
Abstract
Purpose of Review
Bladder outlet obstruction (BOO) encompasses the diagnosis of obstructive urinary flow accompanied by increased detrusor pressure. It can contribute to renal function deterioration, recurrent urinary tract infections, and potentially acute urine retention. While the diagnosis of BOO plays a critical role in clinical management and decision-making, a consensus on the precise evaluation remains elusive. This study aimed to comprehensively review non-invasive methods for diagnosing BOO, primarily in cases related to benign prostatic hyperplasia.
Recent Findings
A systematic literature review was conducted on PubMed from January 2016 to November 2022, focusing on non-invasive tests and lower urinary tract symptoms (LUTS) or bladder outlet obstruction (BOO) in men. A total of 2520 results were included, resulting in 1620 unique findings after removing duplicates. From these, 263 abstracts were thoroughly evaluated, leading to a detailed review of 80 full-text articles and their references. The review identified numerous cutting-edge technologies, primarily ultrasound-based, such as intravesical prostatic protrusion (IPP), bladder wall thickness (BWT), and detrusor wall thickness (DWT), among others. These advancements demonstrate promising sensitivity and specificity, positioning them as valuable tools for evaluating patients with BOO.
Summary
Achieving an accurate diagnosis and implementing effective management strategies for BOO patients can lead to improved patient care, optimized resource allocation for those in need, and significant reductions in unnecessary expenditures. In the near future, a plethora of additional tools will become available, poised to enhance our diagnostic and prognostic approaches for patients with BOO.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Lower urinary tract symptoms (LUTS) refer to a group of symptoms related to the urinary system that occur in the lower part of the urinary tract, which includes the bladder, urethra, and prostate. The prevalence of LUTS is estimated to affect a quarter of men in their 6th decade [1] and up to 70% of men in their 9th decade [2], although the prevalence of LUTS can vary widely depending on the specific symptoms considered and the definition of LUTS used in a particular study [3].
The symptoms are classically divided into voiding symptoms and storage symptoms depending on the abnormality in the urinary cycle phase, though overlap between them is common [4•]. Voiding symptoms include slow-stream, hesitancy, intermittency, and straining, while storage symptoms include urgency, frequency, nocturia, and urge incontinence. These symptoms have a great impact on quality of life, associated with various health conditions [5, 6] and bear substantial economic burden [7].
Bladder outlet obstruction (BOO) refers to the diagnosis of obstruction and is defined as “reduced urine flow rate with a simultaneously increased detrusor pressure” [4•]. BOO may be a factor that can result in the deterioration of renal function [8•], recurrent urinary tract infections (UTI), and acute urine retention (AUR) [9], and these can be life-threatening [10].
While BOO can result in bladder dysfunction [11,12,13], the exact mechanism, the relation to symptoms, and the clinical course are unclear. While the diagnosis of BOO has a pivotal role in clinical management and decision-making [14, 15•], there is no consensus on the exact evaluation required.
In this review, we will focus on the non-invasive methods to diagnose BOO, concentrating on benign prostatic hyperplasia [16]. We will review the currently studied alternatives to the commonly used invasive tests. Urodynamic study (UDS) with the pressure-flow study (PFS) component is currently the gold standard for diagnosing BOO, and specifically differentiating voiding symptoms resulting from BOO or from detrusor underactivity (DU) [4•, 17••].
However, UDS is invasive, expensive, and bothersome [18, 19•] and bears several risks, namely infection [20, 21] and hematuria [22]. Moreover, UDS has several diagnostic drawbacks including suboptimal specificity [23, 24] and sensitivity [25, 26, 27•, 28] and inter-rater variability [29, 30], among others [17••, 31••, 32••]. These disadvantages led to a growing need to establish valid and reliable non-invasive tools to diagnose BOO.
Another invasive alternative is urethrocystoscopy, which can point out structural or anatomical BOO-related bladder wall trabeculations and diverticula [33, 34]. However, the correlation between urethrocystoscopy finding and symptoms is suboptimal and BOO maybe present in 15% of patients with normal cystoscopy finding, and therefore is not recommended to replace UDS in the evaluation of BOO, though it has a place if it may change management prior to minimal invasive BPH interventions [17••].
Literature Review
Methodology
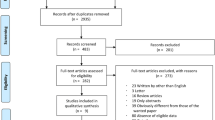
A systematic literature review was conducted on PubMed between January 2016 and November 2022, using a set of specific terms related to non-invasive tests and phrases relevant to LUTS or BOO in men, as outlined in the supplementary materials. Searches were conducted for general terms as well as for specific tests or test groups, few key manuscripts that were essential for specific topics, and manuscripts referred by the key studies yielding a total of 2520 results. After removing duplicates, 1620 unique results were obtained, of which 263 abstracts were reviewed. A total of 80 full-text articles were thoroughly reviewed, including the relevant references, as depicted in Fig. 1.

Flow diagram of the evidence acquisition in this systematic review on non-invasive methods to diagnose bladder outlet obstruction
Following that, we reviewed the current American Urological Association (AUA) and European Association of Urology (EAU) guidelines and commented accordingly on each test, if it was available.
Aim of the Study
The primary aim of this review is to provide a comprehensive analysis of the current literature pertaining to non-invasive methodologies for assessing BOO. In doing so, we will scrutinize the efficacy and benefits of various techniques and methods that have been employed for this purpose. Moreover, we will undertake a thorough evaluation of the diagnostic and prognostic value of these modalities, taking into consideration the varying conditions and scenarios that may influence their utility.
Value of diagnostic steps in the evaluation of voiding LUTS- systematic review
Medical History
The objective of a medical history assessment is to identify possible causes and relevant comorbidities, which includes an evaluation of symptoms; sexual history; past medical history and procedures; history of trauma to the perineum, genitalia, or spine; neurological comorbidities; medication usage; and psychological and emotional factors. Severity of BOO-related symptoms among other LUTS can be assessed using the International Prostate Symptom Score (IPSS) questionnaire, which is commonly used in these settings. The severity of LUTS may be simplified to three grade scales as mild (< 7), moderate [8•, 9,10,11,12,13,14, 15•, 16, 17••, 18, 19•], or severe (≥ 20) LUTS, based on the total IPSS score. Additional question assesses the impact of symptoms on quality of life (QOL) which is pivotal in assessing patient’s level of bother. The IPSS score is useful for initial assessment and also for monitoring LUTS during follow-up. Several studies have found that symptom severity is not well-correlated with or is not an independent indicator of obstruction [25, 26, 27•, 28, 35•, 36], but may indicate the prognosis and the response for some treatments [9, 37,38,39,40]. Systematic reviews (SR) [41•] have also demonstrated poor correlations between IPSS scores and BOO grades. Although some new nomograms [42•, 43•] have shown that IPSS can contribute to models of BOO-prediction, they are not yet widely used.
The latest guidelines recommend incorporating the use of a reliable questionnaire that is valid for LUTS estimation and follow-up, and in our view, it is worthwhile to use IPSS in daily practice.
The assessment of males presenting with LUTS requires a comprehensive physical examination that constitutes an essential component of the diagnostic process. This evaluation usually involves an examination of the suprapubic region to detect significant urinary retention or the existence of a palpable bladder. Additionally, a thorough assessment of the external genitalia and perineum is necessary to identify any indications of urethral stricture, fibrosis, or cutaneous findings suggestive of various pathologies. These pathologies may include lichen sclerosis, sexually transmitted infections, or neoplastic changes, all of which may manifest as BOO if resulted in urethral stricture.
Furthermore, digital rectal examination (DRE) should be routinely performed to assess rectal tone and detect any suspicious nodules in the prostate gland that may indicate prostate cancer (PCa) while excluding acute prostatitis. Although lacking in accuracy [44,45,46,47,48] in determining the prostate size and the cause of BOO, DRE may provide a crude estimation of prostate volume [49, 50•] and raise suspicions for significant pathology requiring further workup. Notably, the EAU and the AUA both recommend a physical examination for the evaluation of men BOO. However, the EAU guidelines additionally suggest a DRE as part of the physical examination, whereas the AUA guidelines do not explicitly include it in their recommendations [17••, 32••].
Uroflowmetry (UF)
Uroflowmetry is a test that is non-invasive and straightforward in its application, assessing the rate and volume of urine flow during urination. The occurrence of BOO may result in a slow urine flow, which is evidenced by a lower maximal flow rate (Qmax). While some researches have suggested that a high Qmax threshold of 15 mL/sec with 99% sensitivity and a negative predictive value (NPV) of 97% be used to rule out BOO [51], others have suggested a cutoff of 10 mL/sec [52, 53•, 54••]. Qmax has been widely incorporated as a component of UDS nomograms, such as the bladder outlet obstruction index (BOOI) and the bladder contractility index (BCI) [55, 56]. However, the use of Qmax to predict BOO is limited due to the variability of the studies’ results [42•, 43•, 52, 53•, 57, 58•].
A lower Qmax has been shown to be associated with higher IPSS [59, 60], onset of new LUTS [61], AUR [9], and a higher success rate in obstruction-relieving surgeries, mainly Holmium laser enucleation of the prostate (HoLEP) [62•] and transurethral resection of the prostate (TURP) [40]. Additionally, several studies have found that lower Qmax is correlated with a higher need for surgical intervention [39, 63•], while others have contradicted this association [64]. It should be noted that low Qmax is not specific to BOO, as DU or poor relaxation of the urinary sphincter may also impede urine flow [65•, 66].
Of note, several studies utilize the graph form of the UF to differentiate BOO from DU. As such, some shapes of the uroflowmetry graph may suggest DU rather than BOO [67, 68]. Some models utilize different parameters of UF to accurately calculate the probability of BOO [69, 70]. A novel method of standardization of volume-corrected Qmax has been investigated as a better predictor of surgery outcome [71].
Given its non-invasive nature, simplicity, and acceptable NPV, UF has a role in the initial evaluation and disease monitoring, particularly in repeated exams over a long follow-up period. The guidelines of the EAU recommend uroflowmetry in the initial assessment, and the AUA keeps it as an optional test. However, both associations strongly recommend it prior to surgical intervention [17••, 32••].
Post-voiding Residual (PVR)
Post void residual (PVR) volume denotes the quantity of urine that remains in the bladder subsequent to voiding. Ordinarily, after micturition, the bladder is expected to be voided completely or contain a negligible residual volume of urine. Chronic urinary retention, as measured by physical examination, or ultrasound (US) using a cutoff of 300 mL in two 6-months-apart measurement is a suggestion by consensus by the AUA guidelines [72•].
The correlation of PVR and the cutoffs used changed very widely from being non-predictive, while others showed predictive value and accuracy of 0.8 [51, 53•, 73, 74].
