
Abstract
Purpose of Review
This study investigated and pooled the long-term trends in prevalence, awareness, treatment, and control of hypertension (HTN) in the Middle East and North Africa (MENA) region. In this systematic review and meta-analysis, we searched MEDLINE/PubMed, Web of Science, Google Scholar, EMBASE, and Scopus between database inception and November 2020. All cross-sectional studies that investigated the prevalence of pre-HTN, HTN, awareness, treatment, and control in the MENA counties were included. The selection study, data extraction, and quality assessment were conducted by two investigators independently. Heterogeneity between studies was assessed using Cochran’s Q test and I-squared, and due to sever heterogeneity between studies, the random effect model was used to pool the estimates. Sensitivity analysis was performed to estimate the long-term trends in prevalence, awareness, treatment, and control rates of HTN according to definition of HTN as systolic blood pressure of 140 mm Hg or more, or diastolic blood pressure of 90 mm Hg or more, or being on pharmacological treatment for HTN.
Recent Findings
Overall, 178 studies met the inclusion criteria. Studies comprised 2,262,797 participants with a mean age of 45.72 ± 8.84 years. According to random effect model, the pooled prevalence of pre-HTN and HTN was 33% (95% CI 28, 39) and 26% (25, 27), respectively. Over the past three decades, prevalence of hypertension increased significantly in the region. The pooled awareness, treatment, and control rates were 50% (48, 53), 41% (38, 44), and 19% (17, 21), receptively. The pooled awareness, treatment, and control rates of HTN were lower significantly in men than women. According to definition of HTN as blood pressures above 140/90 mm Hg, over the past three decades, although the awareness and treatment rates did not change significantly, the control rates improved significantly in the region.
Summary
The findings showed that HTN is a significant public health problem in the MENA region. Although there are low levels of pooled awareness, treatment, and control rates, the control rates improved over the past three decades in the region.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hypertension (HTN) remains one of the significant risk factors for multiple complications such as stroke, coronary artery diseases, and renal failures [1]. Despite the efforts in managing HTN across the globe in recent years, a surge in the prevalence of the condition has been observed [2]. This remains a major public health concern, especially in low- and middle-income countries. Proper management of HTN leads to lower health complications for patients, as well as less burden on the health care system. Recent findings have shown an HTN prevalence rate of 17.5% in low- and middle-income countries. However, only 29.9% of these patients have received treatment for HTN and only 10.3% meet the target blood pressure [1]. In contrast, in high-income countries, the treatment rate seats at 40% with 25% of patients meeting the blood pressure target [1].
Emphasizing the importance of HTN management, every 10 mmHg reduction in systolic blood pressure level can decrease the risk of future cardiovascular events by up to 25% [2]. A screening program is of great value in identifying HTN at early stages, proposing treatment options and providing support for patients in managing their condition. Treatment options vary based on the degree of HTN progress. At the early stages, dietary and lifestyle changes have shown to be sufficient in controlling HTN. However, as the condition progress and is left untreated, pharmaceutical approach may be warranted to achieve optimal blood pressure control [2,3,4]. It is estimated that the prevalence of HTN will increase by more than twofold in the Middle East by 2025 [3]. This is a significant concern and calls on the Middle Eastern countries to develop a presentational strategy. Studies on the prevalence, awareness, treatment, and control rate of HTN are needed to set the path for the public health officials in developing these programs. The majority of studies have been conducted on high-income countries, with a handful focused on the Middle East and North Africa (MENA) region. Since there is not systematic review and meta-analysis based on individual and aggregated data to estimate the overall status of hypertension in the MENA region, thus this study aimed to pool data and estimate the long-term prevalence of pre-hypertension (pre-HTN), HTN, awareness, treatment, and control in this region.
Methods
This systematic review and meta-analysis were conducted based on the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) statement [4].
Search Strategy
A systematic literature search was conducted in electronic databases, including MEDLINE/ PubMed, Google Scholar, EMBASE, Web of Science, and Scopus, for articles about the prevalence of pre-HTN, HTN, awareness, treatment, and management between databases inception and October 21, 2020. Searches were performed using the terms “pre-HTN,” “HTN,” “awareness,” “treatment,” and “control,” and other related keywords according to the search strategy of each database (Appendix Table 3). Searched was performed by one investigator, and the results were reviewed by another investigator.
Eligibility Criteria and Selection Study
All cross-sectional studies, in English that investigated the prevalence of pre-HTN, HTN, awareness, treatment, and control rate in adults and older adults (age ≥ 18 years), were included. All prevalence survey that selected sample participants represented the target population so that the age and sex structure of the sample was consistent with the target population structure for at national or subnational level were included in this study. For multiple publications that used the same source of data, the most recent publication was included. After removing duplicated studies, and removing all self-report studies on the subject, two investigators independently (NM and ES) examined the title, abstract, and full text of related studies, with respect to the eligibility criteria. Probable discrepancies were based on the third expert’s opinion (MQ).
Data Extraction Strategy
Two independent investigators performed data extraction with an electronic data extraction form (NM and ES). The following data was extracted: first author, population, study year, sample size, male/female ratio, age (mean or range), HTN definition (cutoff point), level of study, and prevalence/proportion with 95% confidence interval (CI) for each outcome. Any probable discrepancy was resolved based on the third expert’s opinion.
Definition
Awareness, treatment, and control rate of HTN were calculated in the included studies as the proportion of participants with HTN who were aware of their disease, who were treated, and whose HTN was controlled.
Quality Assessment
Quality assessment of included studies was done based on the Newcastle–Ottawa Scale adapted for cross-sectional studies. The scale has seven items and is consisted of selection, comparability, and outcome components. The total score ranged from 0 to 10, with a higher score indicating a lower risk of bias. Quality assessment of studies was categorized as follows: 0 to 4 for “unsatisfactory studies,” 5–6 points for “satisfactory studies,” 7–8 points for “good studies,” and 9–10 points for “very good studies.” The quality assessment was conducted independently by two investigators (NM and ES). Probable discrepancies were resolved based on the third expert’s opinion (MQ).
