
Opinion Statement
In patients with early-stage cervical cancer, radical hysterectomy and pelvic lymphadenectomy is the gold standard. However, this disease commonly affects women of childbearing age; thus an option to spare fertility is ideal. This option came to fruition in the early 90s when the Dargent procedure or radical trachelectomy was first reported. The procedure has subsequently been modified as technology has improved and now may be performed via minimally invasive techniques. Additionally, with the advent of the sentinel lymph node procedure, the morbidity in this usually young patient population has continued to improve. There is a multitude of data to show that oncologic outcomes, concerning recurrence and mortality, are comparable to radical hysterectomy, as well as obstetrical outcomes are favorable. Data to support its acceptance within the gynecologic oncology community has led to radical trachelectomy being implemented into governing body guidelines and should be offered to appropriate candidates with early-stage cervical cancer who wish to preserve fertility.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
About 13,240 new cases of cervical cancer will be diagnosed and approximately a third of these patients will die of their disease in the year 2018 [1]. Approximately 50% are diagnosed with early-stage disease, defined as tumors 4 cm or less that are confined to the cervix. Overall, women diagnosed with cervical cancer have a 5-year survival rate of 66.2% [2]. Patients with localized disease have a much more favorable prognosis, with a 5-year relative survival rate of 91.7%. Unfortunately, in the USA, only 46% of women are diagnosed with locally confined disease.
Experience and randomized studies have demonstrated that patients with locally confined disease (stage IA2-IB1), without lymph node metastases, may successfully be treated with radical surgery. Surgery typically includes radical hysterectomy and bilateral pelvic lymphadenectomy. This requires removal of the uterus, cervix, and radical excision of the upper vagina and parametria, which eliminates the potential for childbearing. However, as this disease commonly afflicts young women with approximately 38% of women being diagnosed at 45 years or less, these patients may be candidates for fertility-sparing options, such as radical trachelectomy [2].
Radical trachelectomy was developed in 1987 by French surgeon Dr. Daniel Dargent for the treatment of early invasive cervical cancer in order to preserve fertility. He reported on the first radical vaginal trachelectomy. Since that time, over 1000 procedures have reportedly been performed worldwide [3]. This procedure can be performed by multiple approaches including abdominally, vaginally, laparoscopically, and robotically.
In this article, we will review pre-operative considerations, the surgical technique, and common post-operative complications. Additionally, we will review the recent literature with regard to oncologic and fertility outcomes.
Patient selection and pre-operative assessment
Criteria used to determine appropriate candidates for radical trachelectomy have remained similar to when the procedure was first described, and include the following:
-
Reproductive age, typically < 40–45 years of age
-
Squamous carcinoma or adenocarcinoma histology; rare histologies (small cell neuroendocrine, gastric type adenocarcinoma, and adenoma malignum) are not considered suitable for fertility-sparing surgery
-
Stages IA1 with lymphovascular space invasion, IA2, or IB1
-
Tumor size 2 cm or less
-
No evidence of lymph node spread
-
No history of fertility impairment
-
Strong desire to preserve fertility
-
Imaging (pelvic MRI) to rule out upper endocervical involvement
Using these criteria, Sonoda and colleagues evaluated 186 patients < 40 years of age who had undergone radical hysterectomy and determined that 48% would have been eligible for a radical trachelectomy [4]. However, in approximately 14% of cases, the procedure would need to be abandoned because of unexpected disease spread. Criteria for aborting the procedure include a positive endocervical margin not amenable to further resection, positive lymph nodes, or a lesion that is larger than originally anticipated, although this is less likely given improvements in pre-operative imaging techniques.
Pre-operative imaging is crucial in the assessment of tumor size and location with respect to its distance from the internal os, as well as assessing the presence of distant metastases. Magnetic resonance imaging (MRI) plays a vital role in the pre-operative assessment of potential candidates for radical trachelectomy as it allows determination of tumor size, extension into the endocervical canal, and the length of the canal. The reported staging accuracy of MRI compared to physical exam ranges from 75 to 99%, but the superiority of MRI truly lies in its ability to detect the tumor-free distance from the internal os. MRI has a high specificity of 98% and positive predictive value of 95% for predicting the distance between the tumor and the internal os of less than or equal to 5 mm [5].
