
Abstract
Purpose of Review
We aim to systematically review the literature on the effectiveness of pediatric antimicrobial stewardship programs (ASPs) and antimicrobial stewardship (AS) strategies in the United States (US) inpatient setting. Furthermore, we review current gaps and challenges for unique pediatric populations and those in ambulatory settings.
Recent Findings
Misuse and overuse of antimicrobials have been identified as key factors for antimicrobial resistance (AR). Multiple professional organizations support the implementation of hospital-based ASPs to decrease antimicrobial consumption, improve patient outcomes, and reduce healthcare costs. There is limited data on the effectiveness of inpatient pediatric ASPs and AS strategies in unique populations. Furthermore, there is a paucity of evidence on ASPs in ambulatory settings.
Summary
This review contributes to the growing body of evidence that supports the use of pediatric ASPs to optimize antimicrobial therapy in the inpatient setting as well as in unique patient populations and ambulatory settings. Active stewardship is critical and antimicrobial consumption is a key outcome metric for programs.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Misuse and overuse of antimicrobials have been identified as key factors for antimicrobial resistance (AR). In the setting of limited new antimicrobial agents, AR is recognized as a critical public health threat to the United States (US) and is a growing global concern threatening the achievements of modern medicine [1, 2]. From 1999 to 2012, there has been a significant increase in the prevalence of multidrug-resistant (MDR) and carbapenem-resistant Pseudomonas aeruginosa isolates in US children [3•]. The Infectious Diseases Society of America (IDSA) published landmark guidelines for the development of an effective hospital-based stewardship program based on evidence that antimicrobial stewardship programs (ASPs) reduce antimicrobial use, improve patient outcomes, and reduce healthcare costs [4]. Recommendations were largely based on studies and interventions on adult populations. Core ASP strategies identified in the guideline included formulary restriction with preauthorization and prospective audit with feedback (PAF). Antimicrobial use in hospitalized patients has been identified as an important measure of ASP effectiveness [5••].
Hospitalized pediatric and adult patients both commonly receive antimicrobials, and ample opportunities exist to optimize therapy in both patient populations. Gerber et al. [6] found that 60% of children discharged from 40 freestanding US children’s hospitals received at least one antimicrobial agent. Similarly, Pakyz et al. [7] found that 63.5% of adults discharged from 35 US academic health centers received an antimicrobial agent during hospitalization. The authors also found that antimicrobial prescribing in adult patients was increasing over time. In pediatric acute care settings, significant variation in prescribing patterns exists for conditions such as pneumonia, appendicitis, cystic fibrosis, and skin and soft tissue infections [8]. The Centers for Disease Control and Prevention (CDC) estimated that 30–50% of all antimicrobials prescribed in hospitals are suboptimal or unnecessary; however, this is primarily based on adult data [9].
A pediatric-focused ASP is imperative given the specific needs of children, which diverges from adults by varying antimicrobial dosing considerations, adverse events not commonly seen in adults, and the potential for resistance in the setting of a lifetime of antimicrobial exposure. Additionally, pharmacists and physicians with specialized training in pediatrics will likely provide more nuanced and informed antimicrobial recommendations than those without. The number of pediatric centers with formal ASPs is growing, although these programs differ widely in structure and function [10]. Hersh et al. [11•] observed an overall decrease in antimicrobial use, defined as days of therapy (DOT) per 1000 patient days (PD), across 31 freestanding children’s hospitals with or without formal ASPs, although the rate of decline was highest in those with a formalized ASP. There are limited data on the effectiveness of hospital-based pediatric ASPs. Formal recommendations do exist for ambulatory settings, although evidence on the effectiveness of these strategies is limited [12•]. A systematic review of studies published through March 2014 evaluated the effectiveness of inpatient pediatric ASPs and other supplemental antimicrobial stewardship (AS) interventions based on the following outcome measures: antimicrobial utilization, antimicrobial or healthcare costs, prescribing errors, antimicrobial resistance, patient harm, or physician satisfaction [13•]. A reduction in antimicrobial utilization was most commonly found, and where evaluated, no short-term adverse patient outcomes were identified within the study periods.
Herein, we aim to systematically review the literature on the effectiveness of pediatric ASP and AS strategies in the US inpatient setting published since 2014 using similar outcome measures to those utilized in the systematic review published by Smith et al. in 2015 [13•]. We also aim to summarize the most recent literature on AS strategies for unique pediatric populations and those in ambulatory settings as well as review current gaps and challenges for these groups.
Methods
Search Strategy
A PubMed search was performed to identify studies from April 1, 2014 to September 8, 2017 published in the English language. Search terms used alone and in combination included “antimicrobial,” “stewardship,” and “pediatric.” This was supplemented by review of references for relevant studies to identify additional articles. Searches were combined and duplicates were removed.
Study Review and Selection
We included studies that focused on specific outcomes of pediatric ASPs implemented in inpatient settings including antimicrobial utilization, healthcare costs, patient harm, or antimicrobial resistance. Studies were excluded if these were conducted outside the US, if no intervention was implemented, or if an assessment of the intervention was not completed. We divided our inpatient analysis into those studies examining comprehensive ASPs and those evaluating specific AS strategies. Studies on neonatal intensive care unit and hematology-oncology populations were not divided and were discussed separately due to the small number of studies and to review current knowledge, gaps, and challenges in these unique groups. Studies in ambulatory settings were not systematically reviewed, but pertinent current knowledge, gaps, and challenges were also summarized.
Results
Literature Search and Study Selection
Our literature search yielded 258 articles, of which 17 met the inpatient inclusion criteria, of which nine described ASPs, three described AS-based strategies, four focused solely on NICU ASPs and AS strategies, and one focused solely on an AS intervention in hematology-oncology patients (see Fig. 1). Two studies described ASPs in ambulatory settings and were used to summarize current gaps and challenges.

Literature flow diagram
Inpatient Setting: Studies Focused on Formal ASP and AS Strategies
Table 1 provides major findings of nine studies analyzing specific outcomes of inpatient pediatric-ASP interventions (excluding studies focused solely on NICU or hematology/oncology populations). Studies originated from single centers, two of which were non-freestanding children’s hospitals: Randall Children’s Hospital and New York University Langone Center; the remaining studies originated from freestanding children’s hospitals: Children’s Hospital Colorado Anschutz Medical Campus, Children’s Hospital of Pittsburgh, Children’s Hospital of Philadelphia, Monroe Carell Jr. Children’s Hospital at Vanderbilt, Le Bonheur Children’s Hospital, Children’s Hospital of Detroit, and Alfred DuPont Hospital for Children. All studies evaluated PAF, while 6/9 studies evaluated a component of antimicrobial restriction.
Antimicrobial Utilization
Seven studies reported reductions in antimicrobial utilization, measured in DOT per 1000 PD. Two studies focused on ASPs in non-freestanding children’s hospitals. Turner et al. [14•] reported on the impact of a 72-h automated PAF on antimicrobial use. Authors highlight a 16.8% overall decrease in antimicrobial DOT per 1000 PD and a 38% decrease in vancomycin use (38 to 23 DOT per 1000 PD). Lighter-Fisher et al. [15•] implemented a formal ASP with clinical practice guidelines (CPGs), a 48–72-h automated PAF, and restriction of six antimicrobials (daptomycin, polymyxin B sulfate, linezolid, tigecycline, flucytosine, and voriconazole) in a non-freestanding children’s hospital. They found a decrease in the overall aggregate median monthly antimicrobial use from 803 to 761 DOT per 1000 PD. Furthermore, an additional metric, length of therapy (LOT), was used and showed similar results.
