
Abstract
Purpose of Review
The most pertinent clinical question in post-coronary computed tomography angiography (CCTA) patients is the assessment of the physiological significance of an anatomically identified stenosis. The clinical application of radionuclide MPI using single-photon emission computed tomography (SPECT) versus positron emission tomography (PET) in the evaluation and management of patients with an inconclusive CCTA is reviewed using a case-based approach.
Recent Findings
Recent evidence suggests that CCTA is the most sensitive non-invasive test to exclude angiographic CAD and may be an effective first-line test especially among symptomatic low-intermediate risk patients. However, in the presence of angiographic atherosclerosis, its specificity and positive predictive value for identifying flow-limiting stenosis are modest.
Summary
Radionuclide myocardial perfusion imaging offers accurate quantitative assessment of myocardial ischemia, which helps with risk stratification and patient management especially the potential need for revascularization. Routine accurate quantifications of myocardial blood flow and flow reserve are major advantages of PET MPI, which are especially useful when used in patients at intermediate-high clinical risk.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Over the last 10 years, CCTA has emerged as a powerful test for diagnosis of coronary artery disease (CAD) and recent evidence suggests that it may be an effective first-line test especially among symptomatic low-intermediate risk patients [1]. Current evidence suggests that CCTA is the most sensitive non-invasive test to exclude angiographic CAD. However, in the presence of angiographic atherosclerosis, its specificity and positive predictive value for identifying flow-limiting stenosis are modest [1]. Consequently, assessing the physiological significance of angiographically identified stenoses is an important clinical question after CCTA.
Radionuclide myocardial perfusion imaging (MPI) has consistently remained one of the most widely used modalities for the diagnosis of hemodynamically significant CAD. The strengths of radionuclide MPI include its wide availability, accurate and reproducible quantification of myocardial ischemia, and robust risk stratification. The emergence of positron emission tomography now offers the unique ability to quantify regional and global myocardial blood flow (MBF, in mL/min/g of myocardial tissue) and calculate myocardial flow reserve (ratio of stress MBF over that at rest). As discussed below, recent evidence suggests that quantitative PET is a powerful tool for diagnosing flow-limiting CAD, evaluate prognosis and guide selection of patients for revascularization.
In this review, we will use a case-based approach to discuss common clinical scenarios for the use of radionuclide MPI. The presentation will include a discussion of the relative merits of SPECT and PET MPI in each clinical scenario.
Technical Considerations and Clinical Significance of Radionuclide MPI
Table 1 summarizes important technical differences between SPECT and PET myocardial perfusion imaging.
Accuracy of Perfusion Tracers
The basic principle of radionuclide MPI for detecting CAD is based on the ability of a radiotracer to identify a transient regional perfusion deficit in a myocardial region subtended by a coronary artery with a flow-limiting stenosis. Consequently, diagnostic sensitivity of radionuclide MPI depends largely on the relationship between coronary blood flow and radiotracer uptake. Radiotracers with a more linear relationship between coronary blood flow and myocardial retention are typically associated with a higher sensitivity for detecting flow-limiting stenosis. PET myocardial perfusion tracers have a more favorable (more linear) relationship between coronary blood flow and myocardial retention than those for SPECT imaging [2•], thereby increasing sensitivity and decreasing false-negative scans.
Routine Attenuation Correction
Routine-measured (depth independent) attenuation correction with PET decreases false positives and, thus, increases specificity. Attenuation correction is also available for SPECT, but only used in the minority of clinical scans.
Quantitative MBF
Myocardial blood flow (in mL/min/g of myocardium) and myocardial flow reserve (MFR) are measured routinely by post-processing of myocardial perfusion PET images [3]. These measurements integrate the fluid-dynamic effects of focal epicardial coronary stenosis and diffuse atherosclerosis, as well as microvascular dysfunction on myocardial perfusion, thereby providing a sensitive measure of myocardial ischemia [4]. As discussed below, these measurements of MFR have important diagnostic [5,6,7,8,9] and prognostic [10,11,12,13,14,15,16] implications in the evaluation and management [14, 17] of the patients with known or suspected CAD.
