
Abstract
Background
Micro-RNA (miRs) targeting kinases and phosphatases regulate the hyper-phosphorylation of tau protein, which is a characteristic feature of Chronic Traumatic Encephalopathy (CTE).
Primary objective.
Identification of lead dysregulated miR expressed in CTE, and other similar tauopathies.
Methods
A search strategy was devised using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to mine into multiple indexing databases such as Web of Science, Google Scholar, and PubMed spanning from 2005 to June 2022. Seven articles were screened out of 34,221 publications based on inclusion criteria and were categorized into two groups i.e., (1) CTE and its risk factors and (2) Age-related neurodegenerative disorders.
Results
Statistical analysis [RevMan 5.4.1] results showed that the overall risk ratio (RR) of the first group is significant (RR = 0.62, 95% CI = [0.38, 1.00], z = 1.95, p = 0.05) whereas, the second group favours the control population (RR = 1.64, 95% CI = [0.85, 3.16], z = 1.14, p = 0.14).
Conclusion
We observed that among all other dysregulated miRs, miR-181c-5p is significantly overexpressed in Alzhimers disease (AD) and CTE. Further, we found that miR-210-3p is also upregulated notably in all groups. In sum, we conclude that these miRs can be considered as potential target and biomarker in the diagnosis and treatment of various tauopathies.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The central nervous system has always remained enigmatic and attracted the interest of many researchers [1] that, makes neurodegenerative diseases (NDs) a worldwide medical and public health concern. It has significantly impacted brain functions through formation of aberrant intracellular deposits caused by neural apoptosis [2]. It is well recognized that age, genetic variations, phenotypic changes and mitochondrial dysfunction [3], gender susceptibility, inflammation, and oxidative stress will play important role in increasing neurodegeneration [4]. People suffering from metabolic diseases such as stroke, hypertension, diabetes mellitus [5], elite sports persons [6] and military combats [7], are more prone to accelerate the natural neuron deterioration process [8]. Deposition of neurofibrillary tangles (NFTs) is the most common cause of increased neurodegeneration and cognitive decline.
Chronic traumatic encephalopathy (CTE) arises from sports related-head trauma. A repetitive closed-brain injury results in the activation of inflammatory cascades, deposition of tau protein and NFTs [9]. This disease shares the similarity with the AD in the neurodegenerative process but different in the brain region affect and NFTs deposition [10]. Since 1973 to 2005 and currently ongoing, first diagnosed in boxer and then in autopsy of a professional football player, Boston University has made significant contributions to the identification of CTE in an increasing number of instances, making it increasingly frequent and under recognized [11, 12]. A distinguishing factor of CTE lies within the hyper-phosphorylation of tau protein, which occurs frequently in neurodegenerative disorders like Alzheimers disease (AD), Dementia, Amyotrophic lateral sclerosis (ALS), Parkinsons disease (PD), and traumatic brain injury TBI [10]. At present CTE can be diagnosed at the time of post-mortem has increase the need to identify biomarker to diagnose it in life [13]. Treatment strategy for CTE is still limited to management of symptoms and recently tau hyper-phosphorylation and acetylation targets studies are directing the future [14]. Since we know that, miRs are known for therapeutic targets for various conditions such as cancer, diabetes, and heart diseases [15]. miRs have been identified in stable forms within biological fluids, including plasma, serum, and CSF [16]. Thousands of miRs have been discovered in a variety of species, including the central nervous systems of mammals, plants, animals, and viruses [17]. The miRs expressed in the mammalian brain account for around 70% of the identified [18]. Numerous studies indicate that they have a role in neuron development and division [19,20,21].
Micro-RNAs are small non-coding RNAs (22 nucleotides) [22] that control tumor growth, metastasis, and cell proliferation [23, 24]. They control mRNA stability by inhibiting protein synthesis during translation [25]. A small number of studies have demonstrated that miRs that target kinases and phosphatases control Tau expression and phosphorylation [26, 27]. Numerous studies have shown that patients with AD had downregulated levels of a group of mi-RNAs (miR-9, miR-149, miR-181c miR-137, and miR-29a/b) [28,29,30,31]. Other researches align with the expression in various tauopathies, including ALS, Parkinson's disease, traumatic brain injury, and other NDs [32,33,34,35].