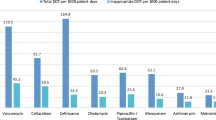
Hurst et al. [16•] also reported on antimicrobial utilization using a unique ASP strategy. The authors implemented a “handshake stewardship” program defined by lack of restriction and preauthorization, review of all prescribed antimicrobials, and a rounding-based, in-person approach to provide feedback by a pharmacist-physician team. This approach effectively reduced hospital-wide antimicrobial consumption by 10.9% (942 to 839 DOT per 1000 PD). Furthermore, the authors observed a 25.7% reduction in vancomycin use (105 to 78 DOT per 1000 PD) and a 22.2% reduction in meropenem use (45 to 35 DOT per 1000 PD).
Willis et al. [17•] implemented an ASP primarily focused on PAF, but that also included elements of prior authorization and CPG development that led to an 11.1% reduction of all parenteral antimicrobial DOT per 1000 PD. Prior to implementation, antimicrobial consumption was decreasing at a rate of 3.7%/year, which was similar to other freestanding hospitals in a large comparator group (median decline, 3.4%/year). After implementation, the median decline for the study hospital was 11.1%/year compared to 5.6%/year for other hospitals over the same time period. The authors observed that the ASP’s impact was greater than would have been expected based on secular trends.
Two studies focused on vancomycin reduction. The first study observed a 21.9% decrease in vancomycin use (114 to 89 DOT per 1000 PD) after implementation of an ASP program focused on automated PAF at 72 h [18•]. When compared with utilization at similar children’s hospitals with and without established ASPs, the authors found a significant reduction, although there was no difference in the slope of change of vancomycin DOT compared to children’s hospitals with ASPs. The second study reported a 45% decline in vancomycin use (378 to 208 DOT per 1000 PD) after implementation of PAF [19•]. Nguyen et al. [20•] observed a 25% reduction in vancomycin use (138.2 to 104.2 DOT per 1000 PD) and 31% reduction in meropenem use (20 to 13.8 per 1000 PD) after implementation of PAF, restriction, and CPGs.
Antimicrobial Costs
Three studies reported changes in antimicrobial costs after introduction of ASPs; all three studies showed decreases, although there was a variation in what the costs were attributed to. Turner et al. [14•] reported a decrease of $67,000/year in drug acquisition costs over the 2-year post-intervention period. Gillion et al. [18•] observed a reduction of pharmacy costs associated with the use of vancomycin by 41% over the 2-year post-intervention period. No quantitative monetary value was provided. Willis et al. [17•] also reported on their cost savings. After ASP implementation, monthly median expenditures for all parenteral antimicrobials decreased by $42,647/month over the 2-year post-intervention period.
Patient Harm
Three studies reported on potential adverse outcomes associated with ASP interventions; none of the studies reported any adverse outcomes. Turner et al. [14•] did not observe any difference in hospital length of stay (LOS) or in-hospital mortality 2 years following implementation of a formal ASP. Molloy et al. [21•] found similar results in addition to no change in all-cause readmission after ASP implementation of a formalized ASP. Ross et al. [22•] implemented an antimicrobial restriction strategy with an automated electronic medical record (EMR) stop order and did not observe a change in hospital mortality, LOS, or readmission rates during the study period.
Antimicrobial Resistance
One study reported on AR. Lighter-Fisher et al. [15•] observed overall stability in susceptibility patterns of common pathogens over the 4-year study period with some decreases in antimicrobial resistance in gram-negative organisms. Rates of susceptibility to piperacillin-tazobactam increased among Enterobacter cloacae and Klebsiella pneumoniae isolates pre and post implementation of a formal ASP. Authors also observed increased susceptibility rates of P. aeruginosa to gentamicin and Escherichia coli to cefoxitin.
Inpatient Settings: Studies Focused on Supplemental Strategies
Three studies analyzed specific outcomes of AS supplemental strategies; all three focused on CPGs. One study used an interrupted time series (ITS) analysis, while two conducted retrospective cohort studies. Two studies evaluated utilization and cost, while one study evaluated harm and cost.
Antimicrobial Utilization
Rutman et al. [23•] described the impact of a community-acquired pneumonia (CAP) CPG at an institution without a formal ASP. The CPG recommended the use of ampicillin as the preferred empiric therapy for patients hospitalized with uncomplicated CAP. Among children with uncomplicated CAP, the authors report an increase in ampicillin use from 8% pre-CPG to 63% post-CPG (DOT per 1000 PD). The CPG was also associated with an increase in CPG-recommended diagnostic testing with an increase in blood cultures and respiratory viral testing among admitted patients.
Prior to implementation of a formal ASP, Lee et al. [24•] developed multiple CPGs for patients in their institution’s pediatric, NICU, and cardiac intensive care units (ICUs) and evaluated antimicrobial utilization. Post guideline implementation, overall antibiotic use decreased by 41, 21, and 18% (DOT per 1000 PD), and targeted broad-spectrum antibiotic use decreased by 99, 75, and 61% (DOT per 1000 PD) in the pediatric, NICU, and cardiac ICUs.
Antimicrobial Costs
The CAP CPG study [23•] did not observe any change in costs of care for admitted patients and for patients discharged from the emergency department (ED) before and after CPG implementation. Hurst et al. [25] evaluated costs associated with a new guideline in an institution with a formal ASP. The authors described a simplified once-daily regimen of ceftriaxone and metronidazole in perforated, non-perforated, and abscessed cases of appendicitis compared to the historic regimen of cefoxitin or ertapenem. Over the 3-year study period, total antibiotic savings were over $110,000. After implementation of multiple ICU-specific guidelines, Lee et al. [24•] observed a 62% decline in yearly purchases of the most common broad-spectrum antibiotics from $230,059 to $86,887.
Patient Harm
The CAP CPG study assessed potential negative outcomes of implementing new guidelines. Rutman et al. [23•] did not observe any significant change in mean ED LOS, percentage of CAP admissions, or mean inpatient LOS 12 months before and after implementation of a CAP CPG. The appendicitis CPG study also assessed potential adverse effects of implementing a new guideline. Hurst et al. [25] found no difference in hospital LOS or post-operative abscess rates before and after implementation.
Unique Patient Populations
Neonatal Intensive Care Unit Patients
Antimicrobials are the most commonly prescribed medications in NICUs [26]. The majority of antimicrobials prescribed are empiric and narrow-spectrum, with only a small fraction directed toward culture-proven infection [27]. Due to an immature immune system and frequent need for invasive medical devices, these patients are at significant risk for infection; however, antimicrobial overuse may lead to MDR, invasive candidiasis, or necrotizing enterocolitis (NEC) [28,29,30]. Optimization of antimicrobial therapy is challenging due to the high risk of infection coupled with the significant adverse outcomes associated with antimicrobial use. Furthermore, identifying infection in this patient population is difficult due to non-specific symptoms.