Surgical technique
Vaginal approach
As discussed previously, the vaginal approach has been well documented [6]. Retroperitoneal or laparoscopic pelvic lymphadenectomy is first performed, as in all approaches, consisting of the removal of the lymph node bearing tissue between the distal one-half of each common iliac artery, the anterior and medial aspect of the proximal half of the external iliac artery and vein, and the distal half of the obturator fat pad anterior to the obturator nerve. The pelvic lymph nodes may be assessed with a complete lymphadenectomy or via sentinel lymph node mapping, which will be discussed in a subsequent section.
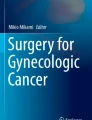
Once the pelvic lymph nodes have been excised, the vaginal approach begins with the excision of 1–2 cm of vaginal mucosa around the cervix. The anterior and posterior edges are then used to cover the cervix in the midline. The vesicovaginal space is developed anteriorly and the paravesical spaces laterally to identify the bladder pillars. The ureters are palpated and identified. The posterior cul-de-sac is opened and the pararectal spaces are identified and the proximal uterosacral ligaments are excised. After relocation of the ureters, the parametrial tissue up to the level of the isthmus is excised. The cervical or descending branch of the uterine artery is ligated. The radical trachelectomy specimen with pelvic nodes is excised approximately 1 cm below the internal os [Fig. 1]. In order to keep the canal patent and prevent canalicular stenosis, a Foley or Malecot catheter may be placed into the uterus and sutured in place. An endocervical cerclage is placed and the vaginal mucosa is reapproximated to the new ectocervix with either interrupted or running sutures.

Radical trachelectomy specimen with pelvic nodes
Abdominal approach
The abdominal radical trachelectomy was described in 1997 by Smith et al., but has subsequently been modified [7, 8]. Entry into the abdomen may be via a midline vertical incision or transverse abdominal incision with a Maylard or Cherney incision to have adequate access to the pelvis. After excising the pelvic lymph nodes, the paravesical and pararectal spaces are developed. The round ligaments in most instances are divided, but may be preserved. The round ligaments are grasped with Kelly clamps for uterine manipulation and the vesicocervical space is developed to dissect the bladder off the cervix. Care is taken to preserve the infundibulopelvic and utero-ovarian vessels as this is the main blood supply for the remaining uterus. Once a complete ureterolysis is performed to the tunnel of Wertheim, the uterine vessels are divided at their origin from the hypogastric vessels. The parametria and paracolpos are mobilized with the trachelectomy specimen. The posterior cul-de-sac is incised and the uterosacral ligaments are divided at their origin. The vagina is then incised to perform an anterior colpotomy, 1–2 cm distal to the external cervical os. This is then carried circumferentially until the specimen is completely separated from the vagina. This step may be facilitated with the use of a vaginal delineator, such a McCartney tube™ or other vaginal cylinder. The lower uterine segment is estimated and clamps are placed at the level of the internal os. The cervix is then incised with a knife approximately 5 mm below the internal os. As in the vaginal approach, patency of the remaining cervical canal may be achieved with the use of a Foley or Malecot catheter followed by the placement of an endocervical cerclage. The lower uterine segment is then sutured to the vaginal mucosa via interrupted or continuous sutures.
Minimally-invasive (laparoscopic and robotic) approach
The steps with either a laparoscopic or robotic approach are the same with regards to the abdominal approach. However, advances in minimally invasive surgery have allowed the performance of many procedures with the advantages provided by this approach. Namely, minimally invasive surgery has allowed for reduced length of hospital stay, reduced blood loss, decreased analgesic requirements, decrease in blood transfusion rates, decrease in complication rates, earlier recovery of physiological functions, and improved esthetic outcomes [9].