Elevated PVR (ePVR) in the presence of BOO may have an important role in predicting the coming clinical course. Several investigators reported a higher rate of disease progression to medication or surgical intervention with a higher PVR [39, 63•, 75•]. Additionally, studies found that PVR is associated with complications of BOO, like recurrent UTI [76], progression of symptoms [77], AUR [63•, 77,78,79], bladder calculi, and renal failure [79]; however, the robustness of the evidence should be better before determining the causality of these factors to BOO complications.
AUA guidelines summarize that PVR does not seem to be a strong predictor of complication in the absence of other high-risk features [32••]. However, EAU guidelines recommend measuring PVR as part of the initial assessment, and the AUA supports including it as an optional test, with more emphasis on following the PVR trend over time, and as a recommended test prior to surgical intervention [17••, 32••].
Laboratory Workup
Prostate-Specific Antigen (PSA) Test
Prostate-specific antigen (PSA) is a protein that is synthesized by the epithelial cells of the prostate gland. While it is primarily used as a biomarker for PCa screening and monitoring, elevated levels of PSA can also indicate other prostate-related conditions, such as prostatitis, benign prostatic hyperplasia (BPH) [80, 81], and UTI [82].
Several studies have demonstrated that PSA levels are well-correlated with prostate volume (PV). For instance, Roehrborn et al. [83] showed that in BPH trials involving 4448 patients, the area under the curve (AUC) for PSA levels (adjusted for age) was 0.76–0.78, with a specificity and sensitivity of 70% for prostate volumes of 30, 40, and 50 mL cutoff. Another study [84] confirmed that PSA levels can predict PV with an accuracy of ± 20% for over 90% of patients. Furthermore, PSA has been found to be a predictor for male LUTS [85]. It has also been shown to correlate with the natural progression of BPH, including future prostate growth [86], worsening symptoms [87], progression to the need for escalating therapy [39], risk of AUR [88, 89], and BPH-related surgery [88]. However, these findings were challenged by Kim et al. [64], who found no correlation between PSA levels and the need for BPH-related surgery among 679 patients.
Higher PSA levels (> 1.4 ng/mL) have also been shown to predict response to 5-alpha-reductase inhibitors (5-ARIs) [90], and this has been incorporated as one of the factors to consider when deciding whether or not to initiate 5-ARI therapy in men with LUTS, according to the AUA guidelines [32••]. While PSA is not recommended as part of the assessment of BOO, it can aid in differential diagnosis and treatment decision-making. However, the use of PSA testing as a part of shared decision-making with the patient remains controversial, as it has been extensively debated in the context of early detection of prostate cancer [91,92,93].
Renal Function
The presence of BOO may result in the retrograde flow of urine into the kidneys, culminating in the development of obstructive uropathy and potentially leading to the insidious onset of renal failure [8•, 94, 95]. In addition to the initial measure of bladder decompression via catheterization, alleviation of the obstruction through interventions such as TURP has been proposed as a means to potentially restore or stabilize kidney function, as evidenced by findings from Lee [96]. While some dispute the strength of this correlation [97], the cost-effectiveness and accessibility of kidney function testing warrant its inclusion as an initial diagnostic step, which may also serve to exclude alternative etiologies. Although renal failure is a belated consequence of BOO and may not manifest in the initial assessment, both the AUA and EAU recommend its use as a baseline test and as a means of monitoring progression over time [17••, 32••].
Urinalysis (UA)
Despite its widespread use as a screening tool for medically important conditions (MIC), a recent study [98•] evaluating the efficacy of urinalysis (UA) for diagnosing these conditions among data obtained from three studies comprising 2894 men found that it was only effective in detecting UTI and diabetes mellitus (DM). However, for these conditions, more sophisticated diagnostic methods, such as urine culture for suspected UTI and glucose blood testing for DM, are available. Moreover, its utility to diagnose UTI was questioned by Khasriya et al. [99]. Despite the limited utility of UA, its low cost, availability, and non-invasive nature have led to its adoption as a routine diagnostic test, which has garnered strong endorsement from leading associations [17••, 32••] and is widely accepted in clinical practice [100].
Prostate Volume (PV)
Prostate volume (PV) is a term that pertains to the size of the prostate gland, which may become enlarged and cause BOO. The conventional methods for PV measurement include transrectal ultrasound (TRUS) and trans-abdominal ultrasound (TAUS), while cystoscopy or cross-sectional imaging techniques such as computed tomography (CT) or magnetic resonance imaging (MRI) are less commonly employed for that purpose [17••, 101]. Of the available methods, TRUS and MRI are deemed the most accurate for PV measurement [41•, 102,103,104].
Despite some debate concerning the correlation between PV and BOO, several studies have indicated moderate association between the two, with larger prostates being linked to an increased likelihood of BOO and its associated symptoms as well as obstructive urodynamic findings [27•, 43•, 75•, 105•]. However, although the applicability of PV to predict may raise an AUC of between 0.6 and 0.7 according to many studies [51, 106,107,108], the cutoff changes widely and so do the PPV and NPV [41•, 58•]. Additionally, there is low to no association between PV and validated symptoms questionnaire [109, 110•, 111, 112]. A recent meta-analysis involving 2767 men demonstrated that a threshold of 40-mL size prostate had an AUC of 0.68, although sensitivity and specificity were limited (0.54 and 0.76, respectively) [54••]. Furthermore,larger PV was associated with a threefold risk for progression to AUR [9], a heightened (OR = 2.48) risk for disease progression [113•], with better response to 5-ARI [114, 115•, 116], and to TURP [40] but not for response to alpha-blockers [117, 118, 119•, 120].
It is imperative to acknowledge, however, that the correlation between PV and BOO is influenced by various factors, including age, hormonal changes, and other medical conditions [121,122,123].
According to the latest guidelines from the EAU, while imaging prior to medication is suggested as a supportive measure, prostate imaging prior to intervention is strongly recommended by the EAU and considered by the AUA [17••, 32••]. This recommendation is aimed at facilitating the selection of an appropriate intervention [32••], as well as aiding in the preparation of the operative room and staff from a technical standpoint.
Intravesical Prostatic Protrusion (IPP)
Intravesical prostatic protrusion (IPP) is a metric used to evaluate the proximity between the median lobe of the prostate and the bladder neck along the midsagittal plane. This assessment is generally conducted using a suprapubically positioned US scanner, and it is classified into three grades based on the extent of protrusion: grade I (0–4.9 mm), grade II (5–10 mm), and grade III (> 10 mm) [17••]. In contrast to PV, which measures the size of the prostate, IPP assesses the configuration of the prostate and the presence of the median lobe, which can result in obstruction even in small prostates through a ball-valve mechanism [32••, 124].
The accuracy of IPP in detecting BOO has been demonstrated, even in patients with normal flow (hence Qmax ≥ 12) [125•], displaying a remarkably high (100%) NPV to rule out BOO while using grade II as a cutoff, and a reasonable specificity (76.6%) for grade III [125•]. Several studies have investigated the correlation between IPP and the BOO index measured in UDS, with correlation coefficients ranging from 0.21 to 0.67 [107, 108, 126,127,128]—higher than PV. The AUC of predicting BOO with an IPP > 10 mm ranges between 0.71 and 0.885 [106, 107, 129]. Other investigators have used varying cutoffs, ranging from 5 to 12 mm, with AUC values ranging from 0.76 to 0.905 [105•, 108, 130, 131]. While a SR of 1013 cases revealed a pooled PPV of 73.8% and NPV of 69.3% [58•], other SRs reported AUC ranging from 0.7 to 0.86 [41•, 132•, 133], and the most big and recent meta-analysis including 2136 cases found AUC of 0.83 [54••]. Whether IPP correlates with symptom severity is a subject to controversy and the results of studies that examined this question vary widely from good to no correlation [27•, 120, 128, 134,135,136,137].
Moreover, IPP had shown to be predictive of BOO outcome. Numerous studies have indicated that higher grades of IPP are correlated with negative outcomes of conservative management, including watchful waiting, alpha-blockers [32••, 119•, 120, 130, 138, 139•, 140, 141], 5ARI [142•], and oral combination therapy [142•, 143].
IPP has exhibited the potential to serve as a prognostic indicator for an elevated probability of advancing to TURP [143], along with a heightened susceptibility to AUR [126], failure to void following AUR [132•, 144, 145], and overall higher probability of disease progression [113•, 146]. Additionally, it is supported by empirical evidence that an elevated IPP parameter is positively associated with superior post-operative outcomes subsequent to surgical interventions targeted at relieving BOO, including HoLEP when contrasted with matched cohorts possessing a smaller IPP parameter [62•] and TURP [147•].
Despite the promising potential of IPP in both diagnosis and prognosis, the optimal cutoff has yet to be determined. Presently, the EAU does not incorporate IPP into its evaluations due to insufficient evidence regarding its reliability and possible learning curves [17••]. The AUA advises considering abdominal ultrasonography before surgical intervention or reevaluating patients in the event of treatment failure; however, there is no explicit requirement of including IPP in the prostate imaging in the initial evaluation of BOO [32••].
Bladder Wall Thickness (BWT) and Detrusor Wall Thickness (DWT)
Bladder wall thickness (BWT) and detrusor wall thickness (DWT) are two measurements used to evaluate the health of the bladder wall, commonly obtained through trans-abdominal ultrasound. BWT and DWT can be thickened pathologically due to prolonged BOO, or thinned in atonic bladder [148]. While BWT measures the entire bladder wall, DWT refers specifically to the thickness of the muscular layer [17••]. Several studies [36, 130, 149, 150] have examined the predictive value of BWT and have shown an area under the curve (AUC) of 0.67–0.94 when using different cutoffs of 3.2/3.7/5 mm, with specificity to diagnose BOO exceeding 90% according to most studies. However, the contribution of BWT in predicting BOO in multivariate analysis, particularly when QMAX is added, is currently debated [36, 149, 151]. Nevertheless, high BWT has shown a poor response to alpha-blocker treatment [130, 152] and TURP surgery [147•].
Detrusor wall thickness (DWT) has emerged as a potentially more precise indicator of BOO compared to BWT. This distinction is attributed to the pivotal role of ultrastructural changes in muscle and connective tissue within the pathophysiology of BOO [153, 154]. Multiple investigations have yielded encouraging results, reporting DWT to have an area under the curve (AUC) ranging from 0.78 to 0.88 [51, 106, 108, 155, 156], accompanied by a notable degree of specificity. In a recent meta-analysis encompassing 1003 patients, DWT demonstrated an AUC of 0.87, exhibiting a sensitivity of 71% and a specificity of 89%. Furthermore, when adopting the widely utilized cutoff of 2 mm, the AUC increased to 0.9, with a sensitivity of 79% and a specificity of 89% [54••].
However, despite the potential importance of BWT and DWT in the pathological pathway of BOO, their usefulness is currently limited due to the lack of standardization of measurements, thresholds, and the operator-dependency of their assessment. Consequently, leading guidelines do not include these measurements in BOO evaluations [17••, 32••]. Therefore, further studies are needed to investigate their clinical utility and establish standardized protocols for their assessment.
