
Abstract
Purpose of Review
Idiopathic non-cirrhotic portal hypertension is described with a very heterogeneous terminology depending on the geographic origin of the patients and on the possible underlying causes of the disease. We aim here to review the current nomenclature and to the pathophysiological origins of this entity.
Recent Findings
In the past, a relevant number of definitions of this condition have been used in the literature, suggesting the presence of several distinct diseases. However, recent findings strongly suggest that there are some common denominators for this disease. Therefore, efforts should be made to develop a unified terminology encompassing the very essential features from clinical, histologic, imaging, laboratory and elastographic data.
Summary
These findings suggest that the common localization of the disease is the portal and the sinusoidal compartment of the liver; therefore, a novel definition should be elaborated.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
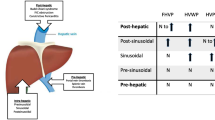
Portal hypertension results from increased resistance to portal venous blood flow and from splanchnic vasodilation, potentially leading to complications including variceal bleeding, splenomegaly and ascites [1]. Idiopathic non-cirrhotic portal hypertension includes a number of conditions or diseases that are characterized by an increased portal pressure due to intrahepatic lesions or changes in the absence of cirrhosis [2]. Histological lesions observed in this disease involve the small branches of the portal vein and the hepatic sinusoids, resulting in a presinusoidal portal hypertension. This explains why, in these patients, hepatic venous pressure gradient values can be much lower than the cut-off for clinical significant portal hypertension in cirrhosis, despite unequivocal signs of portal hypertension [3].
The ‘cartography’ of the portal system, and therefore also the history of portal hypertension, began with the first description of the splenic and mesenteric axis by Vesalius in 1543 [4]. Raciborski in 1841 was the first to show that, because of increased portal pressure, collaterals form between the portal and systemic circulations through the abdominal wall, short gastric and haemorrhoidal veins [5], before Sappey in 1859 described for the first time the development of oesophageal varices [6]. However, the term ‘portal hypertension’ was first used by Gilbert and Villaret in 1906 [7]. Knowledge about variceal development improved gradually up to 1928, when the occurrence of oesophageal varices on thin barium X-ray films as small dilated luminal structures was first described [8].
Origins of the Nomenclature
The terminology related to a disease characterized by hypersplenism and splenomegaly, in the absence of any known haematological disease, was used for the first time at the end of the nineteenth century by the Italian pathologist Guido Banti [9], who reported the existence of a disorder including splenomegaly and anaemia in the early stages, eventually progressing to gastrointestinal bleeding, hepatic failure and death. However, his cohort of patients was heterogeneous and, in addition to patients with idiopathic portal hypertension, it also included patients with cirrhosis and spleen enlargement due to malaria. McMichael attributed in 1936 the pathologic findings corresponding to endophlebitis of the portal vein to the presence of portal hypertension in patients presenting with a disease called ‘hepatolienal fibrosis’, characterized by the presence of splenomegaly without cirrhosis [10].
Additional hypotheses on the possible pathophysiological mechanisms causing obstruction of venous blood flow, and therefore portal hypertension, were formulated some years later by Thomson and colleagues not only in patients with cirrhosis, but also in patients with a normal liver function, when thrombosis of the portal vein or schistosomiasis were present [11].
In 1945, Whipple reported that 26 out of a series of 93 patients with splenomegaly had no cirrhosis, no schistosomiasis and no portal vein thrombosis. A syndrome different from both cirrhosis and extrahepatic obstruction of the portal vein was more clearly reported in 1962 in patients from northern India presenting with portal hypertension and it was called ‘non-cirrhotic portal fibrosis’ [12, 13]. Successively, cases of unexplained portal hypertension were reported, in which liver function and microscopic liver architecture were considered normal, whereby the portal vein was patent. With a more accurate analysis of these cases, a few years later Mikkelsen described a concentric thickening of the portal vein and its ramifications and coined the term ‘hepato-portal sclerosis’ [14]. Most patients had abnormal liver blood tests, presented hepatic encephalopathy and some of them died of liver failure. The term hepato-portal sclerosis was chosen to describe this disease based on the presence of an obliterative process of the portal vein branches. In 1967, Boyer adopted the term ‘idiopathic portal hypertension’ to describe the cases of non-cirrhotic portal fibrosis initially described in India [15]. In this paper, the authors used the term ‘idiopathic portal hypertension’ in the title and ‘non-cirrhotic portal fibrosis’ in the text to describe the presence of portal hypertension in the absence of cirrhosis and of thrombotic obstruction of the portal vein. It became also evident that the outcome of patients presenting with this disease was better than that of patients with cirrhosis.