Statistical Analysis
Heterogeneity between studies was assessed using Cochran’s Q test and I-squared. Due to sever heterogeneity between studies, a random effect model was used to pool prevalence of HTN [5]. A meta-analysis of proportions was used to calculate the pooled prevalence of HTN, awareness, treatment, and control rates [6]. The subgroup meta-analysis was performed based on gender, study period, level of income, HTN definition, study level (regional, sub-national, national), country, and year. Subgroup analysis, according to the country income level, was done according to the World Bank income classifications [7]. Pooled prevalence, awareness, treatment, and control rates of HTN at country level were estimated for countries with more than 4 studies. Subgroup analysis was categorized into studies conducted from 1990 to 1999, 2000 to 2009, and 2010 to 2020. Sensitivity analysis was performed to estimate the long-term trends in prevalence, awareness, treatment, and control rates of HTN according to standard definition of HTN (definition of HTN as systolic blood pressure of 140 mm Hg or more, or diastolic blood pressure of 90 mm Hg or more, or being on pharmacological treatment). In sensitivity analysis, studies which used other definitions were excluded from analysis. Meta-regression model was fitted to explain the heterogeneity in terms of study-level covariates. STATA 14 (StataCorp, College Station, TX, USA) was used for the analysis.
Results
Search Results
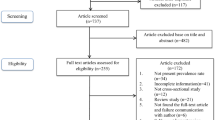
Overall, 2892 studies extracted from the initial search. Upon exclusion of 549 duplicate reviews, the titles, abstracts, and full text of reviews were examined. Totally 178 studies [8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133,134,135,136,137,138,139,140,141,142,143,144,145,146,147,148,149,150,151,152,153,154,155,156,157,158,159,160,161,162,163,164,165,166,167,168,169,170,171,172,173,174,175,176,177,178,179,180,181,182,183,184,185] met the inclusion criteria. The screening and selection processes of studies are summarized in Fig. 1.

Studies search and review flowchart
Qualitative Synthesis
The studies were conducted in the 17 MENA countries from 1992 to 2020. Studies comprised of 2,262,797 participants with a mean age of 45.72 ± 8.84 years. Appendix Table 4 shows the general characteristics and the estimated prevalence of pre-HTN and HTN and also awareness, treatment, and control rates of HTN in the included studies. The most included studies were conducted in Iran (107 studies), and the least were conducted in Qatar and Syria (one study). Totally 140 reported prevalence used 140/90 mmHg, 21 used 130/90 mmHg, and 17 used 160/90 mm Hg as the cutoff for the diagnosis of HTN. The rate of awareness, treatment, and control of HTN varied among countries. Jordan had the highest awareness rate with 62% (59, 66), and Lebanon had the highest treatment and control rate of HTN with 45% (31, 58) and 27% (16, 38), respectively. Overall rate of HTN awareness ranged from 12 (10–14; Syria) to 69% (63–75; Jordan). Overall rate of HTN treatment ranged from 8 (7–11; Syria) to 78% (75–81; Iran).
Quantitative Synthesis
Sever heterogeneity was noted among the included studies in all subgroups of pre-HTN and HTN prevalence and awareness, treatment, and control rate of HTN (I-squared = 99.95, 99.90, 99.34, 99.46, 99.58%, respectively, P < 0.001). Therefore, meta-analysis was performed using random effect model.
Prevalence of Pre-HTN and HTN
The pooled prevalence of pre-HTN and HTN according to gender, population, level of income, HTN definition, and level of studies are illustrated in Table 1. The pooled prevalence of pre-HTN was 33% (95% CI 28, 39). Pre-HTN was more prevalent in males (40%) than females (30%). Pre-HTN was more prevalent in the high-income countries and at national level.
The pooled prevalence of HTN was 26% (25, 27). The highest and lowest pooled prevalence of HTN was in low-middle-income (29%) and high-income countries (24%). The highest prevalence of HTN was reported in studies used the cutoff of 130/90 mm Hg as the definition of HTN. Over the past three decades, the prevalence of hypertension increased significantly in the region (7% increment).
The highest pooled prevalence of HTN in the region was observed in United Arab Emirates with 36% (28–43). Over the three past decades, prevalence of HTN in Iran increased from 22 (1990–2000) to 26% (2010–2020).
HTN Awareness, Treatment, and Control Rates
The pooled awareness, treatment, and control rates of HTN according to gender, population, level of income, HTN definition, and level of studies are illustrated in Table 2. By random effect model, the pooled awareness, treatment, and control rates were 50% (48, 53), 41% (38, 44), and 19% (17, 21), receptively. The pooled awareness, treatment, and control rates were lower significantly in men than women. While the highest awareness of HTN was in upper-middle-income countries with 52% (49, 55), high-income countries had highest rate of treatment and control of HTN with 43% (33, 53) and 25% (17, 33), respectively. The pooled awareness, treatment, and control rates of HTN in studies that used cutoff 160/90 mm Hg for definition were higher in comparison to other definitions. Based on study level, the highest awareness, treatment, and control rates of HTN were at subnational level.
The highest pooled awareness rate of HTN was observed in Jordan (61%), and in all other countries, the awareness rate was approximately 50%. The pooled treatment rates of HTN ranged 40–47% at country level in the region. The highest and lowest pooled control rates of HTN were observed in Lebanon and Turkey, respectively (Appendix Table 5).
Sensitivity Analysis
Sensitivity analysis according to definition of HTN for pooled prevalence of HTN, awareness, treatment, and control rates is presented in Fig. 2. As it shows in the forest plot (Fig. 3), the pooled prevalence of HTN, awareness, treatment, and control rates did not change significantly according to HTN cutoff point > 140/90 mmHg compare to all definitions. According to standard definition of HTN (> 140/90 mm Hg), over the past three decades, the prevalence of hypertension increased linearly in the region. Although over the past three decades, the pooled awareness and treatment rates of HTN did not change significantly, the pooled control rate improved significantly in the region (approximately 10% improvement in the two recent decades) (Fig. 2).

Forest plot of pooled prevalence, awareness, treatment, and control rate of hypertension according to definition of hypertension in the MENA region

Forest plot of pooled prevalence, awareness, treatment and control rates of hypertension according to definition of hypertension more than 140/90 mmHg by study period in the MENA region
Meta-regression
The results of meta-regression showed that heterogeneity among the included studies explained by level of income and level of study for pre-HTN, by mean age of study population, country, level of study for the prevalence of HTN, by mean age of study population and definition for awareness and treatment rate, and by mean age of study population, definition, and level of study for control rate (Appendix Table 6).
Discussion
In the present comprehensive systematic review and meta-analysis study on the prevalence of HTN and its management in 17 MENA countries between 1992 and 2020, the pooled prevalence of pre-HTN and HTN was estimated to be 33% and 26%, respectively. In this regard, the results of a large population-based cohort of Chinese, Malay, and Indian populations showed the HTN prevalence of 31.1% [186]. In a multinational cross-sectional study from six Latin American countries, HTN prevalence was reported as 44%, which is significantly higher than the prevalence rate in the MENA countries [187]. The global prevalence of pre-HTN and HTN in adults has been estimated at 36% and 31%, respectively, in the systematic analyses of population-based studies [188, 189], which is above the MENA countries. Healthcare infrastructure for HTN screening, access to health services, as well as social and economic status could account for this discrepancy.