Over 2000 miRs are encoded by the human genome; each miR controls several hundred genes, making it useful for therapeutic purposes. Because it directly controls DNA and protein molecules in addition to interacting with mRNA, the non-complementary passenger strand of miR is a master regulator in GNRs [36]. After cell injury, miRs passively circulate in the blood, urine, and saliva, making them an easily accessible biomarker for NDs and CTE. Until recently, reviews have focused on CTE diagnosis, managements and its biomarker development; however, as far as our understanding goes, this meta-analysis will pioneer the investigation and clarification of miRs importance as a therapeutic target for CTE.. Therefore, the current meta-analysis aims to identify lead dysregulated miRs expressed in CTE and other similar tauopathies.
Methods
In this study, we have followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 2020 [37], to identify the potentiality and lead miRs regulating tau phosphorylation in various NDs including CTE.
Search strategy
The PubMed database was utilized to search for relevant articles by applying specific keywords, "Alzheimer's disease, OR chronic traumatic encephalopathy, OR amyotrophic lateral sclerosis, OR CTE, OR ALS, OR tauopathies, OR AD AND microRNA OR miRNA OR Micro-RNA OR mi-RNA AND biomarker". Further, other sets of keywords "Concussion, mi-RNA and traumatic brain injury" were used in Google Scholar and Web of Science for identifying relevant studies. We found total 34,221 publication from 2005 to June 2022. These studies were screened based on the inclusion and exclusion criteria.
Screening and data extraction
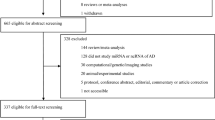
Based on Inclusion criteria mention in the Table 1, studies were screened and selected as shown in Fig. 1 following the PRISMA guideline. Data extraction was performed based on a customized table containing information as in Table 2. A customized excel sheet was used to segregate different miRs dysregulated in selected studies and common miRs were identified in different tauopathies.

PRISMA 2020 flow diagram for study selection
Study quality assessment
Studies were assessed based on the Newcastle–Ottawa quality assessment scale for case–control studies and cohort studies by National Centre for Biotechnology Information (NCBI) [38]. The scale consists of questions on selection such as adequate case definition, repetitiveness, selection and definition of control. The scale as shown in Table S1 also assesses comparability and exposure.
Publication Bias
To generalize the findings of the meta-analysis, it is crucial to consider publication bias. This can be accomplished by analyzing more than 10 studies using a funnel plot technique. All the studies included should pertain to the same identified disease [39].
Statistical analysis
The meta-analysis aims to identify the potential miRs regulating tau pathologies. Effect size (EF) was measured using a dichotomous variable approach as per Sanchez-Meca J et al. (2003) [40]. We performed a meta-analysis by segregating the data into two categories (1) CTE and its risk factors; such as TBI, and concussion (2) Age-related neurodegenerative disorders. Since, the results are not limited to the included population in selected studies, we chose a random effect model and a p-value < 0.05 was defined for two-tailed statistical significance [41]. The statistical analysis was performed on the Review Manager (RevMan) Version 5.4.1, the Cochrane Collaboration, 2020.
Results
Study selection
In this meta-analysis, we retrieved 34,221 articles and 20,331 articles were excluded after applying automation tool (NCBI filter) as per the inclusion criteria mentioned in Table 1. Among them 330 studies were duplicated. 166 review article and meta-analysis were removed, and then 75 studies were excluded on the basis of title and abstracts. The remaining 23 articles were selected for full text review. Total seven articles were selected based on the satisfied inclusion criteria (as shown in Fig. 1).
Study characteristics and quality assessment
This meta-analysis consists of four cohort studies [42,43,44,45], and three case–control studies [46,47,48] representing AD, ALS, FTD, MCI, CTE and other factors responsible for neurodegeneration. From the 7 studies, total 316 cases and total 134 control were obtained. Each study has employed various diagnostics criteria to detect disease and access (qRT-PCR, microarray and nano string technology) the miRs expression profile (shown in Table 2). Articles were assessed for the quality based on Newcastle–Ottawa quality assessment scale and the scores are mention in Tables 2 and S1.
