
Abstract
Purpose of Review
This review explores the current literature surrounding non-surgical and surgical management strategies for urinary tract infections (UTIs) in adult patients with neurogenic lower urinary tract dysfunction. UTIs in patients with neurogenic bladders (NB) are recurrent and lifelong contributors to morbidity and mortality. Diagnosis and treatment of UTIs in this patient population are significantly more challenging and require thoughtful clinical decision-making. Topics such as risk factors, diagnosis, nonoperative treatment strategies, and surgical management will be discussed.
Recent Findings
Current recommendations indicate that only symptomatic UTIs require treatment. Nonoperative treatments such as antibiotic therapies, bladder instillations, and coated catheters are typically exercised before proceeding with more invasive surgical management. There are no clear guidelines to recommend when patients should or are required to have surgical intervention.
Summary
Non-surgical management strategies continue to evolve through recent clinical trials. Major surgical intervention is typically considered only after non-surgical options have been exhausted or based on patient and caregiver preference.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The lower urinary tract functions as a reservoir for urine and a mechanism for micturition. The urinary bladder and sphincter complex in conjunction with the central and peripheral nervous systems allow for achievement of voiding. Damage to these systems can result in discordance of urinary storage and emptying [1]. Neurogenic bladder is defined as bladder dysfunction secondary to impairment of the nervous system. Neurogenic bladder (NB) is most commonly caused by multiple sclerosis (MS) and spinal cord injury (SCI) (sacral nerve). Other frequently associated diagnoses include spina bifida (SB), cerebral palsy (CP), and Parkinson’s disease. Within these populations, certain patients carry a higher risk for long-term complications. The American Urological Association (AUA) Guidelines statement on urodynamics indicates that those with SB, SCI, high burden spinal cord disease, transverse myelitis, and men with MS have a greater predisposition for future complications. These complications include upper urinary tract deterioration such as end stage renal disease, pyelonephritis, and renal scarring as well as nephrolithiasis, refractory urinary incontinence, and malignancy, including a higher risk of squamous cell carcinoma of the bladder [2]. One of the most commonly implicated risk factors and the topic of this review are UTIs in the neuropathic bladder.
UTIs remain the most common infection in this patient population. A US database revealed that 29–36% of NB patients suffer from recurrent UTIs. Recurrent UTIs are defined as more than two infections occurring within a 6-month period or three infections in 12 months with complete resolution for at least 2 weeks [3]. Untreated infections increase the risk for urosepsis, renal deterioration, and poor psychological health. Multiple studies show that detrusor overactivity, poor bladder compliance, and vesicoureteral reflux put NB patients at increased risk for UTI. Typically, recommendations for treatment are limited to symptomatic UTIs in the effort to preserve antibiotic stewardship. Symptomatology in the NB population differs from the symptoms commonly experienced by those patients with functionally intact nervous systems due to the insensate nature of their urinary tract secondary to their underlying neurological disorder. Common symptoms in the NB population include fever, urinary incontinence, spasticity, malaise, cloudy urine, foul urine odor, back and bladder pain, dysuria, and autonomic dysreflexia [4]. In these patients, the choice of antibiotic and length of treatment are primarily based on culture sensitivities, local antibiograms, and provider experience. Prophylactic management options such as bacterial probiotics, bladder irrigation, intravesical botulinum toxin, and antibiotic prophylaxis are currently being explored [1]. The decision to seek surgical management is also an option for patients who are refractory to treatment.
Risk Factors and Current Hypotheses
The detrusor muscle, urinary sphincter complex, and nervous system must work synergistically for micturition to occur. When the neurologic connection to the pontine micturition center (PMC) is damaged, the patient may experience an inability to relax urinary sphincters known as detrusor sphincter dyssynergia (DSD) leading to incomplete bladder emptying and urinary retention. PMC damage may also cause overactive bladder symptoms (OAB) due to loss of urinary reflex [5]. Damage to the pelvic nerves may also lead to desensitization and detrusor areflexia which typically manifests as urinary retention and overflow incontinence. Essentially, the neurogenic bladder lacks the ability to respond appropriately to urinary stimuli, thus, eliminating the most important inherent defense against infection: voiding. One current hypothesis implies that increased intravesical pressure due to bladder overdistension leads to bladder ischemia which predisposes NB patients to infection. The elevated bladder pressure causes tissue hypoperfusion and impedes the delivery of inflammatory cells and antibiotics. These findings are supported by studies that reveal fewer UTIs with improved urodynamic parameters in NB patients [4].