Combination with Exercise
This is a routine for SPECT imaging. The ultrashort physical half-live of PET radiotracers makes a combination with exercise much more challenging. As discussed below, this is important in some clinical scenarios and may determine the choice of imaging technique.
Exam Length
Given the ultrashort half-live of PET radiotracers, imaging protocols are typically shorter than those for SPECT imaging.
Availability and Cost
The production of currently FDA-approved PET radiotracers requires an on-site generator (82Rubidium) or a medical cyclotron (13N-ammonia), thereby increasing the cost for availability of PET imaging compared with SPECT.
Radiation Dosimetry
The use of ultrashort lived radiotracers with PET MPI is associated with a more favorable radiation dose to patients compared with SPECT MPI.
Patient-Centered Clinical Applications of Radionuclide MPI After Coronary CTA
Evaluation of Patients with Intermediate Stenosis on CCTA
Case Vignette # 1
The patient was a 57-year-old female with long-standing hypertension, hyperlipidemia, type 2 diabetes mellitus, and current smoker who presented with moderate intensity, intermittent chest pain that started an hour prior to her arrival to the emergency department. In the emergency department, she was chest pain free. A rest ECG demonstrated normal sinus rhythm with non-specific T wave changes. Serial high-sensitivity troponin T (hs-TnT) was negative. She was referred for a CCTA for evaluation of CAD.
The CCTA images (Fig. 1A) demonstrated a large amount of noncalcified plaque in the mid left circumflex (LCx) artery causing moderate stenosis (50–69%). In addition, there was a moderate amount of predominantly noncalcified plaque in the mid left anterior descending (LAD) artery causing mild stenosis (25–49%), and a small amount of predominantly calcified plaque in the distal ramus intermedius artery causing minimal stenosis (1–24%). In order to determine the hemodynamic significance of the intermediate plaques, especially in the mid LCx, an exercise MPI SPECT study was requested. The patient exercised for 7 mins of a Bruce protocol (8.5 metabolic equivalents [METs]), reaching 90% of age-predicted maximal heart rate (APMHR) with an appropriate blood pressure response to exercise. The ECG response to exercise was negative for ischemia. Regional myocardial perfusion and global systolic function were normal (Fig. 1B). The patient was discharged home after counseling for lifestyle modifications and continuation of statin therapy. Shortly thereafter, she had an invasive coronary angiogram (ICA) for recurrent chest pain that confirmed non-obstructive CAD (Fig. 1C).

Coronary computed tomography angiography (CCTA), SPECT myocardial perfusion, and invasive coronary angiographic images in a patient with atypical chest pain. (A) The CCTA shows a large amount of noncalcified plaque in the mid portion of the left circumflex (LCx) artery causing moderate stenosis (50–69%) (red circle). (B) The stress and rest myocardial perfusion images demonstrate normal regional myocardial perfusion. (C) The ICA images demonstrate non-obstructive CAD
This case illustrates the clinical challenges in choosing the right test for intermediate-high risk patients presenting with chest pain, especially in the setting of cardiometabolic disease. Data from the COroNary CT Angiography Evaluation For Clinical Outcomes: An InteRnational Multicenter Registry (CONFIRM) [18] and the Screening For Asymptomatic Obstructive Coronary Artery Disease Among High-Risk Diabetic Patients Using CT Angiography, Following Core 64 (faCTor-64) [19] showed that approximately 70% of patients with diabetes demonstrate evidence of angiographic atherosclerosis on CCTA. The demonstration of angiographically obstructive plaque by CCTA, as in case vignette 1, usually triggers additional investigations to determine the physiologic significance of those plaques. This patient had no clinical or scintigraphic evidence of stress-induced ischemia at a high cardiac workload. The referral to invasive coronary angiography in the setting of recurrent chest pain confirmed the absence of angiographically obstructive CAD.
