responses after allogeneic bone marrow transplant: correlation with CMV disease and effect of ganciclovir prophylaxis. Blood. 1994;83(7):1971–9 [cited 2019 Jul 5]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/8142663.
Riddell SR, Watanabe K, Goodrich J, Li C, Agha M, Greenberg P. Restoration of viral immunity in immunodeficient humans by the adoptive transfer of T cell clones. Science. 1992;257(5067):238–41 [cited 2019 Jul 5]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/1352912.
Feuchtinger T, Opherk K, Bethge WA, Topp MS, Schuster FR, Weissinger EM, et al. Adoptive transfer of pp65-specific T cells for the treatment of chemorefractory cytomegalovirus disease or reactivation after haploidentical and matched unrelated stem cell transplantation. Blood. 2010;116(20):4360–7 [cited 2019 Jul 5]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/20625005.
Micklethwaite KP, Clancy L, Sandher U, Hansen AM, Blyth E, Antonenas V, et al. Prophylactic infusion of cytomegalovirus-specific cytotoxic T lymphocytes stimulated with Ad5f35pp65 gene-modified dendritic cells after allogeneic hemopoietic stem cell transplantation. Blood. 2008;112(10):3974–81 [cited 2019 Jul 5]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/18768783.
Einsele H. Infusion of cytomegalovirus (CMV)-specific T cells for the treatment of CMV infection not responding to antiviral chemotherapy. Blood. 2002;99(11):3916–22 [cited 2019 Jul 5]. Available from: http://www.bloodjournal.org/cgi/doi/10.1182/blood.V99.11.3916.
Zhao X-Y, Pei X-Y, Chang Y-J, Yu X-X, Xu L-P, Wang Y, et al. First-line therapy with donor-derived HCMV-specific T cells reduces persistent HCMV infection by promoting antiviral immunity after allogenic stem cell transplantation. Clin Infect Dis. 2019. [cited 2019 Jul 5]; Available from: http://www.ncbi.nlm.nih.gov/pubmed/31067570.
Prockop S, Doubrovina E, Hasan AN, Dahi PB, Giralt S, Koehne G, et al. Third party CMV-specific cytotoxic T cells for treatment of antiviral resistant CMV infection after hematopoietic stem cell transplant. Blood. 2016;128(22). [cited 2019 Jul 5]. Available from: http://www.bloodjournal.org/content/128/22/61?sso-checked=true.
O’Reilly RJ, Prockop S, Hasan AN, Koehne G, Doubrovina E. Virus-specific T-cell banks for “off the shelf” adoptive therapy of refractory infections. Bone Marrow Transplant. 2016;51(9):1163–72 [cited 2019 Jul 5]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/27042851.
Tzannou I, Papadopoulou A, Naik S, Leung K, Martinez CA, Ramos CA, et al. Off-the-shelf virus-specific T cells to treat BK virus, human herpesvirus 6, cytomegalovirus, Epstein-Barr virus, and adenovirus infections after allogeneic hematopoietic stem-cell transplantation. J Clin Oncol. 2017;35(31):3547–57 [cited 2019 Jul 5]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28783452.
Egli A, Humar A, Kumar D. State-of-the-art monitoring of cytomegalovirus-specific cell-mediated immunity after organ transplant: a primer for the clinician. Clin Infect Dis. 2012;55(12):1678–89 [cited 2019 Jul 5]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22990848.
Kaminski H, Fishman JA. The cell biology of cytomegalovirus: implications for transplantation. Am J Transplant. 2016;16(8):2254–69. https://doi.org/10.1111/ajt.13791.
Pierucci P, Malouf M, Glanville AR, Beagley L, Smith C, Khanna R. Novel autologous T-cell therapy for drug-resistant cytomegalovirus disease after lung transplantation. J Hear Lung Transplant. 2016;35(5):685–7 [cited 2019 Jul 6]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/27083238.
Brestrich G, Zwinger S, Fischer A, Schmück M, Röhmhild A, Hammer MH, et al. Adoptive T-cell therapy of a lung transplanted patient with severe CMV disease and resistance to antiviral therapy. Am J Transplant. 2009;9(7):1679–84 [cited 2019 Jul 6]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/19459791.
Kontoyiannis DP, Patterson TF. Diagnosis and treatment of invasive fungal infections in the cancer patient: recent progress and ongoing questions. Clin Infect Dis. 2014;59(Suppl 5):S356–9 Available from: http://www.ncbi.nlm.nih.gov/pubmed/25352631.
Macesic N, Langsford D, Nicholls K, Hughes P, Gottlieb DJ, Clancy L, et al. Adoptive T cell immunotherapy for treatment of ganciclovir-resistant cytomegalovirus disease in a renal transplant recipient. Am J Transplant. 2015;15(3):827–32 [cited 2019 Jul 6]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/25648555.
Gliga S, Korth J, Krawczyk A, Wilde B, Horn PA, Witzke O, et al. T-Track-CMV and QuantiFERON-CMV assays for prediction of protection from CMV reactivation in kidney transplant recipients. J Clin Virol. 2018;105:91–6 [cited 2019 Jul 6]. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1386653218301574.
Lee H, Park KH, Ryu JH, Choi A-R, Yu JH, Lim J, et al. Cytomegalovirus (CMV) immune monitoring with ELISPOT and QuantiFERON-CMV assay in seropositive kidney transplant recipients. Akatsuka Y, editor. PLoS One. 2017;12(12):e0189488. [cited 2019 Jul 6]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/29232714.
