
Abstract
Genotype 2 of the hepatitis C virus (HCV) accounts for 10 % of the patients with chronic HCV worldwide. Until 2013, the standard of care (SOC) and only therapeutic option in these patients was a course of 24 weeks of pegylated interferon (PegIFN) plus ribavirin (Rbv), with sustained virological response rates (SVRs) in the 80–90 % range. Despite the potentially high attainable SVR rates, PegIFN plus Rbv is poorly tolerated due to the side effects of both drugs and is often contraindicated due to concomitant comorbid conditions. The improved knowledge of the structure of the HCV genome and its life cycle has allowed to develop drugs that target key viral replication steps with the aim of directly inhibiting HCV replication. Among these so-called directly acting antivirals (DAAs), sofosbuvir (SOF), an NS5B HCV polymerase nucleotide analog inhibitor, has pan-genotypic activity and has been approved for the treatment of HCV genotypes 1, 2, 3, 4, 5, and 6 (HCV-1, HCV-2, HCV-3, HCV-4, HCV-5, and HCV-6) patients in combination with Rbv ± PegIFN. For HCV-2, the combination of SOF plus Rbv represents the first all-oral IFN-free regimen that has become the new standard of care treatment. Phase III trials have reported optimal safety and high efficacy of SOF plus Rbv in patients with chronic HCV infection, with SVR rates for HCV-2 that reached 98–100 % by subgroup analysis. In countries where SOF is not available, treatment optimization of PegIFN/Rbv therapy is essential to maximize efficacy and reduce treatment-related side effects in HCV-2 patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Chronic hepatitis C virus (HCV) infection is a global health burden as it affects nearly 170 million people worldwide accounting for 3 % of the global population, and if the disease remains untreated, it can be complicated by cirrhosis, end-stage liver disease, and hepatocellular carcinoma (HCC). HCV circulates in seven genotypes which have peculiar geographical distribution [1]. HCV-2 accounts for nearly 10 % of all chronic hepatitis C cases, and its prevalence ranges from 5 % in Turkey and some regions of the USA to more than 25 % in Southern Europe and South Korea. In Europe, its mean prevalence is estimated to be 8.2 % [2–4].
Chronic infection with HCV-2 is characterized by some peculiarities, and indeed, HCV-2 patients when left untreated have slower fibrosis progression rates over time than patients infected with other genotypes [5–7]; still, HCV-2 carries a risk of spontaneous viral reactivation that is part of the natural course of HCV chronic infection and is more frequently observed in carriers of HCV-2 than in HCV-1 patients [8, 9]. These sudden increases in alanine aminotransferase (ALT) values lead to a rapid progression of liver damage, fibrosis, and ultimately, the development of cirrhosis. ALT flares can also occur in HCV-2 patients with persistently normal or near-normal ALT levels, suggesting that HCV-2 patients with persistently normal ALT values are also at risk of progressive fibrosis due to ALT flares and thus represent a group of patients with high priority to treatment.
Chronic infection with HCV-2 is also associated with increased incidence of extrahepatic manifestations compared to other genotypes, including hematologic manifestations, as mixed cryoglobulinemia and B cell non-Hodgkin lymphoma [10]. However, the most known and important feature of the HCV-2 infection is its extremely favorable response to IFN-based treatment, with sustained virological response (SVR) rates that reach 90–95 % of cases [11–14]. These high SVR rates have led HCV-2 to be classified as an easy-to-treat genotype.
These high SVR rates do not take into account that many patients with HCV-2 are contraindicated to pegylated interferon (PegIFN)/ribavirin (Rbv) for several reasons including psychiatric disorders such as severe depression, autoimmune diseases, advanced cardiovascular disease, decompensated liver disease, and renal failure. For this reason, the development of all-oral and well-tolerated INF-free regimens represents the holy grail of anti-HCV treatment also for genotype 2 patients [15]. Treatment regimens including the oral nucleotide NS5B polymerase inhibitor sofosbuvir (SOF) have shown optimal efficacy and safety in patients with HCV genotype 2, de facto becoming the new standard of care for this genotype [16].