In addition to improvements in post-operative recovery, it differs by the ability to identify the ascending and descending branches of the uterine artery given the improved visualization provided by the laparoscope. This allows individual ligation of the descending branches to preserve blood supply of the isthmic portion of the uterus.
As in most cases, the round ligament is preserved, the decision to utilize a uterine manipulator is individualized given the patient and tumoral characteristics, but can ease manipulation of the uterus. The use of a colpotomizer also allows easy delineation of the vagina, improved development of the vesicocervical and vesicovaginal spaces, and provides assistance when determining the distance from the external os when performing the upper vaginectomy [Fig. 2].

Upper vaginectomy—margin
Trocar placement for a laparoscopic radical trachelectomy approach typically can be accomplished with 5 mm trocars, although some may prefer a 12 mm midline trocar for a use of 10-mm camera. A central supra-umbilical trocar and three accessory trocars should suffice and the arrangement is similar to a traditional robotic hysterectomy [Fig. 3].

Trocar placement for a laparoscopic and/or robotic radical trachelectomy
Other surgical considerations
Frozen section
Frozen section of the trachelectomy specimen is advocated to ensure an acceptable tumor-free margin has been obtained [10,11,12]. The recommended tumor clearance is at least a 5 mm margin [13]. If this is not achieved, either additional cervical tissue may be excised, if anatomically feasible, or a completion hysterectomy would need to be performed. Frozen section of any suspicious pelvic nodes should be performed prior to beginning a radical trachelectomy to ensure there is no metastatic disease as this would be an indication to abort a fertility-sparing procedure.
Sentinel lymph nodes
Evaluation of the pelvic lymph nodes in patients with early stage cervical cancer should be performed. In these patients, the risk of nodal metastasis is as high 15–20% and pelvic lymphadenectomy is generally sufficient, as the risk of para-aortic nodal metastases is small [14]. More recently and increasing in favor is the use of sentinel lymph node mapping and biopsy to decrease post-operative morbidity in patients up to stage IB1 disease. The SENTICOL study was a multicenter prospective evaluation of patients with stage IA1 disease with lymphovascular space invasion to stage IB1 to assess the accuracy of this procedure [15]. The sentinel lymph node mapping procedure in the 136 patients had a 98.2% negative predictive value, and in the patients who mapped bilaterally, there was a 0% false-negative rate. Emphasis must be placed on the fact that if a hemi-pelvis does not map, a side specific complete lymphadenectomy should be performed to maintain these high rates of reliability, as well as any suspicious lymph nodes, regardless of mapping, should be removed. Additionally, although this technique has been used in tumors up to 4 cm, the best detection and mapping rates are from patients with tumors that are 2 cm or less. Although frozen section should be performed on suspicious lymph nodes to determine if a fertility-sparing procedure should be continued, frozen section on sentinel lymph nodes has poor diagnostic value [16]. Nonetheless, the sentinel lymph node procedure should be considered in this cohort of patients undergoing fertility-sparing surgery for early stage cervical cancer [17].
Cerclage
Cervical cerclage following radical trachelectomy has not always been considered standard [18]. It is now well established that placement of a cervical cerclage at the time of radical trachelectomy plays an important role in preventing premature dilatation of the residual uterine cervical canal and the subsequent occurrence of preterm premature rupture of membranes (PPROM) [19]. The type of suture used to perform the cerclage varies among different reports, including braided and non-braided sutures. No randomized trials have evaluated the optimal suture material. Braided sutures are notable for their strength and ease of removal. Unfortunately, the braided material provides an environment for bacterial incorporation, which is a known contributor to preterm birth [20•]. In contrast, non-braided suture exhibits less tissue reactivity and some data may suggest improved successful pregnancy rates with non-braided sutures (e.g., Nylon ® and Prolene®) [21]. In addition, conventionally, the knot of the cerclage is tied posteriorly to avoid a theoretical risk of erosion into the bladder, but this also has not been evaluated in a randomized trial.