Upper Urinary Tract Imaging
Upper tract imaging pertains to the utilization of diagnostic imaging techniques in assessing the upper urinary tract, encompassing the kidneys and ureters, in situations where BOO is suspected. This obstruction may bring about an accumulation of pressure within the bladder, leading to hydroureteronephrosis and consequential renal damage [95]. Common imaging modalities employed for upper tract imaging comprise TAUS [17••], whereas CT and MRI are seldom conducted for BOO diagnosis, but rather to rule out other medical conditions. Nonetheless, in the absence of accompanying indications such as urinary retention or indications of renal failure, hydroureteronephrosis is infrequently observable during the initial presentation of BOO [157,158,159]. Nevertheless, the EAU advocates for the use of upper tract imaging, while the AUA does not include it in the evaluation of index patients with BOO [17••, 32••]. It is important to note that in a patient with chronic urinary retention, the AUA recommends the utilization of upper tract imaging for diagnosis and monitoring of the disease state [160].
The Utility of Other US Measurements to Diagnose BOO
Ultrasound Estimated Bladder Weight (UEBW)
Ultrasound estimated bladder weight (UEBW) is a technique that employs trans-abdominal ultrasound to estimate the weight of the bladder, leveraging the physiologic principle of BWT by multiplying the volume of the bladder wall by the specific gravity of bladder tissue [161, 162]. Unlike BWT, which assesses a specific part of the bladder, UEBW provides a comprehensive assessment of the entire bladder and therefore may add an advantage.
Several studies have endeavored to investigate the diagnostic and prognostic value of UEBW. While various investigations have posited the potential of UEBW to forecast BOO with an AUC ranging from 0.6 to 0.85 [130, 161, 163], the limited quantity of research and participants, coupled with diverse cutoff values, and conflicting findings, precludes a conclusive determination regarding its clinical applicability [41•, 58•, 164].
UEBW has been modestly positively correlated with the IPSS (r = 0.28), and after prostatectomy, it significantly decreases [162, 165]. Furthermore, UEBW is an identified predictor of alpha-blocker treatment’s inefficacy in a 157-participant study [130]. Additional studies [166, 167] have investigated the potential of UEBW in predicting AUR, with one study [166] reporting that individuals with a heavier bladder had a 13.4-fold increased risk of AUR. Nonetheless, these preliminary findings are yet to achieve standardization, and the predictive power of UEBW remains unclear.
Presently, the EAU and the AUA guidelines do not recommend UEBW’s inclusion in the initial approach or follow-up of BOO patients [17••, 32••].
Measurements of the Prostate Zone: Volume or Index of the Transitional Zone
The measurement of the transitional zone volume (TZV) is indicative of the quantity of prostate tissue present in the area surrounding the urethra. As BPH is known to result in an increase in the size of the transitional zone, the measurement of TZV and its proportion relative to the entire prostate gland (referred to as the transitional zone index (TZI)) may serve as a surrogate marker for BOO [168]. Two large-scale studies found transition zone indices to be good independent predictors in multivariate analysis and included them in a BOO predicting nomogram [36, 43•]. Certain studies have demonstrated that TZV was associated with higher IPSS [169, 170], while others did not [171, 172]. Moreover, TZV can predict acute AUR, with an AUC of 0.74 [78], and likewise, a higher TZI (AUC of 0.775–0.860) showed similar results [78, 89]. Additionally, Qian et al. examined 1038 patients and discovered that disease progression was associated with TZV > 15 mL and TZI > 0.5, with odds ratios of 1.68 and 1.89, respectively [113•]. Other studies have shown that TZI is a predictor of a more favorable response to 5-ARI add-on therapy, with an AUC of 0.71 [116, 173•] and medical combination therapy [174], and that TZI correlated with better response to TURP [40, 175]. Despite these promising preliminary findings, further research is needed before TZV and TZI can be recommended for routine use. The EAU and AUA have yet to incorporate these indices into their BOO index for patient workup [17••, 32••].
Measurement of Resistive Index in the Capsular Arteries
The resistive index (RI) is a measurement of resistance within the prostate capsular arteries. It is calculated by assessing the changes in blood velocity measured through TRUS, specifically peak systolic velocity minus end diastolic velocity divided by peak systolic velocity. Studies have shown that high RI values are associated with BPH and are believed to be due to prostate enlargement, which can compress the capsular arteries against the capsule, thereby increasing resistance.
For instance, several studies have reported RI values predicting BOO with varying thresholds, sensitivities, and specificities, with AUC values ranging from 0.785 to 0.82 [57, 105•, 176], and accuracy of 83.8–86% [177, 178]. Furthermore, RI values have also been found to correlate with the BOOI in multivariate analysis [105•, 179]. However, different investigators reported conflicting results regarding RI correlation with IPSS [180, 181].
Interventions aimed at relieving BOO, such as TURP, have been shown to decrease RI values [163]. In addition, higher baseline RI values have been associated with better outcomes of transurethral resection of the prostate after 12 months, with an AUC of 0.845 and a PPV of 85.1% [40], and a predictor of AUR, with AUC of 0.867 [78].
However, RI has limitations as every cause of endothelial dysfunction may impair vascular compliance and increase RI, such as atherosclerosis and DM [182].
Moreover, it should be noted that the RI is operator dependent and lacks a universally accepted reference point, thereby limiting its applicability across different settings. In light of this, additional research is required to determine the efficacy of RI as a straightforward prognostic tool for both clinical outcomes and BOO, and the AUA and the EAU currently do not recommend the use of RI [17••, 32••].
Urethral Measurements: Prostatic Urethral Angle (PUA)
Several measurements related to the urethra and its positioning in relation to the urinary bladder were meticulously scrutinized. Of particular interest was the acute angle of the prostatic urethra, as it has been postulated to elicit resistance and impede urine flow. Researchers have delved into the role of the prostatic urethral angle (PUA) in BOO, and it was observed that higher PUA was associated with more pronounced symptoms as assessed by the IPSS [136, 137, 183, 184•], with lower Qmax [136], and with BOOI as determined by urodynamic studies, even when IPP was controlled [183]. Higher PUA was also correlated with poor improvement after alpha-blocker treatment with an AUC of 0.65 [184•]. While the PUA measurement is relatively easy to employ, circumvents a learning curve, and enables seamless comparison between operators, its utility is yet to be fully established in BOO. It is plausible that with further investigation, the PUA measurement may become more widely utilized and prove valuable in predicting BOO. In addition, various other ultrasonographic measurements are currently under scrutiny, and more compelling evidence is likely to surface in the foreseeable future.
Near-Infrared Spectroscopy (NIRS)
In the realm of urology, a cutting-edge method for monitoring tissue oxygenation and hemodynamics is near-infrared spectroscopy (NIRS). By detecting changes in the concentrations of oxyhemoglobin (O2Hb) and deoxyhemoglobin (HHb), NIRS can provide a non-invasive optical approach to observe these indicators [185]. In light of this, Macnab and colleagues postulated that during voiding, the thickened detrusor would consume oxygen and subsequently reduce its concentration, thereby enabling differentiation between BOO and DU [186]. Despite the potential of NIRS to estimate the presence of obstruction, there is still a scarcity of studies that employ NIRS as part of an algorithm. Some research groups reported highly encouraging results with a sensitivity of 86%, specificity of 88%, and 94% precision, with an AUC of 0.91 [185, 187, 188]. Conversely, other studies reported much lower values, with a sensitivity and specificity of 68.3% and 62.5%, respectively [189], and an AUC of 0.484 [190]. In a SR conducted by Malde and colleagues, the median sensitivity and specificity were determined to be 85.7% and 87.5%, respectively [58•]. It is important to note, however, that most of these studies are relatively small-scale and did not predict prognosis or treatment outcomes. Additionally, the utilization of NIRS in clinical practice is impeded by the need for specialized equipment and personnel with extensive training, which could limit its routine application. As a result, leading urology associations do not recommend the routine use of NIRS in the evaluation of bladder dysfunction [17••, 32••].
Non-invasive UDS: Penile Cuff Test
The penile cuff test (PCT) aims to achieve the maximum detrusor pressure without requiring catheter insertion. This is accomplished by inflating a cuff around the penis to interrupt the flow, equalizing the internal pressure of the cuff with the isovolumetric pressure of the detrusor [191]. The PCT is a simple, painless, and rapid test [19•] with low inter-observer variability [192], making it an attractive alternative to UDS.
Earlier efforts to diagnose BOO using the PCT had modest results with a PPV of 68% and a NPV of 78% although the addition of the criterion of Qmax < 10 mL/sec improved its accuracy [193]. Subsequent studies have found high sensitivity (NPV = 88–100%), making the PCT a good test for ruling out patients without BOO [19•, 194, 195]. Moreover, a recent meta-analysis involving 806 patients found an AUC of 0.88, a sensitivity of 87%, and a specificity of 78% [54••].
One significant drawback of the PCT is the inability to distinguish between abdominal pressure and detrusor pressure, which is a pivotal factor in UDS in differentiating DU from BOO [196]. In conclusion, the current evidence may support the use of the PCT as an adjunct tool and provide important insights into BOO. However, the evidence is still preliminary for utilizing the PCT as a full substitute for UDS, and leading associations have yet to include it in their assessment recommendations [17••, 32••].
Nomogram Models in Predicting BOO
To seek an alternative to urodynamic testing, one approach is to utilize nomogram models incorporating known and novel risk factors correlated with BOO. A plethora of researchers have proposed diverse models for prognosticating varied outcomes of BOO and predicting treatment outcome.
For the purpose of predicting BOO, Lee et al. (2019) employed a sizeable cohort of 750 medication-refractory individuals to develop a nomogram predicated on age, IPSS, Qmax, prostate volume, and TZI, achieving an AUC of 0.88 for BOO, as well as an AUC of 0.81 on a distinct validation set [43•].
Ganpule (2021) constructed a nomogram predicated on IPSS, PSA, Qmax, PV, and IPP, designed to predict the necessity for surgical intervention. The model demonstrated a sensitivity of 88.24%, specificity of 97.33%, and accuracy of 95.65% [197•].
Furthermore, Tian et al. (2022) developed the PROSTATE nomogram, based on a sample of 356 individuals, using age, IPSS, IPP, BWT, peripheral zone thickness, and transitional zone thickness as predictors, with a PPV of 90.6% and NPV of 43.7% for predicting the efficacy of TURP. The trained model exhibited an AUC of 0.86 [147•].
However, a notable drawback of these studies lies in the absence of standardization, particularly concerning the test population, such as individuals with optimal urinary flow, treatment-resistant symptoms, and varying age demographics, among other factors. Moreover, these nomogram models lack external validation studies involving divergent population groups, impeding the generalization of results to all BOO patients. Currently, these models were not implemented by the AUA and EAU guidelines committees [17••, 32••].