Treatment Options
The goal of therapy is to eradicate HCV infection in order to prevent the complications of HCV-related liver diseases and extrahepatic diseases, including fibrosis, cirrhosis, decompensation, HCC, and death. Morbidity and mortality are decreased with a successful treatment of chronic HCV infection [17].
PegIFN-Based Regimens
Until the end of 2013, the standard of care for patients with HCV-2 was PegIFN in combination with Rbv for 24 weeks, resulting in an SVR in 80–95 % of patients as shown in Table 1.
Predictors of treatment outcome during PegIFN regimens can be useful tools for the decision making and for treatment individualization. Most factors involved in predicting the outcome of therapy with other HCV genotypes, such as HCV baseline viremia or single nucleotide polymorphisms (SNPs) in the interferon lambda 3 (IFNL3) region, do not play a major role in determining the efficacy of PegIFN plus Rbv in HCV-2 patients. An association with IFNL3 was found in a study conducted by Mangia et al. in HCV-2 patients without a rapid virological response (RVR), i.e., those in whom HCV RNA was still detected after 4 weeks of therapy. In this subgroup of patients, the presence of the favorable rs1299860 CC genotype was associated with higher SVR rates than those seen in CT/TT patients (66 vs 45 %). Recently, a large cohort study on more than 1000 patients with HCV-2 and HCV-3 infection reported an association between IFNL3 SNPs and treatment outcome with SVR rates in HCV-2 patients being 79 % in the CC genotype versus 66 % in those with the T allele (p = 0.001) [18].
Conversely, the presence of advanced fibrosis or cirrhosis represents a much strong predictor of treatment failure in HCV-2 patients with lower rates of SVR, with some studies reporting rates as low as 50 %, with a higher trend of virological relapse.
A more practical clinical usefulness can be attributed to treatment predictors such as the achievement of an RVR that is reported in 70–90 % of HCV-2 patients, and that leads to an SVR in 90 % of cases. HCV RNA kinetics plays a fundamental role to optimize treatment in HCV-2 infection, because RVR can identify a subgroup of highly responsive patients that can be considered for abbreviated therapies. Several studies have analyzed the possibility to tailor the duration of PegIFN and Rbv treatment according to treatment response: HCV-2 patients with an RVR were randomized to either 12–16 weeks of PegIFN plus Rbv or 24 weeks of treatment duration, showing that SVR rates did not differ between shorter and standard treatments. In RVR patients, SVR rates of 83.8 % following abbreviated treatments and 89.3 % with standard duration were reported by recent meta-analysis (RR 1.02, 95 % confidence interval (CI) 0.97–1.06). However, the same study demonstrated that weight-based dosing of Rbv (1000–1200 mg/day) is crucial to maximize SVR rates when considering a shortened treatment duration in HCV-2 patients with an RVR. Treatment abbreviation is generally not recommended in those patients with baseline predictors of treatment failure such as advanced fibrosis or cirrhosis, high BMI, high baseline viremia, and insulin resistance. The reason is that these patients are exposed to a higher risk of posttreatment relapse with shorter treatment durations than the standard 24 weeks [12].
Increasing dose or duration of therapy in difficult-to-cure subgroups of HCV-2 patients in theory represents a reasonable treatment option, still a weight-based dose of Rbv has not been shown to be more effective than the standard fixed dose of 800 mg/day [19], while extended treatment duration beyond 24 weeks in patients without RVR or with negative predictors of treatment outcome such as cirrhosis has not been studied properly in a randomized clinical trial. Notwithstanding, many experts suggest an extension of treatment to 48 weeks in this group of patients to reduce relapse rates [20].