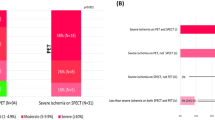
A recent meta-analysis of four randomized controlled trials (RCT) comparing CCTA versus stress testing for triage of acute chest pain in the emergency department showed that the use of CCTA in this setting is associated with decreased emergency department’s cost and length of stay but an increased rate of ICA and subsequent revascularization [20]. In these four RCTs, there were no deaths and no difference in the incidence of myocardial infarction, post-discharge ED visits, or rehospitalizations between the CCTA and stress testing strategies. All four studies reported decreased length of stay with CCTA while three reported cost savings. Compared with stress testing, CCTA was associated with a 36% and 81% relative increase in the likelihood of referral to ICA and revascularization, respectively.
Evaluation of Patients with Chest Pain and Extensive Coronary Calcifications on Cardiac CT
Case Vignette # 2
The patient was a 63-year-old female with hypertension, type 2 diabetes mellitus, and dyslipidemia who presented with atypical chest pain. A recent non-contrast cardiac CT scan demonstrated a coronary artery calcium score of 750. She was referred for a regadenoson MPI PET/CT study to evaluate for CAD. The PET MPI images demonstrated normal regional myocardial perfusion (Fig. 2 upper left) and global systolic function. Extensive coronary artery calcifications were again seen on her transmission CT images especially involving the left main and left anterior descending coronary arteries (Fig. 2 upper right). The quantitative myocardial blood flow and flow reserve values were normal (Fig. 2 lower left), indicating no evidence of flow-limiting CAD or coronary microvascular dysfunction (CMD) as a cause for her chest pain.

Myocardial perfusion PET and non-contrast CT images in a patient with atypical angina. Upper left panel: Regadenoson stress and rest myocardial perfusion PET images demonstrating normal regional myocardial perfusion. Upper right panel: CT transmission images demonstrating extensive and dense coronary artery calcium in the left main and LAD coronary arteries (red circle). Lower left panel: Quantitative PET data demonstrating normal regional and global MBF and flow reserve. Normal stress MBF > 1.8 mL/min/g, and normal flow reserve > 2
This case illustrates the incremental value of quantitative PET myocardial perfusion imaging in the setting of extensive evidence of coronary atherosclerosis by cardiac CT. Recent meta-analyses [21, 22] and a prospective European multicenter study (Evaluation of Integrated CAD Imaging in Ischemic Heart Disease - EVINCI) [23] suggest that PET MPI is one of the most accurate non-invasive techniques for detecting obstructive angiographic stenosis. Furthermore, a recent meta-analysis using fractional flow reserve (FFR) rather than percent angiographic stenosis as gold standard for flow-limiting CAD demonstrated higher sensitivity, specificity, and negative and positive predictive values for PET over SPECT MPI [24].
As outlined above, a unique advantage of PET over SPECT is that it allows routine quantification of myocardial blood flow and flow reserve. These quantitative measures of myocardial perfusion improve the sensitivity and negative predictive value of PET for ruling out high-risk angiographic CAD [5,6,7,8,9]. In fact, the results of the Prospective Comparison of Cardiac PET/CT, SPECT/CT Perfusion Imaging and CT Coronary Angiography With Invasive Coronary Angiography (PACIFIC) study confirmed the superiority of quantitative PET MPI for detection of flow-limiting CAD [25], including the combination of CCTA with CTFFR [26•]. In symptomatic patients without documentation of angiographic stenosis, quantitative myocardial blood flow and flow reserve provide incremental information that helps exclude or establish the diagnosis of CMD as the potential source of patients’ symptoms, which is especially important in a high risk patient with cardiometabolic disease like in case vignette #2 [27, 28]. The normal flow reserve also helps place this patient with diabetes at low clinical risk [12]. In summary, in patients at intermediate-high clinical risk with extensive coronary calcifications, the availability of quantitative MBF information improves certainty regarding the presence or absence of flow-limiting CAD and helps exclude coronary microvascular dysfunction.