Future Directions
The pressing challenge facing physicians today is the need for a precise diagnostic tool that is non-invasive, user-friendly, and effective in identifying obstruction of the urinary bladder outlet. Various avenues for the future are being explored, such as blood or urine markers, wearable technologies, and even in the realms of genetics or genomics. While in other areas of medicine, including urology, these research endeavors are well-established and advanced, no single test has yet been identified to bridge this gap. As BOO is a multifactorial disease that relies on clinical diagnosis, along with the incorporation of diverse metrics, the challenge falls to the clinical judgment of the treating physician.
We anticipate that in the near future, a range of diverse technologies and tests will emerge that will provide a suitable response to the current deficiency in the field.
Conclusions
Bladder outlet obstruction (BOO) represents a frequently encountered phenomenon, exhibiting a wide array of manifestations that span from asymptomatic occurrences to potentially life-threatening comorbidities. Attaining precise diagnosis and implementing effective management strategies for patients afflicted by BOO can yield enhanced standards of patient care, optimized allocation of resources for those in need, and substantial reductions in superfluous expenditures. Within this study, we undertook an extensive examination of the available literature concerning non-invasive diagnostic modalities for BOO, thereby offering treating physicians a valuable instrument to inform their medical decision-making process.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Egan KB. The epidemiology of benign prostatic hyperplasia associated with lower urinary tract symptoms. Urol Clin N Am. 2016;43(3):289–97.
Parsons JK, Bergstrom J, Silberstein J, Barrett-Connor E. Prevalence and characteristics of lower urinary tract symptoms in men aged ≥80 years. Urology. 2008;72(2):318–21.
Solvang M, Elnegaard S, Jarbøl DE. Urological symptoms among 23,240 men in the general danish population - concerns about symptoms, their persistence and influence on primary care contacts. Scand J Prim Health Care. 2018;36(3):227–36.
D’Ancona C, Haylen B, Oelke M, Abranches-Monteiro L, Arnold E, Goldman H, et al. The International Continence Society (ICS) report on the terminology for adult male lower urinary tract and pelvic floor symptoms and dysfunction. Neurourol Urodyn. 2019;38(2):433–77. Include the comprehensive and updated report that defined the subjective and objective pathologies used to this study and their criteria.
Taylor BC, Wilt TJ, Fink HA, Lambert LC, Marshall LM, Hoffman AR, et al. Prevalence, severity, and health correlates of lower urinary tract symptoms among older men: the MrOS study. Urology. 2006;68(4):804–9.
Wong SYS, Hong A, Leung J, Kwok T, Leung PC, Woo J. Lower urinary tract symptoms and depressive symptoms in elderly men. J Affect Disord. 2006;96(1):83–8.
Wei JT, Calhoun E, Jacobsen SJ. Urologic diseases in america project: benign prostatic hyperplasia. J Urol. 2005;173(4):1256–61.
Rule AD, Jacobson DJ, Roberts RO, Girman CJ, McGree ME, Lieber MM, et al. The association between benign prostatic hyperplasia and chronic kidney disease in community-dwelling men. Kidney Int. 2005;67(6):2376–82. This is the most comprehensive and updated study to examine the consequences of BOO and LUTS regarding to kidney damage.
Jacobsen SJ, Jacobson DJ, Girman CJ, Roberts RO, Rhodes T, Guess HA, et al. Natural history of prostatism: risk factors for acute urinary retention. J Urol. 1997;158(2):481–7.
Armitage JN, Sibanda N, Cathcart PJ, Emberton M, van der Meulen JHP. Mortality in men admitted to hospital with acute urinary retention: database analysis. BMJ. 2007;335(7631):1199–202.
Wadie BS, Ebrahim EHE, Gomha MA. The relationship of detrusor instability and symptoms with objective parameters used for diagnosing bladder outlet obstruction: a prospective study. J Urol. 2002;168(1):132–4.
Oelke M, Baard J, Wijkstra H, de la Rosette JJ, Jonas U, Höfner K. Age and bladder outlet obstruction are independently associated with detrusor overactivity in patients with benign prostatic hyperplasia. Eur Urol. 2008;54(2):419–26.
Kang MY, Ku JH, Oh SJ. Non-invasive parameters predicting bladder outlet obstruction in korean men with lower urinary tract symptoms. J Korean Med Sci. 2010;25(2):272–5.
Porru D, Jallous H, Cavalli V, Sallusto F, Rovereto B. Prognostic value of a combination of IPSS, flow rate and residual urine volume compared to pressure-flow studies in the preoperative evaluation of symptomatic BPH. Eur Urol. 2002;41(3):246–9.
Blaivas JG, Forde JC, Davila JL, Policastro L, Tyler M, Aizen J, et al. Surgical treatment of detrusor underactivity: a short term proof of concept study. Int Braz J Urol. 2017;43(3):540–8. This study established the difference in outcomes between DU and BOO, and supports the use of urodynamic findings and their utility in the clinical decision making.
Eckhardt MD, van Venrooij GEPM, Boon TA. Symptoms, prostate volume, and urodynamic findings in elderly male volunteers without and with LUTS and in patients with LUTS suggestive of benign prostatic hyperplasia. Urology. 2001;58(6):966–71.
EAU guidelines on the management of non-neurogenic male LUTS - diagnostic evaluation - Uroweb [Internet]. Uroweb - European Association of Urology. [cited 2022 Sep 13]. Available from: https://uroweb.org/guidelines/management-of-non-neurogenic-male-luts/chapter/diagnostic-evaluation. These guidelines include comprehensive review of many aspects and were used as comparison to our review.
Yiou R, Audureau E, Loche CM, Dussaud M, Lingombet O, Binhas M. Comprehensive evaluation of embarrassment and pain associated with invasive urodynamics. Neurourol Urodyn. 2015;34(2):156–60.
Ko KJ, Suh YS, Kim TH, Sung HH, Ryu GH, Lee KS. Diagnosing bladder outlet obstruction using the penile cuff test in men with lower urinary tract symptoms. Neurourol Urodyn. 2017;36(7):1884–9. This study demonstrates the utility of penile cuff test compared with PFS, in terms of costs, adverse events, and accuracy.
Onur R, Özden M, Orhan I, Kalkan A, Semercioz A. Incidence of bacteraemia after urodynamic study. J Hosp Infect. 2004;57(3):241–4.
Foon R, Toozs‐Hobson P, Latthe P. Prophylactic antibiotics to reduce the risk of urinary tract infections after urodynamic studies. Cochrane Database of Systematic Reviews [Internet]. 2012 [cited 2022 Sep 18];(10). Available from: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD008224.pub2/full.
Porru D, Madeddu G, Campus G, Montisci I, Scarpa RM, Usai E. Evaluation of morbidity of multi-channel pressure-flow studies. Neurourol Urodyn. 1999;18(6):647–52.
Leitner L, Walter M, Sammer U, Knüpfer SC, Mehnert U, Kessler TM. Urodynamic investigation: a valid tool to define normal lower urinary tract function? PLoS ONE. 2016;11(10): e0163847.
Nr S, Je S, Ap K. Artifacts and abnormal findings may limit the use of asymptomatic volunteers as controls for studies of multichannel urodynamics. Minerva urology and nephrology [Internet]. 2021 Oct [cited 2022 Dec 2];73(5). Available from: https://pubmed.ncbi.nlm.nih.gov/32638575/.
Nitti VW, Kim Y, Combs AJ. Correlation of the AUA symptom index with urodynamics in patients with suspected benign prostatic hyperplasia. Neurourol Urodyn. 1994;13(5):521–7 (discussion 527-529).
de la Rosette JJMCH, Witjes WPJ, Schäfer W, Abrams P, Donovan JL, Peters TJ, et al. Relationships between lower urinary tract symptoms and bladder outlet obstruction: results from the ICS-“BPH” study. Neurourol Urodyn. 1998;17(2):99–108.
Reddy SVK, Shaik AB. Non-invasive evaluation of bladder outlet obstruction in benign prostatic hyperplasia: a clinical correlation study. Arab J Urol. 2019;17(4):259–64. This study gave a recent view of the accuracy of few tests to diagnose BOO.
Steele GS, Sullivan MP, Sleep DJ, Yalla SV. Combination of symptom score, flow rate and prostate volume for predicting bladder outflow obstruction in men with lower urinary tract symptoms. J Urol. 2000;164(2):344–8.
Hashim H, Elhilali M, Bjerklund Johansen TE, Abrams P. The immediate and 6-mo reproducibility of pressure–flow studies in men with benign prostatic enlargement. Eur Urol. 2007;52(4):1186–94.
Renganathan A, Cartwright R, Cardozo L, Robinson D, Srikrishna S. Quality control in urodynamics: analysis of an international multi-center study. Neurourol Urodyn. 2009;28(5):380–4.
XLewis AL, Young GJ, Selman LE, Rice C, Clement C, Ochieng CA, et al. Urodynamics tests for the diagnosis and management of bladder outlet obstruction in men: the UPSTREAM non-inferiority RCT. Health Technol Assess. 2020;24(42):1–122. This comprehensive and important study re-opens the discussion about the use and utility of PFS – which may have far-reaching consequences on this issue.
Lerner LB, McVary KT, Barry MJ, Bixler BR, Dahm P, Das AK, et al. Management of lower urinary tract symptoms attributed to benign prostatic hyperplasia: AUA guideline part I—initial work-up and medical management. J Urol. 2021;206(4):806–17. These guidelines include comprehensive review of many aspects and were used as comparison to our review.
Arnolds M, Oelke M. Positioning invasive versus noninvasive urodynamics in the assessment of bladder outlet obstruction. Curr Opin Urol. 2009;19(1):55–62.
Jung JH, Cho SY, Yoo C, Oh SJ. Establishment of the novel cystoscopic classification for bladder trabeculation of neurogenic bladder. Urology. 2014;84(3):515–9.
Takahashi R, Takei M, Namitome R, Yamaguchi O, Eto M. Symptoms and noninvasive test parameters that clinically differentiate detrusor underactivity from bladder outlet obstruction without a pressure-flow-based diagnosis in men with lower urinary tract symptoms. Neurourol Urodyn. 2021;40(1):303–9. This big study includes the predictive value of many parameters and non-invasive tests to differentiate between DU and BOO. This can be used in clinical practice.
De Nunzio C, Autorino R, Bachmann A, Briganti A, Carter S, Chun F, et al. The diagnosis of benign prostatic obstruction: development of a clinical nomogram. Neurourol Urodyn. 2016;35(2):235–40.
Meigs JB, Barry MJ, Giovannucci E, Rimm EB, Stampfer MJ, Kawachi I. Incidence rates and risk factors for acute urinary retention: the health professionals followup study. J Urol. 1999;162(2):376–82.