Pre-HTN was more common in males and high-income countries, while HTN was more prevalent in low-middle-income countries. It seems that there is a relationship between the prevalence of pre-HTN and HTN and the socio-economic status (SES). Results of a meta-analysis confirmed an association between low SES and high blood pressure [190]. However, another opinion is that in developed countries, lower SES is associated with a higher prevalence of HTN. In contrast, in developing countries, higher SES is accompanied by higher HTN prevalence due to higher sodium and alcohol intakes and a higher prevalence of obesity [191].
Moreover, the prevalence of HTN in male and female was not statistically different. This finding is inconsistent with previous studies [153, 192]. To the extent of that in a multi-ethnic cross-sectional survey in the Asian population, age and education have been consistently associated with HTN across all ethnic groups [186].
This systematic review showed that the prevalence of pre-HTN and HTN varied widely in different countries. Early detection of pre-HTN is essential to prevent the development of HTN through cost-effective dietary programs, lifestyle modifications, and regular blood pressure measurements. Reducing tobacco, alcohol and sodium intake, as well as increasing physical activity and consumption of fruits and vegetables are worth considering as a primary prevention method for HTN [193].
Our findings showed that the prevalence HTN increased significantly in the region (7% increment). In contrast, an analysis of nationally representative surveys of high-income countries reported no noticeable change in HTN prevalence from 1976 to 2017, with some age and sex groups showing a decline or increment in prevalence rate [194]. It seems that strategies such as developing evidence-based guidelines for healthcare providers and implementing regular blood pressure measurements have been useful in controlling HTN [194].
The overall awareness, treatment, and control rates of HTN in the MENA countries were estimated at 50%, 41%, and 19%, respectively. About half of the patients with HTN in the MENA were aware of their disease; however, only one-fifth of the patients have managed to control their blood pressure. While in Africa, the treatment and control rate was reported at 59.9% and 24.6%, respectively [195], and the treatment rate reached 82% in Canada [196]. In a multinational population-based study, 46.5% of participants with HTN were aware of their disease, with a controlled rate of 32.5%, which is higher than the MENA [168]. The observed differences in HTN awareness and treatment among countries may be attributable to variations in lifestyle and cultural factors [197, 198].
During the past two decades, the pooled control rate of HTN improved significantly in the region (approximately 10% improvement in the two recent decades). Analysis of 12 high-income countries’ national surveys revealed improvement in HTN awareness, treatment, and control since the 1980s and 1990s. However, the control rates have been plateaued during the past decade in these countries [194].
The low control rate of HTN and the gap between detection and treatment of HTN could be attributed to the high cost of anti-hypertensive agents, poor access to physicians and healthcare facilities, and plow perceptions of the benefit of adherence to medications. Therefore, based on the results of previous experiences, the use of polypill as a combination therapy and initial treatment with non-physician healthcare workers could be reasonable strategies for the prevention and control of HTN in low- and middle-income countries [199].
Regarding the awareness, treatment, and control of HTN, the women and high-income countries had a higher rate. In agreement with similar studies conducted on the Asian population [186], men were more likely to be left undetected and untreated than women. Moreover, in high SES countries, the awareness and control of HTN are generally better because of high access to healthcare services and higher literacy levels [168, 186, 200, 201].
The rate of awareness, treatment, and control of HTN could be translated to the overall healthcare system performance at the national level. In the present study, although the prevalence of HTN in Iran has increased over the past two decades, the level of awareness, treatment, and control of HTN has slightly improved. In a meta-analysis that was conducted on 417,392 Iranian adults, the prevalence of HTN was estimated at 20%, which is comparable to the findings of this review [192].
There has been no other comparative study of long-term trends in HTN prevalence, awareness, treatment, and control in the MENA. The meta-analysis approach with comprehensively investigating databases in the longest possible time to determine the prevalence of HTN was the advantage of this study. One of the limitations of the present study is that some studies did not include prevalence information by gender and other categories. Another limitation was the unequal number of studies in different countries. Moreover, methodological differences between included studies and over time caused high heterogeneity among studies should not be overlooked completely, although we performed subgroup and metaregression analysis. Also, the quality score of some of the included individual studies was low, which could have affected our results.
Conclusion
The result of this study showed that HTN is a significant public health problem in the MENA countries. About half the patients with HTN are unaware of their medical condition. Although the diagnosed patients receive relatively good treatment, the condition is controlled only in a small number of patients. The present study provides a great tool for public health authorities in the MENA to understand the status of screening, prevention, and treatment in their countries. Implementing clinical guidelines with simplified recommendations, alongside regular screening, and physician consultation could provide a major benefit in managing HTN.
References
Fakhrzadeh H, et al. Coronary heart disease and associated risk factors in Qazvin: a population-based study. 2008.
Khogali M. The cardiovascular disease prevention initiative. First attempt to a community based approach in the Arab World (1998–2001). 2002
Perkovic V, et al. The burden of blood pressure-related disease. Hypertension. 2007;50(6):991–7.
Moher D, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA Statement. Open Medicine. 2009;3(3):e123.
Higgins JP, et al. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60.
Nyaga VN, Arbyn M, Aerts M. Metaprop: a Stata command to perform meta-analysis of binomial data. Archives of Public Health. 2014;72(1):39.
Hamida F, et al. Prevalence of hypertension in El-Menia oasis, Algeria, and metabolic characteristics in population. in Annales de Cardiologie et d’Angeiologie. 2013.
Ben Khedda S, Temmar M, Bendaoud N, et al. Prevalence of hypertension in Algeria: results from a national survey. Mustapha Hospital Medical School. 2005.
Latifa BH, Kaouel MJCdéedrfS. Cardiovascular risk factors in Tlemcen (Algeria). 2007;17(3):153–158.
Temmar M, et al. Prevalence and determinants of hypertension in the Algerian Sahara. 2007;25(11):2218–26.
El-Zanaty F, Way A, Demographic E, Survey H. Cairo, Egypt: Ministry of Health, El-Zanaty and Associates, and Macro International. Int Fam Plan Perspect. 2008;2009(29):158–66.
Ibrahim MM, et al. Hypertension prevalence, awareness, treatment, and control in Egypt. Results from the Egyptian National Hypertension Project (NHP). NHP Investigative Team. Hypertension. 1995;26(6 Pt 1):886–90.