Formalized ASP recommendations are lacking for the NICU setting, although expert guidance has been published [31] and international collaborations among NICUs exist [32]. Shulman et al. [33] observed a 40-fold variation in antimicrobial use among 127 California NICUs, with an overall antimicrobial utilization rate [AUR], as defined by the total number of PD that infants were exposed to one or more antibacterial or antifungal agents per 100 PD, which varied from 2.4 to 97.1%. Suggested stewardship interventions include optimization of culture techniques, guidelines for empiric therapy based on NICU-specific antibiograms, use of ancillary laboratory tests, and prompt discontinuation of therapy if infection is no longer suspected [34]. Pneumonia and “culture-negative sepsis” have been identified as frequent reasons for prolonged antimicrobial therapy and potential target areas to reduce treatment duration [27].
Table 2 provides major findings of four studies analyzing specific outcomes of core and supplemental AS interventions. Studies originated from six centers: Yale-New Haven Children’s Hospital, Parkland Hospital, Children’s Memorial Hermann Hospital, Brigham and Women’s Hospital, Massachusetts General Hospital, and New York-Presbyterian Hospital. Two studies used PAF and four studies implemented CPGs for common infections. One study used antibiotic restriction. Most outcomes focused on antimicrobial utilization.
Nzegwu et al. [35•] created a formal NICU ASP using PAF and CPGs, which was led by a multidisciplinary team (including a pediatric infectious disease physician and a pediatric clinical pharmacist). Prior to implementation, this institution was using formulary restriction for select antimicrobials. After implementation, there was a 12.8% reduction in ampicillin use (119 to 103 DOT per 1000 PD). The number of attending-specific late-onset sepsis evaluations and antimicrobial prescription events per 100 days of NICU service was assessed. There was an average reduction of 2.65 late-onset sepsis evaluations and prescription events per year per provider. The authors attribute their success to effective PAF.
Cantey et al. [36•] implemented AS interventions targeted at three areas accounting for a high proportion of antimicrobial consumption at their institution. Interventions included implementing an electronic “hard stop” for rule-out sepsis courses beyond 48 h and limiting treatment duration of culture negative sepsis and suspected pneumonia to 5 days. After implementation, overall antimicrobial utilization decreased by 27% (343 to 252 DOT per 1000 PD) without any short-term adverse outcomes. There was no change in the prevalence of MDR organism colonization between the two study periods.
Two studies focused on CPGs to reduce vancomycin utilization. Holzmann-Pazgal et al. [37] recommended the use of nafcillin instead of vancomycin for initial therapy of late-onset sepsis evaluation, unless a patient was known to be colonized with MRSA, and substitution of ampicillin instead of vancomycin for NEC. Antimicrobial administration episodes were collected and defined as initiation of an antimicrobial for any infant undergoing a late-onset sepsis evaluation; episodes were considered discrete if separated by prior antimicrobial use by 3 days. Observed administration episodes of vancomycin decreased from 118 to 35 over a 5-month period with no change in 30-day mortality. After implementation of PAF, there was no further reduction in episodes. Chiu et al. [38] implemented a narrow-spectrum late-onset sepsis guideline. There were 35 and 62% decreases in vancomycin use (6.9 to 4.5 per 1000 PD and 17 to 6.4 per 1000 PD) across two centers. There was no change in cases of meningitis or death due to late-onset sepsis across the two centers.
Oncology, Bone Marrow Transplant, and Solid Organ Transplant Patients
Oncology and transplant patients frequently utilize antifungal and antiviral therapy for both treatment and prophylaxis for high-risk conditions. In 2016, IDSA and SHEA recommended an expansion of stewardship activities to include antifungal therapy [4]. Goldman et al. [39•] observed significant variability in antifungal and antiviral therapy prescribing in high-risk children among 47 freestanding children’s hospitals. These agents serve as important targets in pediatric stewardship because they are costly, have a high rate of adverse drug effects, and require therapeutic drug monitoring, their inappropriate use can drive resistance, and they are often used for prophylaxis or treatment of high-risk infections.
A cross-sectional survey of AS practices in pediatric oncology across over 100 institutions in North America and Australasia revealed that 41/45 (91%) institutions had a formal ASP [40]. Commonly reported ASP activities in hospitals with formal ASPs included CPGs (80%), dose optimization (78%), resistance monitoring (76%), PAF (71%), monitoring of cultures (7%), clinician education (64%), and intravenous to oral strategies (62%).
There are few studies evaluating AS specifically for pediatric hematology-oncology patients. Only one study was identified. Wattier et al. [41] observed mixed long-term effects on ciprofloxacin and tobramycin DOT per 1000 PD after implementation of a febrile neutropenia guideline. After establishment of a formal ASP using PAF as their core strategy, they observed a sustained decrease in DOT per 1000 PD of tobramycin and ciprofloxacin. There was no change in frequency of resistance to ciprofloxacin among gram-negative isolates during the study period.
Ambulatory Settings
General Pediatric Practice
Antimicrobials are the most commonly prescribed medications for children [42] and are prescribed in 17–18.7% of all pediatric outpatient visits [42,43,44]. The most common reason for prescribing antimicrobials in the ambulatory setting is treatment of acute respiratory tract infections (ARTIs) [45]. The five most common childhood ARTIs are acute otitis media (AOM), sinusitis, bronchitis, upper RTIs, and pharyngitis. Significant variation exists across various primary care practices in prescribing rates, in preference for broad-spectrum agents, and in diagnosis and treatment choices for individual ARTIs [44]. In the post-pneumococcal conjugate vaccine era, an estimated 27.4% of US children with ARTIs have bacterial illness, although antimicrobials are prescribed twice as often during outpatient visits for evaluation of ARTIs [46]. Patients and physicians share concerns regarding a missed bacterial infection and the development of serious sequelae, although the major benefits of antibiotics for sinusitis and AOM are limited to symptom resolution [45]. Furthermore, in 2011, the Pediatric Infectious Diseases Society (PIDS) and the IDSA developed evidence-based CPGs for CAP in infants and children [47]. Handy et al. [48•] observed wide variation in antimicrobial choice for CAP across 31 primary care pediatric practices, independent of microbiologic etiology. Despite current guidelines recommending amoxicillin for most children with CAP, the majority of patients in this retrospective cohort were prescribed macrolides.
Formal AS recommendations exist for ambulatory settings and encompass four core elements: commitment, action for policy and practice, tracking and reporting, and education and expertise [12•]. Outpatient providers should commit to optimize antimicrobial prescribing by creating at least one policy or practice targeted to improve utilization. Unfortunately, there are limited studies evaluating the effectiveness of AS in this setting. Only one study was identified in our review. A cluster randomized trial across 18 community-based pediatric care practices of an outpatient AS intervention focused on PAF and led to a 50% relative reduction in prescribing rates for broad-spectrum antimicrobials [49]. Authors observed a 12.5% reduction in broad-spectrum prescribing (DOT per 1000 PD) among intervention practices vs 5.8% (DOT per 1000 PD) in controls. A follow-up survey assessing physician perceptions of the PAF intervention and antimicrobial use found that many physicians believed antimicrobial use was a problem, but the intervention was viewed with skepticism [50]. Gerber et al. [51] continued to study sites for an additional 18 months beyond the intervention and antimicrobial prescribing increased from 16.7 to 27.9% (DOT per 1000 PD) in the intervention group and from 25.4 to 30.2% (DOT per 1000 PD) in controls.