Emberton M, Elhilali M, Matzkin H, Harving N, van Moorselaar J, Hartung R, et al. Symptom deterioration during treatment and history of AUR are the strongest predictors for AUR and BPH-related surgery in men with LUTS treated with alfuzosin 10 mg once daily. Urology. 2005;66(2):316–22.
Luciani LG, Mattevi D, Ravanelli D, Anceschi U, Giusti G, Cai T, et al. A novel nomogram based on initial features to predict BPH progression. Int J Environ Res Public Health. 2022;19(15):9738.
Shinbo H, Kurita Y, Nakanishi T, Imanishi T, Otsuka A, Furuse H, et al. Resistive index: a newly identified predictor of outcome of transurethral prostatectomy in patients with benign prostatic hyperplasia. Urology. 2010;75(1):143–7.
Vredeveld T, van Benten E, Beekmans REPM, Koops MP, Ket JCF, Mollema J, et al. Reliability and validity of assessment methods available in primary care for bladder outlet obstruction and benign prostatic obstruction in men with lower urinary tract symptoms: a systematic review. BMJ Open. 2022;12(4): e056234. This comprehensive and recent systematic review provides valuable data about the validity and reliability of different parameters, including differences between different ways of achieving them.
de la Cruz MB, Adot Zurbano JM, Gutiérrez-Mínguez E, Gómez Sánchez E, Calvo S, Tamayo GE. Development of a Predictive model for the diagnosis of lower urinary tract obstruction in men. J Urol. 2022;208(3):668–75. This big study made a validated prediction model to differentiate between DU and BOO, based on multivariable analysis made of few easy-to-take parameters.
Lee YJ, Lee JK, Kim JJ, Lee HM, Oh JJ, Lee S, et al. Development and validation of a clinical nomogram predicting bladder outlet obstruction via routine clinical parameters in men with refractory nonneurogenic lower urinary tract symptoms. Asian J Androl. 2019;21(5):486–92. This study provides nomogram and information about the predictive value of many parameters.
Roehrborn CG, Sech S, Montoya J, Rhodes T, Girman CJ. Interexaminer reliability and validity of a three-dimensional model to assess prostate volume by digital rectal examination. Urology. 2001;57(6):1087–92.
Stone BV, Shoag J, Halpern JA, Mittal S, Lewicki P, Golombos DM, et al. Prostate size, nocturia and the digital rectal examination: a cohort study of 30 500 men. BJU Int. 2017;119(2):298–304.
Loeb S, Han M, Roehl KA, Antenor JAV, Catalona WJ. Accuracy of prostate weight estimation by digital rectal examination versus transrectal ultrasonography. J Urol. 2005;173(1):63–5.
Roehrborn CG, Girman CJ, Rhodes T, Hanson KA, Collins GN, Sech SM, et al. Correlation between prostate size estimated by digital rectal examination and measured by transrectal ultrasound. Urology. 1997;49(4):548–57.
Roehrborn CG, Chinn HKW, Fulgham PF, Simpkins KL, Peters PC. The role of transabdominal ultrasound in the prostatic hypertrophy. J Urol. 1986;135(6):1190–3.
Bosch JLHR, Bohnen AM, Groeneveld FPMJ. Validity of digital rectal examination and serum prostate specific antigen in the estimation of prostate volume in community-based men aged 50 to 78 years: The Krimpen Study. Eur Urol. 2004;46(6):753–9.
Su MZ, Lenaghan D, Woo HH. Dichotomous estimation of prostate volume: a diagnostic study of the accuracy of the digital rectal examination. World J Mens Health. 2013;31(3):220–5. This study is the biggest and latest information about the use of digital rectal examination and provides a method to use it properly.
Oelke M, Höfner K, Jonas U, de la Rosette JJ, Ubbink DT, Wijkstra H. Diagnostic accuracy of noninvasive tests to evaluate bladder outlet obstruction in men: detrusor wall thickness, uroflowmetry, postvoid residual urine, and prostate volume. Eur Urol. 2007;52(3):827–35.
Reynard JM, Yang Q, Donovan JL, Peters TJ, Schafer W, de la Rosette JJ, et al. The ICS-’BPH’ study: uroflowmetry, lower urinary tract symptoms and bladder outlet obstruction. Br J Urol. 1998;82(5):619–23.
Wadie BS. How correlated is BOO with different objective parameters commonly used in evaluation of BPH: a prospective study. Int Urol Nephrol. 2021;53(4):635–40. This study examined the correlation (not the predictive value and cutoffs) of the objective parameters commonly used- and showed their limited association with symptoms and obstruction scores.
Cheng Y, Li T, Wu X, Ling Q, Rao K, Yuan X, et al. The diagnostic value of non-invasive methods for diagnosing bladder outlet obstruction in men with lower urinary tract symptoms: a meta-analysis. Front Surg [Internet]. 2022 [cited 2022 Nov 13];9. Available from: https://www.frontiersin.org/articles/10.3389/fsurg.2022.986679. This is the most recent and largest meta-analysis we found that examines the predictive values of many parameters.
Nitti VW. Pressure Flow Urodynamic Studies: The gold standard for diagnosing bladder outlet obstruction. Rev Urol. 2005;7(Suppl 6):S14-21.
Abrams PH, Griffiths DJ. The assessment of prostatic obstruction from urodynamic measurements and from residual urine. Br J Urol. 1979;51(2):129–34.
Zhang X, Li G, Wei X, Mo X, Hu L, Zha Y, et al. Resistive index of prostate capsular arteries: a newly identified parameter to diagnose and assess bladder outlet obstruction in patients with benign prostatic hyperplasia. J Urol. 2012;188(3):881–7.
Malde S, Nambiar AK, Umbach R, Lam TB, Bach T, Bachmann A, et al. Systematic review of the performance of noninvasive tests in diagnosing bladder outlet obstruction in men with lower urinary tract symptoms. Eur Urol. 2017;71(3):391–402. This is an important systematic review and meta-analysis that reviews the properties of the non-invasive tests and their accuracy to predict BOO.
Oranusi CK, Nwofor AE, Mbonu O. Correlation between international prostate symptom score and uroflowmetry in patients with benign prostatic hyperplasia. Niger J Clin Pract. 2017;20(4):454–8.
Garg A, Bansal S, Saha S, Kumar A. Study of correlation of urodynamic profile with symptom scoring and ultrasonographic parameters in patients with benign prostatic hyperplasia. J Family Med Prim Care. 2020;9(1):215–20.
Simon RM, Howard LE, Moreira DM, Roehrborn C, Vidal A, Castro-Santamaria R, et al. Does peak urine flow rate predict the development of incident lower urinary tract symptoms in men with mild to no current symptoms? Results from REDUCE. J Urol. 2017;198(3):650–6.
Chen X, Man Q, Wei X, Ren X, Li G, Lu Z, et al. Predictive value of preoperative comprehensive evaluation on the efficacy of HoLEP. Transl Androl Urol. 2020;9(4):1603–10. This study provides us a view about the prognostic predictive value of non-invasive tests in the context of HOLEP procedure and not only in the context of BOO diagnosis.
Gravas S, Palacios-Moreno JM, Thompson D, Concas F, Kamola PJ, Roehrborn CG, et al. Understanding treatment response in individual profiles of men with prostatic enlargement at risk of progression. Eur Urol Focus [Internet]. 2022 Aug 18 [cited 2022 Oct 7]; Available from: https://www.sciencedirect.com/science/article/pii/S2405456922001651. This huge data analysis provides us a comprehensive view about the prognostic predictive value of non-invasive tests in the context of pharmacological treatment and not only in the context of BOO diagnosis. This can aid to guide the decision making and enhance the treatment outcomes.
Kim BS, Ko YH, Song PH, Kim TH, Kim KH, Kim BH. Prostatic urethral length as a predictive factor for surgical treatment of benign prostatic hyperplasia: a prospective, multiinstitutional study. Prostate Int. 2019;7(1):30–4.
Namitome R, Takei M, Takahashi R, Kikutake C, Yokomizo A, Yamaguchi O, et al. A prediction model of detrusor underactivity based on symptoms and noninvasive test parameters in men with lower urinary tract symptoms: an analysis of a large group of patients undergoing pressure-flow studies. J Urol. 2020;203(4):779–85. This big study made a prediction model to differentiate between DU and BOO, based on few parameters.
Jiang YH, Kuo HC. Video-urodynamic characteristics of non-neurogenic, idiopathic underactive bladder in men - a comparison of men with normal tracing and bladder outlet obstruction. PLoS ONE. 2017;12(4): e0174593.
Matsukawa Y, Yoshida M, Yamaguchi O, Takai S, Majima T, Funahashi Y, et al. Clinical characteristics and useful signs to differentiate detrusor underactivity from bladder outlet obstruction in men with non-neurogenic lower urinary tract symptoms. Int J Urol. 2020;27(1):47–52.
Wada N, Watanabe M, Ishikawa M, Takeuchi K, Miyauchi K, Abe N, et al. Uroflowmetry pattern in detrusor underactivity and bladder outlet obstruction in male patients with lower urinary tract symptoms. LUTS. 2021;13(3):361–5.
Yoldas M. Non-invasive diagnosis of under active bladder: a pilot study. Arch Ital Urol Androl. 2022;94(1):51–6.
Lambert E, Denys MA, Poelaert F, Everaert K, Lumen N. Validated uroflowmetry-based predictive model for the primary diagnosis of urethral stricture disease in men. Int J Urol. 2018;25(9):792–8.
Bray A, Harding C, Pickard R, Drinnan M. Individualized volume-corrected maximum flow rate correlates with outcome from bladder outlet surgery in men with lower urinary tract symptoms. Int J Urol. 2016;23(7):587–92.
Non-neurogenic chronic urinary retention: consensus definition, management strategies, and future opportunities - American Urological Association [Internet]. [cited 2023 May 28]. Available from: https://www.auanet.org/guidelines-and-quality/quality-and-measurement/quality-improvement/clinical-consensus-statement-and-quality-improvement-issue-brief-(ccs-and-qiib)/chronic-urinary-retention. This consensus is important to understand the definition, diagnosis and management of chronic urinary retention and the use of PVR test.
Lee KS, Song PH, Ko YH. Does uroflowmetry parameter facilitate discrimination between detrusor underactivity and bladder outlet obstruction? Investig Clin Urol. 2016;57(6):437–41.
Kalil J, D Ancona CAL. Detrusor underactivity versus bladder outlet obstruction clinical and urodynamic factors. Int Braz J Urol. 2020;46(3):419–24.
• Choo MS, Yoo C, Cho SY, Jeong SJ, Jeong CW, Ku JH, et al. Development of decision support formulas for the prediction of bladder outlet obstruction and prostatic surgery in patients with lower urinary tract symptom/benign prostatic hyperplasia: Part I, Development of the Formula and its Internal Validation. Int Neurourol J. 2017;21(Suppl 1):S55-65. This is a big innovative study that recruits the different common tests to predict (and maybe guide) the decision about surgery, in addition to prediction of BOO.