Mohamed M, et al. Hypertension control indicators among rural population in Egypt. 2000;75(5–6):391–401.
Akbar-Zadeh F, et al. Prevalence of cardiovascular diseases and cardiac risk factors in northwestern Tabriz. Med J Tabriz Univ Med Sci Health Serv. 2003;59(11).
Amiri M, et al. The prevalence of hypertension and associated coronary risk factors in Bushehr Port. Iranian South Med J. 2000;3:34–9.
Fakhrzadeh H, PR, Amininik S, Mahbubnia M. Hypertension in Bushehr population aged over 19 years old [in Persian]. Iranian South Med J. 1998.
Fakhrzadeh H, Nabipour I, Dehdari A. The association of hypertension and ischemic heart disease: a populationbased study [in Persian]. Iranian South Med J. 2001;2001.
Latifi S, Mozafari A. Determination of the prevalence of hypertension among the over thirty years, old population in Ahwaz City. 2000.
Mostafavi H, ZN. Prevalence of hypertension in elderly population of Shiraz [In Persian]. Med J Tabriz Univ Med Sci Health Serv. 2004.
Mostafavi H. Blood pressure distribution among people residing in the city of Shiraz. 2002.
Navaei L, et al. Epidemiologic survey on hypertension and its relation with obesity, diabetes, and hyperlipidemia in Islamshahr. Iran J Shaheed Beheshti Univ Med Sci Health Serv. 1998;2:40–52.
Navaei L, Mehrabi YE, Azizi F. An epidemiologic study of hyperlipidemia, obesity, and hypertension in Tehran villages. 2000.
Shahbazpour N. Prevalence of overweight and obesity and their relation to hypertension in adult male university students in Kerman, Iran. International Journal of Endocrinology and Metabolism. 2003;1(2).
Abdollahi A, et al. Epidemiology of hypertension among urban population in Golestan province in north of Iran. 2007.
Abtahi F, et al. Correlation between cigarette smoking and blood pressure and pulse pressure among teachers residing in Shiraz, Southern Iran. 2011.
Aghaei Meybodi HR, et al. Prevalence of hypertension in an Iranian population. 2014;36(1):87–91.
Agha SK, et al. The prevalence of coronary risk factors in Iranian lor migrating tribe. 2008.
Agheli N. L’évaluation des facteurs de risque des maladies cardiovasculaires chez la population iranienne: rôle de l’hypertriglycéridémie. Angéiologie (Paris). 2006;58(3):24–7.
Ahmadi A, et al. Prevalence of cardiovascular risk factors in the elderly of Yasuj. 2000.
Alikhani S, et al. A province-based surveillance system for the risk factors of non-communicable diseases: a prototype for integration of risk factor surveillance into primary healthcare systems of developing countries. Public Health. 2009;123(5):358–64.
Amiri M, et al. Risk factors of cardiovascular diseases in Bushehr port on the basis of the WHO MONICA Project. The Persian Gulf Healthy Heart Project. ISMJ. 2004;6(2):151–161.
Amiri ZM, et al. Hypertension in iranian urban population: prevalence, awareness, control and affecting factors. La Prensa Medica Argentina. 2015;101:4.
Amir KF, et al. Assessment of blood pressure status and its relationship with anthropometric indices among women in rural areas of Kerman province, Iran. 2008.
Arefi SH, et al. Prevalence, patient awareness and control rates of high blood pressure in the adult population of Tehran: a report from the Tehran Blood Pressure Study, 1990–1991. Med J Islam Repub Iran. 1996;10(2):125–35.
Asgari S, et al. Status of hypertension in Tehran: potential impact of the ACC/AHA 2017 and JNC7 guidelines, 2012–2015. Sci Rep. 2019;9(1).
Azimi-Nezhad M, et al. Newly detected hypertension in an Iranian population: an epidemiological study. Asian Biomed. 2010;3(6):653–62.
Azizi F, Esmaeilzadeh A, Mirmiran P. Obesity and cardiovascular risk factors: an epidemiological study in Tehran [in Persian], Iran. J Endocrinol Metabol. 2004;5(suppl 4):389–397.
Azizi F, et al. Glucose intolerance and cardiovascular risk factors in Tehran urban population:“Tehran Lipid and Glucose Study.” Iranian Journal of Endocrinology and Metabolism. 2001;3(4):247–56.
Azizi A, et al. The prevalence of hypertension and its association with age, sex and BMI in a population being educated using community-based medicine in Kermanshah: 2003. 2008;10(4):323–329.
Azizi F, et al. Serum lipid levels in an Iranian adults population: Tehran Lipid and Glucose Study. Eur J Epidemiol. 2003;18(4):311–9.
Azizi F, et al. Distribution of blood pressure and prevalence of hypertension in Tehran adult population: Tehran Lipid and Glucose Study (TLGS), 1999–2000. J Hum Hypertens. 2002;16(5):305–12.
Badakhsh MH, et al. Prehypertension; patient awareness and associated cardiovascular risk factors in an urban population in Iran. Med J Islam Repub Iran. 2015;29(1):1124–8.
Barikani A. Prevalence of hypertension among women aged 30+ in Minoodar region of Qazvin in 2009. The Journal of Qazvin University of Medical Sciences. 2010;14(1):41–8.
Baroogh N, et al. Hypertension and lifestyle in 24–65 year old people in Qazvin Kosar region in 2007. Pajoohandeh Journal. 2010;15(5):193–8.
Behforuz M, Sajadi M, SAYADI AAR. Prevalence, awarness, treatment and control of hypertension, in people over 18 years old in Rafsanjan. 2002.
Boskabadi MH, EM., Hasanzadeh AA, Salimi N, Ghamami G, Mazlom R, Haji Zadeh S. Study of the blood pressure in subjects older than eighteen years in Mashhad. Physiol Pharmacol. 2006;9:195–202.
Chaman R, et al. Investigating hypertension prevalence and some of its influential factors in an ethnically variant rural sample. 2008;3:39–42.
Dabaghmanesh MH, Mostafavi H, Zare N. blood pressure levels, risk factors and hypertension control status in adult population of shiraz. Hormozgan Medical Journal. 2007;11(1).
Delavari A, et al. Prevalence of hypertension in Iranian urban and rural populations aged over 20 years in 2004. 2007;17(58):79–86.
Delpishe A, SK. Blood pressure in Illam workers above 40 years old and its correlation with their lifestyle and BMI [in Persian]. J Illam Univ Med Sci Health Serv. 2000;9(32 & 33):11–17.