Uterine artery preservation
One of the most frequently debated issues is whether uterine artery preservation should be the norm when performing radical trachelectomy or whether it is safe to transect the uterine vessels. Several authors have addressed uterine perfusion after radical trachelectomy. The first report, from Tang et al. [22], including 26 patients (the uterine arteries were preserved in 16 and ligated in 10 of them) who underwent computed tomography angiography (CTA), demonstrated 87.2% rate of unilateral or bilateral uterine artery occlusion when these vessels were spared.
More recently, Escobar et al. measured and analyzed uterine perfusion utilizing laser angiography with ICG during uterine artery sparing and non-sparing radical trachelectomy. Based on real-time intraoperative angiography observations, the authors concluded that there is no need to preserve the uterine artery during radical trachelectomy to maintain uterine viability. [23•].
Post-operative morbidity
Surgical outcomes of radical trachelectomy indicate that it is a safe procedure with comparable complication rates to radical hysterectomy. In a systematic review comparing peri-operative morbidity of laparotomic radical trachelectomy (n = 143) and hysterectomy (n = 186), the rates of intraoperative and postoperative complications were similar for both groups (intraoperative complications 3.5 and 1.1%, respectively; postoperative complications 35.7 and 33.3, respectively) [24]. The only significant difference seen was in median operative time (155 vs 115 min, respectively). These findings are similar to other studies across all approaches of radical trachelectomy to radical hysterectomy [25,26,27, 28••].
A common complication of radical trachelectomy is the development of cervical stenosis, which is seen in up to 10–15% of patients [21, 27, 29, 30]. In a series of patients who underwent robotic radical or abdominal trachelectomy, the rate of cervical stenosis prior to the use of an intrauterine cannula (Smitt sleeve) was 14%, and after implementation, the rate was reduced to 0% [27]. In a review of 1547 patients undergoing radical trachelectomy, in whom 424 or 27% used anti-stenosis tools, the incidence of cervical stenosis was 4.6% with and 12.7% without, a significant difference [21]. The most frequently used tool to prevent stenosis was a catheter in 68% of patients. Most catheters are kept for a minimum of 3–5 days, but range to as long as 8 weeks. The use of anti-stenosis tools, most commonly a catheter, is advocated by the authors to prevent cervical stenosis.
Oncologic outcomes
There is a strong body of literature to suggest that the oncologic outcomes following radical trachelectomy are comparable to radical hysterectomy for tumors of similar size when meticulous surgical technique is used. Maintaining strict criteria for patient selection is of paramount importance as unusual recurrences are seen in patients with larger tumor sizes and unusual histologies [18, 31, 32].
Numerous studies have proven that radical trachelectomy can obtain a similar death rate compared to radical hysterectomy and is a safe alternative for fertility conservation. Initial reviews of the procedure suggested recurrence rates of 4.5% and mortality rates of 3%. In the largest meta-analysis of oncologic outcomes in patients undergoing radical trachelectomy, which included 2479 patients, with regards to recurrence and mortality, the rates are similar at 2.3% and 0.7%, respectively [33••]. Follow-up ranged from 9 to 96 months and 81.4% of the patients had follow-up greater than 2 years. A sampling of the literature used to compose these numbers is included in Table 1.
Fertility and obstetrical outcomes
There have been hundreds of pregnancies reported, mostly with the vaginal approach, but increasingly now with the abdominal approach. First trimester miscarriage rates are similar to the general population at under 20% [Table 2]. Interestingly enough, as many patients undergo this procedure for fertility preservation, a 5% elective termination rate is seen. Although the 2nd trimester miscarriage rate for patients undergoing radical trachelectomy is higher than in the general population, 10% vs 3%, respectively, almost 70% of pregnancies reach the 3rd trimester. Of those, 85% will result in delivery after 32 weeks gestation, with the majority reaching term (> 37 weeks gestation). In total, a large systematic review of the wide body of literature reporting on obstetrical outcomes in patients undergoing fertility-sparing surgery for early stage cervical cancer, aggregated rates of miscarriage and preterm labor are 24% and 26.6% with a pooled pregnancy rate of 20.5% [33••].