Töz E, Kurt S, Sahin Ç, Canda MT. Frequency of recurrent urinary tract infection in patients with pelvic organ prolapse. Res Rep Urol. 2015;7:9–12.
Roehrborn CG, Group AS. Alfuzosin 10 mg once daily prevents overall clinical progression of benign prostatic hyperplasia but not acute urinary retention: results of a 2-year placebo-controlled study. BJU Int. 2006;97(4):734–41.
Shinbo H, Kurita Y, Takada S, Imanishi T, Otsuka A, Furuse H, et al. Resistive index as risk factor for acute urinary retention in patients with benign prostatic hyperplasia. Urology. 2010;76(6):1440–5.
Roehrborn CG, Kaplan SA, Lee MW, Slawin KM, McVary KT, Kusek JW, et al. 1638: Baseline post void residual urine volume as a predictor of urinary outcomes in men with BPH in the MTOPS study. J Urol. 2005;173(4S):443–4.
Nadler RB, Humphrey PA, Smith DS, Catalona WJ, Ratliff TL. Effect of inflammation and benign prostatic hyperplasia on elevated serum prostate specific antigen levels. J Urol. 1995;154(2 Pt 1):407–13.
Lokant MT, Naz RK. Presence of PSA auto-antibodies in men with prostate abnormalities (prostate cancer/benign prostatic hyperplasia/prostatitis). Andrologia. 2015;47(3):328–32.
Zackrisson B, Ulleryd P, Aus G, Lilja H, Sandberg T, Hugosson J. Evolution of free, complexed, and total serum prostate-specific antigen and their ratios during 1 year of follow-up of men with febrile urinary tract infection. Urology. 2003;62(2):278–81.
Roehrborn CG, Boyle P, Gould AL, Waldstreicher J. Serum prostate-specific antigen as a predictor of prostate volume in men with benign prostatic hyperplasia. Urology. 1999;53(3):581–9.
Morote J, Encabo G, López M, de Torres IM. Prediction of prostate volume based on total and free serum prostate–specific antigen: is it reliable? EUR. 2000;38(1):91–5.
Patel DN, Feng T, Simon RM, Howard LE, Vidal AC, Moreira DM, et al. PSA predicts development of incident lower urinary tract symptoms: results from the REDUCE study. Prostate Cancer Prostatic Dis. 2018;21(2):238–44.
Roehrborn CG, McConnell J, Bonilla J, Rosenblatt S, Hudson PB, Malek GH, et al. Serum prostate specific antigen is a strong predictor of future prostate growth in men with benign prostatic hyperplasia. PROSCAR long-term efficacy and safety study. J Urol. 2000;163(1):13–20.
Kok ET, Schouten BW, Bohnen AM, Groeneveld FPMW, Thomas S, Bosch JLHR. Risk factors for lower urinary tract symptoms suggestive of benign prostatic hyperplasia in a community based population of healthy aging men: the Krimpen study. J Urol. 2009;181(2):710–6.
Roehrborn CG, McConnell JD, Lieber M, Kaplan S, Geller J, Malek GH, et al. Serum prostate-specific antigen concentration is a powerful predictor of acute urinary retention and need for surgery in men with clinical benign prostatic hyperplasia11A complete list of the members of the PLESS Study Group is given in the Appendix. Urology. 1999;53(3):473–80.
Milonas D, Trumbeckas D. Prostate-specific antigen and transition zone index - powerful predictors for acute urinary retention in men with benign prostatic hyperplasia. Medicina (Kaunas). 2003;39(11):1071–7.
Roehrborn CG, Boyle P, Bergner D, Gray T, Gittelman M, Shown T, et al. Serum prostate-specific antigen and prostate volume predict long-term changes in symptoms and flow rate: results of a four-year, randomized trial comparing finasteride versus placebo. Urology. 1999;54(4):662–9.
Wei JT, Barocas D, Carlsson S, Coakley F, Eggener S, Etzioni R, et al. Early detection of prostate cancer: AUA/SUO guideline part i: prostate cancer screening. J Urol. 2023;0(0). https://doi.org/10.1097/JU.0000000000003491.
Ilic D, Djulbegovic M, Jung JH, Hwang EC, Zhou Q, Cleves A, et al. Prostate cancer screening with prostate-specific antigen (PSA) test: a systematic review and meta-analysis. BMJ. 2018;5(362): k3519.
US Preventive Services Task Force. Screening for prostate cancer: US Preventive Services Task Force recommendation statement. JAMA. 2018;319(18):1901–13.
Styles RA, Neal DE, Griffiths CJ, Ramsden PD. Long-term monitoring of bladder pressure in chronic retention of urine: the relationship between detrusor activity and upper tract dilatation. J Urol. 1988;140(2):330–4.
George NJ, O’Reilly PH, Barnard RJ, Blacklock NJ. High pressure chronic retention. Br Med J (Clin Res Ed). 1983;286(6380):1780–3.
Lee DS, Kim HW, Lee SJ. Transurethral prostate surgery as a preventive method against progression of chronic kidney disease in patients with urodynamically proven bladder outlet obstruction. World J Urol. 2020;38(10):2583–93.
Comiter CV, Sullivan MP, Schacterle RS, Cohen LH, Valla SV. Urodynamic risk factors for renal dysfunction in men with obstructive and nonobstructive voiding dysfunction. J Urol. 1997;158(1):181–5.
• Lowe FC, Michel MC, Wruck JM, Verbeek AE. Is dipstick urinalysis screening beneficial in men with lower urinary tract symptoms? Adv Ther. 2019;36(10):2954–67. This huge study shines light on the information that dipstick urinalysis can provide us to diagnose clinically important pathologies.
Khasriya R, Khan S, Lunawat R, Bishara S, Bignal J, Malone-Lee M, et al. The inadequacy of urinary dipstick and microscopy as surrogate markers of urinary tract infection in urological outpatients with lower urinary tract symptoms without acute frequency and dysuria. Journal of Urology. 2010;183(5):1843–7.
Doolin J, Reese ZA, Mukamal KJ. National trends in the use of PSA, urinalysis, and digital rectal exam for evaluation of lower urinary tract symptoms in men. World J Urol. 2021;39(3):855–60.
Grossfeld GD, Coakley FV. Benign prostatic hyperplasia: clinical overview and value of diagnostic imaging. Radiol Clin N Am. 2000;38(1):31–47.
Stravodimos KG, Petrolekas A, Kapetanakis T, Vourekas S, Koritsiadis G, Adamakis I, et al. TRUS versus transabdominal ultrasound as a predictor of enucleated adenoma weight in patients with BPH. Int Urol Nephrol. 2009;41(4):767–71.
Jia G, Baudendistel KT, von Tengg-Kobligk H, Heverhagen JT, Polzer H, Henry H, et al. Assessing prostate volume by magnetic resonance imaging: a comparison of different measurement approaches for organ volume analysis. Invest Radiol. 2005;40(4):243–8.
Rahmouni A, Yang A, Tempany CMC, Frenkel T, Epstein J, Walsh P, et al. Accuracy of in-vivo assessment of prostatic volume by MRI and transrectal ultrasonography. J Comput Assist Tomogr. 1992;16(6):935–40.
• Garg G, Sankhwar SN, Goel A, Pandey S, Sharma D, Parihar A. Evaluation of resistive index of the prostate and bladder sonomorphologic parameters as replacements for urodynamics to predict bladder outlet obstruction in patients with lower urinary tract symptoms suggestive of benign prostatic hyperplasia. Low Urin Tract Symptoms. 2019;11(3):163–8. This study provides us with valuable data about the predictive value of different parameters to diagnose BOO.
Abdel-Aal A, El-Karamany T, Al-Adl AM, Abdel-Wahab O, Farouk H. Assessment of noninvasive predictors of bladder outlet obstruction and acute urinary retention secondary to benign prostatic enlargement. Arab J Urol. 2011;9(3):209–14.
Lim KB, Ho H, Foo KT, Wong MYC, Fook-Chong S. Comparison of intravesical prostatic protrusion, prostate volume and serum prostatic-specific antigen in the evaluation of bladder outlet obstruction. Int J Urol. 2006;13(12):1509–13.
Franco G, De Nunzio C, Leonardo C, Tubaro A, Ciccariello M, De Dominicis C, et al. Ultrasound assessment of intravesical prostatic protrusion and detrusor wall thickness–new standards for noninvasive bladder outlet obstruction diagnosis? J Urol. 2010;183(6):2270–4.
Deebajah M, Bazzi M, Walton E, Pantelic M, Park H, Dabaja A, et al. Prostate volume measured by magnetic resonance imaging is not a predictor of lower urinary tract symptoms. J Family Med Prim Care. 2019;8(4):1370–3.
• Yang TK, Chang CC, Chang HC, Yang HJ, Huang KH. Factors associated with bothersome lower urinary tract symptoms in middle-aged men receiving health checkup. Sci Rep. 2019;9(1):901. This study shed light on the association between symptoms and different parameters.
Gyasi-Sarpong CK, Acheampong E, Yeboah FA, Aboah K, Laing EF, Amoah G. Predictors of the international prostate symptoms scores for patients with lower urinary tract symptoms: a descriptive cross-sectional study. Urol Ann. 2018;10(3):317–23.
Barry MJ, Cockett ATK, Holtgrewe HL, McConnell JD, Sihelnik SA, Winfield HN. Relationship of symptoms of prostatism to commonly used physiological and anatomical measures of the severity of benign prostatic hyperplasia. J Urol. 1993;150(2 Part 1):351–8.
• Qian S, Zhang S, Xia W, Xu D, Qi J, Shen H, et al. Correlation of prostatic morphological parameters and clinical progression in aging Chinese men with benign prostatic hyperplasia: results from a cross-sectional study. Prostate. 2021;81(8):478–86. This study aims to find the association between different parameters and disease progression, and not only obstruction. This can guide informed decisions to a patient.
Boyle P, Lawrence Gould A, Roehrborn CG. Prostate volume predicts outcome of treatment of benign prostatic hyperplasia with finasteride: meta-analysis of randomized clinical trials. Urology. 1996;48(3):398–405.
• Hashimoto M, Shimizu N, Sugimoto K, Hongoh S, Minami T, Nozawa M, et al. Efficacy of Adding dutasteride to α-blocker therapy treated benign prostatic hyperplasia patients with small volume prostate (<30 mL). LUTS. 2017;9(3):157–60. This study provided us with valuable data about the significance of prostate size in the context of pharmacological treatment and thus the value of this test regardless of its use to diagnose BOO. The results of studies as such- influenced the current AUA guidelines.
Marks LS, Roehrborn CG, Wolford E, Wilson TH. The effect of dutasteride on the peripheral and transition zones of the prostate and the value of the transition zone index in predicting treatment response. J Urol. 2007;177(4):1408–13.
