
Abstract
Background
The rate of ACL injury in adolescents has been rising in recent years. Surgical options include transphyseal and physeal-sparing ACL reconstruction.
Aims
In this study, we performed a transphyseal ACL reconstruction and followed up patients to assess functional outcomes and to assess for growth disturbance.
Method
There were 22 patients seen at follow-up between the age of 12 and 16. Skeletal age assessment was performed using an MRI atlas with an average skeletal age of 14.7 (range 12–16). The mean follow-up time was 36 months (range 14–63 months). Clinical examination was performed to assess for leg length discrepancy, and leg length radiographs were used to assess for angular deformity. Patients’ post-surgery functionality was assessed with the IKDC score and the Tegner Lysholm score.
Results
The mean IKDC and Lysholm scores at follow-up were found to be 91 and 94, respectively. The median Tegner score prior to injury was 8.5 and postoperatively was 7.5. There were no cases of leg length discrepancy found on clinical examination, and there were no cases of significant angular deformity. Four patients ruptured again and went on to have repeat ACL reconstruction.
Conclusions
Midterm results at an average follow-up of 3 years after the surgery showed good functional outcomes using the transphyseal ACL reconstruction technique with good return to activity. There were no cases of leg length discrepancy or angular deformity. Transphyseal ACL reconstruction is a viable method of treatment for adolescent ACL tears.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In recent times, there has been an increase in incidence of paediatric anterior cruciate ligament (ACL) tears. This has largely be attributed to increased participation of children in organized sports, as well as an improvement in the quality of imaging in reaching the diagnosis of an ACL tear [1]. Around 3% of paediatric knee injuries are due to ACL injury [2]. Janarv et al. [3] estimate that the incidence rate is 1/10,000 children. The most appropriate treatment for a paediatric ACL tear is a controversial topic in comparison with adult ACL injury, because of the open epiphyseal plate and the potential for developing a growth disturbance [4,5,6]. In this study, we performed a complete transphyseal ACL reconstruction with tunnelling crossing both the femoral and tibial physes. As part of the study, we followed up patients to assess for growth deformity resulting in either a leg length discrepancy or angular deformity as well as assessing their return to activity and functional outcomes.
The surgical technique used in this study was the complete transphyseal ACL reconstruction. The complete transphyseal ACL reconstruction is a modified version of the adult ACL reconstruction to minimize the risk of physeal disturbance. With this technique, the tunnels cross both the femoral and tibial physes with care taken to minimize the insult on the physes. In this study, we followed up patients that underwent this method of ACL reconstruction between the ages of 12 and 16 with a mean follow-up time of 36 months (range 14–63 months). We assessed postoperative functionality with subjective knee scores and assessed for leg length discrepancy with clinical exam and leg length discrepancy with leg length X-rays.
Methods
Study design
This was a retrospective case series on patients who received a complete transphyseal ACL reconstruction. Ethical approval was obtained from the Clinical Research Ethics Committee of University College Cork. The criteria we chose for inclusion in this study were those who received an ACL reconstruction between the age of 12 and 16 with open physes seen on MRI. There were 28 patients that met the criteria with 10 knees having a comorbid meniscal tear at the time of surgery. The timeframe for the surgeries was from June 2009 to October 2014 with the average age at the time of surgery 14.5 years (range 12-15.9 years).
Surgical technique
The patients of this study underwent a transphyseal ACL reconstruction where the gracilis and semitendinosus tendons were harvested and used to form either a quadruple or triple bundled (5 strand) stranded graft to replace the ACL. A triple bundled 5 strand graft was performed in some patients to increase the diameter of the graft as some of the patients had small hamstring tendons. An intercondylar notch was debrided using a shaver. The femoral and tibial tunnels crossed the physes of both the femur and tibia of the patients with tunnel diameters ranging from 7 to 9 mm. In order to reduce the risk of physeal disturbance, care was taken to minimize the tunnel diameter. For graft fixation on the femoral aspect, an Endobutton was used, and for graft fixation on the tibial aspect, an interface screw was used. After the ACL reconstruction was performed, the graft patency was assessed with the Lachman and pivot shift tests.