Ebrahimi M, et al. Social disparities in prevalence, treatment and control of hypertension in Iran: second national surveillance of risk factors of noncommunicable diseases, 2006. 2010;28(8):1620–1629.
Ebrahimi M, et al. Prevalence of hypertension, pre-hypertension and undetected hypertension in Mashhad, Iran. 2016;9(3):213–23.
Eghbali M, et al. Prevalence, awareness, treatment, control, and risk factors of hypertension among adults: a cross-sectional study in Iran. Epidemiol Health. 2018;40:e2018020.
Esteghamati A, et al. Awareness, treatment and control of pre-hypertension and hypertension among adults in Iran. Arch Iran Med. 2016;19(7):456–64.
Esteghamati A, et al. Third national surveillance of risk factors of non-communicable diseases (SuRFNCD-2007) in Iran: methods and results on prevalence of diabetes, hypertension, obesity, central obesity, and dyslipidemia. BMC Public Health. 2009;9.
Esteghamati A, et al. Prevalence, awareness, treatment, and risk factors associated with hypertension in the Iranian population: the national survey of risk factors for noncommunicable diseases of Iran. Am J Hypertens. 2008;21(6):620–6.
Fakhrzadeh H, Batoei M, Faridnia P, Taeb M. Overweight and obesity in oil industry workers on Kharg Island [in Persian]. Iranian South Med J. 2002.
Fakhrzadeh H, et al. Prevalence of hypertension and correlated risk factors among 25–64 aged inhabitants of Tehran University of medical sciences population lab region. 2004;3:37–43.
Farzadfar F, et al. Effectiveness of diabetes and hypertension management by rural primary health-care workers (Behvarz workers) in Iran: a nationally representative observational study. Lancet. 2012;379(9810):47–54.
Fatahi E, Ghandchilar N. Study of hypertension in urban and rural population of Tabriz and its correlation with various factors. 2000.
Gandomkar A, et al. Prevalence, awareness, treatment, control, and correlates of hypertension in the pars cohort study. Arch Iran Med. 2018;21(8):335–43.
Ghanbarian A, et al. Distribution of blood pressure and prevalence of hypertension in Tehran adult population: Tehran Lipid And Glucose Study. Iranian Journal Of Endocrinology And Metabolism (IJEM). 2004;5(Supplement (4)).
Gharipour M, et al. The impact of a community trial on the pharmacological treatment in the individuals with the metabolic syndrome: findings from the Isfahan Healthy Heart Program, 2001–2007. Arch Med Sci. 2012;8(6):1009–17.
Ghazanfari Z, et al. Prevalence of coronary artery diseases risk factors in Kerman. Iranian Journal Of Critical Care Nursing (IJCCN), 2010;3(1).
Faramarzi H, et al. The comparison of prevalence of diabete and hypertension between rural areas of fars and rural area of EMRO region. Iranian Journal of Endocrinology and Metabolism. 2011;13(2):157–164+225.
Ghorbani Z, et al. Hypertension prevalence, awareness, treatment and its correlates among people 35 years and older: Result from pilot phase of the Azar cohort study. J Educ Health Promot. 2018;7:45.
Goodarzei MR, et al. Hypertension prevalence in over 18-year-old population of Zabol. 2005;11(43):.
Hadaegh F, et al. Prehypertension tsunami: a decade follow-up of an Iranian Adult Population. PLoS One. 2015;10(10):e0139412.
DH. Epidemiological study of blood pressure rate in Arak city, 1997–98. Arak Med Univ J 1999;2:13–17.
Kazem M, M-AHI. Iranian health profile survey. Iranian Ministry of Health, Department of Research, Tehran, Iran. 1999.
Jahromi MK, et al. Risk factors of heart disease in nurses. Iran J Nurs Midwifery Res. 2017;22(4):332–7.
Janghorbani M, et al. Nationwide survey of prevalence and risk factors of prehypertension and hypertension in Iranian adults. J Hypertens. 2008;26(3):419–26.
HJ. Prevalence of hypertension among the over 20 years old population in Qazvin city. J Qazvin Univ Med Sci. 2008;3:23–29.
Azimiyan J, et al. Prevalence of cardiovascular risk factors among women in Minoodar district of Qazvin; interventional propositions. QUMS. 2009;13(2):35–42.
HR J. Prevalence of hypertension in Qazvin [in Persian]. J Qazvin Univ Med Sci Health Serv. 1999;9:23–29.
Kalani Z, et al. Hypertension in the Yazd adult population. Payesh (Health Monitor) 2011;10(1):101–107.
Kassaei SA, et al. Hypertension awareness, treatment, control and prevalence in Zanjan province, Iran. 2010.
Katibeh M, et al. Hypertension and associated factors in the Islamic Republic of Iran: a population-based study. 2019;25.
Kazemi T, et al. Prevalence and determinants of hypertension among Iranian adults, Birjand, Iran. Int J Prev Med. 2017;8:36.
Kazemi T, et al. Prevalence of pre-hypertension and risk factors in an Iranian population: east of Iran. Int Cardiovasc Res J. 2018;12(1):34–7.
Kelishadi R, et al. Cardiovascular disease risk factors, metabolic syndrome and obesity in an Iranian population. 2008.
Khadirsharbiani VM. A Study of prevalence of coronary artery disease risk factors in arak city and role of training program in their modifications. Arak Med Univ J. 2001;4:13–16. [Persian].
Khajedaluee M, et al. The prevalence of hypertension and its relationship with demographic factors, biochemical, and anthropometric indicators: a population-based study. ARYA Atherosclerosis. 2016;12(6):259–65.
Khani M, et al. Prevalence of hypertension and some related risk factors in rural population affiliated to Tarom Health Network in 2001. 2002;10(40).
Khosravi A, et al. The impact of a 6-year comprehensive community trial on the awareness, treatment and control rates of hypertension in Iran: experiences from the Isfahan healthy heart program. BMC Cardiovasc Disord. 2010;10:61.
Malekzadeh MM, et al. Prevalence, awareness and risk factors of hypertension in a large cohort of Iranian adult population. J Hypertens. 2013;31(7):1364–71. discussion 1371.
Maracy MR, Feizi A, Bagherynejad M. The prevalence and correlated determinants of hypertension and type 2 diabetes: a large community-based study in Isfahan, Iran. Pakistan Journal of Medical Sciences. 2012;28(2):247–52.
Mardani M, et al. Association of waist to hip ratio and hypertention among people referred to urban health clinics in Arak city in 2008. scientific magazine yafte. 2009;11(3):63–71.