Evaluation of Patients with Known CAD and Abnormal CCTA
Case Vignette # 3
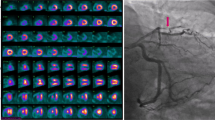
The patient was a 78-year-old man with a history of ST segment elevation myocardial infarction/ventricular fibrillation status post-percutaneous coronary intervention (PCI) with a bare metal stent in 1996, who presented to the office with recent onset dyspnea on exertion. A CCTA (Fig. 3) was notable for extensive calcified coronary plaque in all major epicardial coronary arteries, a complete occlusion of the proximal LAD stent (red circle), and severe luminal narrowing of the right and left circumflex coronary arteries. He underwent a regadenoson MPI PET/CT study that demonstrated transient ischemic dilatation during stress, extensive and severe stress-induced ischemia throughout the anterior, anteroseptal, and LV apex (Fig. 4 upper left), which on quantitative analysis involved 46% of the LAD territory (Fig. 4 upper right). On quantitative blood flow analysis, there was severe diffuse and severe reduction in stress myocardial blood flow and flow reserve in all major coronary artery territories, consistent with multivessel myocardial ischemia (Fig. 4 lower left). Global LV systolic function was normal. ICA demonstrated a total occlusion of the LAD coronary artery and extensive non-obstructive atherosclerosis of the right and left circumflex coronary arteries. The patient was referred for intervention of the chronic total occlusion of the LAD coronary artery.

Coronary computed tomography angiography (CCTA) images in a symptomatic patient with known CAD. The CCTA images demonstrate extensive calcified coronary plaque, complete luminal occlusion of the proximal LAD stent, along with severe luminal narrowing of the RCA and LCx. The red circle shows complete occlusion of the proximal LAD stent

Myocardial perfusion PET images in a patient with known CAD. Upper left panel: Regadenoson stress and rest myocardial perfusion PET images demonstrate transient ischemic dilatation and a large and severe area of stress-induced ischemia throughout the anterior and anteroseptal walls and the LV apex. Upper right panel: Polar maps demonstrate a large reversible perfusion defect, indicating ischemia, throughout the LAD territory. Lower left panel: Quantitative PET data demonstrating severely reduced regional and global MBF and flow reserve. Normal stress MBF > 1.8 mL/min/g, and normal flow reserve > 2
This case illustrates the role of stress imaging in patients with severe CAD. The PET scan identified extensive and severe myocardial ischemia in the territory of the LAD chronic total occlusion, which helped guide the decision to intervene in this symptomatic patient [29]. In light of the ICA findings, the severe diffuse reduction in stress myocardial blood flow and flow reserve in the left circumflex and right coronary territories is consistent with the presence of diffuse atherosclerosis and coronary microvascular dysfunction. Indeed, diffuse non-obstructive atherosclerosis in the epicardial coronary arteries is commonly found in over two-thirds of symptomatic patients with CMD [27, 30, 31, 32]. The presence of diffuse atherosclerosis increases coronary artery resistance even in the absence of focally obstructive stenosis [33] resulting in a base-to-apical longitudinal pressure gradient that affects myocardial tissue perfusion [34] and contributes to myocardial ischemia and symptoms. This may help to explain the presence of ischemic symptoms in patients without obstructive stenosis on coronary angiography [35,36,37,38,39].
Evaluation of Patients with Anomalous Coronary Arteries on CCTA
Case Vignette # 4
The patient was a 65-year-old female with a history of atrial fibrillation first detected in May 2018, a history of hypothyroidism and gastroesophageal reflux disease. An exercise treadmill test (ETT) at the time was equivocal due to ECG changes at peak exercise that resolved 1 min into recovery (Fig. 5). She exercised for 9 min of standard Bruce protocol (10.1 METs), reaching 160 beats per minute (103% of age-predicted maximal heart rate) with a blunted blood pressure response. The test was terminated for dyspnea and lightheadedness. She underwent successful cardioversion. However, she had recurrent atrial fibrillation 6 months later, prompting transesophageal echocardiogram-guided repeat cardioversion that proved only transiently successful. She then underwent gated cardiac CT for pulmonary vein mapping prior to ablation of atrial fibrillation. Incidentally, the CCTA (Fig. 6A) revealed an anomalous left coronary artery arising from the right coronary sinus with a subpulmonic, not intramural, course. There was no plaque or stenosis noted in the coronary CTA. She underwent exercise SPECT myocardial perfusion imaging, which showed normal myocardial perfusion and systolic function (Fig. 6B).