Emergency Department
No studies assessing the effectiveness of ED-based pediatric ASPs have been conducted. The ED has unique challenges in stewardship due to the fast-paced setting, frequent need for empiric antimicrobial therapy in the absence of a confirmatory diagnosis, and essential role in obtaining relevant cultures before therapy is started [52]. In a retrospective cohort at a single ED, Watson et al. [53] observed that half of patients less than 21 years of age prescribed empiric antimicrobial therapy for a presumed urinary tract infection (UTI) did not have a positive urine culture to confirm the UTI diagnosis. This study highlights an opportunity for diagnostic test stewardship. Mistry et al. [54•] conducted a cross-sectional survey of 37 children’s hospitals participating in the Sharing Antimicrobial Resistance Practices (SHARPs) collaboration and found that production of antibiograms (77.8%) and creation of CPGs for pneumonia (83.3%) were the two main AS activities reported for the ED. In this multicenter study, no hospital ASPs actively monitored outpatient ED prescribing. Most ED leaders preferred a clinical decision support tool integrated into the electronic medical record (EMR) for implementation of an ED-based ASP.
External regulatory pressures (such as compliance with sepsis management metrics) can be at odds with AS in EDs. Multiple studies have demonstrated improved mortality in severe sepsis and septic shock with timely antimicrobial administration [55, 56]. Current surviving sepsis guidelines recommend administration of broad-spectrum antimicrobial therapy within 1 h of recognition of septic shock and severe sepsis without septic shock whether they are located in the general ward, in the ED, or in the ICU [57••]. The Centers for Medicare and Medicaid Services (CMS) issued core measures for the management of sepsis on October 1, 2015, including the administration of broad-spectrum antimicrobial therapy within 3 h of presentation of severe sepsis [58]. A large systematic review and meta-analysis in adult patients did not find a significant mortality benefit of administering antibiotics within 3 h of ED triage or within 1 h of shock recognition in severe sepsis and septic shock [59]. The diagnosis of sepsis is multifactorial and complex, and there is no gold standard definition for sepsis, severe sepsis, or septic shock in pediatric or adult patients. Adult patients presenting to an academic ED with suspected sepsis based on the evidence of two or more systemic inflammatory response syndrome (SIRS) criteria were found to have a confirmed bacterial infection 36% of the time, while 35% were classified as suspected bacterial infection without microbiologic evidence. Despite the absence of proven bacterial disease in 29% of the patients, median antimicrobial duration was 7 days [60]. The initial antimicrobial choice made by the ED may have significant influence on what therapy is continued on the inpatient setting and represents an important opportunity for AS intervention.
Outpatient Parenteral Antimicrobial Therapy
Osteomyelitis is the most common condition managed by outpatient parenteral antimicrobial therapy (OPAT), and there is a significant variation in OPAT use for this condition [61]. Furthermore, complications with OPAT are common [62], and there is increasing evidence that OPAT is overused and misused. A retrospective cohort study at a large academic children’s hospital revealed that OPAT episodes without infectious disease consultation were most commonly: intra-abdominal infections (29%), central line infections/bacteremia (28%), cystic fibrosis exacerbations (9%), and UTI/pyelonephritis (7%) [63]. Of these OPAT cases, the authors determined that 40% of the time OPAT was not indicated. Goldman et al. [64•] studied OPAT in a large population of US children enrolled in Medicaid and found a high rate of adverse events coupled with administration of systemic agents that are highly bioavailable that could be given orally.
Traditionally, ASP involvement in OPAT has been limited. One study described one ASP’s experience in including OPAT. Hersh et al. [65•] implemented multiple strategies to detect and review cases of patients being discharged with an OPAT prescription. The number of children discharged on OPAT with infectious disease consultation increased from 47 to 87%, and OPAT use (defined as the number of patients per month discharged with OPAT per 1000 hospital discharges) decreased by from 23.4 to 17.8 per 1000 discharges during the intervention period.
Other Considerations
Metrics
Traditionally, volume-based metrics, such as DOT per 1000 PD, have been used to compare antimicrobial use in hospitalized patients [66••]. This method provides a standard measurement to compare antimicrobial consumption data across hospitals, but it does not take into account the antimicrobial spectrum of drug exposure. A hospital that uses more narrow-spectrum antimicrobials may have the same overall DOT per 1000 PD as a hospital that uses broader-spectrum antimicrobials. Furthermore, an AS intervention to change from broad-spectrum monotherapy to two more narrow antimicrobials would result in higher overall DOT per 1000 PD. To address these issues, Gerber et al. [67•] developed an antibiotic spectrum index (ASI) to measure and compare the broad spectrum of antimicrobial use across US children’s hospitals. This metric, based on spectrum of activity against clinically relevant pathogens, provides a new opportunity to assess ASPs along with the standard metric of DOT per 1000 PD. The authors created a novel scoring system, which assigns a point value based on the spectrum of activity of antimicrobials against clinically important isolates. For example, amoxicillin’s ASI is 1, while vancomycin and meropenem have ASIs of 5 and 10, respectively. Aggregate ASIs for a single day are obtained by calculating and summing the ASI of all antimicrobials prescribed and reported as ASI per antibiotic day. Using the Pediatric Health Information System (PHIS), the authors identified children across 44 freestanding US children’s hospitals discharged with the diagnosis of CAP. Examining the impact of AS strategies targeting CAP to choose more narrow-spectrum empiric therapy revealed no change in DOT per 1000 PD, but did reveal a reduction in ASI per antibiotic day indicating an overall change from broader to more narrow antimicrobial therapy. This metric may be helpful in evaluating the effectiveness of ASP at decreasing the utilization of broad-spectrum antimicrobials.
Discussion
A growing body of evidence suggests the use of ASPs to optimize antimicrobial therapy. In 2014, the CDC recommended that all acute care hospitals implement an ASP [68]. Effective on January 1, 2017, the Joint Commission required all hospitals to have an ASP based on current scientific literature [69••]. Furthermore, CMS has proposed that hospitals and critical access hospitals be required to implement ASPs for appropriate use of antimicrobials [70].
ASPs have been formally recommended since 2007 by the IDSA, but there are few studies evaluating the effectiveness of pediatric ASPs. A previous systematic review [13•] of inpatient ASPs found nine studies evaluating comprehensive ASPs and eight studies evaluating AS strategies. The nine studies on formal ASPs originated from only four centers. This review found nine additional studies on formal ASPs in the inpatient setting. Each study originates from a different institution, including two non-freestanding children’s hospitals. In comparison, a systematic review of inpatient adult ASPs from years 2000 to 2013 found 37 articles evaluating the effectiveness of AS strategies [71]. Despite the small number of pediatric studies, these data suggest that pediatric ASPs are expanding to institutions of various sizes and resources.
Inpatient pediatric ASPs within larger institutions have a unique opportunity to create programs specific for the needs of the population they serve. In two studies in non-freestanding children’s hospitals [14•, 15•], PAF was an effective intervention in reducing antimicrobial utilization. After implementation of a pediatric-specific ASP, Turner et al. [14•] did not observe a change in antimicrobial consumption at the attached adult facility (that did not participate in ASP), suggesting that hospital-wide policy did not play a role in reduction of antimicrobial consumption within the children’s hospital.