Sarraf-Zadegan N, Sajady F. Hypertension and diabetes situation in the Eastern Mediterranean Region: with special reference to Iran. In: Frontiers in Cardiovascular Health. Springer; 2003. p. 451–72.
Mohamadi-Fard N, et al. The prevalence of cardiovascular risk factors in rural and urban population of Isfahan & Markazi provinces. J Qazvin Univ Med Sci. 2003;7(2):5–14.
Mohtasham-Amiri Z, et al. Hypertension in the lowest decile income population of Guilan, North of Iran. 2018;36:e342–3.
Naghibi M, et al. Prevalence of chronic kidney disease and its risk factors in Gonabad, Iran. Iranian Journal of Kidney Diseases. 2015;9(6):449–53.
Naghavi M. The survey of hypertension prevalence in Gonabad City. 2000.
Najafipour H, et al. Hypertension: diagnosis, control status and its predictors in general population aged between 15 and 75 years: a community-based study in southeastern Iran. Int J Public Health. 2014;59(6):999–1009.
Namayandeh S, et al. Hypertension in Iranian urban population, epidemiology, awareness, treatment and control. Iran J Public Health. 2011;40(3):63–70.
Nikpour M, et al. Shift work and metabolic syndrome: a multi-center cross-sectional study on females of reproductive age. Biomedical Reports. 2019;10(5):311–7.
Palafox B, et al. Wealth and cardiovascular health: a cross-sectional study of wealth-related inequalities in the awareness, treatment and control of hypertension in high-, middle- and low-income countries. Int J Equity Health. 2016;15(1):199.
Peymani P, et al. The prevalence of high blood pressure and its relationship with anthropometric indicators; a population based study in Fars Province, IR Iran. 2012;6(2).
Rajati F, et al. Prevalence, awareness, treatment, and control of hypertension and their determinants: Results from the first cohort of non-communicable diseases in a Kurdish settlement. 2019;9.
Ramezani MA, et al. Determinants of awareness, treatment and control of hypertension in Isfahan. Central Iran Archives of Medical Science. 2009;5(4):523–30.
Ramezankhani A, et al. Classification-based data mining for identification of risk patterns associated with hypertension in Middle Eastern population: a 12-year longitudinal study. 2016;95(35).
Rezazadehkermani MJAIM. Epidemiology and heterogeneity of hypertension in Iran: a systematic review. 2008;11(4):444–52.
Roohafza H, et al. Stress as a risk factor for noncompliance with treatment regimens in patients with diabetes and hypertension. ARYA Atherosclerosis. 2016;12(4):166–71.
Sadeghi M, Roohafza HR, Kelishadi R. Blood pressure and associated cardiovascular risk factors in Iran: Isfahan Healthy Heart Programme. Med J Malaysia. 2004;59(4):460–7.
Sadeghi E, et al. Controlled blood pressure in Iranian patients: a multi-center report. Glob J Health Sci. 2015;8(4):188–95.
Safari Moradabadi A, et al. Prevalence of hypertension and respective risk factors in adults in Bandar Abbas, Iran. Hormozgan Medical Journal, 2014;18(3).
Sahraki M, et al. Hypertension among 30+ year-old people in Zahedan (Southeast of Iran). 2011.
Sarraf Zadegan N, et al. Prevalence of hypertension and associated risk factors in Isfahan, Islamic Republic of Iran. 1999.
Sarraf Zadegan N, AminiNik S. Blood pressure pattern in urban and rural areas in Isfahan, Iran. J Hum Hypertens. 1997;11(7):425–8.
Sarraf-Zadegan N, Boshtam M, Rafiei M. Risk factors for coronary artery disease in Isfahan, Iran. Eur J Public Health. 1999;9(1):20–26.
Sepanlou SG, et al. Hypertension and mortality in the Golestan Cohort Study: a prospective study of 50 000 adults in Iran. J Hum Hypertens. 2016;30(4):260–7.
Shirani S, et al. Awareness, treatment and control of hypertension, dyslipidaemia and diabetes mellitus in an Iranian population: the IHHP study. East Mediterr Health J. 2009;15(6):1455–63.
Tabrizi JS, et al. Prevalence and associated factors of prehypertension and hypertension in Iranian Population: the Lifestyle Promotion Project (LPP). 2016;11(10):e0165264.
Gharipour M, et al. PP.29.15: Anthropometric indices predicting incident hypertension in an Iranian population: the Isfahan Cohort Study. J Hypertens. 2015;33:E394.
Taleban A, S-ZM, Ranjbar-Bafghi A, Amraei A. Prevalence of systemic arterial hypertension in male in Yazd. J Shahid Sadughi Univ Med Sci Health Serv. 1999.
Veghari G, et al. Impact of literacy on the prevalence, awareness, treatment and control of hypertension in adults in Golestan province (northern Iran). Caspian J Intern Med. 2012;4(1):580–4.
Yazdanpanah L, et al. Prevalence, awareness and risk factors of hypertension in southwest of Iran. J Renal Inj Prev. 2015;4(2):51–6.
Yazdanpanah K, Ghanei H, Ahmadi A. Study of prevalence of hypertension and its relation with age, height, and hyperlipidemia among above ten-year-old population of Sanandaj [in Persian]. Scientific J Kurdisatn Univ Med Sci. 1998;10:14–18.
Yusufali AM, et al. Prevalence, awareness, treatment and control of hypertension in four Middle East countries. J Hypertens. 2017;35(7):1457–64.
Zarei M, Abavi-Sani SA, Khalili H, Ghasemi SH. Survey on impact of socio-individual factors in hypertensives above thirty years of age in Sabzevar [in Persian]. Asrar J Sabzevar School Med Sci. 1996;2:48–53.
Saka M, Shabu S, Shabila N. Prevalence of hypertension and associated risk factors in a population sample of older adults in Kurdistan, Iraq. 2019. 25: p. 2–2.
Abu-Saad K, et al. Blood pressure level and hypertension awareness and control differ by marital status, sex, and ethnicity: a population-based study. Am J Hypertens. 2014;27(12):1511–20.
Amad S, Rosenthal T, Grossman EJJohh. The prevalence and awareness of hypertension among Israeli Arabs. 1996;10:S31–3.
Ikeda N, et al. Control of hypertension with medication: a comparative analysis of national surveys in 20 countries. Bull World Health Organ. 2014;92(1):10–9.
Ajlouni K, Jaddou H, Batieha A. Obesity in Jordan. Int J Obes. 1998;22(7):624–8.