Baseline, peak stress, and recovery 12-lead ECGs in a patient with atrial fibrillation undergoing exercise treadmill testing. The rest ECG is notable for atrial fibrillation. At peak exercise, there is 1.5 horizontal ST segment depression in infero-lateral leads, which resolves 1 min into the recovery

Coronary computed tomography angiography (CCTA) and SPECT myocardial perfusion images in a patient with equivocal stress testing and atrial fibrillation. (A) The CCTA demonstrated an anomalous course of a long left main artery arising from the right sinus of Valsalva with a subpulmonic course. The yellow arrows are showing the course of the right and left coronary arteries. There was no plaque or stenosis. (B) The exercise-stress and rest SPECT myocardial perfusion images demonstrate normal regional myocardial perfusion. Stress-U, stress upright images; Stress-S, stress supine images
This case illustrates the role of radionuclide MPI to exclude objective evidence of ischemia in a patient with anomalous left coronary artery arising from the right sinus of Valsalva. Like in case vignette 4, most coronary anomalies are discovered as incidental findings on coronary CTA [40, 41]. The left coronary artery did not have any of the described malignant characteristics including an intramural course or slit-like long proximal narrowing [40, 41]. However, she did have an equivocal ETT study. Given the absence of angiographic high risk features, the normal exercise SPECT myocardial perfusion study was not unexpected. However, it was clinically reassuring. In cases where stress imaging is performed, it is important to use exercise (as opposed to pharmacologic) stress testing in an attempt to uncover phasic stenosis of the inter-arterial coronary segment [42].
Conclusions
It is likely that the expanded use of coronary CT angiography as a first-line test for CAD, as advocated by the NICE guidelines, will increase the need of stress imaging. Radionuclide myocardial perfusion imaging offers accurate quantitative assessment of myocardial ischemia, which helps with risk stratification and patient management especially the potential need for revascularization. SPECT and PET myocardial perfusion imaging have strengths and weaknesses that should be considered when selecting a test. Routine accurate quantifications of myocardial blood flow and flow reserve are major advantages of PET MPI, which are especially useful when used in patients at intermediate-high clinical risk.
Abbreviations
- MPI:
-
Myocardial perfusion imaging
- CAD:
-
Coronary artery disease
- SPECT:
-
Single-photon emission computed tomography
- PET:
-
Positron emission tomography
- CCTA:
-
Coronary computed tomography angiography
- MBF:
-
Myocardial blood flow
- MFR:
-
Myocardial flow reserve
- HTN:
-
Hypertension
- HLD:
-
Hyperlipidemia
- DM:
-
Diabetes mellitus
- ER:
-
Emergency department
- ECG:
-
Electrocardiogram
- hs-TnT:
-
High-sensitivity troponin T
- LCx:
-
Left circumflex
- LAD:
-
Left anterior descending
- RI:
-
Ramus intermedius
- METs:
-
Metabolic equivalents
- APMHR:
-
Age-predicted maximal heart rate
- BP:
-
Blood pressure
- ICA:
-
Invasive coronary angiogram
- LV:
-
Left ventricular
- RV:
-
Right ventricular
- CMD:
-
Coronary microvascular dysfunction
- CTO:
-
Chronic total occlusion
- PCI:
-
Percutaneous coronary intervention
- RCA:
-
Right coronary artery
- CABG:
-
Coronary artery bypass grafting
- CKD:
-
Chronic kidney disease
- LM:
-
Left main
- LIMA:
-
Left internal mammary artery
- SVG:
-
Saphenous venous graft
- RPDA:
-
Right posterior descending artery
- RPLV:
-
Right posterolateral vessel
- Afib:
-
Atrial fibrillation
- ETT:
-
Exercise treadmill test
- CV:
-
Cardioversion
- PHTN:
-
Pulmonary hypertension
- FFR:
-
Fractional flow reserve
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
Knuuti J, Wijns W, Saraste A, et al. 2019 ESC guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020;41(3):407–668.