IFN-Free Therapies
Although patients with HCV-2 usually achieve high SVR rates to a course of 24 weeks of PegIFN plus Rbv, there are categories of patients that still reach suboptimal SVR rates and are therefore in need of more effective treatment regimens. Moreover, a considerable proportion of patients (70 %) [21] still remain untreated because of absolute or relative contraindications to interferon therapy, such as hepatic decompensation, autoimmune diseases, and psychiatric disorders. In addition, IFN still carries well-known adverse events that can cause a range of constitutional symptoms or hematologic abnormalities that may require discontinuation of therapy in a considerable number of patients.
Furthermore, many other patients without known contraindications to therapy but intolerant to PegIFN plus Rbv treatment, such as liver transplant recipients, still remain without effective and safe treatment options. Clearly, this highlights the need for alternative and effective IFN-free regimens for HCV-2 patients. Significant improvements in the knowledge of the HCV genome structure and the HCV life cycle have led to the development of drugs that directly inhibit HCV replication, the directly acting antivirals (DAAs).
The first-generation DAAs, the NS3/4A protease inhibitors started a new era in HCV infection treatment. Boceprevir (BOC) and telaprevir (TVR), combined with PegIFN plus Rbv, allowed an overall improvement in SVR rates from approximately 40 to 60 % in HCV-1 patients. However, these DAAs should be used only in patients with genotype 1 infection, as their efficacy in other HCV genotypes has not been clearly defined. TVR in patients with HCV genotype 2 was studied by Foster and colleagues in 23 HCV-2 and 26 HCV-3 treatment-naïve patients [22]. They were randomized to receive either TVR monotherapy for 2 weeks (group A), TVR triple therapy, in combination with PegIFN/Rbv, for 2 weeks (group B) or placebo plus PegIFN/Rbv for 2 weeks (group C). Following the first 2 weeks of therapy, all patients received 24 weeks of PegIFN and Rbv. The reported SVR rates were 56 % in group A, 100 % in group B, and 89 % in group C. No patient achieved HCV RNA undetectability at week 2, while some cases of viral breakthrough were seen between days 12 and 15 of monotherapy.
The safety and efficacy of BOC in patients with genotype 2 was assessed by Silva et al. in a study including seven treatment-naïve patients [23]. BOC was given in monotherapy for 2 weeks at different doses: 200 mg twice daily (BID), 400 mg BID, 400 mg three times a day (TID), or placebo. The maximum decrease in HCV RNA values was similar between placebo and BOC 200 mg BID (0.48 IU/mL log10) and BOC 400 mg BID (0.28 IU/mL log10), while it was higher than placebo in the patients who received BOC 400 mg TID (1.39 IU/mL log10). HCV RNA undetectability after 15 days of BOC monotherapy was never achieved in the study. Based on these two studies, it is safe to conclude that TVR and BOC possess some anti-HCV genotype 2 activity in vivo, but still due to limited data and their suboptimal tolerability, they cannot be recommended as a treatment option in the clinical practice for HCV-2 patients.
For HCV genotype 2, an all-oral regimen of SOF with Rbv has become the new standard of care treatment. On December 2013, SOF was approved by the US Food and Drug Administration as the first nucleotide therapy for the treatment of hepatitis C, and it received European Medical Agency approval in January 2014. This represents a landmark in HCV treatment, because, for the first time, a patient can be treated with an all-oral IFN-free regimen and no longer have to suffer the debilitating side effects associated with a 24-week course of IFN. The all-oral regimen is extremely simple as it consists of a single 400-mg pill of SOF and a BID weight-based dose of Rbv for 12 weeks.
SOF is an oral nucleotide analog inhibitor of the NS5B polymerase, which demonstrates potent in vitro activity against all HCV genotypes. Its clinical efficacy has been demonstrated in a variety of populations, which include all ethnic groups, advanced liver disease, cirrhotics, previous treatment experienced, and posttransplant, and also has a high barrier to resistance [16]. SOF is excreted by kidneys and, as such, does not require dose modifications in the case of severe liver function impairment; however, it is contraindicated in patients with estimated glomerular filtration rate <30 mL/min/1.73 m or with end-stage renal disease.