The majority of inpatient pediatric-specific ASPs focused primarily on PAF with or without restriction. One study effectively reduced vancomycin usage with PAF alone, and the addition of restriction did not lead to any further significant reduction [19•]. Hurst et al. utilized a “handshake stewardship” that utilized PAF but not restriction [16•]. This approach was effective at reducing total antimicrobial consumption (in DOT per 1000 PD). PAF alone may be an effective strategy to decrease antimicrobial use and healthcare costs in pediatric ASP.
No formalized AS recommendations exist for the NICU setting, but some expert guidance has been published [31]. A high proportion of narrow-spectrum antimicrobials account for overall antimicrobial prescribing in the NICU and are unlikely to be monitored by most hospital-based ASPs. Review of the four published NICU-based studies indicates that CPGs for common infections and targeted interventions have been effective at decreasing antimicrobial utilization in this setting and may serve as starting points for NICU-specific AS strategies.
Despite the high utilization of antifungal and antiviral therapy in pediatric hematology-oncology patients, there are limited published studies of targeted ASP interventions in this unique population. Both NICU and hematology/oncology patient populations likely fall under the scope of an inpatient ASP, but each vulnerable population has unique challenges necessitating nuanced, tailored AS strategies. Recently, the CDC adapted core elements of hospital-based ASPs to expand AS activities to a vulnerable adult population: residents of nursing homes (NHs) [72]. A systematic review of ASPs in NHs found evidence that suggests NH ASPs can reduce antimicrobial prescriptions and improve provider adherence to proposed AS guidelines [73•]. Unique pediatric populations may also benefit from specific AS activities, and more studies to evaluate effective strategies in these unique pediatric groups are needed.
There are limited data on ASP in ambulatory settings. A cluster randomized trial [49] across multiple pediatric clinics was effective at decreasing utilization of broad-spectrum antimicrobials, but the impact was not sustained after the AS intervention ended [51]. Extending ASP activities to ambulatory settings can be effective, but sustained efforts are critical. There has also traditionally been limited ASP involvement in the ED. The ED has many unique challenges, and further studies are needed to determine which AS strategies are most effective in this setting. Lastly, Hersh et al. [65•] demonstrated that OPAT stewardship can be successfully integrated into an ASP with a reduction in patients discharged inappropriately on OPAT.
Conclusions
Most of the formal inpatient ASPs reviewed conducted an interrupted time series analysis (ITS) and were multifaceted, each with a slightly different approach. Few had comparison groups (no randomized control trials, and only three ITS studies had control groups), and no study directly compared one intervention with another. Although the current literature is limited, existing evidence indicates that inpatient pediatric ASPs can reduce antimicrobial utilization and costs without short-term adverse patient outcomes. Data to support a link between ASPs and reduced antimicrobial resistance are lacking. It is not possible to outline a universally optimal pediatric ASP structure with associated activities based on the current literature. Using published national guidelines as a framework, pediatric ASPs need to tailor their structure and activities based on local resources and needs. The literature does suggest that active stewardship is critical and that antimicrobial consumption is a key outcome metric for programs. There is a paucity of evidence on the effectiveness of ASP strategies in the NICU and pediatric hematology/oncology patients. To date, the majority of AS efforts targeted the inpatient setting. However, outpatient settings and emergency departments are important future targets for ASPs.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Society for Healthcare Epidemiology of America, Infectious Diseases Society of America, Pediatric Infectious Diseases Society. Policy statement on antimicrobial stewardship by the Society for Healthcare Epidemiology of America (SHEA), the Infectious Diseases Society of America (IDSA), and the Pediatric Infectious Diseases Society (PIDS). Infect Control Hosp Epidemiol. 2012;33(4):322–327.
Antimicrobial resistance: global report on surveillance 2014 [Internet]. World Health Organization [cited 2018 April 10]. Available from: http://apps.who.int/iris/bitstream/handle/10665/112642/9789241564748_eng.pdf?sequence=1
• Logan LK, Gandra S, Mandal S, Klein EY, Levinson J, Weinstein RA, et al. Multidrug- and carbapenem-resistant Pseudomonas aeruginosa in children, United States, 1999–2012. J Pediatric Infect Dis Soc 2016 Nov 16. These authors highlight the increasing rate of multidrug-resistant Pseudomonas aeruginosa isolates in US children between 1999 and 2012.
Dellit TH, Owens RC, McGowan JE Jr, Gerding DN, Weinstein RA, Burke JP, et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin Infect Dis. 2007 Jan 15;44(2):159–77.
•• Barlam TF, Cosgrove SE, Abbo LM, MacDougall C, Schuetz AN, Septimus EJ, et al. Implementing an antibiotic stewardship program: guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin Infect Dis. 2016;62(10):e51–77. This article provides evidence-based guidelines and expert guidance from the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America on antimicrobial stewardship program approaches for optimization of antimicrobial use in the inpatient setting.
Gerber JS, Newland JG, Coffin SE, Hall M, Thurm C, Prasad PA, et al. Variability in antibiotic use at children’s hospitals. Pediatrics. 2010 Dec;126(6):1067–73.
Pakyz AL, MacDougall C, Oinonen M, Polk RE. Trends in antibacterial use in US academic health centers: 2002 to 2006. Arch Intern Med. 2008 Nov 10;168(20):2254–60.
Gerber JS, Kronman MP, Ross RK, Hersh AL, Newland JG, Metjian TA, et al. Identifying targets for antimicrobial stewardship in children’s hospitals. Infect Control Hosp Epidemiol. 2013 Dec;34(12):1252–8.
Antibiotic prescribing and use in hospitals and long-term care [Internet]. Atlanta (GA): Centers for Disease Control and Prevention. 2017 [cited 2017 Jan 8]. Available from: http://www.cdc.gov/getsmart/healthcare/.
Newland JG, Gerber JS, Weissman SJ, Shah SS, Turgeon C, Hedican EB, et al. Prevalence and characteristics of antimicrobial stewardship programs at freestanding children’s hospitals in the United States. Infect Control Hosp Epidemiol. 2014 Mar;35(3):265–71.
• Hersh AL, De Lurgio SA, Thurm C, Lee BR, Weissman SJ, Courter JD, et al. Antimicrobial stewardship programs in freestanding children's hospitals. Pediatrics. 2015;135(1):33–9. This is a multicenter study across freestanding children’s hospitals. Authors observed an overall decrease in antimicrobial use in DOT per 1000 PD across freestanding children’s hospitals with or without ASP. The rate of decline was highest in those with a formalized ASP. This study adds to the growing body of evidence that suggests inpatient pediatric ASPs can be effective at decreasing antimicrobial consumption
• Sanchez GV, Fleming-Dutra KE, Roberts RM, Hicks LA. Core elements of outpatient antibiotic stewardship. MMWR Recomm Rep. 2016;65(6):1–12. These authors provide guidance for antimicrobial stewardship in the outpatient setting based on existing evidence-based guidelines and expert opinion from other clinical settings.