Feher A, Sinusas AJ. Quantitative assessment of coronary microvascular function: dynamic single-photon emission computed tomography, positron emission tomography, ultrasound, computed tomography, and magnetic resonance imaging. Circ Cardiovasc Imaging. 2017;10(8):e006427. This review describes the key concepts of coronary and microvascular physiology, available modalities for dynamic imaging for quantitative assessment of coronary perfusion and myocardial blood flow, and discusses their application in distinct forms of coronary microvascular dysfunction.
Murthy VL, Di Carli MF. Non-invasive quantification of coronary vascular dysfunction for diagnosis and management of coronary artery disease. J Nucl Cardiol. 2012;19:1060–72 quiz 1075.
Hachamovitch R, Di Carli MF. Nuclear imaging and PET. In: de Lemos JAOT, editor. Chronic coronary artery disease: a companion to Braunwald’s heart disease. Philadelphia, PA: Elsevier Inc; 2018. p. 147–73.
Danad I, Uusitalo V, Kero T, Saraste A, Raijmakers PG, Lammertsma AA, et al. Quantitative assessment of myocardial perfusion in the detection of significant coronary artery disease: cutoff values and diagnostic accuracy of quantitative [(15)O]H2O PET imaging. J Am Coll Cardiol. 2014;64:1464–75.
Johnson NP, Gould KL. Physiological basis for angina and ST-segment change PET-verified thresholds of quantitative stress myocardial perfusion and coronary flow reserve. JACC Cardiovasc Imaging. 2011;4:990–8.
Kajander S, Joutsiniemi E, Saraste M, Pietilä M, Ukkonen H, Saraste A, et al. Cardiac positron emission tomography/computed tomography imaging accurately detects anatomically and functionally significant coronary artery disease. Circulation. 2010;122:603–13.
Naya M, Murthy VL, Taqueti VR, Foster CR, Klein J, Garber M, et al. Preserved coronary flow reserve effectively excludes high-risk coronary artery disease on angiography. J Nucl Med. 2014;55:248–55.
Ziadi MC, Dekemp RA, Williams K, Guo A, Renaud JM, Chow BJ, et al. Does quantification of myocardial flow reserve using rubidium-82 positron emission tomography facilitate detection of multivessel coronary artery disease? J Nucl Cardiol. 2012;19:670–80.
Fukushima K, Javadi MS, Higuchi T, Lautamäki R, Merrill J, Nekolla SG, et al. Prediction of short-term cardiovascular events using quantification of global myocardial flow reserve in patients referred for clinical 82Rb PET perfusion imaging. J Nucl Med. 2011;52:726–32.
Herzog BA, Husmann L, Valenta I, Gaemperli O, Siegrist PT, Tay FM, et al. Long-term prognostic value of 13N-ammonia myocardial perfusion positron emission tomography added value of coronary flow reserve. J Am Coll Cardiol. 2009;54:150–6.
Murthy VL, Naya M, Foster CR, Gaber M, Hainer J, Klein J, et al. Association between coronary vascular dysfunction and cardiac mortality in patients with and without diabetes mellitus. Circulation. 2012;126:1858–68.
Murthy VL, Naya M, Foster CR, Hainer J, Gaber M, di Carli G, et al. Improved cardiac risk assessment with noninvasive measures of coronary flow reserve. Circulation. 2011;124:2215–24.
Taqueti VR, Hachamovitch R, Murthy VL, Naya M, Foster CR, Hainer J, et al. Global coronary flow reserve is associated with adverse cardiovascular events independently of luminal angiographic severity and modifies the effect of early revascularization. Circulation. 2015;131:19–27.
Tio RA, Dabeshlim A, Siebelink HM, et al. Comparison between the prognostic value of left ventricular function and myocardial perfusion reserve in patients with ischemic heart disease. J Nucl Med. 2009;50:214–9.