Study participants and background
In this meta-analysis, total 316 cases and 134 control were included in seven studies. Four studies represent the age and gender matched case and control group of ALS disease [44,45,46,47]. Remaining studies did not match the case and control group ratio in different conditions [42, 43, 48]. Two studies that, included younger population (> 14-year-old) are Di Pietro et al. (2018) they included rugby players diagnosed with concussion and healthy non-concussed players as control group; while Redell et al. (2010) had TBI group due to accident, assault and brain injury. Most of the studies included old age population in range of 64–77 years having familial and sporadic ALS, AD, MCI and FTD. One study included familial ALS case group with healthy control group but the age was not clearly mentioned. Another study included sporadic ALS with gender-matched ratio of case and control. A study done by Alvia et al., 2022 included brain tissue samples from brain doners.
All the participants included in studies were recruited from various sources. Participants were identified from Hospitals, medical universities, Department of Veterans Affairs, Biorepository Brain Bank, Understanding Neurology Injury and Traumatic Encephalopathy (UNITE), research centres, ALS clinics, and emergency departments. All the studies had prior ethical clearance and written informed consent. One study did not mention the recruitment source [43].
Micro-RNA expression analysis
All the significant miRs based on disease and sample source are shown in Fig. 2. Studies reported different miRs expression in ALS condition such as, 24 miRs by Freischmidt et al. (2014) and 5 miRs by Lo et al. (2021) were significantly downregulated. Whereas, 11 miRs were upregulated in ALS condition by Toivonen et al. (2014) and Lo et al. (2021). Di Pietro et al. (2018) reported overexpression of 21 miRs in concussion. Alvia et al. (2022) identified significant overexpression of 5 miRs in CTE, 2 in ALS, 2 in CTE + ALS condition. Siedlecki-Wullich et al. (2019) reported 3 miRs significantly upregulated in AD, MCI and FTD respectively. In tissue and saliva samples, miR 16-5p was commonly increased in CTE and concussion. Redell et al. (2010) and Toivonen et al. (2014) show a simultaneous expression profile of different identified miRs of ALS and TBI in Fig. 3. Commonly found in CTE, ALS, MCI, and AD were miR-181c-5p and miR-210-3p among the identified miRs. Meanwhile, an increased expression of miR-16-5p was discovered in those suffering from concussion and CTE. Among all the identified miR top lead and common miRs are as listed in Table 3.

Micro-RNA dysregulation in various tau pathologies. A The disease specific dysregulation. B The tissue specific in human case groups. The red downward and green up-ward arrow mark shows the downregulation and upregulation miRs, respectively

Micro-RNAs expressed in ALS and TBI test group of two different studies
Risk ratio assessment
Chronic traumatic encephalopathy and its risk factors
In CTE and its risk factors such as concussion and TBI, the result of 4 studies of different conditions CTE, TBI, MCI, FTD and concussion were analysed and represented in forest plot as shown in Fig. 4. The miR expression in included studies was assessed using brain tissue sample, saliva, and plasma from a total of 75 test and 54 control groups with reported events. The resulting overall risk ratio is 0.62, 95% CI = [0.38, 1.00], which is significant at z-value = 1.95, p-value = 0.05. The present meta-analysis showed a less moderate heterogeneity [tau2 = 0.14, chi2 = 8.34, p = 0.08, I2 = 52%].

Micro-RNA as a diagnostic marker in CTE and its risk factors favoring test group has a significant outcome
Age-related neurodegeneration includes AD and ALS
For age-related neurodegeneration, events occurring in 118-test group diagnosed with AD, ALS and 45 controls were included out of five selected studies. The results showed non-significant overall risk ratio 1.64, 95% CI = [0.85, 3.16] (Z = 1.14, p = 0.14) as shown in Fig. 5. The present forest plot shows significant heterogeneity in the considered data [tau2 = 0.32, chi2 = 15.78, p = 0.003]; I2 = 75%.

Identification of miR expression in age related tau phosphorylated neurodegenerative disease having heterogeneity of outcome
Discussion
The present meta-analysis aimed to investigate miRs as a potential biomarker, especially focusing on CTE and its similar NDs such as AD, FTD, PD and ALS. Brain donor tissues have been the basis of understanding CTE progression in post-mortem analysis [49]. Recently, researchers have emphasized developing a diagnostic biomarker for CTE during lifetime. At the present scenario, they can be diagnosed with many criteria such as GCS, MACE 2 (Military Acute Concussion Evaluation), neuroimaging techniques (MRI, and CT), the diagnostic marker (S100B, UCHL-1, GFAP) and prognostic markers (tau protein and antibodies against tau protein) other than assessment of symptoms such as dizziness, headache, nausea, vomiting, cognition problems [50]. Through the process of miR target recognition and subsequent binding with mRNA, microRNAs perform their essential function of regulating gene expression [25].