Jaddou HY, Bateiha AM, Ajlouni KM. Prevalence, awareness and management of hypertension in a recently urbanised community, eastern Jordan. J Hum Hypertens. 2000;14(8):497–501.
Jaddou H, et al. Hypertension prevalence, awareness, treatment and control, and associated factors: results from a national survey, Jordan. 2011;2011.
Jaddou HY, et al. Epidemiology and management of hypertension among Bedouins in Northern Jordan. 2003;24(5):472–6.
Khader Y, et al. Hypertension in Jordan: prevalence, awareness, control, and its associated factors. 2019. 2019.
Abolfotouh MA, et al. Prevalence of hypertension in south-western Saudi Arabia. 1996;2(2):211–8.
Al-Baghli NA, et al. Control of hypertension in eastern saudi arabia: results of screening campaign. J Family Community Med. 2009;16(1):19–25.
Al-Nozha MM, Ali MS, Osman AKJAoSm. Arterial hypertension in Saudi Arabia. 1997;17(2):170–174.
Al-Shammari SA, et al. Blood lipid concentrations and other cardiovascular risk factors among Saudis. Fam Pract. 1994;11(2):153–158.
Aldiab A, et al. Prevalence of hypertension and prehypertension and its associated cardioembolic risk factors; a population based cross-sectional study in Alkharj, Saudi Arabia. 2018;18(1):1327.
Al-Nozha MM, et al. Hypertension in saudi arabia. 2007;28(1):77.
Al-Nozha MM, Osman AK. The prevalence of hypertension in different geographical regions of Saudi Arabia. 1998;18(5):401–407.
El Bcheraoui C, et al. Hypertension and its associated risk factors in the kingdom of saudi arabia, 2013: a national survey. 2014;2014.
Elkhalifa AM, et al. Prevalence of hypertension in a population of healthy individuals. 2011;20(2):152–5.
Osman A, Al Nozha M. Risk factors of coronary artery disease in different regions of Saudi Arabia. EMHJ-Eastern Mediterranean Health Journal. 2000;6(2–3):465–474.
Saeed AA, et al. Prevalence, awareness, treatment, and control of hypertension among Saudi adult population: a national survey. 2011;2011.
Soyannwo M, et al. Contrasting influence of the living environment and gender on systemic hypertension in Saudi population of Gassim, Saudi Arabia. Afr J Med Med Sci. 1997;26(3–4):145–52.
Wahid AS, et al. Prevalence of hypertension and sociodemographic characteristics of adult hypertensives in Riyadh City, Saudi Arabia. 1996;10(9):583–7.
Warsy A, El Hazmi M. Diabetes mellitus, hypertension and obesity-common multifactorial disorders in Saudis. EMHJ-Eastern Mediterranean Health Journal. 1999;5(6):1236–1242.
Cherfan M, et al. Prevalence and risk factors of hypertension: a nationwide cross-sectional study in Lebanon. 2018;20(5):867–79.
Dhalla N, et al. Hypertension and diabetes situation in the Eastern Mediterranean Region: with special reference to Iran. Frontiers in Cardiovascular Health. 2012;9:7.
Matar D, et al. Prevalence, awareness, treatment, and control of hypertension in Lebanon. 2015;17(5):381–388.
Mouhtadi BB, et al. Prevalence, awareness, treatment, control and risk factors associated with hypertension in Lebanese adults: a cross sectional study. 2018;2018(1).
Noubani A, et al. Prevalence, awareness, and control of hypertension in Greater Beirut Area, Lebanon. Int J Hypertens. 2018;2018:5419861.
Tohme R, Jurjus A, Estephan A. The prevalence of hypertension and its association with other cardiovascular disease risk factors in a representative sample of the Lebanese population. 2005;19(11):861.
Beaney T, et al. May Measurement Month 2018: a pragmatic global screening campaign to raise awareness of blood pressure by the International Society of Hypertension. 2019;40(25):2006–2017.
Tazi MA, et al. Prevalence of the main cardiovascular risk factors in Morocco: results of a National Survey, 2000. J Hypertens. 2003;21(5):897–903.
Adeloye D, Basquill C. Estimating the prevalence and awareness rates of hypertension in Africa: a systematic analysis. 2014;9(8):e104300.
Al Riyami AA, Afifi MM. Hypertension in Oman: distribution and correlates. 2002;77(3–4):383–407.
El-Aty MAA, et al. Hypertension in the adult Omani population: predictors for unawareness and uncontrolled hypertension. 2015;90(3):125–32.
Hasab A, Jaffer A, Hallaj Z. Blood pressure patterns among the Omani population. EMHJ-Eastern Mediterranean Health Journal. 1999;5(1):46–54.
Abdul-Rahim HF, et al. The metabolic syndrome in the West Bank population: an urban-rural comparison. Diabetes Care. 2001;24(2):275–9.
Khdour M, et al. Prevalence, awareness, treatment and control of hypertension in the Palestinian population. 2013;27(10):623.
Shahwan AJ, et al. Epidemiology of coronary artery disease and stroke and associated risk factors in Gaza community–Palestine. 2019;14(1):e0211131.
Bener A, et al. Epidemiology of hypertension and its associated risk factors in the Qatari population. 2004;18(7):529.
Maziak W, et al. Cardiovascular health among adults in Syria: a model from developing countries. 2007;17(9):713–20.
Romdhane HB, et al. Hypertension among Tunisian adults: results of the TAHINA project. Hypertens Res. 2012;35(3):341–7.
Allal-Elasmi M, et al. Prehypertension among adults in Great Tunis region (Tunisia): A population-based study. Pathol Biol (Paris). 2012;60(3):174–9.
Ben HR, et al. Hypertension prevalence, awareness, treatment and control: results from a community based survey. Tunis Med. 2005;83:41–6.
Ghannem H, Fredj AH. Epidemiology of hypertension and other cardiovascular disease risk factors in the urban population of Soussa, Tunisia. EMHJ-Eastern Mediterranean Health Journal. 1997;3(3):472–479.
Altun B, et al. Prevalence, awareness, treatment and control of hypertension in Turkey (the PatenT study) in 2003. 2005;23(10):1817–1823.
Arici M, et al. Hypertension incidence in Turkey (HinT): a population-based study. 2010;28(2):240–244.
Chow CK, et al. Prevalence, awareness, treatment, and control of hypertension in rural and urban communities in high-, middle-, and low-income countries. 2013;310(9):959–968.
Dastan I, et al. Awareness, treatment, control of hypertension, and associated factors: Results from a Turkish national study. 2018;40(1):90–98.