Follow-up assessment
There were two patients that were excluded from all data analysis. One patient was excluded because he initially underwent an ACL repair using cancellous screws for a tibial eminence fracture and then underwent transphyseal ACL reconstruction after this ruptured. This patient also developed a tibial varus deformity from the initial ACL repair which was corrected before undergoing complete reconstruction. Another patient was excluded because he had undergone bilateral ACL reconstruction, with his first ACL being reconstructed by another surgeon.
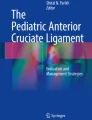
At follow-up assessment, all patients received weight-bearing leg length radiographs which were used to assess for any angular deformity. The angles of the nonoperative knee were used as a control to compare with the operated knee. The angles used for measurement were the medial mechanical axis of the knee and the lateral distal femoral articular angle using the anatomical axis of the femur (aLDFA) (Fig. 1). Leg length discrepancy was assessed by a clinical exam with measurement of the ASIS to medial malleolus. The strength of the reconstructed ACL was assessed with the Lachman test.

Medial mechanical axis of the knee; aLDFA
The International Knee Documentation Committee (IKDC) [7] and Lysholm [8] subjective knee scores were used to assess the functional capacity of the knee. The Tegner activity score [9] was used give a graded pre-injury and post-surgery activity level of the patient. Patients that re-injured their ACL and underwent a repeat ACL reconstruction over the age of 16 had their subjective knee scores excluded from the data analysis. Patients who had other comorbidities at the follow-up assessment also had their subjective knee scores excluded.
We grouped the patients for the purpose of the data analysis into an angle assessment group and a functionality assessment group. The angle group included the 22 patients that qualified for data analysis, and for the functional group, we excluded the patients with comorbidities when seen at follow-up, as well as patients who ruptured and underwent adult ACL reconstruction.
At follow-up, there was one ACL rupture, one patellar tendinopathy, two failed meniscal tears, and one new meniscal tear that were excluded from the functional group. The patients labelled as 17A-22A in the tables are the patients in the angle group that were excluded from functional analysis.
Skeletal age assessment
Skeletal age assessment was performed as chronological age is not an accurate assessment of adolescents due to the differing ages in which people reach puberty. Skeletal age assessment was performed using the Pennock and Bomar MRI Atlas of Skeletal Development of the Knee [10]. We performed this assessment using the preoperative MRIs. Figure 2 displays the coronal assessment of the femur with the “oreo sign” seen, which is due to the laminated appearance of the subchondral epiphyseal cartilage. Figure 3 displays the sagittal assessment of the fibula.

Coronal view displaying oreo sign

Sagittal view of fibular head
Results
Demographic results
For the patients seen at follow-up, the average age at the time of surgery was 14.4 ± 1.1 years (range 12.1–15.8 years). The average skeletal age at the time of surgery was 14.7 ± 1.2 years. The most significant difference between chronological age and skeletal age was patient 8 who was 13.2 years at the time of her first surgery and had a skeletal age of 16. At the time of her repeat transphyseal ACL reconstruction aged 14.5, she had a skeletal age of 17. Comparing the difference between chronologic age and skeletal age yielded a p value of 0.130. The average age at follow-up was 17.4 years (range 14.8–20.8 years) with the mean time follow-up being 36 months (range 14–63 months). Eight of the 22 patients included for data analysis had comorbid meniscal tears at the time of surgery. There was a graft failure rate of 4 of 22 knees. The demographics of these can be seen in Table 1.