To date, no significant drug-drug interaction has been reported, even in patients typically difficult to treat because of other concomitant medications, such as those coinfected with HIV virus or transplant recipients. Only potent P-gp inducers such as rifampin, carbamazepine, phenytoin, or St. John’s Wort significantly decrease SOF plasma concentrations and may lead to a reduced therapeutic effect. No food effect has been observed with SOF, and thus far, no significant safety signal has been reported. Finally, although the S282T NS5B mutation has been identified in vitro as associated with resistance to SOF, only one case of S282T has been identified during treatment in the phases II and III program. All these characteristics make SOF safe, effective, and well tolerated.
Phase II trials showed that SOF, at the dose of 400 mg once daily, achieves potent and rapid suppression of HCV replication. Also, phase II studies demonstrated the possibility to treat patients with HCV genotype 2 with SOF in combination with Rbv without PegIFN. This was not the case for other HCV genotypes where the addition of PegIFN to SOF plus Rbv treatment increases the response rate for HCV genotypes and, as such, is recommended for HCV-1, HCV-4, and HCV-6.
Data from phase III trials demonstrated the safety and efficacy of SOF in patients with chronic HCV infection. Three trials were conducted in subjects with HCV genotype 2 or 3, and one study evaluated genotypes 1, 4, 5, and 6.
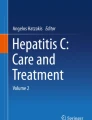
The FISSION study assessed treatment-naïve patients with HCV-2 or HCV-3 infection, comparing an IFN-free regimen of Rbv plus SOF for 12 weeks with 24 weeks of PegIFN plus Rbv. The IFN-free regimen was well tolerated with no resistance reported, and it was associated with a higher SVR12 rate in patients infected with HCV-2, with an SVR rate of 97 versus 78 % for the PegIFN/Rbv treatment arm (Fig. 1). Non-cirrhotic patients also had higher SVR12 rates than cirrhotic patients in both treatment groups [24].

SVR12 rates in HCV-2 patients stratified by disease severity, the FISSION, FUSION, and POSITRON study results
The FUSION study evaluated SOF plus Rbv for 12 or 16 weeks in treatment-experienced patients who previously failed an interferon-based therapy. The 16-week treatment duration group was included to evaluate the benefits of an extended duration of treatment in this difficult-to-treat population. In non-cirrhotic HCV-2 patients, 12-weeks of SOF plus Rbv were effective and well tolerated, whereas for cirrhotic patients, the 16-week regimen of treatment provided an added benefit in terms of SVR rates.
SVR rates increased from 86 % with 12 weeks of treatment to 94 % with the 16-week schedule, and the most significant benefit was seen in cirrhotics where treatment extension to 16 weeks increased the SVR from 60 to 78 % (Fig. 1) [25].
The safety and tolerability profile was excellent, with the most common adverse event being fatigue (40 % of patients), headache (23 %), and nausea (20 %). Side effect incidence was similar in patients receiving SOF plus Rbv treatment for 12 or 16 weeks.
Interestingly in the phase III development program of SOF, no genotypic or phenotypic viral resistance to SOF was detected.
The POSITRON study was a double-blinded, placebo-controlled, phase 3 trial that assessed patients infected with HCV-2 or HCV-3 who were ineligible, intolerant, or unwilling to take IFN therapy. Patients received SOF plus Rbv therapy or placebo for 12 weeks. The majority of patients considered IFN-ineligible had psychiatric comorbidity (58 %), while most IFN intolerance was attributed to flu-like symptoms (32 %). HCV-2 patients showed SVR rates of 93 %, while cirrhotic patients had an SVR rate of 94 % (Fig. 1) [25].