• Smith MJ, Gerber JS, Hersh AL. Inpatient antimicrobial stewardship in pediatrics: a systematic review. J Pediatric Infect Dis Soc. 2015;4(4):e127–35. This is a systematic review of studies published through March 2014 that evaluated the effectiveness of inpatient pediatric ASPs and other supplemental AS interventions. These data suggest that pediatric ASPs can be effective at decreasing antimicrobial consumption without short-term adverse events.
• Turner RB, Valcarlos E, Loeffler AM, Gilbert M, Chan D. Impact of an Antimicrobial Stewardship Program on Antibiotic Use at a Nonfreestanding Children's Hospital. J Pediatric Infect Dis Soc. 2017;6(3):e36–40. This is a single-center study in a non-freestanding children’s hospital that reported on the impact of PAF on antimicrobial consumption. Authors found an overall reduction of antimicrobial use and vancomycin use in DOT per 1000 PD without a difference in hospital LOS or in-hospital mortality. This study adds to the growing body of evidence that suggests inpatient pediatric ASPs can be effective at decreasing antimicrobial consumption without affecting patient safety
• Lighter-Fisher J, Desai S, Stachel A, Pham VP, Klejmont L, Dubrovskaya Y. Implementing an inpatient pediatric prospective audit and feedback antimicrobial stewardship program within a larger medical center. Hosp Pediatr. 2017;7(9):516–22. This is a single-center study in a non-freestanding children’s hospital. Authors implemented a formal ASP with CPG, PAF, and restriction and found an overall reduction in antimicrobial use in DOT per 1000 PD. This study adds to the growing body of evidence that suggests inpatient pediatric ASPs can be effective at decreasing antimicrobial consumption.
• Hurst AL, Child J, Pearce K, Palmer C, Todd JK, Parker SK. Handshake stewardship: a highly effective rounding-based antimicrobial optimization service. Pediatr Infect Dis J. 2016;35(10):1104–10. This is a single-center study in a freestanding children’s hospital. Authors implemented a “handshake stewardship” program defined by lack of restriction and preauthorization, review of all prescribed antimicrobials, and rounding-based feedback by a pharmacist-physician team. This approach reduced hospital-wide antimicrobial consumption and reduced meropenem and vancomycin use as well. This study adds to the growing body of evidence that suggests inpatient pediatric ASPs can be effective at decreasing antimicrobial consumption.
• Willis ZI, Gillon J, Xu M, Slaughter JC, Di Pentima MC. Reducing antimicrobial use in an academic pediatric institution: evaluation of the effectiveness of a prospective audit with real-time feedback. J Pediatric Infect Dis Soc. 2017;6(4):339–45. This is a single-center center that implemented an ASP primarily focused on PAF, but that also included elements of prior authorization and CPG development, which led to an overall reduction of antimicrobial DOT per 1000 PD. Using a comparator group, authors concluded that the ASPs impact was greater than would have been expected based on secular trends.
• Gillon J, Xu M, Slaughter J, Di Pentima MC. Vancomycin use: room for improvement among hospitalized children. J Pharm Pract. 2017;30(3):296–9. This is a single-center center that implemented an ASP primarily focused on PAF which led to a reduction in vancomycin DOT per 1000 PD. Using a comparator group, authors concluded that vancomycin use was lower compared to hospitals without an ASP. This study adds to the growing body of evidence that suggests pediatric ASPs can be effective at decreasing antimicrobial consumption.
• Chan S, Hossain J, Di Pentima MC. Implications and impact of prior authorization policy on vancomycin use at a tertiary pediatric teaching hospital. Pediatr Infect Dis J. 2015;34(5):506–8. This is a single-center center that implemented an ASP primarily focused on PAF which led to a reduction in vancomycin DOT per 1000 PD. This study adds to the growing body of evidence that suggests pediatric ASPs can be effective at decreasing antimicrobial consumption.
• Nguyen-Ha PT, Howrie D, Crowley K, Vetterly CG, McGhee W, Berry D, et al. A quality assessment of a collaborative model of a pediatric antimicrobial stewardship program. Pediatrics 2016;137(5):https://doi.org/10.1542/peds.2015-0316. Epub 2016 Apr 6. This is a single-center center that implemented an ASP focused on PAF, restriction, and CPGs and found a reduction in vancomycin and meropenem DOT per 1000 PD. This study adds to the growing body of evidence that suggests inpatient pediatric ASPs can be effective at decreasing antimicrobial consumption.
• Molloy L, McGrath E, Thomas R, Kaye KS, Rybak MJ. Acceptance of pharmacist-driven antimicrobial stewardship recommendations with differing levels of physician involvement in a children’s hospital. Clin Pediatr (Phila). 2017;56(8):744–51. This is a single-center center that implemented a pharmacist-driven ASP and found no difference in hospital LOS, in-hospital mortality, or all-cause readmission after implementation. This study adds to the growing body of evidence that suggests inpatient pediatric ASPs can be effective at decreasing antimicrobial consumption.
• Ross RK, Beus JM, Metjian TA, Localio AR, Shelov ED, Desai BR, et al. Safety of automatic end dates for antimicrobial orders to facilitate stewardship. Infect Control Hosp Epidemiol. 2016;37(8):974–8. This is a single-center center that implemented an ASP focused on restriction with an automated EMR stop order and found no difference in hospital LOS, in-hospital mortality, or readmission rates during the study period. This study adds to the growing body of evidence that suggests inpatient pediatric ASPs can be implemented without affecting patient safety.
• Rutman L, Wright DR, O'Callaghan J, Spencer S, Lion KC, Kronman MP, et al. A comprehensive approach to pediatric pneumonia: relationship between standardization, antimicrobial stewardship, clinical testing, and cost. J Healthc Qual. 2017;39(4):e59–69. This is a single-center center that implemented a CAP CPG at an institution without a formal ASP, which led to increased consumption of a more narrow empiric antimicrobial agent. This study adds to the growing body of evidence that suggests pediatric AS interventions can be effective at decreasing antimicrobial consumption.
• Lee KR, Bagga B, Arnold SR. Reduction of broad-spectrum antimicrobial use in a tertiary children’s hospital post antimicrobial stewardship program guideline implementation. Pediatr Crit Care Med. 2016;17(3):187–93. This is a single-center center that implemented multiple CPGS for patients in their institution’s pediatric, NICU, and cardiac ICU. Authors found a reduction in overall and targeted antimicrobial consumption across studied units.
Hurst AL, Olson D, Somme S, Child J, Pyle L, Ranade D, et al. Once-daily ceftriaxone plus metronidazole versus ertapenem and/or cefoxitin for pediatric appendicitis. J Pediatric Infect Dis Soc. 2017 Mar 1;6(1):57–64.
Clark RH, Bloom BT, Spitzer AR, Gerstmann DR. Reported medication use in the neonatal intensive care unit: data from a large national data set. Pediatrics. 2006 Jun;117(6):1979–87.
Cantey JB, Wozniak PS, Sanchez PJ. Prospective surveillance of antibiotic use in the neonatal intensive care unit: results from the SCOUT study. Pediatr Infect Dis J. 2015 Mar;34(3):267–72.
Cotten CM, McDonald S, Stoll B, Goldberg RN, Poole K, Benjamin DK Jr, et al. The association of third-generation cephalosporin use and invasive candidiasis in extremely low birth-weight infants. Pediatrics. 2006 Aug;118(2):717–22.