Other histological liver lesions have been described in patients with idiopathic non-cirrhotic portal hypertension [16]. The term ‘obliterative portal venopathy’ was suggested by Nayak and Ramalingaswami in 1969 to describe an entity characterized by segmental, sub endothelial thickening of large and medium-sized intrahepatic portal vein branches with scarring and obliteration of the small portal vein branches along with an increase in small vascular channels in the portal tracts and incomplete thin fibrous septa [17]. While obliterative portal venopathy refers to luminal narrowing or obliteration of small portal venous ramifications, associated with deposits of elastic fibres [18], ‘nodular regenerative hyperplasia’ refers to diffuse micronodular transformation of the hepatic parenchyma without fibrotic septa between the nodules [19]. Additional names attributed to this disorder included benign intrahepatic portal hypertension [20] and idiopathic presinusoidal portal hypertension [21].
All these terms have progressively been considered somehow clinically equivalent [22], as they all belong to a heterogeneous group of liver abnormalities characterized by portal hypertension in association with specific changes in the liver architecture and microcirculation, in the absence of cirrhosis [23, 24]. This proliferation of terms and definitions has conducted to a lack of clarity and misunderstandings. Efforts of clarification have however been made. In Japan, the name ‘idiopathic portal hypertension’ was adopted in a report of the Ministry of health in 1976 [25]. In the Western world, in 2011 a group of European experts in portal hypertension proposed the term ‘idiopathic non-cirrhotic portal hypertension’ to be used in forthcoming cooperative multi-centric studies [2]. The Asian Pacific Association for the Study of the Liver defined this entity as a disease of uncertain aetiology characterized by periportal fibrosis and involvement of small and medium branches of the portal vein, resulting in the development of portal hypertension [26]. More recently, a working group from the European Association for the Study of the Liver has elaborated several criteria, summarized in Table 1, that more precisely contribute to the definition of idiopathic non-cirrhotic portal hypertension [27].
Evolution and Open Issues
The term ‘idiopathic non-cirrhotic portal hypertension’ has however some limitations: (a) it is an exclusion diagnosis; (b) some patients have histological lesions of nodular regenerative hyperplasia and/or obliterative portal venopathy but no portal hypertension [18, 28, 29]; (c) this liver disease is frequently associated with predisposing factors including drugs, immunological disorders, infections, prothrombotic conditions, so that the term ‘idiopathic’ might not be appropriate.
These limitations together with the plethora of terms indicating similar conditions leading to the development of portal hypertension in the absence of cirrhosis raise the need for the elaboration of a clear descriptive unifying definition based on positive elements, though excluding cirrhosis. Such a definition would allow a better understanding of this condition but also favour the design of future international studies with a common denominator.
Pathological Features
A common denominator of all described entities is the absence of cirrhosis together with the presence of one or several lesions involving portal veinules and/or sinusoids. Some lesions on liver biopsy can be considered specific of these entities including obliterative portal venopathy (including thickening of the vessel wall, occlusion of the lumen or vanishing of the portal veins), nodular regenerative hyperplasia or incomplete septal fibrosis. Other lesions can be observed on liver biopsy, but seem less specific, including portal tract abnormalities with multiplication, dilatation of arteries, periportal vascular channels, aberrant vessels, architectural disturbance with irregular distribution of the portal tracts and central veins, non-zonal sinusoidal dilatation and mild peri-sinusoidal fibrosis. There is currently no consensus on the pathologic features that should be included in the definition of a novel entity encompassing all the characteristics described in the previous lines and paragraphs. Moreover, there is a need for a consensus on the precise definition of each lesion.
Clinical, Imaging and Laboratory Features
Although not mandatory, portal hypertension is a key feature of the entities described above. Manifestations can be gastric, esophageal or ectopic varices, and/or portal hypertensive bleeding, but also portosystemic collaterals demonstrated by ultrasound, CT-scan or magnetic resonance imaging, ascites, splenomegaly, with a diameter of 13 cm or more or thrombocytopenia. It should be kept in mind that ascites, splenomegaly and thrombocytopenia are not specific of portal hypertension, in particular in patients with blood or systemic disorder.