Various factors are associated with the high rates of miscarriage, preterm labor, and subsequent preterm premature rupture of membranes seen following radical trachelectomy in patients who achieve pregnancy. An initial theory pertained to the possibility that these complications could be a result of a lack of adequate blood flow to the uterus following transection of the uterine artery. However, Umemura and colleagues evaluated the uterine blood supply post radical trachelectomy using 3D CT scanning and showed that ligation of several supplying arteries to the uterus during radical trachelectomy actually induces new arterial vascularization and did not affect fetal growth or placental function [49]. This was also confirmed using contrast-enhanced MRI showing that there was no significant decrease of uterine enhancement rate following abdominal radical trachelectomy, suggesting that uterine function and fertility may be preserved after this procedure [50].
Additionally, a major etiology of 2nd trimester losses and preterm deliveries is likely due to mechanical changes to the remaining cervix and support to the growing lower uterine segment (i.e., short cervix). A short cervix prevents formation of a normal mucous plug, the main physiologic barrier to prevent ascending infections and subclinical chorioamnionitis [38].
Maternal fetal medicine consultation is critical for these patients to ensure they are receiving adequate perinatal care with the most up to date guidelines for the management of a short cervix including ultrasound cervical lengths [51, 52]. Additionally, if these patients have recurrent 2nd trimester miscarriages, there is evidence to suggest that an abdominal cerclage may be preventative [53]. Patients who reach term should be delivered via cesarean section given the permanent cerclage.
Conclusions
Radical trachelectomy for the treatment of early stage cervical cancer in women who desire to preserve fertility is a valuable alternative to radical hysterectomy. Its increasing acceptance and implementation have allowed for pooling of a wealth of retrospective data. The improvements over the past two decades with regards to laparoscopic and robotic surgery have revolutionized the surgical management of cervical cancer. Post-operative complications and oncologic outcomes are comparable to the gold standard, radical hysterectomy, in patients with similar-sized tumors. Although there is a high rate of miscarriage and early preterm birth, the majority of pregnancies reach > 32 weeks. The Dargent procedure, or radical trachelectomy, is one of the most important surgical advances in the treatment of early-stage cervical cancer. Future directions will push the envelope with respect to less radical procedures, but at this time, radical trachelectomy is a comparable and very valuable option for patients with early stage cervical cancer.
References and Recommending Reading
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
American Cancer Society. Cancer Facts & Figs. 2018. Atlanta, Ga: American Cancer Society; 2018. https://www.cancer.org/cancer/cervical-cancer/about/key-statistics.html#references. Accessed 15 July 2018
SEER Cancer Stat Facts: Cervical Cancer. National Cancer Institute. Bethesda, MD. https://seer.cancer.gov/statfacts/html/cervix.html. Accessed 15 July 2018
Rob L, Skapa P, Robova H. Fertility-sparing surgery in patients with cervical cancer. Lancet Oncol. 2011;12:192–200.
Sonoda Y, Abu-Rustum NR, Gemignani ML, Chi DS, Brown CL, Poynor EA, et al. A fertility-sparing alternative to radical hysterectomy: how many patients may be eligible? Gynecol Oncol. 2004;95(3):534–8.
Bhosale PR, Iyer RB, Ramalingam P, Schmeler KM, Wei W, Bassett RL, et al. Is MRI helpful in assessing the distance of the tumor from the internal os in patients with cervical cancer below FIGO Stage IB2? Clin Radiol. 2016;71(6):515–22.
Roy M, Plante M. Radical vaginal trachelectomy. In: Querleu D, Dargent D, Childers JM, editors. Laparoscopic Surgery in Gynecological Oncology. London: Blackwell Science; 1999. p. 78–82.