Erem C, et al. Prevalence of diabetes, obesity and hypertension in a Turkish population (Trabzon city). Diabetes Res Clin Pract. 2001;54(3):203–8.
Erem C, et al. Prevalence of prehypertension and hypertension and associated risk factors among Turkish adults: Trabzon Hypertension Study. 2008;31(1):47–58.
Gokcel A, et al. High prevalence of diabetes in Adana, a southern province of Turkey. Diabetes Care. 2003;26(11):3031–4.
Gündogan K, et al. Prevalence of metabolic syndrome in the Mediterranean region of Turkey: evaluation of hypertension, diabetes mellitus, obesity, and dyslipidemia. 2009;7(5):427–434.
Mahley RW, et al. Turkish Heart Study: lipids, lipoproteins, and apolipoproteins. J Lipid Res. 1995;36(4):839–59.
Metintas S, et al. Awareness of hypertension and other cardiovascular risk factors in rural and urban areas in Turkey. 2009;103(8):812–8.
Sariişik A, Oğuz A, Uzunlulu M. Control of hypertension in Turkey--is it improving? The Kocaeli 2 study. 2009;37:13–16.
Satman I, et al. Population-based study of diabetes and risk characteristics in Turkey: results of the Turkish Diabetes Epidemiology Study (TURDEP). Diabetes Care. 2002;25(9):1551–6.
Sengul S, et al. Controlling hypertension in Turkey: not a hopeless dream. 2013;3(4):326–31.
Sönmez H, et al. The epidemiology of elevated blood pressure as an estimate for hypertension in Aydın, Turkey. 1999;13(6):399.
Tezcan S, et al. Cardiovascular risk factor levels in a lower middle-class community in Ankara, Turkey. Trop Med Int Health. 2003;8(7):660–7.
Tugay Aytekin N, et al. Distribution of blood pressures in Gemlik District, north-west Turkey. Health Soc Care Community. 2002;10(5):394–401.
Baynouna LM, et al. High prevalence of the cardiovascular risk factors in Al-Ain, United Arab Emirates. 2008;29(8):1173–8.
Yusufali A, et al. May Measurement Month 2017: an analysis of blood pressure screening results from the United Arab Emirates—Northern Africa and Middle East. 2019;21(Supplement_D):D118-D120.
Gunaid A. Prevalence of known diabetes and hypertension in the Republic of Yemen. EMHJ-Eastern Mediterranean Health Journal. 2002;8(2–3):374–385.
Modesti PA, et al. Epidemiology of hypertension in Yemen: effects of urbanization and geographical area. 2013;36(8):711.
Liew SJ, et al. Sociodemographic factors in relation to hypertension prevalence, awareness, treatment and control in a multi-ethnic Asian population: a cross-sectional study. BMJ Open. 2019;9(5):e025869.
Lamelas P, et al. Prevalence, awareness, treatment and control of hypertension in rural and urban communities in Latin American countries. J Hypertens. 2019;37(9):1813–21.
Mills KT, et al. Global disparities of hypertension prevalence and control: a systematic analysis of population-based studies from 90 countries. 2016;134(6):441–450.
Guo X, et al. Prehypertension: a meta-analysis of the epidemiology, risk factors, and predictors of progression. 2011;38(6):643.
Leng B, et al. Socioeconomic status and hypertension: a meta-analysis. J Hypertens. 2015;33(2):221–9.
Colhoun HM, Hemingway H, Poulter NR. Socio-economic status and blood pressure: an overview analysis. J Hum Hypertens. 1998;12(2):91–110.
Afsargharehbagh R, et al. Hypertension and pre-hypertension among Iranian adults population: a meta-analysis of prevalence, awareness, treatment, and control. Curr Hypertens Rep. 2019;21(4).
Nicoll R, Henein MY. Hypertension and lifestyle modification: how useful are the guidelines? Br J Gen Pract. 2010;60(581):879–80.
Zhou B, et al. Long-term and recent trends in hypertension awareness, treatment, and control in 12 high-income countries: an analysis of 123 nationally representative surveys. The Lancet. 2019;394(10199):639–51.
Dzudie A, et al. Prevalence, awareness, treatment and control of hypertension in a self-selected sub-Saharan African urban population: a cross-sectional study. BMJ Open. 2012;2(4):e001217.
Gee ME, et al. Antihypertensive medication use, adherence, stops, and starts in canadians with hypertension. Can J Cardiol. 2012;28(3):383–9.
Okonofua EC, et al. Ethnic differences in older americans: awareness, knowledge, and beliefs about hypertension*. Am J Hypertens. 2005;18(7):972–9.
Pettey CM, et al. African Americans’ perceptions of adherence to medications and lifestyle changes prescribed to treat hypertension. Sage Open. 2016;6(1).
Huffman MD, Xavier D, Perel P. Uses of polypills for cardiovascular disease and evidence to date. The Lancet. 2017;389(10073):1055–65.
Liu X, et al. Hypertension prevalence, awareness, treatment, control, and associated factors in Southwest China: an update. J Hypertens. 2017;35(3):637–44.
Doulougou B, et al. Factors associated with hypertension prevalence, awareness, treatment and control among participants in the International Mobility in Aging Study (IMIAS). J Hum Hypertens. 2016;30(2):112–9.
Acknowledgements
We acknowledge Imam Ali and Rajaei Clinical Development Research Center, Alborz University of Medical Sciences for their administrative assistances.
Funding
This study was funded by Alborz University of Medical Sciences.
Author information
Authors and Affiliations
Contributions
MQ, NMK, and SD designed the study. NMK, SD, JH, and AMG searched data. NMK, ES, and BHZ screened and extracted data. ES, AS, NMK, and MQ analyzed data and prepared results. NMK, HSE, and MQ wrote the first draft of the paper. All other authors provided input into interpretation.
Corresponding author
Ethics declarations
Conflict of Interest
None; the authors declare that there is no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any data with human or animal subjects performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Prevention of Hypertension: Public Health Challenges
Appendix
Appendix
Rights and permissions
About this article

Cite this article
Mohammadian Khonsari, N., Shahrestanaki, E., Ejtahed, HS. et al. Long-term Trends in Hypertension Prevalence, Awareness, Treatment, and Control Rate in the Middle East and North Africa: a Systematic Review and Meta-analysis of 178 Population-Based Studies. Curr Hypertens Rep 23, 41 (2021). https://doi.org/10.1007/s11906-021-01159-0
Accepted:
Published:
DOI: https://doi.org/10.1007/s11906-021-01159-0