Bladder Drainage
Catheterization is the mainstay of management for NB. Data demonstrates that these medical devices represent a nidus for recurrent UTIs due to urethral trauma and irritation. Among these, indwelling catheters carry the highest risk.
Urolithiasis
UTIs are independent risk factors for the development of urolithiasis in NB patients due to urinary stagnation and persistent bacteriuria [2]. Stone disease, both obstructing and non-obstructing, can increase the risk for recurrent infections. One retrospective study showed that in a cohort of asymptomatic patients with non-obstructive renal stones and recurrent UTIs, approximately 50% of patients were infection free following surgical removal [6]. The use of bladder drainage devices in the NB population also increases the risk for stone disease. It is important to consider the possibility of urolithiasis if the infection persists following appropriate antibiotic therapy, if the culture is positive for urease-producing organisms, or if urinary catheters exhibit crusting or obstruction. In such cases, a workup including cystoscopy and upper tract imaging are encouraged.
Immune Dysfunction
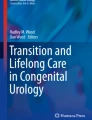
Current hypotheses suggest that immune dysfunction in SCI patients with NB may predispose to UTIs. Decreased proinflammatory responses to uropathogenic Escherichia coli (UPEC) and subsequent inappropriate suppression of inflammatory factors were analyzed in a rat model study leading to continuous bacterial replication. Patients on immunosuppressive therapies, such as MS patients, may also experience increased infection rates as a result of immune dysfunction [1]. Figure 1 illustrates the factors affecting UTI predisposition in NG patients.

Management schema for UTIs in neurogenic bladder patients
Common Infectious Organisms
In the NB population, the most commonly isolated organisms are E. coli and Klebsiella species. The Pseudomonas, Acinetobacter, and Enterococcus species are also often seen in the NB population due to frequent hospitalizations. NB patients with recent antibiotic use and/or indwelling catheters (IC) are also more susceptible to fungal infections. A large prospective study of SCI patients demonstrated the rate of candida UTI to be 10× higher in those patients with indwelling catheters and suprapubic catheters (SPC) compared to those who used clean intermittent catheterization (CIC). Figure 2 illustrates the distribution of commonly implicated organisms associated with NB-UTIs [4].

Infectious pathogens in complicated and uncomplicated UTIs
Diagnosis
When working up a NB patient, the objective is to characterize the severity of dysfunction of the urinary tract secondary to the underlying neurologic concern. These patients are typically assessed with multiple and frequent diagnostic tests including urinalysis, urine culture and cytology, PVR, ultrasonography, urodynamic studies, uroflowmetry, and pelvic floor neurophysiology [2].
UTI Diagnosis and Surveillance
In patients with neuropathic bladders, between 50 and 75% of urine cultures will be positive regardless of symptomatic or asymptomatic status [7]. Over the years, this has led to overdiagnosis and poor antibiotic stewardship within this population. As a result, antibiotic-resistant organisms are being cultured more frequently. Several organizations have attempted to provide definitions for UTIs in neuropathic bladders in order to clarify treatment parameters. Notably, no consensus has been established. The Infectious Disease Society of America [8] published their definition of a catheter-associated UTI as having signs and symptoms of an infection and ≥103 colony forming units (CFU) of at least one bacterial species in a single catheterized urine sample [7]. The National Institute on Disability and Rehabilitation Research offers their guidelines for UTI diagnosis in NB-SCI patients as pyuria and UTI symptoms plus greater than 102 CFU/mL from an intermittent catheterized specimen, or greater than 104 CFU/mL from a condom catheter, or any value from indwelling and suprapubic catheters [1].
In the NB population, it may be difficult to differentiate the acute UTI symptomatology from chronic bladder pain. However, one study showed that NB-SCI patients are able to predict the presence of an UTI with a positive predictive value of 32.6% and predict the absence of UTIs with a negative predictive value of 82.8%. The study demonstrated that malodorous urine was a poor predictor for UTIs with a low sensitivity of 48.3%. The same study revealed that the presence of pyuria had the highest sensitivity in predicting UTIs and its absence strongly disproves UTIs as the cause of the symptomatology [1].
