
Abstract
Purpose of Review
The association between mental health, pain, and treatment-resistant hypertension is an important consideration for treating physicians. We review and discuss the connection between conditions of anxiety, depression, and chronic pain and their effect on uncontrolled hypertension.
Recent Findings
There is significant co-occurrence of hypertension with anxiety, depression, and chronic pain which may lead to undertreatment of hypertension and undertreatment of the underlying mental health disorder. The association between mental health and hypertension is complex and is modulated by physiologic and environmental factors.
Summary
Physicians treating patients with hypertension should be cognizant of the role anxiety, depression, and chronic pain play in treatment efficacy and compliance. Patients undergoing treatment should be screened for mental health disorders at treatment initiation and frequently thereafter to ensure optimal overall health and compliance.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
There has been considerable interest in the link between hypertension, anxiety, and pain in the recent literature given the significant disease burden and associated cardiovascular mortality. Approximately 45% of the adult US population live with hypertension and about 76% of those patients continue to be sub-optimally treated despite lifestyle and medication modifications [1••]. In addition, psychological comorbidities have been linked to worse cardiovascular outcomes [2,3,4]. With an estimated prevalence of 19.1% of the adult US population [5], anxiety has the potential to significantly worsen hypertension and alter disease progression.
In addition to mental health, pain and perception of pain has similarly been associated with elevated blood pressure. We provide a review of the recent literature discussing hypertension and its connection to pain and anxiety and how it relates to diagnosis, treatment, prognosis, and overall quality of life.
Anxiety and Hypertension
Approximately 45% adults in the USA live with a diagnosis of hypertension [1••] and approximately 19% of the adult population suffers from disorders of anxiety [5]. Given the high prevalence of both diseases, it is important to understand the relationship between anxiety and hypertension. Data from the 2005 National Ambulatory Medical Care Survey and National Hospital Ambulatory Medical Care Survey showed that up to 32.5% of outpatients presenting for anxiety treatment had unrecognized elevated blood pressure measurements, compared to 24.6% of all ambulatory patient visits [6].
Relationship Between Anxiety and Hypertension
The link between hypertension, anxiety, and stress can be evident as soon as early adulthood. Sujatha et al. assessed the prevalence of prehypertension in association with stress and anxiety in college-age patients. In a cohort of 323 patients, prehypertension was highest among medical students (55.6%), more than their engineering and art major peers. Medical students also had the highest levels of anxiety (20.3%), while engineering students had a higher prevalence of stress (58.9%). Furthermore, prehypertension was 1.8 times more likely in students with anxiety and 1.4 times more likely with students with high stress [7]. In a different study assessing anxiety in older adults (mean age 69 years), hypertensive patients, especially those with a history of stroke and depression, were more likely to develop anxiety, suggesting that screening and early intervention for anxiety may be beneficial in older adults with hypertension [8].
Acute stress has also been linked to elevated blood pressure. Turkish researchers collected blood pressure values 1 day before an elective cholecystectomy from 90 participants [9]. Half of the participants were randomly selected to be shown the operating room the day before the procedure, while the rest were not. The researchers found that patients who were shown the operating room had lower blood pressure values compared to those who did not see the operating rooms until the day of surgery. The stress of the unknown played a role in increased blood pressure values prior to the procedure; previewing the operating room prior to surgery helped to alleviate stress which in turn helped to lower blood pressure measurements [9].