Smith JR, Boyle DC, Corless DJ, Ungar L, Lawson AD, Del Priore G, et al. Abdominal radical trachelectomy: a new surgical technique for the conservative management of cervical carcinoma. Br J Obstet Gynaecol. 1997;104(10):1196.
Abu-Rustum NR, Sonoda Y, Black D, Levine DA, Chi DS, Barakat RR. Fertility-sparing radical abdominal trachelectomy for cervical carcinoma: technique and review of the literature. Gynecol Oncol. 2006;103(3):807–13.
Obermair A, Gebski V, Frumovitz M, Soliman PT, Schmeler KM, Levenback C, et al. A phase III randomized clinical trial comparing laparoscopic or robotic radical hysterectomy with abdominal radical hysterectomy in patients with early stage cervical cancer. J Minim Invasive Gynecol. 2008;15(5):584–8.
Zhang D, Ge H, Li J, Wu X. A new method of surgical margin assuring for abdominal radical trachelectomy in frozen section. Eur J Cancer. 2015;51(6):734–41.
Park KJ, Soslow RA, Sonoda Y, Barakat RR, Abu-Rustum NR. Frozen-section evaluation of cervical adenocarcinoma at time of radical trachelectomy: pathologic pitfalls and the application of an objective scoring system. Gynecol Oncol. 2008;110(3):316–23.
Ismiil N, Ghorab Z, Covens A, Nofech-Mozes S, Saad RE, Dube V, et al. Intraoperative margin assessment of the radical trachelectomy specimen. Gynecol Oncol. 2009;113(1):42–6.
Tanguay C, Plante M, Renaud MC, Roy M, Tetu B. Vaginal radical trachelectomy in the treatment of cervical cancer: the role of frozen section. Int J Gynecol Pathol. 2004;23(2):170–5.
Zigras T, Lennox G, Willows K, Covens A. Early cervical cancer: current dilemmas of staging and surgery. Curr Oncol Rep. 2017;19(8):51.
Lecuru F, Mathevet P, Querleu D, Leblanc E, Morice P, Darai E, et al. Bilateral negative sentinel lymph nodes accurately predict absence of lymph node metastases in early cervical cancer: results of the SENTICOL study. J Clin Oncol. 2011;29(13):1686–91.
Bats AS, Buenerd A, Querleu D, Leblanc E, Darai E, Morice P, et al. Diagnostic value of intraoperative examination of sentinel lymph node in early cervical cancer: a prospective, multicenter study. Gynecol Oncol. 2011;123(2):230–5.
National Comprehensive Cancer Network. Cervical Cancer (Version 1.2018). http://www.nccn.org/professionals/physician_gls/pdf/cervix.pdf. Accessed 17 Apr 2018.
Ungar L, Palfalvi L, Hogg R, Siklos P, Bpyle DCM, del Priore G, et al. Abdominal radical trachelectomy: a fertility-preserving option for women with early cervical cancer. Br J Obstet Gynaecol. 2005;112:366–9.
Kim M, Ishioka S, Endo T, Baba T, Akashi Y, Morishita M, et al. Importance of uterine cervical cerclage to maintain a successful pregnancy for patients who undergo vaginal radical trachelectomy. Int J Clin Oncol. 2014;19(5):906–11.
• Li X, Li J, Wu X. Incidence, risk factors, and treatment of cervical stenosis after radical trachelectomy. Eur J Cancer. 2015;51(13):1751–9. A systematic review of cervical stenosis following radical trachelectomy.
Israfil-Bayli F, Toozs-Hobson P, Lees C, Slack M, Ismail KMK. Pregnancy outcome after elective cervical cerclage in relation to type of suture material used. Med Hypotheses. 2013;81(1):119–21.
Tang J, Li J, Wang S, Zhang D, Wu X. On what scale does it benefit the patients if uterine arteries were preserved during ART? Gynecol Oncol. 2014;134(1):154–9.