Recently, Zeuzem et al. conducted a study on naïve and experienced HCV-2 and HCV-3 patients, where SOF plus Rbv treatment was given for 12 weeks to HCV-2 patients and extended to 24 weeks in HCV-3 patients. An SVR was seen in 68 out of 73 patients (93 %; 95 % CI 85 to 98) with HCV genotype 2 infection who were treated for 12 weeks [26].
The overall message from the phase III trials of SOF plus Rbv in HCV-2 patients is that 12 weeks of treatment achieve SVR rates in the 90 % in most patients, but treatment extension to 16 weeks increases SVR rates in cirrhotics who failed the previous course of PegIFN and ribavirin.
In this difficult-to-cure group of HCV-2, another treatment option is the triple therapy PegIFN/Rbv/SOF regimen which was investigated in the LONESTAR-2 study. LONESTAR-2 is a phase IIb study enrolling 23 treatment-experienced HCV-2 patients, including 14 with cirrhosis, who received 12 weeks of PegIFN plus Rbv plus SOF, wherein an SVR was reported in 96 % of patients.
The new EASL Recommendations on Treatment of Hepatitis C support SOF plus Rbv for 12 weeks as the standard of care for HCV-2 patients. In difficult-to-treat population, as cirrhotics, especially if treatment experienced, a prolongation to 16 or 20 weeks is recommended. Alternatively, cirrhotic and/or treatment-experienced patients could be treated with PegIFN plus Rbv plus SOF for 12 weeks. In settings where these options are not available, the combination of PegIFN plus Rbv remains acceptable [27].
Future Treatment Options
The combination of SOF plus Rbv attains optimal SVR rates in most patients with HCV-2 infection, and still, it requires an extension to 16 weeks or a combination with PegIFN in some difficult-to-cure groups of patients. Moreover, Rbv is associated with side effects that impair the quality of life of the patients, is contraindicated during pregnancy, and is hard to manage due to accumulation in the blood in patients with renal impairment. For these reasons, there is still a place for drug development in anti-HCV-2 treatment. To eliminate Rbv and to shorten treatment duration down to 6–8 weeks, SOF needs to be combined with another DAA active on genotype 2 of HCV. Second-wave protease inhibitors and first- and second-generation NS5A inhibitors are effective against this viral strain and, in theory, could be optimal partners for sofosbuvir [28]. To date, only one study examined the association of SOF with another DAA, namely daclatasvir, a first-in-class NS5A inhibitor, that shows high antiviral activity against all HCV genotypes at a dose of 60 mg orally once daily. SOF plus daclatasvir given for 24 weeks, with and without Rbv, was studied in HCV genotypes 1, 2, and 3 treatment-naïve and treatment-experienced patients in a study conducted by Sulkowsky et al. Overall, 211 patients received treatment. Among patients with genotype 2 infection, 92 % of them achieved an SVR with an Rbv-free 24-week treatment course [29].
Conclusions
Infection with HCV-2 is characterized by elevated SVR rates to PegIFN plus Rbv, with the possibility to optimize treatment by shortening the overall duration without compromising efficacy in a large group of patients, those with an RVR.
SOF plus Rbv, the new gold standard for these patients, seems to be an effective answer to HCV-2 infection, but PegIFN, in addition to SOF plus Rbv, still remains a viable option especially in difficult-to-treat patients, such as those with cirrhosis.
The combination of multiple DAAs, with or without SOF, is likely to allow for shorter and Rbv-free regimens in the next 2 years [30].
Abbreviations
- HCV:
-
Hepatitis C virus
- SNP:
-
Single nucleotide polymorphism
- SVR:
-
Sustained virological response
- RVR:
-
Rapid virological response
- PegIFN:
-
Pegylated interferon
- Rbv:
-
Ribavirin
- BID:
-
Twice daily
- TID:
-
Three times a day
- DAA:
-
Directly acting antiviral
- TVR:
-
Telaprevir
- BOC:
-
Boceprevir
- SOF:
-
Sofosbuvir
- HCC:
-
Hepatocellular carcinoma
References
Smith DB, Bukh J, Kuiken C, Muerhoff AS, Rice CM, Stapleton JT, et al. Expanded classification of hepatitis C virus into 7 genotypes and 67 subtypes: updated criteria and genotype assignment web resource. Hepatology. 2014;59(1):318–27.