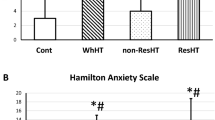
The prevalence of hypertension in the general population is a result of modifiable (environmental factors, diet, obesity, sodium intake, and physical activity) and non-modifiable risk factors (genetic predisposition) [10]. Whether anxiety predisposes an individual to develop hypertension remains controversial. Recent studies show a high incidence of anxiety in patients with treatment-resistant hypertension [11, 12•]. In addition, rates of anxiety are higher in hypertensive patients who have poor adherence to medical therapy [13]. Lambert et al. evaluated whether obesity and diabetes with concomitant anxiety made individuals more susceptible to the development of hypertension. They found that stress from chronic anxiety modulated a sympathetic firing pattern activating both sympathetic nervous system and hypothalamic-pituitary-adrenal axis in patients with metabolic syndrome resulting in elevated blood pressure [14]. However, this study was limited by small sample size, and long-term sequela was not explored. In contrast, the large-scale Norwegian HUNT study compared levels of anxiety among 55,472 patients with their corresponding blood pressures and found no association between anxiety and hypertension [15]. Given the findings of the HUNT study, the association between anxiety and hypertension is weak.
White Coat Hypertension and Over-/Undertreatment
White coat hypertension (WCH), which is a transient elevation in blood pressure measurements restricted to clinical settings, has a prevalence of 13–35% [16]. Between 1 and 5% of patients with WCH progress to clinical hypertension [10]. White coat hypertension may lead to overdiagnosis of hypertension and increased use of antihypertensive therapy despite the lack of association of WCH with cardiovascular disease and all-cause mortality [10, 17]. Patients that perceived themselves as hypertensive often reported a greater degree of anxiety in the outpatient setting and showed a larger degree of WCH [17]. Nevertheless, Murata et al. [18] found that WCH was not associated with anxiety after controlling for confounding variables and that WCH in healthy normotensive elderly patients could reflect a decrease in endothelial function rather than anxiety.
Despite the challenges WCH presents, the American College of Cardiology (ACC) and the American Heart Association (AHA) recommend utilizing ambulatory blood pressure monitoring (ABPM), supplemented with home blood pressure measurements (HBPM), to more accurately delineate hypertension from WCH, better predict cardiovascular disease risk, and guide therapy [10].
Effect of Anxiety on Circadian Rhythm and Hypertension
Anxiety has a significant effect on quality of life, both physiological through sympathetic arousal and circulating catecholamines and behavioral responses such as increased eating, alcohol consumption, or smoking. Anxiety may also play a role in developing circadian abnormalities [2]. Özpelit et al. [2] found that anxious patients were more likely to experience diurnal hypertension, with a lack of blood pressure dip during the night and elevated blood pressure readings in the morning. Furthermore, hypertensive patients with disrupted circadian rhythm were found to have increased circulating inflammatory markers and decreased vagal modulation of blood pressure upon awakening [19].
Depression and Hypertension
Several studies have shown an association between depression and hypertension. While the Norwegian HUNT study did not find an association between anxiety and hypertension, there was a positive relationship between depressive symptoms and multi-drug antihypertensive medication regimens. This study suggested that poor antihypertensive treatment adherence potentially leads to polypharmacy in patients with depression [15]. Studies from Nigeria, Ghana, and Pakistan have shown the prevalence of depression among hypertensive patients to be between 26 and 42% [20, 21]. In a large Finland study of 4450 patients, depression was found to be present in 14.1% of patients diagnosed with hypertension (as compared to 8.7% of patients without hypertension) [22]. Depressed patients had 1.4 times higher likelihood of having hypertension, and reported stress similarly increased the likelihood of hypertension by 1.4 times [21]. In a study assessing risk factors for developing depression in patients with hypertension, Rantanen et al. [22] identified female gender, excess alcohol use, elevated body mass index, smoking, and low physical activity as risk factors.
The link between depression and increased rates of hypertension has also been explored using physiological scales. Peng et al. [23] found a significant relationship between depression, arterial stiffness, and hypertension in a study conducted in China. Patients had brachial-ankle pulse wave velocities (baPWV) measured to determine arterial stiffness. Patients with depressive symptoms were found to have increased baPWV when controlling for confounding variables. They concluded that the degree of depressive symptoms was independently associated with arterial stiffness [23].