Asymptomatic bacteriuria in NB patients is another important consideration. The majority of the organisms that grow at baseline in NB patients are those most commonly identified on standard urine culture. This explains the elevated incidence of ABU in these patients. The IDSA guidelines regarding ABU in patients with SCI, patients with short-term indwelling catheters (<30 days), and those with SPTs and long-term indwelling catheters strongly recommend against screening or treating ABU. There are no current recommendations from the IDSA for or against screening or treating ABU at the time of catheter removal [8].
Nonoperative Treatment
Antibiotic Therapies
Culture-specific, narrow-spectrum antibiotics are recommended for the treatment of UTIs in NB patients. For cases of uncomplicated cystitis, nitrofurantoin is suggested due to lower resistance rates and effect on enteric flora. Fluroquinolones are recommended for more severe infections. Duration of therapy is another important consideration. Because neuropathic bladder UTIs are considered complicated, single-shot or short-term antibiotic treatments are not recommended. Further investigation demonstrates efficacy in 7–10-day antibiotic treatment for afebrile UTIs and 14-day therapy for febrile UTIs. Recommendations insist on extending the duration of therapy if organ involvement is present [9•]. In the case of SCI-NB patients with UTIs, current recommendations are 5 days of antibiotic therapy such as nitrofurantoin or trimethoprim for chronic afebrile UTIs and 7 days of fluroquinolones or cefuroxime for acute, afebrile exacerbations. Febrile UTIs should be treated for 14 days with broad spectrum intravenous coverage [1]. In NB patients with CA-UTIs secondary to indwelling Foley catheters, the IDSA recommends early catheter exchange and 7–14 days of culture-specific antibiotics [1]. Recent studies support longer treatment durations as necessary in NB patients to prevent infectious relapses.
Antibiotic Prophylaxis
Routine antibiotic prophylaxis is not recommended in the NB population for UTI prevention due to increases in bacterial resistance and lack of evidence to support long-term benefits. Moreover, the current literature does not support antibiotic prophylaxis for UTI prevention in patients using CIC. Presently, antibiotic-altering proteins are being researched to augment antimicrobial treatments. The supplementary enzymes bromelain and trypsin are hypothesized to enhance antibiotic efficacy. However, only limited evidence is available to support this research at this time [10]. Weekly oral cycling antibiotics (WOCA) has recently been a topic of interest. WOCA is a regimen consisting of two antibiotics administered once a week for a 2-year period at minimum. Evidence shows a significant reduction in the number of UTIs annually and no adverse events [9•]. A 2019 study reveals the effectiveness of WOCA prophylaxis in NB-SCI patients with recurrent UTIs. In the cohort, the regimen was well tolerated, and no antibiotic resistance was observed on enteric and nasal cultures [11••].
Coated Catheters
The current standard of care in patient with neuropathic bladders is CIC. Indwelling catheters are more commonly associated with infection, stone disease, and urinary tract deterioration.
New catheter modifications are designed to prevent biofilm formation, a common source for UTI development in neuropathic bladders. Researchers have been studying the incorporation of antifouling and biocidal materials into biocompatible, antimicrobial catheter coatings.
Antifouling materials utilize steric and electrostatic repulsion to prevent bacterial attachment to surfaces and biofilm formation but do not directly kill bacteria. The two main types of antifouling materials are hydrophilic materials and polyzwitterions. Several studies demonstrate the efficacy of these materials. On the other hand, biocidal materials directly kill microbes, and this type of coating is especially useful in preventing catheter encrustation. Clinically tested biocidal materials include antibiotics and silver ions. Silver alloy is an FDA-approved antimicrobial agent for urinary catheter coatings. They have been studied extensively in the past and exhibited drawbacks such as restricted efficacy as an antimicrobial agent in urinary catheters, cytotoxicity, and high costs [12]. A 2017 clinical study evaluated the efficacy of urinary catheters impregnated with a synergistic composite of amikacin, nitrofurantoin, and silver nanoparticles (SNP) in preventing biofilm formation. After 2 years, the cohort of patients who received catheters impregnated with both antibiotics and SNPs demonstrated 90% inhibition of microbial adhesion compared to 25% inhibition in the cohort who used only antibiotic impregnated urinary catheters [13••]. This combination appears to be a superior way to limit biofilm formation and decrease multi-drug-resistant uropathogens. Many biocidal and antifouling agents still remain under research such as chlorhexidine, triclosan, antimicrobial peptides, bacteriophages, enzymes, nitric oxide, and liposomes.