• Escobar PF, Ramirez PT, Garcia Ocasio RE, Pareja R, Zimberg S, Sprague M, et al. Utility of indocyanine green (ICG) intra-operative angiography to determine uterine vascular perfusion at the time of radical trachelectomy. Gynecol Oncol. 2016;143(2):357–61. First evaluation of ICG fluorescence angiography in patients undergoing radical trachelectomy to evaluate uterine perfusion. Based on our real-time intraoperative angiography observations, there is no need to preserve the uterine artery during radical trachelectomy to maintain uterine viability.
Guo J, Zhang Y, Chen X, Sun L, Chen K, Sheng X. Surgical and oncologic outcomes of radical abdominal trachelectomy versus hysterectomy for stage IA2-IB1 cervical cancer. J Minim Invasive Gynecol.
Alexander-Sefre F, Chee N, Spencer C, Menon U, Shepherd JH. Surgical morbidity associated with radical trachelectomy and radical hysterectomy. Gynecol Oncol. 2006;101(3):450.
Xu L, Sun FQ, Wang ZH. Radical trachelectomy versus radical hysterectomy for the treatment of early cervical cancer: a systematic review. Acta Obstet Gynecol Scand. 2011;90(11):1200–9.
Nick AM, Frumovitz MM, Soliman PT, Schmeler KM, Ramirez PT. Fertility sparing surgery for treatment of early-stage cervical cancer: open vs robotic radical trachelectomy. Gynecol Oncol. 2012;124:276–80.
•• Vieira MA, Rendon GJ, Munsell M, Echeverri L, Frumovitz M, Schmeler KM, et al. Radical trachelectomy in early-stage cervical cancer: A comparison of laparotomy and minimally invasive surgery. Gynecol Oncol. 2015;138(3):585–9. This is the largest comparative series of open vs. MIS of radical trachelectomy.
Boss EA, van Golde RJ, Beerendonk CC, Massuger LF. Pregnancy after radical trachelectomy: a real option? Gynecol Oncol. 2005;99(3 Suppl 1):S152.
Pareja R, Rendon GJ, Sanz-Lomana CM, Monzon O, Ramirez PT. Surgical, oncological, and obstetrical outcomes after abdominal radical trachelectomy- a systematic literature review. Gynecol Oncol. 2013;131(1):77–82.
Morice P, Dargent D, Haie-Meder C, Duvillard P, Castaigne D. First case of a centropelvic recurrence after radical trachelectomy: literature review and implications for the preoperative selection of patients. Gynecol Oncol. 2004;92(3):1002–5.
Del Priore G, Ungar L, Richard Smith J, Heller PB. Regarding “First case of a centropelvic recurrence after radical trachelectomy: literature review and implications for the preoperative selection of patients,” (92:1002–5) by Morice et al. Gynecol Oncol. 2004;95(2):414 author reply:414–6.
•• Zhang Q, Li W, Kanis MJ, Qi G, Li M, Yang X, et al. Oncologic and obstetrical outcomes with fertility-sparing treatment of cervical cancer: systematic review and meta-analysis. Oncotarget. 2017;8:46580–92 This is one of the largest meta-analysis to evaluate the rates of recurrence, survival, pregnancy and pregnancy outcomes of early-stage cervical cancer treated with fertility-sparing methods such as cervical conization and radical trachelectomy with or without pelvic lymphadenectomy.
Plante M, Renaud M-C, Francois H, Roy M. Vaginal radical trachelectomy: an oncologically safe fertility-preserving surgery. An updated series of 72 cases and review of the literature. Gynecol Oncol. 2004;94:614–23.
Roy M, Plante M. Pregnancies after radical vaginal trachelectomy for early-stage cervical cancer. Am J Obstet Gynecol. 1998;179(6):1491.
Steed H, Covens A. Radical vaginal trachelectomy and laparoscopic pelvic lymphadenopathy for preservation of fertility. Postgrad Obstet Gynecol. 2003;23:1.
Covens A. Preserving fertility in early stage cervical cancer with radical trachelectomy. Contemp Obstet Gynecol. 2003;48:46–66.