Antidepressant therapy is also independently associated with elevated blood pressures. The National Study of Adolescent to Adult Health (ADD Health) is a longitudinal study that followed 20,745 teenagers to adulthood. The study, which included 11,183 final participants, concluded that antidepressant use was associated with hypertension and that men on antidepressants had a greater likelihood of having elevated blood pressure versus men not taking antidepressants. There was no association among women taking antidepressants and having hypertension [24]. The study also found that use of antidepressants led to an average increase of 1.6 mmHg diastolic blood pressure levels without any increase in systolic blood pressure levels. This study questions whether depression itself leads to elevated blood pressures or treatment of depression causes elevation in blood pressure [24], a question that remains unanswered in the current literature.
Effect of Psychiatric Illness on Perceptions of Blood Pressure Control/Barriers to Treatment
Medication adherence to lower blood pressures to goal are important in preventing development of cardiovascular and end-organ complications which can become difficult with multiple comorbidities including psychiatric illness. The Framingham Heart Study examined risk factors for medication adherence and suggested that depressive symptoms may act as a barrier to medication adherence, which exacerbates cardiovascular disease risk factors, including hypertension, in older adults [25•]. Additionally, in a retrospective cohort analysis of 431,591 patients, factors that included chronic mental illness and adherence to psychiatric medications predicted adherence to antihypertensive therapy [26].
Additionally, patients with chronic medical conditions such as hypertension can develop negative emotions leading to anxiety, stress, and depression and these patients exhibit a higher likelihood of medication non-compliance [27].
Pain and Hypertension
In addition to psychiatric illness, hypertension has been shown to be more prevalent in individuals with persistent pain as compared to those in the general community [28]. Giummarra et al. [28] performed a registry-based study of 40,000 individuals reporting persistent non-cancer pain registered to the electronic Persistent Pain Outcomes Collaboration (ePPOC) registry in Australia. Compared with the general and primary care Australian population, hypertension was found to be more prevalent in patients in the ePPOC cohort. When adjusted for age, hypertension prevalence was 1.7 times more prevalent in the ePPOC pain cohort [28]. Sub-analysis of the ePPOC cohort did not find correlation between hypertension and quality of life components of chronic pain severity such as widespread pain, interference with daily living, or frequency of pain catastrophizing [28].
Elevated blood pressure in the presence of acute or chronic pain has been evaluated. Frequently, elevated blood pressures in the Emergency Department (ED) are disregarded in the setting of acute pain [29••]. Poon et al. [29••] evaluated the relationship between ED blood pressure and follow up blood pressure readings for 1 year after ED visit. After analyzing data from 8150 patients, they found no evidence that high blood pressure in the ED is attributable to pain. They also found that patients with elevated BP in the ED, regardless of chief complaint, including pain-related complaints, were associated with elevated blood pressures after the ED visit [29••]. This highlights the need for follow-up and close blood pressure monitoring and treatment after ED visits in patients with elevated ED blood pressures.
Several studies have evaluated the physiological link between pain and hypertension [30,31,32,33,34]. These effects can be distinguished between individuals suffering acute or chronic pain. In the acute pain response, a nociceptive stimulus activates the sympathetic nervous system and the hypothalamic-pituitary-adrenal axis which compounds the sympathetic response leading to adrenergic and cardiovascular responses directly elevating blood pressure [35•].
Altered Pain Perception in the Hypertensive Patient
Elevated blood pressure has been associated with down-regulation of the pain response, termed the hypertension-hypoalgesia response [36]. There are two proposed mechanisms for the hypertension-hypoalgesia response. The first is baroreceptor-mediated reduction of cerebral arousal, with the nucleus of the solitary tract proposed as a link between the vagus nerve and spinal dorsal column [36]. This was described in an animal model where rats showed decreased running to avoid noxious stimuli with phenylephrine infusions rather than with saline, and this effect was abolished with denervated baroreceptors [37]. In an alternative mechanism, opioid systems are theorized to contribute to the hypertension-hypoalgesia phenomenon. Reduced pain sensitivity in hypertensive rats was found to be pharmacologically reversible with opioid receptor inhibitors [38]. Human studies have attempted to demonstrate opioid system mechanisms without success [31, 32, 39].