Bladder Instillations
Prophylactic antibiotic bladder instillations have provided an optimistic future in the management of NB. Daily intravesical instillations have proven to be superior to oral antibiotic therapies for the prevention of recurrent UTIs in the NG population due to unchanged rates of drug resistance in urinary microbes following bladder instillations. In fact, studies show that urinary microorganisms have become less multidrug-resistant after instillations [14]. Neomycin-polymyxin and gentamicin are commonly used antibiotics for intravesical instillation. A prospective study between 2014 and 2017 of 63 adults with recurrent multi-drug-resistant pathogenic UTIs treated with daily intravesical gentamicin demonstrated a reduction in the average number of UTIs from 4.8 to 1. The resistance rate of urinary pathogens decreased from 78 to 23% indicating that intravesical antibiotic instillations reduce the number of recurrent UTIs and the antibiotic resistance [15••]. A 2019 randomized controlled trial examined the effects of platelet rich plasma bladder instillations in a cohort of women with recurrent bacterial cystitis. The study showed a significant decrease in infectious recurrences up to 12 months after the instillation without adverse events [16]. Similarly, a 2020 case series compared 12 patients who were treated with gentamycin or tobramycin bladder instillations and found that the average rate of UTIs decreased from a median of 2.5 to 1.5 and both the number of pathogen types and antibiotic resistance also demonstrated significant decrease [17•]. However, the current data in adults remains largely heterogenous and requires further investigation specifically focused on NB patients.
Probiotics and Oral Preventative Strategies
Bacterial probiotic supplements are currently theorized to prevent UTIs in neurogenic bladders. However, the data in this field is minimal. A Cochrane review compared 3 studies data up to 2017 and failed to identify any supporting evidence that supported oral probiotics an effective prophylactic strategy in NB patients. These studies also examined the intravesical instillation of 2 strains of nonvirulent E. coli and concluded that while there was little harm associated with the treatment, there was also limited evidence to prove beneficial [18]. A 2019 randomized controlled trial failed to prevent UTIs in patients with SCI-NB when compared to a placebo [19]. Supplements such as D-mannose, ascorbic acid, and methenamine hippurate have shown poor long-term prevention of UTIs in clinical studies [20].
Botulinum Neurotoxin
Since its approval for use in OAB, botulinum toxin A has gained popularity among researchers and clinicians. Intravesical injection of the toxin allows for the reduction of detrusor pressures and thus decreases the risk for future infections. A study analyzing SCI-NB patients revealed that administration of the toxin resulted in a reduction of total UTIs in the cohort [1]. Future studies with larger patient cohorts are required to validate this data further but the potential for UTI prophylaxis in neuropathic bladders remains promising.
Sacral Neuromodulation Devices
The sacral neuromodulation (SNM) device commercially available is called InterStim (Medtronic, Minneapolis, MN, USA). The implant functions by stimulating the sacral nerve root to suppress detrusor overactivity. Although it is clear that these SNM devices require continued research, their ability to control urinary symptoms may theoretically decrease recurrent UTIs in this patient population.
Surgical Management
There are no clear guidelines to recommend when patients should or need to have surgical intervention related to recurrent UTIs in the neurogenic bladder. Major surgical intervention such as cystectomy/enteric conduit is usually considered only after non-surgical options have been exhausted or based on patient and caregiver preference. Surgical intervention can range from relatively simple operations such as bladder neck closure and suprapubic tube placement, to more complex reconstructive procedures such as enterocystoplasty, ileovesicostomy, and enteric conduit with or without cystectomy. We will focus on cystectomy and ileal conduit in this review.
If a patient should desire to undergo a urinary diversion with ileal conduit as management for recurrent UTIs, they must be counseled on the risks associated with this surgery. Pyelonephritis and pyocystitis are not infrequent complications, and in a recent study published in 2020, a cohort of neurogenic bladder patients who were followed for a median time of 8 years, and a significant percentage (60%) were hospitalized with urosepsis after their surgery during that time span [21•]. Pyocystitis of the native bladder can occur when ileal conduit is performed without concurrent cystectomy. Past studies have quoted rates of pyocystitis as high as 52% in those who did not undergo cystectomy at time of urinary diversion [22]. A recent study published in 2016 out of Vanderbilt noted that concurrent cystectomy at time of ileal conduit rates for benign conditions such as neurogenic bladder has increased over the 13 years from about 20 to 35% across the nation [23]. Performing cystectomy at time of ileal conduit does add morbidity to the surgery. A 2015 study that analyzed patients undergoing cystectomy for refractory lower urinary tract symptoms noted a 30-day complication rate of almost 66% [24]. Another study published in 2018 out of Paris, France, evaluated 102 patients who underwent non-continent urinary diversion for neurogenic bladder related to spinal cord injury [25••]. These patients had failed conservative management or had elected for diversion. The rate of early (<30 days post op) pyelonephritis was 12.7%. The rate of late (>30 days) infectious complications in this group (pyocystitis or pyelonephritis) were about 10%. All 3 patients who developed pyocystitis underwent delayed cystectomy. These are not insignificant numbers, especially for patients who may be choosing to undergo a procedure with significant morbidity in attempt to avoid recurrent infections. These factors must be considered when counseling patients who desire urinary diversion.