Many pathways associated with neuroinflammation and cellular changes have been identified with miRs dysregulation [50]. In our findings, miR's expression was favouring CTE and its risk factor condition suggests that miR's dysregulated expression profile identification can be a therapeutic target for CTE and its related risk factors such as concussion and TBI. Identification of miRNA-mRNA target interactions is essential for understanding the regulatory networks governed by miRNAs. In the experimental approach described by Riolo et al. (2020) [51], miR responsive elements (mREs) can be utilized to recognize the target sites of miRs. Compared to proteins, miRs are considered more significant and reliable as biomarkers because the potential changes induced by miRs can be measured at the protein level with mREs [52]. CTE, characterized by tau protein hyper phosphorylation, is associated with key factors such as concussions and brain injuries [53]. The upregulated miRs (miR-181c-5p, and miR-210-3p) found in this study are highly expressed in brain tissue, suggesting a potential association between these miRs and the translation of tau protein [54]. The overexpression of miR 181c and the NCAPG protein complex are inversely correlated, according to a study on hepatocellular carcinoma [55]. The inhibition of the Notch2 pathway may impede cell division in gliomas, as suggested by Catanzaro et al., which report decreased levels of miR-181c expression [56]. Evidence from the study supports the notion that decreased expression of miR-181c-5p is connected to elevated Aβ1–40 levels, highlighting the relationship between these two factors [57]. We can propose miRNAs as a therapeutic target for brain injury and concussion in light of the aforementioned findings. Some lines of review based on CNS injury and miRs as therapeutic target has previously suggested mimic and inhibitor as a protective agent for ischemic stroke [58]. In another study inhibition of miR-181 family improved outcomes of stroke in rat models [59]. Generally, the mechanism of action was reducing the anti-inflammatory factors, improving the blood brain Barrie function and decrease the edema in various regions of the brain [58]. A systematic review has suggested panel of 10 regulated miRs in early stage of AD, hence miRs identified in our meta-analsis can be biomarkers for CTE [60].
We found 93 miRs significantly up regulated, whereas 67 miRs were significantly down regulated in different tau pathologies. In the context of this study, it was found that among these molecules, miR-181c-5p shows consistent upregulation in both CTE and AD conditions (Fig. S1). However, miR-210-3p demonstrates a significant increase in expression levels not only in CTE but also in ALS, AD, and MCI conditions (as depicted in Fig. S2). Additionally, our investigation reveals the upregulation of miR-124-3p, miR-197-3p, miR-100-5p, and Let‐7i‐5p specifically within individuals with CTE. Moreover, we also identified concurrent expression of miR-26a-5p, miR-17, miR-19b, miR-106b, and miR-24 in subjects with ALS as well as those with TBI [47, 48]. In our meta-analysis, sports related injury data is limited but literature exploration on the miR expression in the sports related concussion suggest other data such as, Svingos et al. (2019) reported miR-153–3p, miR-let-7a-5p and miR-223–3p upregulation in collegiate athletes [61]. Parallel to the findings, miR-27a-3p and miR-221-3p downregulation was reported by Shultz et al. (2022) in Australian Football Players [62]. Here, miR-221-3p is among the top ten miRs reported by this meta-analysis (Table 3). Various miRs and different expression reported by many studies makes the meta-analysis heterogenic in nature.
The variation of study outcomes between studies is defined as heterogeneity in the meta-analysis [39]. In this study, we found significant heterogeneity in tau phosphorylated neurodegenerative diseases such as AD and ALS conditions. It was heterogeneous in terms of the sample, distribution of population, miRs identification method and disease condition, Whereas CTE and its risk factors were not significantly heterogeneous in respective terms. This suggests the miRs expression as a potential tool for identifying the underlying condition.
The restricted databases and language limitations in our search strategy led to reporting bias, which is a limitation of our study. Moreover, publication bias indicates that the studies chosen for the meta-analysis may not accurately represent the overall research [63]. The publication bias can be performed on a minimum of 10 studies included in the meta-analysis as per the Recommendations on testing for funnel plot asymmetry [39]. This study gives insight to in-vitro and in-vivo studies by using their mimic and inhibiting the over and down expression of miRs in various tauopathies related to sports. Correlational studies using the miRs expression pattern and different drugs can be designed for the treatment strategy. Furthers studies using their sensitivity and specificity in particular disease can be assessed for confirmation.