Further work done by Guasti et al. has confirmed changes in pain perception in patients with hypertension. Researchers randomized known hypertensive patients to angiotensin converting enzyme inhibitor therapy and compared hypoalgesic effects in pain perception [40]. Untreated hypertensives showed reduced perception to painful stimuli compared with normotensives [40]. This effect was found both with the ACE inhibitor and enalapril, and with the angiotensin receptor blocker, losartan.
Chronic Pain and the Hypertension-Hypoalgesia Response
The hypertension-hypoalgesia response is dysregulated in patients suffering from chronic pain. Chronic pain patients are known to exhibit wind-up, or frequency-dependent increase in afferent nociceptive fiber stimulation of spinal cord neurons [41]. Chung et al. tested resting blood pressure and baroreflex activity effect on wind-up in health controls as compared to chronic pain patients. Their findings confirmed higher resting systolic blood pressure and baroreceptor sensitivity to be associated with lower wind-up, and found this pathway was altered in individuals with chronic pain [41]. Similar findings were noted in the Tromso study [42]. This confirmed the link between chronic pain and impaired cardiovascular regulation, with chronic pain groups displaying lower heart rate variation and lower baroreflex sensitivity than pain free controls [42]. Disrupted autonomic balance and decreased parasympathetic tone is proposed by Tracy et al. [43] in meta-analytic work for decreased heart rate variability in chronic pain patients. This meta-analysis reviewed 26 studies on the subject of heart rate variation and confirmed a moderate to large decrease in heart rate variability [43]. Further work could be done to directly connect these findings to the abolition of the hypertension-hypoalgesia response seen in individuals with chronic pain.
The differences among patients experiencing acute versus chronic pain may be due to diminished endogenous opioid levels found in chronic pain patients [44]. Subsequent work by Bruehl et al. [32] suggested an inverse relationship between blood pressure and pain sensitivity in pain free subjects, and found that this was not affected by opioid blockade administration. When low back pain subjects were included in the analyses, the relationships between blood pressure and pain ratings became positive rather than negative, consistent with suspected dysregulation of cardiovascular and pain regulatory systems in chronic pain [32]. Further work by Ring et al. [31] used a double-blind placebo-controlled study to compare naltrexone versus placebo on electrocutaneous pain. Hypertensive patients experienced less pain than normotensive patients, but this effect was not moderated by naltrexone [31]. Parallel work compared effects of naltrexone and placebo on cold and ischemic pain in patients newly diagnosed with essential hypertension performing cold pressor and forearm ischemia tasks. This again showed no moderation of pain and pressor responses with opioid receptor blockade [45].
Non-Pharmacologic Treatment Strategies for Patients with Uncontrolled Hypertension
Mental health disorders and chronic pain can lead to uncontrolled hypertension either due to medication non-compliance, underdiagnosis, or lack of addressing hypertension in psychiatric health visits. In addition to standard pharmacologic therapy, patients with chronic mental health disorders or chronic pain may benefit from non-traditional treatment strategies as adjuncts to control blood pressure.
Regular exercise has shown to help pain scores which may also be beneficial to improve blood pressure. In a small case-control study evaluating 53 patients, Kruk and Nowicki tested how regular exercise affects pain scores, anxiety, and depression in patients with treatment-resistant hypertension [46••]. Patients who underwent regular exercise saw a statistically significant reduction in patient pain scores, depression scores, and anxiety scores. While not powered or the primary aim of the study, they also noted a correlation between reduction in pain score and reduction in nocturnal systolic blood pressure, heart rate, and anxiety levels [46••].