Other signs suggesting idiopathic non-cirrhotic portal hypertension or associated entities include a smooth liver surface (the presence of nodules does not exclude this disease) in a patient with portal hypertension, thickening or obstruction of intrahepatic portal branches, mural calcifications of the portal veins, hepatic vein to vein communications at liver catheterisation or an increased visualisation of intrahepatic arteries close to the liver capsule. Finally, liver elastography showing normal or slightly elevated stiffness values in a patient with portal hypertension is also suggestive.
Possible Novel Diagnostic Criteria
When considering the possibility of a modern disease definition of idiopathic non-cirrhotic portal hypertension and associated entities, taking into account histological imaging and clinical criteria listed above, the question of the possible coexistence of other causes of liver disease or portal hypertension should be addressed. This includes portal vein thrombosis without cavernoma, a history of organ transplantation (including the liver) chronic hepatitis B or C virus infection or non-alcoholic fatty liver disease.
Whether specific diseases causing liver vessels abnormalities should or not be excluded from this definition has to be determined. This concerns particularly portal cavernoma, schistosomiasis, Abernethy malformation, chronic cholestatic diseases and liver neoplastic infiltration. Most likely, lesions to centrilobular veins (sinusoidal obstruction syndrome and venooclusive disease) will have to be excluded since these lesions are associated with a different presentation and outcome. A manner can be to exclude conditions like bone marrow transplantation, hepatic outflow obstruction, cardiac failure or Fontan surgery.
Liver biopsy remains a fundamental diagnostic tool for the diagnosis of the disease, although new non-invasive tools such as elastography may be considered in the near future.
Conclusions
The terminology used so far to describe idiopathic non-cirrhotic portal hypertension has been very heterogeneous depending on the geographic origin of the patients and on the possible underlying causes of the disease. In the past, a relevant number of definitions of this condition have been used in the literature, suggesting the presence of several distinct diseases. However, recent findings strongly suggest that there are some common denominators for this disease. Therefore, efforts should be made to develop a unified terminology encompassing the very essential features from clinical, histologic, imaging, laboratory and elastographic data. These findings suggest that the common localization of the disease is the portal and the sinusoidal compartment of the liver. The acknowledgment of these observations should be the driver for the elaboration of a novel, simplified and pathophysiologically oriented definition of this disease.
References
Bosch J, Mastai R, Kravetz D, Navasa M, Rodés J. Hemodynamic evaluation of the patient with portal hypertension. Semin Liver Dis. 1986;6(4):309–17.
Schouten JNL, Garcia-Pagan JC, Valla DC, Janssen HLA. Idiopathic noncirrhotic portal hypertension. Hepatol Baltim Md. 2011;54(3):1071–81.
Seijo S, Reverter E, Miquel R, Berzigotti A, Abraldes JG, Bosch J, u. a. Role of hepatic vein catheterisation and transient elastography in the diagnosis of idiopathic portal hypertension. Dig Liver Dis Off J Ital Soc Gastroenterol Ital Assoc Study Liver 2012;44(10):855–860.
Vesalius. De Humani Corporis fabrica Basileae. 1543;
Raciborski. Histoire de decouvertes relatives au système veineux, envisage dans le rapport anatomique, physiologique, pathologique et therapeutique depuis Morgagni jusqu’à nos jours. Mem Acad R Med. 1841;
Sappey P. Memoire sur un point d’anatomie pathologique relatif à l’ histoire de la cirrhose. Mem Acad Imp Med. 1859;
Gilbert A, Villaret M. Contribution à l’etude du syndrome d’hypertension portale; cytologie des liquides d’ascite dans les cirrhoses. 1906;(60):820–823.
Wolf G. Die Erkennung von Ösophagus-Varizen im Röntgenbilde. Fortschr Röntgenst. 1928;37:890–3.
Banti, Guido. Splenomegalie mit Leberzirrhose. Beitr Path Anat. 1898;(24).
McMichael J. The pathology of hepatolienal fibbosis. J Pathol Bacteriol. 1934;39:481–502.
Thompson WP, Caughey JL, Whipple AO, Rousselot LM. Splenic vein pressure in congestive splenomegaly (Banti’s syndrome). J Clin Invest. 1937;16(4):571–2.
Basu AK, Boyer J, Bhattacharya R, Mallik KC, Sen Gupta KP. Non-cirrhotic portal fibrosis with portal hypertension: a new syndrome. I. Clinical and function studies and results of operations. Indian J Med Res. 1967;55(4):336–50.