Assessment of physeal disturbance
For assessment of physeal disturbance, there were no cases of leg length discrepancy > 1 cm found on clinical exam. For angular deformity assessment, the nonoperative leg was used as a control. The mechanical axis of the knee was found to have a mean valgus angle of Diff 0.80 ± 2.40 valgus (range 50 valgus angle to 30 varus angle) (p value = 0.150). Comparing male and females rendered a p value of 0.744. The distal femoral articular angle had a mean valgus angle of 0.90 ± 2.40 valgus (range 70 valgus angle to 20 varus angle) (p value = 0.086). Comparing males and females had a p value of 0.744. The angle values for each patient can be seen in Table 2.
Subjective scores
The mean IKDC score for patients at the follow-up assessment was 91 ± 8 (77–100). The mean Lysholm score was 94 ± 7 (79–100). There was no statistical difference found when comparing the means of the male and female IKDC and Lysholm scores with p values of 0.249 and 0.704, respectively. The median Tegner score prior to injury was 8.5 and the median Tegner score at follow-up was 7.5. The difference in p value = 0.227. The IKDC, Lysholm, and Tegner values for each patient can be seen in Table 2.
Discussion
There have been a number of different management options developed for paediatric cruciate ligament injury. While the management protocol for adult ACL injury is well established, paediatric ACL injury is a controversial subject due the risk of damaging the epiphyseal plates with surgical intervention [4, 11, 12].
The complete transphyseal ACL reconstruction is a modified version of the adult ACL reconstruction to minimize the risk of physeal disturbance. With this technique, the tunnels cross both the femoral and tibial physes. Smaller drill holes compared with adult surgery are used to minimize physeal disturbance. In a study on rabbits, it was found that tunnels which occupy < 5% of the cross-sectional area did not cause growth deformity and that the tunnels had to occupy 7–9% of cross-sectional area of physis to cause growth disturbance [13]. Kercher et al. [14] studied 31 patients between 10 and 15 years of age using MRI imaging of the knee to determine the average volume of the tibial and femoral physis. They reported that the tunnels of 8 mm in diameter removed 2.5% of the distal femoral physis and 2.4% of the proximal tibial physis, whereas an 11 mm diameter tunnel removed up to 7.8% of the physis. It is better to use soft tissue graft compared with bone-patellar-bone graft as it reduces the risk of growth arrest due to the placement of a bony block across the physes [15, 16]. Therefore, the hamstring tendon autograft was used.
The conservative management option involves nonoperative management with ACL bracing, strengthening, and rehabilitation, followed by delayed anatomical reconstruction when skeletal maturity is reached. But with this treatment method, there was found to be a high incidence of meniscal and chondral injuries due to the chronic anterior instability [17,18,19], and patients who received an immediate ACL reconstruction had less instability and lower rates of meniscal and chondral tears, and they also had higher activity levels with more returning to sport.
With surgical management, there have been a number of options developed which include physeal-sparing reconstruction and partial transphyseal reconstruction. With these techniques, the ACL is not in an anatomically accurate position [18, 20]. Nonanatomical ACL positioning is associated with a residual instability and an increased incidence of meniscal and chondral injuries [18, 20]. There have also been questions raised about the long-term function of grafts in a nonanatomic position as there is a potential graft elongation as the knee goes into extension [21].
In our study, we found good functional midterm outcomes with the transphyseal ACL reconstruction with good Lysholm and IKDC scores, as well as a good return rate to previous activity levels. There was a reduction of activity levels from pre-injury activity levels to activity levels at follow-up according to the Tegner activity scale. This was a decrease from a median of 8.5 for pre-injury activity levels to 7.5 for activity levels at the time of follow up. The p value was > 0.05 with the value of 0.227. This is a great return to activity levels compared with other studies. It must be noted that a reduction in activity levels is also seen in adult surgery also which may be due to fear of re-injury and loss of interest in sport participation with an increase in age [22].