Wang et al. [47] evaluated the effect of mind sound resonance technique (MSRT), a yoga-based relaxation technique, on blood pressure, heart rate, and anxiety in individuals with hypertension. Thirty patients attended two 30-min yoga sessions on consecutive days, one for MSRT and one for supine relaxation. Systolic and diastolic blood pressure measurements, heart rate, and anxiety scores were measured before and after the two sessions. Both groups saw a reduction in heart rate and anxiety immediately afterwards, but patients practicing MSRT experienced reduction in systolic and diastolic blood pressures. Although limited, the study suggests that regular yoga activity may be one modality to help reduce both blood pressure and anxiety [47]. Further studies and meta-analysis have also demonstrated blood pressure improvement with yoga, although its effects are modest [48].
Deep breathing and relaxation techniques have also shown promise at reducing blood pressure. Jefferson studied the effects of combined diaphragmatic breathing with therapeutic massage on blood pressure, stress, and anxiety in hypertensive African American females [49]. After 1 week, there was statistically significant reduction in anxiety/pain surveys as well as reduction in systolic and diastolic blood pressure measurements [49].
Acupuncture therapy for hypertension has also been evaluated. The study by Li et al. revealed that patients undergoing auricular point therapy and relaxation techniques had a reduction in blood pressure and anxiety scores after 2 weeks of intervention [50]. However, these effects do not appear to be sustained. A Cochrane review evaluating the effects of acupuncture on blood pressure measurements showed no evidence for sustained blood pressure lowering effect after evaluating data from 22 randomized control trials [51].
Conclusions
The connection between hypertension, mental health, and chronic pain is complex and when present lead to treatment-resistant hypertension, medication non-compliance, and worse outcomes. Clinicians should be cognizant of the relationship between mental health, pain, and hypertension when initiating treatment (Fig. 1). A thorough history with particular attention to anxiety, depressive symptoms, comorbid conditions, and pain should be elucidated both at diagnosis and treatment initiation, and during follow-up visits for hypertension management in the primary care setting. In addition to gold-standard pharmacological therapy, non-traditional therapies at reducing stress, anxiety, and depression should be considered for treatment-resistant hypertension. Compliance and barriers to medication compliance should also be addressed.

Outline for the evaluation, follow-up, and treatment of elevated blood pressure in patients with underlying pain or psychiatric illness
Addressing anxiety during these visits may also lead to improved quality of life for patients [52]. Overall, studies assessing the relationship between anxiety, depression, and hypertension stress the importance of addressing anxiety and other mental disorders in hypertension patients in an attempt to guide medical therapy, enhance medication compliance, and better control blood pressure [13].
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
•• Centers for Disease Control and Prevention (CDC). Hypertension cascade: hypertension prevalence, treatment and control estimates among US adults aged 18 years and older applying the criteria from the American College of Cardiology and American Heart Association’s 2017 Hypertension Guideline—NHANES 2013–2016. Atlanta, GA: US Department of Health and Human Services; 2019 [cited 2020 May 8]. Available from: https://millionhearts.hhs.gov/data-reports/hypertension-prevalence.html. Accessed 7 Nov 2020. This report shows a break down in treatment modalities for American patients with hypertension and the large proportion of those patients who continue to have uncontrolled hypertension according the American College of Cardiology and American Heart Association’s (ACC/AHA) 2017 hypertension clinical practice guidelines.
Özpelit ME, Özpelit E, Doğan NB, Pekel N, Ozyurtlu F, Yılmaz A, et al. Impact of anxiety level on circadian rhythm of blood pressure in hypertensive patients. Int J Clin Exp Med. 2015;8(9):16252–8.
Roest AM, Martens EJ, de Jonge P, Denollet J. Anxiety and risk of incident coronary heart disease: a meta-analysis. J Am Coll Cardiol. 2010;56(1):38–46.
Nicholson A, Kuper H, Hemingway H. Depression as an aetiologic and prognostic factor in coronary heart disease: a meta-analysis of 6362 events among 146 538 participants in 54 observational studies. Eur Heart J. 2006;27(23):2763–74.
Kessler RC, Chiu WT, Demler O, Merikangas KR, Walters EE. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):617–27.