Conclusion
By definition, UTIs in the neurogenic bladder are considered complicated infections. Current recommendations indicate that only symptomatic UTIs require treatment. Nonoperative treatments such as antibiotic therapies, bladder instillations, and coated catheters are typically exercised before proceeding with more invasive surgical management. Surgical intervention such as cystectomy/enteric conduit should only be considered after non-surgical options have been exhausted or based on patient and caregiver preference.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
McKibben M, Seed P, Ross S, Borawski K. Urinary tract infection and neurogenic bladder. Urol Clin N Am. 2015;42:527–36. https://doi.org/10.1016/j.ucl.2015.05.006.
Nseyo U, Santiago-Lastra Y. Long-term complications of the neurogenic bladder. Urol Clin N Am. 2017;44:355–66. https://doi.org/10.1016/j.ucl.2017.04.003.
Bergamin P, Kiosoglous A. Non-surgical management of recurrent urinary tract infections in women. Transl Androl Urol. 2017;6:S142–52. https://doi.org/10.21037/tau.2017.06.09.
Vigil HR, Hickling DR. Urinary tract infection in the neurogenic bladder. Transl Androl Urol. 2016;5(1):72–87. https://doi.org/10.3978/j.issn.2223-4683.2016.01.06.
Vurture G, Peyronnet B, Palma J, et al. Urodynamic mechanisms underlying overactive bladder symptoms in patients with parkinson disease. Int Neurourol J. 2019;23:211–8. https://doi.org/10.5213/inj.1938086.043.
Ragab M, Yang B, Davies M. Urinary tract infections of the neurogenic bladder. Female Urinary Tract Infections in Clinical Practice. 2019;2020:85–97. https://doi.org/10.1007/978-3-030-27909-7_14.
Forster C, Pohl H. Diagnosis of urinary tract infection in the neuropathic bladder: changing the paradigm to include the microbiome. Top Spinal Cord Inj Rehabil. 2019;25:222–7. https://doi.org/10.1310/sci2503-222.
Nicolle L, Gupta K, Bradley S, et al. Clinical practice guideline for the management of asymptomatic bacteriuria: 2019 update by the Infectious Diseases Society of America. Clin Infect Dis. 2019. https://doi.org/10.1093/cid/ciy1121.
• Pannek J, Wöllner J. Management of urinary tract infections in patients with neurogenic bladder: challenges and solutions. Res Rep Urol. 2017;9:121–7. https://doi.org/10.2147/RRU.S113610Summarizes current strategies for diagnosis, prophylaxis, and treatment of urinary tract infections in patients with neurogenic bladder.
Linsenmeyer T. Catheter-associated urinary tract infections in persons with neurogenic bladders. J Spinal Cord Med. 2018;41:132–41. https://doi.org/10.1080/10790268.2017.1415419.
•• Dinh A, Hallouin-Bernard M, Davido B, et al. Weekly Sequential antibioprophylaxis for recurrent urinary tract infections among patients with neurogenic bladder: a randomized controlled trial. Clin Infect Dis. 2019. https://doi.org/10.1093/cid/ciz1207This trial assessed the efficacy of weekly oral cyclic antibiotic prophylaxis in preventing recurrent urinary tract infections in patients with neurogenic bladder as a result of spinal cord injury.
Singha P, Locklin J, Handa H. A review of the recent advances in antimicrobial coatings for urinary catheters. Acta Biomater. 2017;50:20–40. https://doi.org/10.1016/j.actbio.
•• Mala R, Annie Aglin A, Ruby Celsia A, Geerthika S, Kiruthika N, VazagaPriya C, et al. Foley catheters functionalised with a synergistic combination of antibiotics and silver nanoparticles resist biofilm formation. IET Nanobiotechnol. 2017;11:612–20. https://doi.org/10.1049/iet-nbt.2016.0148This trial studied the efficacy of urinary catheter impregnation with a combination of antibiotics and silver nanoparticles in preventing biofilm formation.