Hong SJ, Ko WJ, Kim SI, Chung BH. Identification of baseline clinical factors which predict medical treatment failure of benign prostatic hyperplasia: an observational cohort study. Eur Urol. 2003;44(1):94–100.
Hong KP, Byun YJ, Yoon H, Park YY, Chung WS. Prospective factor analysis of alpha blocker monotherapy failure in benign prostatic hyperplasia. Korean J Urol. 2010;51(7):488–91.
• Matsukawa Y, Ishida S, Majima T, Funahashi Y, Sassa N, Kato M, et al. Intravesical prostatic protrusion can predict therapeutic response to silodosin in male patients with lower urinary tract symptoms. Int J Urol. 2017;24(6):454–9. This study provided us valuable data about the significance of different parameters (especially IPP) in context of pharmacological treatment and thus the value of this test regardless of its use to diagnose BOO.
Kalkanli A, Tandogdu Z, Aydin M, Karaca AS, Hazar AI, Balci MBC, et al. Intravesical prostatic protrusion: a potential marker of alpha-blocker treatment success in patients with benign prostatic enlargement. Urology. 2016;1(88):161–5.
Moore RA. Benign hypertrophy and carcinoma of the prostate: occurrence and experimental production in animals. Surgery. 1944;16(1):152–67.
Meikle AW, Stephenson RA, Lewis CM, Middleton RG. Effects of age and sex hormones on transition and peripheral zone volumes of prostate and benign prostatic hyperplasia in twins*. J Clin Endocrinol Metab. 1997;82(2):571–5.
Berges R, Oelke M. Age-stratified normal values for prostate volume, PSA, maximum urinary flow rate, IPSS, and other LUTS/BPH indicators in the German male community-dwelling population aged 50 years or older. World J Urol. 2011;29(2):171–8.
Chia SJ, Heng CT, Chan SP, Foo KT. Correlation of intravesical prostatic protrusion with bladder outlet obstruction. BJU Int. 2003;91(4):371–4.
• Lee A, Lee HJ, Lim KB, Huang HH, Ho H, Foo KT. Can intravesical prostatic protrusion predict bladder outlet obstruction even in men with good flow? Asian J Urol. 2016;3(1):39–43. This study gave us a new concept about the ability of non-invasive tests (IPP) to adjunct prediction of BOO even in men with good urinary flow.
Keqin Z, Zhishun X, Jing Z, Haixin W, Dongqing Z, Benkang S. Clinical significance of intravesical prostatic protrusion in patients with benign prostatic enlargement. Urology. 2007;70(6):1096–9.
Krivoborodov GG, Efremov NS, Bolotov AD. Ultrasound indicators of the prostate, urinary bladder and uroflowmetry parameters in the diagnosis of infravesical obstruction in men with benign prostatic hyperplasia. Urologiia. 2017;5:9–14.
Park SC, Lee JW, Rim JS. Relación entre la protrusión prostática intravesical y los hallazgos del estudio de presión-flujo en pacientes con obstrucción prostática benigna/síntomas del tracto urinario inferior. Actas Urológicas Españolas. 2012;36(3):165–70.
Aganovic D, Hasanbegovic M, Prcic A, Kulovac B, Hadziosmanovic O. Which is a better indicator of bladder outlet obstruction in patients with benign prostatic enlargement–intravesical protrusion of prostate or bladder wall thickness? Med Arch. 2012;66(5):324–8.
Ahmed AF. Sonographic parameters predicting the outcome of patients with lower urinary tract symptoms/benign prostatic hyperplasia treated with alpha1-adrenoreceptor antagonist. Urology. 2016;88:143–8.
Shin SH, Kim JW, Kim JW, Oh MM, Moon DG. Defining the degree of intravesical prostatic protrusion in association with bladder outlet obstruction. Korean J Urol. 2013;54(6):369–72.
• Tan YG, Teo JS, Kuo TLC, Guo L, Shi L, Shutchaidat V, et al. A systemic review and meta-analysis of transabdominal intravesical prostatic protrusion assessment in determining bladder outlet obstruction and unsuccessful trial without catheter. Eur Urol Focus. 2022;8(4):1003–14. This comprehensive systematic review gave valuable data about trans-abdominal IPP test.
Rieken M, Presicce F, Autorino R, De Nunzio C. Clinical significance of intravesical prostatic protrusion in the management of benign prostatic enlargement: a systematic review and critical analysis of current evidence. Minerva Urol Nephrol [Internet]. 2017 Oct [cited 2022 Sep 14];69(6). Available from: https://www.minervamedica.it/index2.php?show=R19Y2017N06A0548.
Raphael JE, Abhulimen V. Is there any relationship between total prostate volume, intravesical prostatic protrusion and lower urinary tract symptoms in adult Nigerian men with benign prostatic enlargement? West Afr J Med. 2021;38(6):578–82.
Eze BU, Mbaeri TU, Oranusi KC, Abiahu JA, Nwofor AM, Orakwe JC, et al. Correlation between intravesical prostatic protrusion and international prostate symptom score among Nigerian men with benign prostatic hyperplasia. Niger J Clin Pract. 2019;22(4):454.
Bang WJ, Kim HW, Lee JY, Lee DH, Hah YS, Lee HH, et al. Prostatic urethral angulation associated with urinary flow rate and urinary symptom scores in men with lower urinary tract symptoms. Urology. 2012;80(6):1333–7.
Park YJ, Bae KH, Jin BS, Jung HJ, Park JS. Is increased prostatic urethral angle related to lower urinary tract symptoms in males with benign prostatic hyperplasia/lower urinary tract symptoms? Korean J Urol. 2012;53(6):410–3.
Cumpanas AA, Botoca M, Minciu R, Bucuras V. Intravesical prostatic protrusion can be a predicting factor for the treatment outcome in patients with lower urinary tract symptoms due to benign prostatic obstruction Treated With Tamsulosin. Urology. 2013;81(4):859–63.
• Topazio L, Perugia C, De Nunzio C, et al. Intravescical prostatic protrusion is a predictor of alpha blockers response: results from an observational study. BMC Urol 2018;18:6. https://doi.org/10.1186/s12894-018-0320-0. This study provides us data about the clinically significance of IPP in the meaning of therapeutic response.
Park HY, Lee JY, Park SY, Lee SW, Kim YT, Choi HY, et al. Efficacy of alpha blocker treatment according to the degree of intravesical prostatic protrusion detected by transrectal ultrasonography in patients with benign prostatic hyperplasia. Korean J Urol. 2012;53(2):92–7.
Seo YM, Kim HJ. Impact of intravesical protrusion of the prostate in the treatment of lower urinary tract symptoms/benign prostatic hyperplasia of moderate size by alpha receptor antagonist. Int Neurourol J. 2012;16(4):187–90.
• Matsukawa Y, Kato M, Funahashi Y, Majima T, Yamamoto T, Gotoh M. What are the predicting factors for the therapeutic effects of dutasteride in male patients with lower urinary tract symptoms? Investigation using a urodynamic study. Neurourol Urodyn. 2017;36(7):1809–15. This study reveals the predictive tests for therapeutic effects of dutasteride in male patients with lower urinary tract symptoms.
Hirayama K, Masui K, Hamada A, Shichiri Y, Masuzawa N, Hamada S. Evaluation of intravesical prostatic protrusion as a predictor of dutasteride-resistant lower urinary tract symptoms/benign prostatic enlargement with a high likelihood of surgical intervention. Urology. 2015;86(3):565–9.
Mariappan P, Brown DJG, McNeill AS. Intravesical prostatic protrusion is better than prostate volume in predicting the outcome of trial without catheter in white men presenting with acute urinary retention: a prospective clinical study. J Urol. 2007;178(2):573–7 (discussion 577).
Foo KT, Tan YH. Intravesical prostatic protrusion predicts the outcome of a trial without catheter following acute urine retention. J Urol. 2003;170(6 Pt 1):2339–41.
Lee LS, Sim HG, Lim KB, Wang D, Foo KT. Intravesical prostatic protrusion predicts clinical progression of benign prostatic enlargement in patients receiving medical treatment. Int J Urol. 2010;17(1):69–74.
• Tian Y, Zhang H, Cao Y, Yang L, Luo G. The P.R.OS.T.A.T.E nomogram for the preoperative prediction of clinical efficacy of transurethral resection of the prostate in benign prostatic hyperplasia patients. Clin Interv Aging. 2022;17:845–55. This study provided us data about the preoperative parameters that can predict the outcome of TURP and made a nomogram for them.
Rademakers KLJ, van Koeveringe GA, Oelke M. FORCE Research Group, Maastricht and Hannover. Ultrasound detrusor wall thickness measurement in combination with bladder capacity can safely detect detrusor underactivity in adult men. World J Urol. 2017;35(1):153–9.
Manieri C, Carter SS, Romano G, Trucchi A, Valenti M, Tubaro A. The diagnosis of bladder outlet obstruction in men by ultrasound measurement of bladder wall thickness. J Urol. 1998;159(3):761–5.
Ding Z, Wang H, Zhang W, et al. Bladder wall thickness measured by CT can predict bladder outlet obstruction in men: a retrospective cohort study. Int Urol Nephrol. 2023;55:43–9. https://doi.org/10.1007/s11255-022-03361-8.
Farag F, Elbadry M, Saber M, Badawy AA, Heesakkers J. A novel algorithm for the non-invasive detection of bladder outlet obstruction in men with lower urinary tract symptoms. Arab J Urol. 2017;15(2):153–8.
Salah Azab S, Elsheikh MG. The impact of the bladder wall thickness on the outcome of the medical treatment using alpha-blocker of BPH patients with LUTS. Aging Male. 2015;18(2):89–92.
Elbadawi A, Yalla SV, Resnick NM. Structural basis of geriatric voiding dysfunction. I. Methods of a prospective ultrastructural/urodynamic study and an overview of the findings. J Urol. 1993;150(5 Pt 2):1650–6.
Inui E, Ochiai A, Naya Y, Ukimura O, Kojima M. Comparative morphometric study of bladder detrusor between patients with benign prostatic hyperplasia and controls. J Urol. 1999;161(3):827–30.
Oelke M, Höfner K, Wiese B, Grünewald V, Jonas U. Increase in detrusor wall thickness indicates bladder outlet obstruction (BOO) in men. World J Urol. 2002;19(6):443–52.
Kessler TM, Gerber R, Burkhard FC, Studer UE, Danuser H. Ultrasound assessment of detrusor thickness in men-can it predict bladder outlet obstruction and replace pressure flow study? J Urol. 2006;175(6):2170–3.