Altuglu I, Soyler I, Ozacar T, Erensoy S. Distribution of hepatitis C virus genotypes in patients with chronic hepatitis C infection in Western Turkey. Int J Infect Dis. 2008;12(3):239–44.
Young AM, Crosby RA, Oser CB, Leukefeld CG, Stephens DB, Havens JR. Hepatitis C viremia and genotype distribution among a sample of nonmedical prescription drug users exposed to HCV in rural Appalachia. J Med Virol. 2012;84(9):1376–87.
Oh DJ, Park YM, Seo YI, Lee JS, Lee JY. Prevalence of hepatitis C virus infections and distribution of hepatitis C virus genotypes among Korean blood donors. Ann Lab Med. 2012;32(3):210–5.
Marabita F, Aghemo A, De Nicola S, et al. Genetic variation in the interleukin-28B gene is not associated with fibrosis progression in patients with chronic hepatitis C and known date of infection. Hepatology. 2011;54(4):1127–34.
Bochud PY, Cai T, Overbeck K, et al. Genotype 3 is associated with accelerated fibrosis progression in chronic hepatitis C. J Hepatol. 2009;51(4):655–66.
De Nicola S, Aghemo A, Rumi MG, Colombo M. HCV genotype 3: an independent predictor of fibrosis progression in chronic hepatitis C. J Hepatol. 2009;51(5):964–6.
Rumi MG, De Filippi F, Donato MF, Del Ninno E, Colombo M. Progressive hepatic fibrosis in healthy carriers of hepatitis C virus with a transaminase breakthrough. J Viral Hepat. 2002;9(1):71–4.
Rumi MG, De Filippi F, La Vecchia C, et al. Hepatitis C reactivation in patients with chronic infection with genotypes 1b and 2c: a retrospective cohort study of 206 untreated patients. Gut. 2005;54(3):402–6.
Hartridge-Lambert SK, Stein EM, Markowitz AJ, Portlock CS. Hepatitis C and non-Hodgkin lymphoma: the clinical perspective. Hepatology. 2012;55(2):634–41.
Rizzetto M. Treatment of hepatitis C virus genotype 2 and 3 with pegylated interferon plus ribavirin. J Hepatol. 2005;42(2):275–6.
Aghemo A, Rumi MG, Monico S, et al. The pattern of pegylated interferon-alpha2b and ribavirin treatment failure in cirrhotic patients depends on hepatitis C virus genotype. Antivir Ther. 2009;14(4):577–84.
Rumi MG, Aghemo A, Prati GM, et al. Randomized study of peginterferon-alpha2a plus ribavirin vs peginterferon-alpha2b plus ribavirin in chronic hepatitis C. Gastroenterology. 2010;138(1):108–15.
European Association for the Study of the Liver. EASL Clinical Practice Guidelines: management of hepatitis C virus infection. J Hepatol. 2011;55:245–64.
Grassi E, Aghemo A. How to optimize HCV therapy in genotype 2 patients. Liver Int. 2013;33 Suppl 1:35–40.
Degasperi E, Aghemo A. Sofosbuvir for the treatment of chronic hepatitis C: between current evidence and future perspectives. Hepat Med. 2014;6:25–33.
Aghemo A, Lampertico P, Colombo M. Assessing long-term treatment efficacy in chronic hepatitis B and C: between evidence and common sense. J Hepatol. 2012;57(6):1326–35.