Player MS, Mainous AG, Carnemolla M. Anxiety and unrecognized high blood pressure in U.S. ambulatory care settings: an analysis of the 2005 National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey. Int J Psychiatry Med. 2008;38(1):91–101.
Abeetha S, Sureka V, Brinda S, Ganesh M, Olickel J, Sujatha S. Prevalence of prehypertension and its association with levels of stress and anxiety among students of various disciplines in Chennai - a cross-sectional study. Natl J Physiol Pharm Pharmacol. 2018;8(9):1.
Ismail Z, Mohamad M, Isa MR, Fadzil MA, Yassin SM, Ma KT, et al. Factors associated with anxiety among elderly hypertensive in primary care setting. J Ment Health. 2015;24(1):29–32.
Yuzkat N, Soyalp C, Turk O, Keskin S, Gulhas N. Effects of showing the operating room on preoperative anxiety and hemodynamics among patients with hypertension: A randomized controlled trial. Clin Exp Hypertens. 2020;42(6):553–8.
Whelton PK, Carey RM, Aronow WS, Casey DE, Collins KJ, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and Management of high blood pressure in adults. J Am Coll Cardiol. 2018;71(19):e127–248.
Hamrah MS, Hamrah MH, Ishii H, Suzuki S, Hamrah MH, Hamrah AE, et al. Anxiety and depression among hypertensive outpatients in Afghanistan: a cross-sectional study in Andkhoy City. Int J Hypertens. 2018;2018:1–8.
• Schmieder RE, Grassi G, Kjeldsen SE. Patients with treatment-resistant hypertension report increased stress and anxiety: a worldwide study. J Hypertens. 2013;31(3):610–5; discussion 615. This study highlights the emotional impact that uncontrolled and treatment-resistant hypertension have on patients overall mental well-being.
Emre N, Topal K, Edirne T, Gereklioğlu Ç. Factors affecting risk of anxiety and depression among diabetic and hypertensive patients who refer to family health centers. Int J Diabetes Dev Ctries. 2018;38(3):305–11.
Lambert E, Dawood T, Straznicky N, Sari C, Schlaich M, Esler M, et al. Association between the sympathetic firing pattern and anxiety level in patients with the metabolic syndrome and elevated blood pressure. J Hypertens. 2010;28(3):543–50.
Johansen A, Holmen J, Stewart R, Bjerkeset O. Anxiety and depression symptoms in arterial hypertension: the influence of antihypertensive treatment. The HUNT study, Norway. Eur J Epidemiol. 2012;27(1):63–72.
Pickering TG. How common is white coat hypertension? JAMA. 1988;259(2):225–8.
Spruill TM, Pickering TG, Schwartz JE, Mostofsky E, Ogedegbe G, Clemow L, et al. The impact of perceived hypertension status on anxiety and the white coat effect. Ann Behav Med. 2007;34(1):1–9.
Murata T, Narita K, Hamada T, Takahashi T, Omori M, Yoshida H, et al. White coat phenomenon, anxiety and endothelial function in healthy normotensive elderly subjects. Blood Press. 2006;15(2):88–92.
Fang C, Lei J, Zhou S, Zhang Y, Yuan G, Wang J. Association of higher resistin levels with inflammatory activation and endothelial dysfunction in patients with essential hypertension. Chin Med J. 2013;126(4):646–9.
Ademola A, Boima V, Odusola A, Agyekum F, Nwafor C, Salako B. Prevalence and determinants of depression among patients with hypertension: a cross-sectional comparison study in Ghana and Nigeria. Niger J Clin Pract. 2019;22(4):558.
Mushtaq M, Najam N. Depression, anxiety, stress and demographic determinants of hypertension disease. Pak J Med Sci. 2014;30(6):1293–8.
Rantanen AT, Korkeila JJA, Löyttyniemi ES, Saxén UKM, Korhonen PE. Awareness of hypertension and depressive symptoms: a cross-sectional study in a primary care population. Scand J Prim Health Care. 2018;36(3):323–8.