Sinha S, Matai L. Is isolated bladder outlet obstruction associated with hydronephrosis? A database analysis. Neurourol Urodyn. 2020;39(8):2361–7.
van der Waart TH, Boender H, van de Beek C, Wolfs GG, Janknegt RA, Knottnerus JA. Utility of ultrasound of the upper urinary tract in elderly men with indicators of obstructive symptoms or abnormal flow: how often can silent hydronephrosis be detected in general practice? Fam Pract. 1998;15(6):534–6.
Koch WF, Ezz el Din K, de Wildt MJ, Debruyne FM, de la Rosette JJ. The outcome of renal ultrasound in the assessment of 556 consecutive patients with benign prostatic hyperplasia. J Urol. 1996;155(1):186–9.
Stoffel JT, Peterson AC, Sandhu JS, Suskind AM, Wei JT, Lightner DJ. AUA white paper on nonneurogenic chronic urinary retention: consensus definition, treatment algorithm, and outcome end points. J Urol. 2017;198(1):153–60.
Kojima M, Inui E, Ochiai A, Naya Y, Ukimura O, Watanabe H. Ultrasonic estimation of bladder weight as a measure of bladder hypertrophy in men with infravesical obstruction: a preliminary report. Urology. 1996;47(6):942–7.
Ochiai A, Kojima M. Correlation of ultrasound-estimated bladder weight with ultrasound appearance of the prostate and postvoid residual urine in men with lower urinary tract symptoms. Urology. 1998;51(5):722–9.
Kojima M, Inui E, Ochiai A, Naya Y, Ukimura O, Watanabe H. Noninvasive quantitative estimation of infravesical obstruction using ultrasonic measurement of bladder weight. J Urol. 1997;157(2):476–9.
Presicce F, De Nunzio C, Gacci M, Finazzi Agrò E, Tubaro A. Non-invasive ultrasound measurements in male patients with LUTS and benign prostatic obstruction: implication for diagnosis and treatment. Minerva Urol Nefrol. 2017;69(3):220–33.
Li HZ, Zhang XB, Li JC, Xiao H, Huang ZM. Study on the change of bladder wall weight pre and after surgery in patients with benign prostatic hyperplasia. Zhonghua Wai Ke Za Zhi. 2007;45(14):954–6.
Miyashita H, Kojima M, Miki T. Ultrasonic measurement of bladder weight as a possible predictor of acute urinary retention in men with lower urinary tract symptoms suggestive of benign prostatic hyperplasia. Ultrasound Med Biol. 2002;28(8):985–90.
Ho CCK, Ngoo KS, Hamzaini AH, Rizal AMM, Zulkifli MZ. Urinary bladder characteristics via ultrasound as predictors of acute urinary retention in men with benign prostatic hyperplasia. Clin Ter. 2014;165(2):75–81.
Greene DR, Egawa S, Hellerstein DK, Scardino PT. Sonographic measurements of transition zone of prostate in men with and without benign prostatc hyperplasia. Urology. 1990;36(4):293–9.
Kaplan SA, Te AE, Pressler LB, Olsson CA. Transition zone index as a method of assessing benign prostatic hyperplasia: correlation with symptoms, urine flow and detrusor pressure. J Urol. 1995;154(5):1764–9.
Qalawena MM, Al-Shatouri MA, Motawaa MA, El-Sakka AI. Association between prostate zonal volume and erectile dysfunction in patients with benign prostatic hyperplasia. Sex Med. 2020;8(2):205–13.
Tian Y, Liu HM, Yang B, Yang XS, Sun ZL, Sun F, et al. Prostatic anatomical parameters correlate with clinical characteristics suggestive of benign prostatic hyperplasia. Asian J Androl. 2021;23(1):64–8.
Lepor H, Nieder A, Feser J, O’Connell C, Dixon C. Total prostate and transition zone volumes, and transition zone index are poorly correlated with objective measures of clinical benign prostatic hyperplasia. J Urol. 1997;158(1):85–8.
• Kurokawa S, Kamei J, Sakata K, Sugihara T, Fujisaki A, Ando S, et al. The cutoff value of transitional zone index predicting the efficacy of dutasteride on subjective symptoms in patients with benign prostate hyperplasia. LUTS. 2022;14(4):261–6. This study provides us with data about different parameters (especially TZI) that can predict the outcome of pharmacological treatment.
Choi JD, Kim JH, Ahn SH. Transitional zone index as a predictor of the efficacy of α-blocker and 5α-reductase inhibitor combination therapy in Korean patients with benign prostatic hyperplasia. Urol Int. 2016;96(4):406–12.
Ohtani T, Hayashi Y, Kishino TE, Fujimoto K, Hirao Y, Ozono S, et al. A new parameter in decision making for transurethral electroresection of benign prostate hyperplasia. Eur Urol. 1999;35(3):185–91.
Kojima M, Ochiai A, Naya Y, Okihara K, Ukimura O, Miki T. Doppler resistive index in benign prostatic hyperplasia: correlation with ultrasonic appearance of the prostate and infravesical obstruction. Eur Urol. 2000;37(4):436–42.
Aldaqadossi HA, Elgamal SA, Saad M. The value of measuring the prostatic resistive index vs. pressure-flow studies in the diagnosis of bladder outlet obstruction caused by benign prostatic hyperplasia. Arab J Urol. 2012;10(2):186–91.
Belenky A, Abarbanel Y, Cohen M, Yossepowitch O, Livne PM, Bachar GN. Detrusor resistive index evaluated by Doppler ultrasonography as a potential indicator of bladder outlet obstruction. Urology. 2003;62(4):647–50.
Suzuki T, Otsuka A, Ozono S. Combination of intravesical prostatic protrusion and resistive index is useful to predict bladder outlet obstruction in patients with lower urinary tract symptoms suggestive of benign prostatic hyperplasia. Int J Urol. 2016;23(11):929–33.
Tsuru N, Kurita Y, Masuda H, Suzuki K, Fujita K. Role of Doppler ultrasound and resistive index in benign prostatic hypertrophy. Int J Urol. 2002;9(8):427–30.
Kwon SY, Ryu JW, Choi DH, Lee KS. Clinical significance of the resistive index of prostatic blood flow according to prostate size in benign prostatic hyperplasia. Int Neurourol J. 2016;20(1):75–80.
Berger AP, Bartsch G, Deibl M, Alber H, Pachinger O, Fritsche G, et al. Atherosclerosis as a risk factor for benign prostatic hyperplasia. BJU Int. 2006;98(5):1038–42.
Ku JH, Ko DW, Cho JY, Oh SJ. Correlation between prostatic urethral angle and bladder outlet obstruction index in patients with lower urinary tract symptoms. Urology. 2010;75(6):1467–71.
• Kim BH, Kim KH, Ko YH, Song PH, Kim TH, Kim BS. The prostatic urethral angle can predict the response to alpha adrenoceptor antagonist monotherapy for treating nocturia in men with lower urinary tract symptom: A multicenter study. Prostate Int. 2016;4(1):30–5. This study provides us data about different parameters (especially prostatic urethral angle) that can predict the outcome of pharmacological treatment.
Farag FF, Meletiadis J, Saleem MD, Feitz WF, Heesakkers JP. Near-infrared spectroscopy of the urinary bladder during voiding in men with lower urinary tract symptoms: a preliminary study. Biomed Res Int. 2013;2013: 452857.
Macnab AJ, Stothers L. Development of a near-infrared spectroscopy instrument for applications in urology. Can J Urol. 2008;15(5):4233–40.
Stothers L, Guevara R, Macnab A. Classification of male lower urinary tract symptoms using mathematical modelling and a regression tree algorithm of noninvasive near-infrared spectroscopy parameters. Eur Urol. 2010;57(2):327–33.
Yurt M, Süer E, Gülpınar Ö, Telli O, Arıkan N. Diagnosis of bladder outlet obstruction in men with lower urinary tract symptoms: comparison of near infrared spectroscopy algorithm and pressure flow study in a prospective study. Urology. 2012;80(1):182–6.
Zhang P, Yang Y, Wu ZJ, Zhang CH, Zhang XD. Diagnosis of bladder outlet obstruction in men using a near-infrared spectroscopy instrument as the noninvasive monitor for bladder function. Urology. 2013;82(5):1098–102.
Chung DE, Lee RK, Kaplan SA, Te AE. Concordance of near infrared spectroscopy with pressure flow studies in men with lower urinary tract symptoms. J Urol. 2010;184(6):2434–9.
McRae LP, Bottaccini MR, Gleason DM. Noninvasive quantitative method for measuring isovolumetric bladder pressure and urethral resistance in the male: I. Experimental validation of the theory. Neurourol Urodyn. 1995;14(2):101–14.
Drinnan MJ, McIntosh SL, Robson WA, Pickard RS, Ramsden PD, Griffiths CJ. Inter-observer agreement in the estimation of bladder pressure using a penile cuff. Neurourol Urodyn. 2003;22(4):296–300.
Griffiths CJ, Harding C, Blake C, McIntosh S, Drinnan MJ, Robson WA, et al. A nomogram to classify men with lower urinary tract symptoms using urine flow and noninvasive measurement of bladder pressure. J Urol. 2005;174(4):1323–6 (discussion 1326; author reply 1326).
Bianchi D, Di Santo A, Gaziev G, Miano R, Musco S, Vespasiani G, et al. Correlation between penile cuff test and pressure-flow study in patients candidates for trans-urethral resection of prostate. BMC Urol. 2014;14(1):103.
Borrini L, Lukacs B, Ciofu C, Gaibisso B, Haab F, Amarenco G. Predictive value of the penile cuff-test for the assessment of bladder outlet obstruction in men. Prog Urol. 2012;22(11):657–64.
Parsons BA, Bright E, Shaban AM, Whitehouse A, Drake MJ. The role of invasive and non-invasive urodynamics in male voiding lower urinary tract symptoms. World J Urol. 2011;29(2):191–7.
• Ganpule AP, Batra RS, Shete NB, Singh AG, Sabnis RB, Desai MR. BPH nomogram using IPSS, prostate volume, peak flow rate, PSA and median lobe protrusion for predicting the need for intervention: development and internal validation. Am J Clin Exp Urol. 2021;9(3):202–10. This study provides us data about nomogram made of different parameters that can predict the need for surgical intervention.
Funding
This study was not supported by any fund.
Author information
Authors and Affiliations
Contributions
RBM: Literature review, Manuscript writing/editing YW: Manuscript revising and editing, quality control MM: Protocol/project development, Manuscript writing/editing, Supervising project.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics Approval
This article does not contain any studies with human or animal subjects performed by any of the authors and therefore required no inform consent.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ben Muvhar, R., Wagmaister, J. & Mekayten, M. Navigating the Diagnostic Maze: Unraveling the Non-invasive Evaluation of Bladder Outlet Obstruction in Men—a Comprehensive Systematic Review. Curr Bladder Dysfunct Rep 18, 318–332 (2023). https://doi.org/10.1007/s11884-023-00717-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11884-023-00717-3