Huen K, Nik-Ahd F, Chen L, Lerman S, Singer J. Neomycin-polymyxin or gentamicin bladder instillations decrease symptomatic urinary tract infections in neurogenic bladder patients on clean intermittent catheterization. J Pediatr Urol. 2019;15:178.e1–7. https://doi.org/10.1016/j.jpurol.2018.12.001.
•• Stalenhoef J, van Nieuwkoop C, Menken P, Bernards S, Elzevier H, van Dissel J. Intravesical gentamicin treatment for recurrent urinary tract infections caused by multidrug resistant bacteria. J Urol. 2019;201:549–55. https://doi.org/10.1016/j.juro.2018.10.004This trial showed the value of intravesical gentamicin instillation in reducing urinary tract infections and antimicrobial resistance for patients with refractory recurrent urinary tract infections.
Mirzaei M, Daneshpajooh A, Farsinezhad A, Jafarian Z, Ebadzadeh MR, Saberi N, et al. The therapeutic effect of intravesical instillation of platelet rich plasma on recurrent bacterial cystitis in women: a randomized clinical trial. Urol J. 2019;6:609–13. https://doi.org/10.22037/uj.v0i0.5239.
• Chernyak S, Salamon C. Intravesical antibiotic administration in the treatment of recurrent urinary tract infections. Female Pelvic Med Reconstr Surg. 2020;26:152–4. https://doi.org/10.1097/SPV.0000000000000810This case series compared the rate of urinary tract infections before and after intravesical antibiotic instillations.
Lucas E. Medical management of neurogenic bladder for children and adults: a review. Top Spinal Cord Inj Rehabil. 2019;25:195–204. https://doi.org/10.1310/sci2503-195.
Toh S, Lee B, Ryan S, et al. Probiotics [LGG-BB12 or RC14-GR1] versus placebo as prophylaxis for urinary tract infection in persons with spinal cord injury [ProSCIUTTU]: a randomised controlled trial. Spinal Cord. 2019;57:550–61.
Castle A, Park A, Mitchell A, Bliss D, Gelfand J, De E. Neurogenic bladder: recurrent urinary tract infections—beyond antibiotics. Curr Bladder Dysfunct Rep. 2018;13:191–200. https://doi.org/10.1007/s11884-018-0481-4.
• Husmann D, Viers B. Neurogenic bladder: management of the severely impaired patient with complete urethral destruction: ileovesicostomy, suprapubic tube drainage or urinary diversion—is one treatment modality better than another? Transl Androl Urol. 2020;9:132–41. https://doi.org/10.21037/tau.2019.09.06This study examined surgical complications in the management of patients with neurogenic bladder and complete urethral destruction.
Singh G, Wilkinson J, Thomas D. Supravesical diversion for incontinence: a long-term follow-up. BJU Int. 1997;79:348–53. https://doi.org/10.1046/j.1464-410x.
Brown E, Osborn D, Mock S, Ni S, Graves A, Milam L, et al. Temporal trends in conduit urinary diversion with concomitant cystectomy for benign indications: a population-based analysis. Urology. 2016;98:70–4.
Al Hussein Al Awamlh B, Lee D, Nguyen D, Green D, Shariat S, Scherr D. Assessment of the quality-of-life and functional outcomes in patients undergoing cystectomy and urinary diversion for the management of radiation-induced refractory benign disease. Urology. 2015;85:394–40. https://doi.org/10.1016/j.urology.2014.08.047.
•• Guillot-Tantay C, Chartier-Kastler E, Perrouin-Verbe M, Denys P, Léon P, Phé V. Complications of non-continent cutaneous urinary diversion in adults with spinal cord injury: a retrospective study. Spinal Cord. 2018;56:856–62. https://doi.org/10.1038/s41393-018-0083This study examined long-term complications in adult spinal cord injury patients who underwent urinary diversion.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Neurogenic Bladder
Rights and permissions
About this article

Cite this article
Delgado, J., Heilbronn, C. & Mellon, M.J. Urinary Tract Infection in the Neurogenic Bladder: an Update of Surgical and Non-surgical Management. Curr Bladder Dysfunct Rep 16, 34–40 (2021). https://doi.org/10.1007/s11884-021-00628-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11884-021-00628-1