Jarque M, Melilli E, Crespo E, Manonelles A, Montero N, Torras J, et al. CMV-specific cell-mediated immunity at 3-month prophylaxis withdrawal discriminates D+/R+ kidney transplants at risk of late-onset CMV infection regardless the type of induction therapy. Transplantation. 2018;102(11):e472–80 [cited 2019 Jul 10]. Available from: http://insights.ovid.com/crossref?an=00007890-201811000-00033.
Cantisán S, Lara R, Montejo M, Redel J, Rodríguez-Benot A, Gutiérrez-Aroca J, et al. Pretransplant interferon-γ secretion by CMV-specific CD8+ T cells informs the risk of CMV replication after transplantation. Am J Transplant. 2013;13(3):738–45. https://doi.org/10.1111/ajt.12049.
Bestard O, Crespo E, Stein M, Lúcia M, Roelen DL, de Vaal YJ, et al. Cross-validation of IFN-γ Elispot assay for measuring alloreactive memory/effector T cell responses in renal transplant recipients. Am J Transplant. 2013;13(7):1880–90 [cited 2019 Jul 6]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/23763435.
El Haddad L, Ariza-Heredia E, Shah DP, Jiang Y, Blanchard T, Ghantoji SS, et al. The ability of a cytomegalovirus ELISPOT assay to predict outcome of low-level CMV reactivation in hematopoietic cell transplant recipients. J Infect Dis. 2019;219(6):898–907 [cited 2019 Jul 10]. Available from: https://academic.oup.com/jid/article/219/6/898/5122855.
Walker S, Fazou C, Crough T, Holdsworth R, Kiely P, Veale M, et al. Ex vivo monitoring of human cytomegalovirus-specific CD8+ T-cell responses using QuantiFERON-CMV. Transpl Infect Dis. 2007;9(2):165–70. https://doi.org/10.1111/j.1399-3062.2006.00199.x.
Manuel O, Husain S, Kumar D, Zayas C, Mawhorter S, Levi ME, et al. Assessment of cytomegalovirus-specific cell-mediated immunity for the prediction of cytomegalovirus disease in high-risk solid-organ transplant recipients: a multicenter cohort study. Clin Infect Dis. 2013;56(6):817–24 [cited 2019 Jul 6]. Available from: https://academic.oup.com/cid/article-lookup/doi/10.1093/cid/cis993.
Kumar D, Mian M, Singer L, Humar A. An interventional study using cell-mediated immunity to personalize therapy for cytomegalovirus infection after transplantation. Am J Transplant. 2017;17(9):2468–73 [cited 2019 Jul 6]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28500691.
Westall GP, Cristiano Y, Levvey BJ, Whitford H, Paraskeva MA, Paul E, et al. A randomized study of quantiferon CMV-directed versus fixed-duration valganciclovir prophylaxis to reduce late CMV after lung transplantation. Transplantation. 2019;103(5):1005–13 [cited 2019 Jul 10]. Available from: http://insights.ovid.com/crossref?an=00007890-900000000-96365.
Singh N, Gayowski T, Wagener MM, Zeevi A. T-helper cell responses in liver transplant recipients: correlation with cytomegalovirus and other major infections. Transpl Infect Dis. 2004;6(2):93–6 [cited 2019 Jul 6]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/15522114.
Lilleri D, Gerna G, Zelini P, Chiesa A, Rognoni V, Mastronuzzi A, et al. Monitoring of human cytomegalovirus and virus-specific T-cell response in young patients receiving allogeneic hematopoietic stem cell transplantation. Perez-Martinez A, editor. PLoS One. 2012;7(7):e41648. https://doi.org/10.1371/journal.pone.0041648.
Lilleri D, Gerna G, Fornara C, Chiesa A, Comolli G, Zecca M, et al. Human cytomegalovirus-specific T cell reconstitution in young patients receiving T cell-depleted, allogeneic hematopoietic stem cell transplantation. J Infect Dis. 2009;199(6):829–36 [cited 2019 Jul 6]. Available from: https://academic.oup.com/jid/article-lookup/doi/10.1086/597123.
Widmann T, Sester U, Gärtner BC, Schubert J, Pfreundschuh M, Köhler H, et al. Levels of CMV specific CD4 T cells are dynamic and correlate with CMV viremia after allogeneic stem cell transplantation. Stevenson PG, editor. PLoS One. 2008;3(11):e3634. https://doi.org/10.1371/journal.pone.0003634.
Camargo JF, Wieder ED, Kimble E, Benjamin CL, Kolonias DS, Kwon D, et al. Deep functional immunophenotyping predicts risk of cytomegalovirus reactivation after hematopoietic cell transplantation. Blood. 2019;133(8):867–77 [cited 2019 Jul 10]. Available from: http://www.bloodjournal.org/lookup/doi/10.1182/blood-2018-10-878918.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Anat Stern declares that she has no conflict of interest.
Genovefa Papanicolaou has been an investigator for Astellas Pharma, Chimerix Inc., Merck & Co, and Shire and has received funding and/or other fees from Astellas Pharma, Chimerix Inc., Merck & Co, Clinigen, Ideogen, and Oxford Immunotech.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Transplant and Oncology
Rights and permissions
About this article

Cite this article
Stern, A., Papanicolaou, G.A. CMV Prevention and Treatment in Transplantation: What’s New in 2019. Curr Infect Dis Rep 21, 45 (2019). https://doi.org/10.1007/s11908-019-0699-0
Published:
DOI: https://doi.org/10.1007/s11908-019-0699-0