Peng L, Bi S, Liu X, Long T, Zhao Y, Li F, et al. Association between depressive symptoms and arterial stiffness: a cross-sectional study in the general Chinese population. BMJ Open. 2020;10(2):e033408.
Crookes DM, Demmer RT, Keyes KM, Koenen KC, Suglia SF. Depressive symptoms, antidepressant use, and hypertension in young adulthood. Epidemiology. 2018;29(4):547–55.
• Hennein R, Hwang S-J, Au R, Levy D, Muntner P, Fox CS, et al. Barriers to medication adherence and links to cardiovascular disease risk factor control: the Framingham Heart Study. Intern Med J. 2018;48(4):414–21 This study used data from the Framingham Heart Study to show that depressive symptoms may act as a barrier to medication compliance.
MacEwan JP, Silverstein AR, Shafrin J, Lakdawalla DN, Hatch A, Forma FM. Medication adherence patterns among patients with multiple serious mental and physical illnesses. Adv Ther. 2018;35(5):671–85.
Kretchy IA, Owusu-Daaku FT, Danquah SA. Mental health in hypertension: assessing symptoms of anxiety, depression and stress on anti-hypertensive medication adherence. Int J Ment Heal Syst. 2014;8:25.
Giummarra MJ, Tardif H, Blanchard M, Tonkin A, Arnold CA. Hypertension prevalence in patients attending tertiary pain management services, a registry-based Australian cohort study. PLoS One. 2020;15(1):e0228173.
•• Poon SJ, Roumie CL, O'Shea CJ, Fabbri D, R Coco J, Collins SP, et al. Association of elevated blood pressure in the emergency department with chronically elevated blood pressure. J Am Heart Assoc. 2020;9(12):e015985. This study shows that patients with no history of hypertension who present to the ED and are found to have elevated blood pressure, regardless of chief complaint, are likely to have elevated blood pressure in the year following their ED visit.
Bruehl S, Burns JW, Chung OY, Magid E, Chont M, Gilliam W, et al. Hypoalgesia associated with elevated resting blood pressure: evidence for endogenous opioid involvement. J Behav Med. 2010;33(2):168–76.
Ring C, France CR, al’Absi M, Edwards L, McIntyre D, Carroll D, et al. Effects of naltrexone on electrocutaneous pain in patients with hypertension compared to normotensive individuals. Biol Psychol. 2008;77(2):191–6.
Bruehl S, Chung OY, Ward P, Johnson B, McCubbin JA. The relationship between resting blood pressure and acute pain sensitivity in healthy normotensives and chronic back pain sufferers: the effects of opioid blockade. Pain. 2002;100(1–2):191–201.
Ghione S. Hypertension-associated hypalgesia: evidence in experimental animals and humans, pathophysiological mechanisms, and potential clinical consequences. Hypertension. 1996;28(3):494–504.
Sitsen JMA, de Jong W. Observations on pain perception and hypertension in spontaneously hypertensive rats. Clin Exp Hypertens A. 1984;6(7):1345–56.
• Saccò M, Meschi M, Regolisti G, Detrenis S, Bianchi L, Bertorelli M, et al. The relationship between blood pressure and pain. J Clin Hypertens (Greenwich). 2013;15(8):600–5 This review discusses the pathophysiological mechanisms underlying pain and chronic hypertension.
Randich A, Maixner W. Interactions between cardiovascular and pain regulatory systems. Neurosci Biobehav Rev. 1984;8(3):343–67.
Bruehl S, Chung OY, Jirjis JN, Biridepalli S. Prevalence of clinical hypertension in patients with chronic pain compared to nonpain general medical patients. Clin J Pain. 2005;21(2):147–53.
Saavedra JM. Naloxone reversible decrease in pain sensitivity in young and adult spontaneously hypertensive rats. Brain Res. 1981;209(1):245–9.