Cotten CM, Taylor S, Stoll B, Goldberg RN, Hansen NI, Sanchez PJ, et al. Prolonged duration of initial empirical antibiotic treatment is associated with increased rates of necrotizing enterocolitis and death for extremely low birth weight infants. Pediatrics. 2009 Jan;123(1):58–66.
Tsai MH, Chu SM, Hsu JF, Lien R, Huang HR, Chiang MC, et al. Risk factors and outcomes for multidrug-resistant Gram-negative bacteremia in the NICU. Pediatrics. 2014 Feb;133(2):e322–9.
Patel SJ, Saiman L. Principles and strategies of antimicrobial stewardship in the neonatal intensive care unit. Semin Perinatol. 2012 Dec;36(6):431–6.
iNICQ 2017: choosing antibiotics wisely [Internet]. Vermont Oxford Network; 2018. [cited 2018 Jan 8]. Available from: http://public.vtoxford.org/quality-education/inicq-2017-choosing-antibiotics-wisely/.
Schulman J, Dimand RJ, Lee HC, Duenas GV, Bennett MV, Gould JB. Neonatal intensive care unit antibiotic use. Pediatrics. 2015 May;135(5):826–33.
Cantey JB, Patel SJ. Antimicrobial stewardship in the NICU. Infect Dis Clin N Am. 2014 Jun;28(2):247–61.
• Nzegwu NI, Rychalsky MR, Nallu LA, Song X, Deng Y, Natusch AM, et al. Implementation of an antimicrobial stewardship program in a neonatal intensive care unit. Infect Control Hosp Epidemiol. 2017;38(10):1137–43. This is a single-center study that created a formal NICU ASP using PF and CPGs, which was led by a multidisciplinary team. Authors found a reduction in ampicillin DOT per 1000 PD. This study adds to the growing body of evidence that suggests ASPs in NICU can be effective at decreasing antimicrobial consumption.
• Cantey JB, Wozniak PS, Pruszynski JE, Sanchez PJ. Reducing unnecessary antibiotic use in the neonatal intensive care unit (SCOUT): a prospective interrupted time-series study. Lancet Infect Dis. 2016;16(10):1178–84. This is a single-center study that implemented AS interventions targeting areas of high proportion antimicrobial use at their institution. After implementation, authors found a reduction of overall antimicrobial utilization without any short-term adverse outcomes. This study adds to the growing body of evidence that suggests AS interventions in NICU can be effective at decreasing antimicrobial consumption without affecting patient safety.
Holzmann-Pazgal G, Khan AM, Northrup TF, Domonoske C, Eichenwald EC. Decreasing vancomycin utilization in a neonatal intensive care unit. Am J Infect Control. 2015 Nov;43(11):1255–7.
Chiu CH, Michelow IC, Cronin J, Ringer SA, Ferris TG, Puopolo KM. Effectiveness of a guideline to reduce vancomycin use in the neonatal intensive care unit. Pediatr Infect Dis J. 2011 Apr;30(4):273–8.
• Goldman JL, Ross RK, Lee BR, Newland JG, Hersh AL, Kronman MP, et al. Variability in antifungal and antiviral use in hospitalized children. Infect Control Hosp Epidemiol. 2017;38(6):743–6. Authors found significant variability in antifungal and antiviral therapy prescribing in high-risk children among freestanding children’s hospitals. This study highlights the importance of an inpatient ASP targeting these agents.
Wolf J, Sun Y, Tang L, Newland JG, Gerber JS, Van Dyke CJ, et al. Antimicrobial stewardship barriers and goals in pediatric oncology and bone marrow transplantation: a survey of antimicrobial stewardship practitioners. Infect Control Hosp Epidemiol. 2016 Mar;37(3):343–7.
Wattier RL, Levy ER, Sabnis AJ, Dvorak CC, Auerbach AD. Reducing second gram-negative antibiotic therapy on pediatric oncology and hematopoietic stem cell transplantation services. Infect Control Hosp Epidemiol. 2017 Sep;38(9):1039–47.
Chai G, Governale L, McMahon AW, Trinidad JP, Staffa J, Murphy D. Trends of outpatient prescription drug utilization in US children, 2002–2010. Pediatrics. 2012 Jul;130(1):23–31.
Saleh EA, Schroeder DR, Hanson AC, Banerjee R. Guideline-concordant antibiotic prescribing for pediatric outpatients with otitis media, community-acquired pneumonia, and skin and soft tissue infections in a large multispecialty healthcare system. Clin Res Infect Dis 2015;2(1).
Gerber JS, Prasad PA, Russell Localio A, Fiks AG, Grundmeier RW, Bell LM, et al. Variation in antibiotic prescribing across a pediatric primary care network. J Pediatric Infect Dis Soc. 2015 Dec;4(4):297–304.
Hersh AL, Jackson MA, Hicks LA, American Academy of Pediatrics Committee on Infectious Diseases. Principles of judicious antibiotic prescribing for upper respiratory tract infections in pediatrics. Pediatrics. 2013;132(6):1146–54.
Kronman MP, Zhou C, Mangione-Smith R. Bacterial prevalence and antimicrobial prescribing trends for acute respiratory tract infections. Pediatrics. 2014 Oct;134(4):e956–65.
Bradley JS, Byington CL, Shah SS, Azlverson B, Carter ER, Harrison C, et al. Executive summary: the management of community-acquired pneumonia in infants and children older than 3 months of age: clinical practice guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America. Clin Infect Dis. 2011 Oct;53(7):617–30.
• Handy LK, Bryan M, Gerber JS, Zaoutis T, Feemster KA. Variability in antibiotic prescribing for community-acquired pneumonia. Pediatrics. 2017;139(4):https://doi.org/10.1542/peds.2016-2331. Epub 2017 Mar 7. Authors found significant variability in antimicrobial prescribing for CAP across multiple, pediatric outpatient practices independent of microbiologic etiology. This article highlights the need for AS intervention or a formalized ASP in the outpatient setting to optimize antimicrobial prescribing for this patient population.
Gerber JS, Prasad PA, Fiks AG, Localio AR, Grundmeier RW, Bell LM, et al. Effect of an outpatient antimicrobial stewardship intervention on broad-spectrum antibiotic prescribing by primary care pediatricians: a randomized trial. JAMA. 2013 Jun 12;309(22):2345–52.
Szymczak JE, Feemster KA, Zaoutis TE, Gerber JS. Pediatrician perceptions of an outpatient antimicrobial stewardship intervention. Infect Control Hosp Epidemiol. 2014 Oct;35(Suppl 3):S69–78.
Gerber JS, Prasad PA, Fiks AG, Localio AR, Bell LM, Keren R, et al. Durability of benefits of an outpatient antimicrobial stewardship intervention after discontinuation of audit and feedback. JAMA. 2014 Dec 17;312(23):2569–70.
May L, Cosgrove S, L'Archeveque M, Talan DA, Payne P, Jordan J, et al. A call to action for antimicrobial stewardship in the emergency department: approaches and strategies. Ann Emerg Med 2013 Jul;62(1):69–77.e2.