Conclusion
In conclusion, our study identifies dysregulation of miRs in the context of CTE, AD, and ALS. Among the 160 total identified miRs, only two—namely miR-181c-5p and miR-210—exhibited consistent expression levels in both CTE and AD cases. This meta-analysis enhances the comprehension of the dysregulation of miR in different cause and risk factors of tauopathies.. The findings can be used as therapeutic target for concussions and brain injuries in the progression of NDs. The overall risk ratio was significant in CTE & its risk factors in the meta-analysis. Age related neurodegeneration was found to be significantly heterogeneous.
Data availability
The detailed methodology and dataset generated during the meta-analysis are available from the corresponding author upon reasonable request.
Code availability
Not applicable.
References
Batista-García-Ramó K, Fernández-Verdecia CI (2018) What we know about the brain structure-function relationship. Behav Sci (Basel) 8(4)
Kornienko VN, Pronin IN (2009) Neurodegenerative disorders of the central nervous system, in Diagnostic neuroradiology. Springer Berlin Heidelberg: Berlin, Heidelberg. p. 1075–1092. https://doi.org/10.1007/978-3-540-75653-8_14
Checkoway H, Lundin JI, Kelada SN (2011) Neurodegenerative diseases. IARC Sci Publ 163:407–419
Brown RC, Lockwood AH, Sonawane BR (2005) Neurodegenerative diseases: an overview of environmental risk factors. Environ Health Perspect 113(9):1250–1256
Abbott RD et al (2003) Environmental, life-style, and physical precursors of clinical Parkinson's disease: recent findings from the Honolulu-Asia Aging Study. J Neurol 250(3):30–9
Costanza A et al (2011) Review: Contact sport-related chronic traumatic encephalopathy in the elderly: clinical expression and structural substrates. Neuropathol Appl Neurobiol 37(6):570–584
Weiner MW et al (2013) Military risk factors for Alzheimer’s disease. Alzheimers Dement 9(4):445–451
Barth JT et al (2010) Acute battlefield assessment of concussion/mild TBI and return-to-duty evaluations. Military neuropsychology 127–174
McKee AC et al (2014) The neuropathology of sport. Acta Neuropathol 127(1):29–51
Montenigro PH et al (2015) Chronic traumatic encephalopathy: historical origins and current perspective. Annu Rev Clin Psychol 11:309–330
Omalu BI et al (2005) Chronic traumatic encephalopathy in a National Football League player. Neurosurgery 57(1):128–34 discussion 128–34
McKee AC et al (2013) The spectrum of disease in chronic traumatic encephalopathy. Brain 136(Pt 1):43–64
McKee AC (2020) The Neuropathology of Chronic Traumatic Encephalopathy: The Status of the Literature. Semin Neurol 40(4):359–369
Pierre K et al (2021) Chronic traumatic encephalopathy: update on current clinical diagnosis and management. Biomedicines 9(4)
Ganju A et al (2017) miRNA nanotherapeutics for cancer. Drug Discov Today 22(2):424–432
Weber JA et al (2010) The MicroRNA Spectrum in 12 Body Fluids. Clin Chem 56(11):1733–1741
Bhaskaran M, Mohan M (2014) MicroRNAs: history, biogenesis, and their evolving role in animal development and disease. Vet Pathol 51(4):759–774
Adlakha YK, Saini N (2014) Brain microRNAs and insights into biological functions and therapeutic potential of brain enriched miRNA-128. Mol Cancer 13(1):33
Radhakrishnan B, Alwin Prem Anand A (2016) Role of miRNA-9 in brain development. J Exp Neurosci 10:101–120
Cho KHT et al (2019) Emerging Roles of miRNAs in Brain Development and Perinatal Brain Injury. Front Physiol 10:227
Ma Q, Zhang L, Pearce WJ (2019) MicroRNAs in brain development and cerebrovascular pathophysiology. Am J Physiol Cell Physiol 317(1):C3-c19
Bartel DP (2004) MicroRNAs: genomics, biogenesis, mechanism, and function. Cell 116(2):281–297
Hwang HW, Mendell JT (2006) MicroRNAs in cell proliferation, cell death, and tumorigenesis. Br J Cancer 94(6):776–780
Baranwal S, Alahari SK (2010) miRNA control of tumor cell invasion and metastasis. Int J Cancer 126(6):1283–1290