We had an ACL revision rate of 4 of 22 knees. This is a good result as many studies on paediatric and adolescent ACL reconstruction have a high revision rate [23]. It proposed that the high revision rate for paediatric ACL reconstruction is due to the lack of compliance with rehabilitation programmes, changing of the position of graft due to further growth of the knee moving it out of an anatomical position. Schmale et al. [24] follow up study on transphyseal ACL reconstruction that had 4 repeat ACL reconstructions out of 29 knees after a mean follow-up of 39 months (8–66 months).
In analysing the data for angular deformity, there was no statistically significant difference when comparing the operated leg with the control leg for both the mechanical axis of the knee and the distal femoral articular angle with the p values both being > 0.05, given their p values scoring of 0.150 and 0.086, respectively.
There were many limitations in this study. The study was limited by being a retrospective study. This study had a small sample size with 22, consistent with many studies on the subject. There was no group involved in this study which could be used as comparison for another management option. The nonoperative leg was used as a control for angle analysis, where preoperative films using the same leg for assessment of postoperative change would be more accurate. Graft assessment using the KT-1000 arthrometer could have been used to give a numerical assessment of laxity as opposed to clinical assessment using Lachman’s test. There were five patients lost to follow-up which could be a source of attrition bias.
Conclusion
The complete transphyseal anterior cruciate ligament reconstruction provided good midterm results with good functionality and good return of physical activity. No patients involved in the study developed leg length discrepancy of angular deformity. Based on this case series, we would consider the complete transphyseal ACL reconstruction a safe option in management of an adolescent ACL injury with good functional outcomes. We would like to highlight that this study was based on an adolescent population and not a generalized paediatric population.
References
Dorizas JA, Stanitski CL (2003) Anterior cruciate ligament injury in the skeletally immature. Orthop Clin North Am 34(3):355–363
Souryal TO, Freeman TR (1993) Intercondylar notch size and anterior cruciate ligament injuries in athletes. A prospective study. Am J Sports Med 21(4):535–539
Janarv PM, Nystrom A, Werner S, Hirsch G (1996) Anterior cruciate ligament injuries in skeletally immature patients. J Pediatr Orthop 16(5):673–677
Kocher MS, Saxon HS, Hovis WD, Hawkins RJ (2002) Management and complications of anterior cruciate ligament injuries in skeletally immature patients: survey of the Herodicus Society and The ACL Study Group. J Pediatr Orthop 22(4):452–457
Chotel F, Henry J, Seil R et al (2010) Growth disturbances without growth arrest after ACL reconstruction in children. Knee Surg Sports Traumatol Arthrosc 18(11):1496–1500. https://doi.org/10.1007/s00167-010-1069-5
Meller R, Kendoff D, Hankemeier S, Jagodzinski M et al (2008) Hindlimb growth after a transphyseal reconstruction of the anterior cruciate ligament: a study in skeletally immature sheep with wide-open physes. Am J Sports Med 36(12):2437–2443. https://doi.org/10.1177/0363546508322884
Hefti F, Muller W, Jakob RP, Staubli HU (1993) Evaluation of knee ligament injuries with the IKDC form. Knee Surg Sports Traumatol Arthrosc 1(3–4):226–234
Lysholm J, Gillquist J (1982) Evaluation of knee ligament surgery results with special emphasis on use of a scoring scale. Am J Sports Med 10(3):150–154
Tegner Y, Lysholm J (1985) Rating systems in the evaluation of knee ligament injuries. Clin Orthop Relat Res 198:43–49
Pennock AT, Bomar JD (2017) Bone age assessment utilizing knee MRI. Orthop J Sports Med 5(7 suppl6):2325967117S2325900428. https://doi.org/10.1177/2325967117S00428