Watson JR, Sanchez PJ, Spencer JD, Cohen DM, Hains DS. Urinary tract infection and antimicrobial stewardship in the emergency department. Pediatr Emerg Care. 2016.
• Mistry RD, Newland JG, Gerber JS, Hersh AL, May L, Perman SM, et al. Current state of antimicrobial stewardship in children’s hospital emergency departments. Infect Control Hosp Epidemiol. 2017;38(4):469–75. This multicenter study highlights current AS activities reported in emergency departments in children’s hospitals participating in the Sharing Antimicrobial Resistance Practices (SHARPs) collaboration. This is an important descriptive study addressing current AS practices in this ambulatory setting.
Ferrer R, Martin-Loeches I, Phillips G, Osborn TM, Townsend S, Dellinger RP, et al. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: results from a guideline-based performance improvement program. Crit Care Med. 2014 Aug;42(8):1749–55.
Gaieski DF, Mikkelsen ME, Band RA, Pines JM, Massone R, Furia FF, et al. Impact of time to antibiotics on survival in patients with severe sepsis or septic shock in whom early goal-directed therapy was initiated in the emergency department. Crit Care Med. 2010 Apr;38(4):1045–53.
•• Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, et al. Surviving sepsis campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017;43(3):304–77. This is an important article highlighting the consensus statements of the surviving sepsis guideline panel on the best care for patients with sepsis using evidence-based recommendations.
Sepsis Bundle Project (SEP) Specifications Manual for National Hospital Inpatient Quality Measures Discharges [Internet]. Centers for Medicare and Medicaid Services [cited 2018 March 3]. Available from: http://www.Nhfca.org/psf/resources/updates/SEP-1%20measure%20information%20form%20(MIF).pdf.
Sterling SA, Miller WR, Pryor J, Puskarich MA, Jones AE. The impact of timing of antibiotics on outcomes in severe Sepsis and septic shock: a systematic review and meta-analysis. Crit Care Med. 2015 Sep;43(9):1907–15.
Minderhoud TC, Spruyt C, Huisman S, Oskam E, Schuit SCE, Levin MD. Microbiological outcomes and antibiotic overuse in emergency department patients with suspected sepsis. Neth J Med. 2017 Jun;75(5):196–203.
Banerjee R, Beekmann SE, Doby EH, Polgreen PM, Rathore MH, Hersh AL. Outpatient parenteral antimicrobial therapy practices among pediatric infectious diseases consultants: results of an emerging infections network survey. J Pediatric Infect Dis Soc. 2014 Mar;3(1):85–8.
Barrier A, Williams DJ, Connelly M, Creech CB. Frequency of peripherally inserted central catheter complications in children. Pediatr Infect Dis J. 2012 May;31(5):519–21.
Knackstedt ED, Stockmann C, Davis CR, Thorell EA, Pavia AT, Hersh AL. Outpatient parenteral antimicrobial therapy in pediatrics: an opportunity to expand antimicrobial stewardship. Infect Control Hosp Epidemiol. 2015 Feb;36(2):222–4.
• Goldman JL, Richardson T, Newland JG, Lee B, Gerber JS, Hall M, et al. Outpatient parenteral antimicrobial therapy in pediatric Medicaid enrollees. J Pediatric Infect Dis Soc. 2017;6(1):65–71. Authors studied outpatient parenteral antibiotic therapy (OPAT) in a large population of US children enrolled in Medicaid and found a high rate of adverse events coupled with administration of systemic agents that are highly bioavailable that could be given orally. OPAT may be a suitable target for an outpatient-based ASP.
• Hersh AL, Olson J, Stockmann C, Thorell EA, Knackstedt ED, Esquibel L, et al. Impact of antimicrobial stewardship for pediatric outpatient parenteral antibiotic therapy. J Pediatric Infect Dis Soc 2017. This is a single-center study where authors incorporated outpatient parenteral antibiotic therapy into their established ASP. This study demonstrates that traditional ASPs can be extended and incorporated in the outpatient setting.
•• Moehring RW, Anderson DJ, Cochran RL, Hicks LA, Srinivasan A, Dodds Ashley ES, et al. Expert consensus on metrics to assess the impact of patient-level antimicrobial stewardship interventions in acute-care settings. Clin Infect Dis. 2017;64(3):377–83. This article provides expert consensus on appropriate metrics to assess ASP interventions in inpatient settings.
• Gerber JS, Hersh AL, Kronman MP, Newland JG, Ross RK, Metjian TA. Development and application of an antibiotic spectrum index for benchmarking antibiotic selection patterns across hospitals. Infect Control Hosp Epidemiol. 2017;38(8):993–7. Authors created an antibiotic spectrum index to measure and compare the broad spectrum of antimicrobial use across US children’s hospitals. This metric, based on spectrum of activity against clinically relevant pathogens, provides a new opportunity to assess ASPs along with the standard metric of DOT per 1000 PD. This metric may be helpful in evaluating the effectiveness of ASP at decreasing the utilization of broad-spectrum antimicrobials.
Pollack LA, Srinivasan A. Core elements of hospital antibiotic stewardship programs from the Centers for Disease Control and Prevention. Clin Infect Dis. 2014;59(Suppl 3):S97–100.
•• Joint Commission on Hospital Accreditation. APPROVED: new antimicrobial stewardship standard. Jt Comm Perspect. 2016;36(7):1, 3–4, 8. This statement from the Joint Commission requires that all hospitals implement an ASP based on current scientific literature, which was effective on January 1, 2017.
Centers for Medicare and Medicaid Services. CMS issues proposed rule that prohibits discrimination, reduces hospital-acquired conditions, and promotes antibiotic stewardship in hospitals [Internet]. 2016 June [cited 2018 March 3]. Available from: https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2016-Fact-sheets-items/2016-06-13.html
Wagner B, Filice GA, Drekonja D, Greer N, MacDonald R, Rutks I, et al. Antimicrobial stewardship programs in inpatient hospital settings: a systematic review. Infect Control Hosp Epidemiol. 2014 Oct;35(10):1209–28.
Federal Register: The Daily Journal of the United States Government. Medicare and Medicaid programs; reform of requirements for long-term-care facilities [Internet]. 2016 September [cited 2018 Jan 8]. Available from: https://www.federalregister.gov/documents/2016/10/04/2016-23503/medicare-and-medicaid-programs-reform-of-requirements-for-long-term-care-facilities
• Feldstein D, Sloane PD, Feltner C. Antibiotic stewardship programs in nursing homes: a systematic review. J Am Med Dir Assoc 2017. This is a systematic review of studies published on the effectiveness of ASPs in nursing homes. Authors concluded that ASPs in this unique patient population can reduce antimicrobial prescriptions and improve provider adherence to proposed AS guidelines. This study adds to the growing body of evidence that ASPs can be effectively used in unique patient populations.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflicts of interest.
Human and Animal Rights
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Healthcare Associated Infections
Rights and permissions
About this article

Cite this article
Godbout, E.J., Pakyz, A.L., Markley, J.D. et al. Pediatric Antimicrobial Stewardship: State of the Art. Curr Infect Dis Rep 20, 39 (2018). https://doi.org/10.1007/s11908-018-0644-7
Published:
DOI: https://doi.org/10.1007/s11908-018-0644-7