Wu Y-Y, Kuo H-C (2020) Functional roles and networks of non-coding RNAs in the pathogenesis of neurodegenerative diseases. J Biomed Sci 27(1):49
Praticò D (2020) The functional role of microRNAs in the pathogenesis of tauopathy. Cells 9(10)
Gui Y et al (2015) Altered microRNA profiles in cerebrospinal fluid exosome in Parkinson disease and Alzheimer disease. Oncotarget 6(35)
Du W, Lei C, Dong Y (2021) MicroRNA-149 is downregulated in Alzheimer’s disease and inhibits β-amyloid accumulation and ameliorates neuronal viability through targeting BACE1. Genet Mol Biol 44(1):e20200064
Indrieri A et al (2020) The pervasive role of the miR-181 family in development, neurodegeneration, and cancer. Int J Mol Sci 21(6)
Kou X, Chen D, Chen N (2020) The Regulation of microRNAs in Alzheimer’s Disease. Front Neurol 11:288
Yuen SC et al (2021) Prediction of differentially expressed microRNAs in blood as potential biomarkers for Alzheimer’s disease by meta-analysis and adaptive boosting ensemble learning. Alzheimers Res Ther 13(1):126
Cao T, Zhen XC (2018) Dysregulation of miRNA and its potential therapeutic application in schizophrenia. CNS Neurosci Ther 24(7):586–597
Liu J et al (2022) The Biogenesis of miRNAs and Their Role in the Development of Amyotrophic Lateral Sclerosis. Cells 11(3)
Salemi M et al (202) Role and Dysregulation of miRNA in Patients with Parkinson's Disease. Int J Mol Sci 24(1)
Atif H, Hicks SD (2019) A Review of MicroRNA Biomarkers in Traumatic Brain Injury. J Exp Neurosci 13:1179069519832286
O'Brien J et al (2018) Overview of microRNA biogenesis, mechanisms of actions, and circulation. Front Endocrinol 9
Page MJ et al (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372:n71
Stang A (2010) Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol 25(9):603–605
Higgins JPT, GS ed (2011) Cochrane handbook for systematic reviews of interventions. Vol. 5.1.0. The Cochrane Collaboration
Sánchez-Meca J, Marín-Martínez F, Chacón-Moscoso S (2003) Effect-size indices for dichotomized outcomes in meta-analysis. Psychol Methods 8(4):448–467
Hall JA, Rosenthal R (2018) Choosing between random effects models in meta-analysis: Units of analysis and the generalizability of obtained results. Soc Pers Psychol Compass 12(10):e12414
Siedlecki-Wullich D et al (2019) Altered microRNAs related to synaptic function as potential plasma biomarkers for Alzheimer’s disease. Alzheimers Res Ther 11(1):46
Freischmidt A et al (2015) Serum microRNAs in sporadic amyotrophic lateral sclerosis. Neurobiol Aging 36(9):2660.e15–20. https://doi.org/10.1016/j.neurobiolaging.2015.06.003
Di Pietro V et al (2018) Salivary microRNAs: diagnostic markers of mild traumatic brain injury in contact-sport. Front Mole Neurosci 11
Lo TW et al (2021) Extracellular Vesicles in Serum and Central Nervous System Tissues Contain microRNA Signatures in Sporadic Amyotrophic Lateral Sclerosis. Front Mol Neurosci 14:739016
Alvia M et al (2022) MicroRNA Alterations in Chronic Traumatic Encephalopathy and Amyotrophic Lateral Sclerosis. Front Neurosci 16:855096
Toivonen JM et al (2014) MicroRNA-206: a potential circulating biomarker candidate for amyotrophic lateral sclerosis. PLoS ONE 9(2):e89065
Redell JB et al (2010) Human traumatic brain injury alters plasma microRNA levels. J Neurotrauma 27(12):2147–2156
McKee AC, Abdolmohammadi B, Stein TD (2018) Chapter 28 - The neuropathology of chronic traumatic encephalopathy, in Handbook of clinical neurology, Hainline B, Stern RA Editors Elsevier 297–307
Devoto C et al (2022) Remote blast-related mild traumatic brain injury is associated with differential expression of exosomal microRNAs identified in neurodegenerative and immunological processes. Brain Inj 36(5):652–661
Riolo G et al (2020) miRNA targets: from prediction tools to experimental validation. Methods Protoc 4(1)
Seok H et al (2016) MicroRNA Target Recognition: Insights from Transcriptome-Wide Non-Canonical Interactions. Mol Cells 39(5):375–381