Ziadi MC, Dekemp RA, Williams KA, Guo A, Chow BJ, Renaud JM, et al. Impaired myocardial flow reserve on rubidium-82 positron emission tomography imaging predicts adverse outcomes in patients assessed for myocardial ischemia. J Am Coll Cardiol. 2011;58:740–8.
Patel KK, Spertus JA, Chan PS, et al. Myocardial blood flow reserve assessed by positron emission tomography myocardial perfusion imaging identifies patients with a survival benefit from early revascularization. Eur Heart J. 2020;41(6):759–68.
Rana JS, Dunning A, Achenbach S, al-Mallah M, Budoff MJ, Cademartiri F, et al. Differences in prevalence, extent, severity, and prognosis of coronary artery disease among patients with and without diabetes undergoing coronary computed tomography angiography: results from 10,110 individuals from the CONFIRM (COronary CT Angiography EvaluatioN For Clinical Outcomes): an InteRnational Multicenter Registry. Diabetes Care. 2012;35:1787–94.
Muhlestein JB, Lappe DL, Lima JA, et al. Effect of screening for coronary artery disease using CT angiography on mortality and cardiac events in high-risk patients with diabetes: the FACTOR-64 randomized clinical trial. JAMA. 2014;312:2234–43.
Hulten E, Pickett C, Bittencourt MS, Villines TC, Petrillo S, di Carli MF, et al. Outcomes after coronary computed tomography angiography in the emergency department: a systematic review and meta-analysis of randomized, controlled trials. J Am Coll Cardiol. 2013;61:880–92.
Mc Ardle BA, Dowsley TF, deKemp RA, Wells GA, Beanlands RS. Does rubidium-82 PET have superior accuracy to SPECT perfusion imaging for the diagnosis of obstructive coronary disease? A systematic review and meta-analysis. J Am Coll Cardiol. 2012;60:1828–37.
Parker MW, Iskandar A, Limone B, Perugini A, Kim H, Jones C, et al. Diagnostic accuracy of cardiac positron emission tomography versus single photon emission computed tomography for coronary artery disease: a bivariate meta-analysis. Circ Cardiovasc Imaging. 2012;5:700–7.
Neglia D, Rovai D, Caselli C, et al. Detection of significant coronary artery disease by noninvasive anatomical and functional imaging. Circ Cardiovasc Imaging. 2015;8(3):e002179.
Takx RA, Blomberg BA, El Aidi H, et al. Diagnostic accuracy of stress myocardial perfusion imaging compared to invasive coronary angiography with fractional flow reserve meta-analysis. Circ Cardiovasc Imaging. 2015;8(1):e002666.
Danad I, Raijmakers PG, Driessen RS, Leipsic J, Raju R, Naoum C, et al. Comparison of coronary CT angiography, SPECT, PET, and hybrid imaging for diagnosis of ischemic heart disease determined by fractional flow reserve. JAMA Cardiol. 2017;2:1100–7.
Driessen RS, Danad I, Stuijfzand WJ, et al. Comparison of coronary computed tomography angiography, fractional flow reserve, and perfusion imaging for ischemia diagnosis. J Am Coll Cardiol. 2019;73:161–73 This study showed that FFR-CT had a higher diagnostic performance than standard coronary CTA, SPECT, and PET for vessel-specific ischemia, provided coronary CTA images were evaluable by FFR-CT; however, PET had a favorable performance in per-patient and intention-to-diagnose analysis.
Murthy VL, Naya M, Taqueti VR, Foster CR, Gaber M, Hainer J, et al. Effects of sex on coronary microvascular dysfunction and cardiac outcomes. Circulation. 2014;129:2518–27.
Taqueti VR, Shaw LJ, Cook NR, Murthy VL, Shah NR, Foster CR, et al. Excess cardiovascular risk in women relative to men referred for coronary angiography is associated with severely impaired coronary flow reserve, not obstructive disease. Circulation. 2017;135:566–77.
Galassi AR, Brilakis ES, Boukhris M, Tomasello SD, Sianos G, Karmpaliotis D, et al. Appropriateness of percutaneous revascularization of coronary chronic total occlusions: an overview. Eur Heart J. 2016;37:2692–700.