Shepherd JH, Spencer C, Herod J, Ind TEJ. Radical vaginal trachelectomy as a fertility-sparing procedure in women with early-stage cervical cancer-cumulative pregnancy rate in a series of 123 women. BJOG. 2006;113(6):719–24.
Hertel H, Kohler C, Hillemanns P, et al. Radical vaginal trachelectomy (RVT) combined with laparoscopic pelvic lymphadenectomy; prospective multicenter study of 100 patients with early cervical cancer. Gynecol Oncol. 2006;103:506–11.
Dargent D, Martin X, Sacchetoni A, Mathevet P. Laparoscopic vaginal trachelectomy: a treatment to preserve the fertility of cervical carcinoma patients. Cancer. 2000;88:1877–82.
Mathevet P, Laszlo de Kaszon E, Dargent D. Fertility preservation in early cervical cancer. Gynecol Obstet Fertil. 2003;31:706.
Ungar L, Palfalvi L, Smith JR, et al. Update on and long term follow-up of 91 abdominal radical trachelectomies. Gynecol Oncol. 2006;101:S20.
Diaz JP, Sonoda Y, Leitao MM, et al. Oncologic outcome of fertility-sparing radical trachelectomy versus radical hysterectomy for stage IB1 cervical carcinoma. Gynecol Oncol. 2008;111(2):255.
Wethington, Cibula D, Duska LR, et al. An international series on abdominal radical trachelectomy: 101 patients and 28 pregnancies. Int J Gynecol Cancer. 2012;22:1251–7.
Burnett AF, Roman LD, O’meara AT, Morrow CP. Radical vaginal trachelectomy and pelvic lymphadenectomy for preservation of fertility in early cervical carcinoma. Gynecol Oncol. 2003;88:419–23.
Schlaerth JB, Spirtos NM, Schlaerth AC. Radical trachelectomy and pelvic lymphadenectomy with uterine preservation in the treatment of cervical cancer. Am J Obstet Gynecol. 2003;188:29–34.
Bernardini M, Barrett J, Seaward G, et al. Pregnancy outcome in patients post radical trachelectomy. Am J Obstet Gynecol. 2003;189:1378.
Kim CH, Abu-Rustum NR, Chi DS, et al. Reproductive outcomes of patients undergoing radical trachelectomy for early-stage cervical cancer. Gynecol Oncol. 2012;125(3):585.
Umemura K, Ishioka S, Endo T, et al. Changes of uterine blood flow after vaginal radical trachelectomy (VRT) in patients with early-stage uterine invasive cervical cancer. Int J Med Sci. 2010;7(5):260–6.
Makino H, Kato H, Furui T, Hayasaki Y, Morishige K, Kanematsu M. Assessment of uterine enhancement rate after abdominal radical trachelectomy using dynamic contrast-enhanced magnetic resonance imaging. Arch Gynecol Obstet. 2016;293(3):625–32.
Plante M, Renaud MC, Hoskins IA, Roy M. Vaginal radical trachelectomy: a valuable fertility-preserving option in the management of early-stage cervical cancer. A series of 50 pregnancies and review of the literature. Gynecol Oncol. 2005;98:3.
Kasuga Y, Miyakoshi K, Nishio H, et al. Mid-trimester residual cervical length and the risk of preterm birth in pregnancies after abdominal radical trachelectomy: a retrospective analysis. BJOG. 2017;124(11):1729–35.
Ishioka S, Endo T, Baba T, et al. Successful delivery after transabdominal cerclage of uterine cervix for cervical incompetence after radical trachelectomy. J Obstet Gynaecol Res. 2015;41(8):1295–9.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Gynecologic Cancers
Rights and permissions
About this article

Cite this article
Costales, A., Michener, C. & Escobar-Rodriguez, P.F. Radical Trachelectomy for Early Stage Cervical Cancer. Curr. Treat. Options in Oncol. 19, 75 (2018). https://doi.org/10.1007/s11864-018-0591-4
Published:
DOI: https://doi.org/10.1007/s11864-018-0591-4