Schobel HP, Handwerker HO, Schmieder RE, Heusser K, Dominiak P, Luft FC. Effects of naloxone on hemodynamic and sympathetic nerve responses to pain in normotensive vs. borderline hypertensive men. J Auton Nerv Syst. 1998;69(1):49–55.
Guasti L, Zanotta D, Diolisi A, Garganico D, Simoni C, Gaudio G, et al. Changes in pain perception during treatment with angiotensin converting enzyme-inhibitors and angiotensin II type 1 receptor blockade. J Hypertens. 2002;20(3):485–91.
Chung OY, Bruehl S, Diedrich L, Diedrich A. The impact of blood pressure and baroreflex sensitivity on wind-up. Anesth Analg. 2008;107(3):1018–25.
Bruehl S, Olsen RB, Tronstad C, Sevre K, Burns JW, Schirmer H, et al. Chronic pain-related changes in cardiovascular regulation and impact on comorbid hypertension in a general population: the Tromsø study. Pain. 2018;159(1):119–27.
Tracy LM, Ioannou L, Baker KS, Gibson SJ, Georgiou-Karistianis N, Giummarra MJ. Meta-analytic evidence for decreased heart rate variability in chronic pain implicating parasympathetic nervous system dysregulation. Pain. 2016;157(1):7–29.
Bruehl S, McCubbin JA, Harden RN. Theoretical review: altered pain regulatory systems in chronic pain. Neurosci Biobehav Rev. 1999;23(6):877–90.
Ring C, France CR, al’Absi M, Beesley L, Edwards L, McIntyre D, et al. Effects of opioid blockade with naltrexone and distraction on cold and ischemic pain in hypertension. J Behav Med. 2007;30(1):59–68.
•• Kruk PJ, Nowicki M. Effect of the physical activity program on the treatment of resistant hypertension in primary care. Prim Health Care Res Dev. 2018;19(6):575–83. This study shows that regular exercise improves pain and anxiety and reduces blood pressure in patients with treatment-resistant hypertension, which can be a beneficial adjunct in the treatment plan of these patients.
Wang Y, Metri KG, Singh A, Raghuram N. Immediate effect of mind sound resonance technique (MSRT - a yoga-based relaxation technique) on blood pressure, heart rate, and state anxiety in individuals with hypertension: a pilot study. J Complement Integr Med. 2018;17(2).
Hagins M, States R, Selfe T, Innes K. Effectiveness of yoga for hypertension: systematic review and meta-analysis. Evid Based Complement Alternat Med. 2013;2013:1–13.
Jefferson LL. Exploring effects of therapeutic massage and patient teaching in the practice of diaphragmatic breathing on blood pressure, stress, and anxiety in hypertensive African-American women: an intervention study. J Natl Black Nurses Assoc. 2010;21(1):17–24.
Li L, Zhang K, Shi N. Effects of the traditional Chinese auricular point therapy combined with relaxation training on patients with hypertension and anxiety. Biomed Res India. 2017;28(12):5224–8.
Yang J, Chen J, Yang M, Yu S, Ying L, Liu GJ, et al. Acupuncture for hypertension. Cochrane Database Syst Rev. 2018;11(11):CD008821.
Serafini G, Pompili M, Innamorati M, Iacorossi G, Cuomo I, Della Vista M, et al. The impact of anxiety, depression, and suicidality on quality of life and functional status of patients with congestive heart failure and hypertension: an observational cross-sectional study. Prim Care Companion J Clin Psychiatry. 2010;12(6).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no conflicts of interest relevant to this manuscript.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of Topical Collection on Hypertension and Emergency Medicine
Rights and permissions
About this article

Cite this article
Hamam, M.S., Kunjummen, E., Hussain, M.S. et al. Anxiety, Depression, and Pain: Considerations in the Treatment of Patients with Uncontrolled Hypertension. Curr Hypertens Rep 22, 106 (2020). https://doi.org/10.1007/s11906-020-01117-2
Accepted:
Published:
DOI: https://doi.org/10.1007/s11906-020-01117-2