Khuddus MA, Pepine CJ, Handberg EM, Bairey Merz CN, Sopko G, Bavry AA, et al. An intravascular ultrasound analysis in women experiencing chest pain in the absence of obstructive coronary artery disease: a substudy from the National Heart, Lung and Blood Institute-Sponsored Women’s Ischemia Syndrome Evaluation (WISE). J Interv Cardiol. 2010;23:511–9.
Lee BK, Lim HS, Fearon WF, Yong AS, Yamada R, Tanaka S, et al. Invasive evaluation of patients with angina in the absence of obstructive coronary artery disease. Circulation. 2015;131:1054–60.
Taqueti VR, Di Carli MF. Coronary microvascular disease pathogenic mechanisms and therapeutic options: JACC state-of-the-art review. J Am Coll Cardiol. 2018;72:2625–41.
De Bruyne B, Hersbach F, Pijls NH, et al. Abnormal epicardial coronary resistance in patients with diffuse atherosclerosis but "Normal" coronary angiography. Circulation. 2001;104:2401–6.
Gould KL, Nakagawa Y, Nakagawa K, Sdringola S, Hess MJ, Haynie M, et al. Frequency and clinical implications of fluid dynamically significant diffuse coronary artery disease manifest as graded, longitudinal, base-to-apex myocardial perfusion abnormalities by noninvasive positron emission tomography. Circulation. 2000;101:1931–9.
Jespersen L, Hvelplund A, Abildstrom SZ, et al. Stable angina pectoris with no obstructive coronary artery disease is associated with increased risks of major adverse cardiovascular events. Eur Heart J. 2012;33:734–44.
Maddox TM, Stanislawski MA, Grunwald GK, Bradley SM, Ho PM, Tsai TT, et al. Nonobstructive coronary artery disease and risk of myocardial infarction. JAMA. 2014;312:1754–63.
Patel MR, Peterson ED, Dai D, Brennan JM, Redberg RF, Anderson HV, et al. Low diagnostic yield of elective coronary angiography. N Engl J Med. 2010;362:886–95.
Hoffmann U, Ferencik M, Udelson JE, Picard MH, Truong QA, Patel MR, et al. Prognostic value of noninvasive cardiovascular testing in patients with stable chest pain: insights from the PROMISE trial (Prospective Multicenter Imaging Study for Evaluation of chest pain). Circulation. 2017;135:2320–32.
Investigators S-H. CT coronary angiography in patients with suspected angina due to coronary heart disease (SCOT-HEART): an open-label, parallel-group, multicentre trial. Lancet. 2015;385:2383–91.
Angelini P, Uribe C. Anatomic spectrum of left coronary artery anomalies and associated mechanisms of coronary insufficiency. Catheter Cardiovasc Interv. 2018;92:313–21.
Cheezum MK, Ghoshhajra B, Bittencourt MS, Hulten EA, Bhatt A, Mousavi N, et al. Anomalous origin of the coronary artery arising from the opposite sinus: prevalence and outcomes in patients undergoing coronary CTA. Eur Heart J Cardiovasc Imaging. 2017;18:224–35.
Rigatelli G, Zuin M, Galasso P, et al. Mechanisms of myocardial ischemia inducing sudden cardiac death in athletes with anomalous coronary origin from the opposite sinus: insights from a computational fluid dynamic study. Cardiovasc Revasc Med. 2019;20(12):1112–6
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Vasvi Singh declares that she has no conflict of interest.
Marcelo F. Di Carli has research grants from Spectrum Dynamics and Gilead Sciences, and consulting fees from Bayer and Janssen.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Nuclear Cardiology
Rights and permissions
About this article

Cite this article
Singh, V., Di Carli, M.F. SPECT Versus PET Myocardial Perfusion Imaging in Patients with Equivocal CT. Curr Cardiol Rep 22, 43 (2020). https://doi.org/10.1007/s11886-020-01287-0
Published:
DOI: https://doi.org/10.1007/s11886-020-01287-0