Mallik KC, Sen Gupta KP, Basu AK, Biswas SK, Pal NC, Boyer J. Non-cirrhotic portal fibrosis with portal hypertension: a new syndrome. II. Histopathological studies. Indian J Med Res. 1967;55(4):351–9.
Mikkelsen WP, Edmondson HA, Peters RL, Redeker AG, Reynolds TB. Extra- and intrahepatic portal hypertension without cirrhosis (hepatoportal sclerosis). Ann Surg. 1965;162(4):602–20.
Boyer JL, Sen Gupta KP, Biswas SK, Pal NC, Basu Mallick KC, Iber FL, u. a. Idiopathic portal hypertension. Comparison with the portal hypertension of cirrhosis and extrahepatic portal vein obstruction. Ann Intern Med 1967;66(1):41–68.
Plessier A, Rautou P-E, Valla D-C. Management of hepatic vascular diseases. J Hepatol. 2012;56(Suppl 1):S25–38.
Nayak NC, Ramalingaswami V. Obliterative portal venopathy of the liver. Associated with so-called idiopathic portal hypertension or tropical splenomegaly. Arch Pathol. 1969;87(4):359–69.
Cazals-Hatem D, Hillaire S, Rudler M, Plessier A, Paradis V, Condat B, u. a. Obliterative portal venopathy: portal hypertension is not always present at diagnosis. J Hepatol März 2011;54(3):455–461.
Wanless IR. Micronodular transformation (nodular regenerative hyperplasia) of the liver: a report of 64 cases among 2,500 autopsies and a new classification of benign hepatocellular nodules. Hepatol Baltim Md. 1990;11(5):787–97.
Levison DA, Kingham JG, Dawson AM, Stansfeld AG. Slow cirrhosis—or no cirrhosis? A lesion causing benign intrahepatic portal hypertension. J Pathol Juli. 1982;137(3):253–72.
Polish E, Christie J, Cohen A, Sullivan B. Idiopathic presinusoidal portal hypertension (Banti’s syndrome). Ann Intern Med. 1962;56:624–7.
Okuda K. Non-cirrhotic portal hypertension versus idiopathic portal hypertension. J Gastroenterol Hepatol. 2002;17(Suppl 3):S204–13.
Schouten JNL, Verheij J, Seijo S. Idiopathic non-cirrhotic portal hypertension: a review. Orphanet J Rare Dis. 2015;10:67.
Khanna R, Sarin SK. Non-cirrhotic portal hypertension—diagnosis and management. J Hepatol Februar. 2014;60(2):421–41.
Kobayashi Y, Inokuchi K, Saku M. Epidemiology of idiopathic portal hypertension based on a nationwide survey. Rep Minist Health Welf Res Comm Idiopathic Portal Hypertens. 1976:10–5.
Sarin SK, Kumar A, Chawla YK, Baijal SS, Dhiman RK, Jafri W, u. a. Noncirrhotic portal fibrosis/idiopathic portal hypertension: APASL recommendations for diagnosis and treatment. Hepatol Int 2007;1(3):398–413.
European Association for the Study of the Liver. Electronic address: easloffice@easloffice.eu. EASL Clinical Practice Guidelines. Vascular diseases of the liver. J Hepatol Januar. 2016;64(1):179–202.
Guido M, Sarcognato S, Sonzogni A, Lucà MG, Senzolo M, Fagiuoli S, u. a. Obliterative portal venopathy without portal hypertension: an underestimated condition. Liver Int Off J Int Assoc Study Liver. 2016;36(3):454–460.
Barge S, Grando V, Nault J-C, Broudin C, Beaugrand M, Ganne-Carrié N, u. a. Prevalence and clinical significance of nodular regenerative hyperplasia in liver biopsies. Liver Int Off J Int Assoc Study Liver 2016;36(7):1059–1066.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Andrea De Gottardi and Pierre-Emmanuel Rautou each declare no potential conflicts of interest.
Human and Animal Rights and Informed Consent
This article contains no studies with human or animal subjects performed by any of the authors.
Additional information
Andrea De Gottardi and Pierre-Emmanuel Rautou VALDIG, the vascular liver disease group
This article is part of the Topical Collection on Portal Hypertension
Rights and permissions
About this article

Cite this article
De Gottardi, A., Rautou, PE. Idiopathic Non-cirrhotic Portal Hypertension and Close Entities: a Need for Clarifying Terminology. Curr Hepatology Rep 16, 237–240 (2017). https://doi.org/10.1007/s11901-017-0358-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11901-017-0358-6