Rodrigo Medeiros DB-V, Frank LaFerla M (2011) The role of tau in Alzheimer’s disease and related disorders. CNS Neurosci Ther 17:514–524
Stelzer G, Rosen R, Plaschkes I, Zimmerman S, Twik M, Fishilevich S, Iny Stein T, Nudel R, Lieder I, Mazor Y, Kaplan S, Dahary, D, Warshawsky D, Guan - Golan Y, Kohn A, Rappaport N, Safran M, Lancet D (2016) The GeneCards Suite: From Gene Data Mining to Disease Genome Sequence Analyses. Curr Protoc Bioinformatics 54:1.30.1-1.30.33. https://doi.org/10.1002/cpbi.5. (PMID: 27322403 ; Citations: 2,262)
Ai J et al (2019) MicroRNA-181c suppresses growth and metastasis of hepatocellular carcinoma by modulating NCAPG. Cancer Manag Res 11:3455–3467
Catanzaro G et al (2017) Loss of miR-107, miR-181c and miR-29a-3p promote activation of notch2 signaling in pediatric high-grade gliomas (pHGGs). Int J Mol Sci 18(12)
Manzano-Crespo M, Atienza M, Cantero JL (2019) Lower serum expression of miR-181c-5p is associated with increased plasma levels of amyloid-beta 1–40 and cerebral vulnerability in normal aging. Translational Neurodegeneration 8(1):34
Sun P et al (2018) MicroRNA-based therapeutics in central nervous system injuries. J Cereb Blood Flow Metab 38(7):1125–1148
Moon JM, Xu L, Giffard RG (2013) Inhibition of microRNA-181 reduces forebrain ischemia-induced neuronal loss. J Cereb Blood Flow Metab 33(12):1976–1982
Swarbrick S et al (2019) Systematic Review of miRNA as Biomarkers in Alzheimer’s Disease. Mol Neurobiol 56(9):6156–6167
Svingos AM et al (2019) Exploratory study of sport-related concussion effects on peripheral micro-RNA expression. Brain Inj 33(4):1–7
Shultz SR et al (2022) Decrease in Plasma miR-27a and miR-221 After Concussion in Australian Football Players. Biomark Insights 17:11772719221081318
Rothstein HR, Sutton AJ, Borenstein M ed (2005) Publication bias in meta-analysis. Chichester: John Wiley & Sons, Ltd
Funding
The study was supported by DST-INSPIRE project (DST/INSPIRE/04/2019/002618, UGC-start-up grant (F.30–547/2021), UGC-JRF (Ref. No.: 210510135543) and Central University of Rajasthan.
Author information
Authors and Affiliations
Contributions
Harshita Tak: Idea generation, hypothesis formulation, methodology development and study design creation, data collection and scrutiny, statistical analysis, initial draft writing, and manuscript finalization. Arpan Chattopadhyay: Review and Editing. Dr Hemanth Naick B: Developing the idea, designing the hypothesis, securing funds, editing and revising. All persons who meet authorship criteria are listed as authors and all authors certify that they have approved the version of the manuscript to be published and take responsibility for the content of the manuscript.
Corresponding author
Ethics declarations
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Consent to publish
Not applicable.
Conflict of interest
Authors declared no conflict of interest at any stage of the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Key points
• Treatment for chronic traumatic encephalopathy is limited to symptom management, and targeting tau hyper-phosphorylation and acetylation is a promising area of research.
• In the present study, it was observed that miR-181c-5p and miR-210-3p, which were upregulated, showed prominent expression levels in brain tissue, indicating a possible link between these specific miRNAs and tau protein translation.
• An analysis of multiple studies indicates that MiR-16 5p is often, raised in cases of CTE and concussion. On the other hand, miR 181c 5p and miR 210 3p are prevalent in individuals with CTE, ALS, AD, and MCI.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Tak, H., Chattopadhyay, A. & Banavath, H.N. A meta-analysis of differentially expressed circulatory micro-RNAs in chronic traumatic encephalopathy and other tauopathies: A significant role of miR-181c-5p. Ir J Med Sci 193, 999–1007 (2024). https://doi.org/10.1007/s11845-023-03469-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11845-023-03469-5