Eslam M, Leung R, Romero-Gomez M, Mangia A, Irving WL, Sheridan D, et al. IFNL3 polymorphisms predict response to therapy in chronic hepatitis C genotype 2/3 infection. J Hepatol. 2014;61(2):235–41.
Jacobson IM, Brown Jr RS, McCone J, Black M, Albert C, Dragutsky MS, et al. Impact of weight-based ribavirin with peginterferon alfa-2b in African Americans with hepatitis C virus genotype 1. Hepatology. 2007;46(4):982–90.
Craxì A, Pawlotsky JM, Wedemeyer H, Bjoro K, Flisiak R, Forns X, et al. EASL Clinical Practice Guidelines: management of hepatitis C virus infection. J Hepatol. 2011;55(2):245–64.
Falck-Ytter Y, Kale H, Mullen KD, Sarbah SA, Sorescu L, McCullough AJ. Surprisingly small effect of antiviral treatment in patients with hepatitis C. Ann Intern Med. 2002;136(4):288–92.
Foster GR, Hézode C, Bronowicki JP, et al. Telaprevir alone or with peginterferon and ribavirin reduces HCV RNA in patients with chronic genotype 2 but not genotype 3 infections. Gastroenterology. 2011;141(3):881–9.
Silva MO, Treitel M, Graham DJ, Curry S, Frontera MJ, McMonagle P, et al. Antiviral activity of boceprevir monotherapy in treatment-naive subjects with chronic hepatitis C genotype 2/3. J Hepatol. 2013;59(1):31–7.
Lawitz E, Mangia A, Wyles D, et al. Sofosbuvir for previously untreated chronic hepatitis C infection. N Engl J Med. 2013;368:1878–87.
Jacobson IM, Gordon SC, Kowdley KV, et al. Sofosbuvir for hepatitis C genotype 2 or 3 in patients without treatment options. N Engl J Med. 2013;368:1867–77.
Zeuzem S, Dusheiko GM, Salupere R, Mangia A, Flisiak R, Hyland RH, et al. Sofosbuvir and ribavirin in HCV genotypes 2 and 3. N Engl J Med. 2014;370(21):1993–2001.
European Association for the Study of the Liver. EASL Recommendations on Treatment of Hepatitis C 2014. J Hepatol. 2014;61(2):373–95.
Pawlotsky JM. New hepatitis C therapies: the toolbox, strategies, and challenges. Gastroenterology. 2014;146(5):1176–92.
Sulkowski MS, Gardiner DF, Rodriguez-Torres M, Reddy KR, Hassanein T, Jacobson I, et al. Daclatasvir plus sofosbuvir for previously treated or untreated chronic HCV infection. N Engl J Med. 2014;370(3):211–2.
Gaetano JN. Benefit-risk assessment of new and emerging treatments for hepatitis C: focus on simeprevir and sofosbuvir. Drug Healthc Patient Saf. 2014;6:37–45.
Compliance with Ethics Guidelines
Conflict of Interest
Massimo Colombo, M.D., received grant and research support from BMS and Gilead Science; is a member of advisory committees of Merck, Roche, Novartis, Bayer, BMS, Gilead Science, Tibotec, Vertex, Janssen Cilag, Achillion, Lundbeck, GSK, GenSpera, AbbVie, Alfa Wasserman, and Jennerex; and is a person in charge in speaking and teaching in Tibotec, Roche, Novartis, Bayer, BMS, Gilead Science, Vertex, Merck, Janssen, and Sanofi.
Alessio Aghemo, M.D., is a member of the advisory board of AbbVie and Gilead Sciences and of the speaker bureau of AbbVie, Gilead Sciences, Janssen, and Merck.
Eleonora Grassi, M.D., declares no financial disclosure.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by the authors.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Grassi, E., Aghemo, A. & Colombo, M. Optimal Management of Hepatitis C Genotype 2 Chronic Infection. Curr Hepatology Rep 13, 273–278 (2014). https://doi.org/10.1007/s11901-014-0248-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11901-014-0248-0