Bales CP, Guettler JH, Moorman CT 3rd (2004) Anterior cruciate ligament injuries in children with open physes: evolving strategies of treatment. Am J Sports Med 32(8):1978–1985
Frank JS, Gambacorta PL (2013) Anterior cruciate ligament injuries in the skeletally immature athlete: diagnosis and management. J Am Acad Orthop Surg 21(2):78–87. https://doi.org/10.5435/jaaos-21-02-78
Janarv PM, Wikstrom B, Hirsch G (1998) The influence of transphyseal drilling and tendon grafting on bone growth: an experimental study in the rabbit. J Pediatr Orthop 18(2):149–154
Kercher J, Xerogeanes J, Tannenbaum A, Al-Hakim R et al (2009) Anterior cruciate ligament reconstruction in the skeletally immature: an anatomical study utilizing 3-dimensional magnetic resonance imaging reconstructions. J Pediatr Orthop 29(2):124–129. https://doi.org/10.1097/BPO.0b013e3181982228
Simonian PT, Metcalf MH, Larson RV (1999) Anterior cruciate ligament injuries in the skeletally immature patient. Am J Orthop (Belle Mead NJ) 28(11):624–628
Andrews M, Noyes FR, Barber-Westin SD (1994) Anterior cruciate ligament allograft reconstruction in the skeletally immature athlete. Am J Sports Med 22(1):48–54
Lawrence JT, Argawal N, Ganley TJ (2011) Degeneration of the knee joint in skeletally immature patients with a diagnosis of an anterior cruciate ligament tear: is there harm in delay of treatment? Am J Sports Med 39(12):2582–2587. https://doi.org/10.1177/0363546511420818
McCarroll JR, Rettig AC, Shelbourne KD (1988) Anterior cruciate ligament injuries in the young athlete with open physes. Am J Sports Med 16(1):44–47
Graf BK, Lange RH, Fujisaki CK, Landry GL et al (1992) Anterior cruciate ligament tears in skeletally immature patients: meniscal pathology at presentation and after attempted conservative treatment. Arthroscopy 8(2):229–233. https://doi.org/10.1016/0749-8063(92)90041-9
McCarroll JR, Shelbourne KD, Porter DA, Rettig AC et al (1994) Patellar tendon graft reconstruction for midsubstance anterior cruciate ligament rupture in junior high school athletes. An algorithm for management. Am J Sports Med 22(4):478–484
Odensten M, Gillquist J (1985) Functional anatomy of the anterior cruciate ligament and a rationale for reconstruction. J Bone Joint Surg Am 67(2):257–262
Seijas R, Ares O, Sallent A, Alvarez P et al (2016) Return to prelesional Tegner level after anatomic anterior cruciate ligament reconstruction. Arch Orthop Trauma Surg 136(12):1695–1699. https://doi.org/10.1007/s00402-016-2544-3
Frosch KH, Stengel D, Brodhun T, Stietencron I et al (2010) Outcomes and risks of operative treatment of rupture of the anterior cruciate ligament in children and adolescents. Arthroscopy 26(11):1539–1550. https://doi.org/10.1016/j.arthro.2010.04.077
Schmale GA, Kweon C, Larson RV, Bompadre V (2014) High satisfaction yet decreased activity 4 years after transphyseal ACL reconstruction. Clin Orthop Relat Res 472(7):2168–2174. https://doi.org/10.1007/s11999-014-3561-6
Author information
Authors and Affiliations
Contributions
All authors have participated in (a) conception and design or analysis and interpretation of the data, (b) drafting the article or revising it critically for important intellectual content, and (c) approval of the final version.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no affiliation with any organization with a direct or indirect financial interest in the subject matter discussed in the manuscript.
Ethical approval
Ethical approval was obtained by Clinical Research Ethics Committee of the Cork Teaching Hospitals.
Informed consent
Informed consent was obtained from all individual participants in the study.
Additional information
The Article I have submitted to the journal for review is original, has been written by the stated authors, and has not been published elsewhere.
This manuscript has not been submitted to, nor is under review at, another journal or other publishing venue.
Images used in the article do not have any identifiable data present.
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
McCarthy, C.J., Harty, J.A. Follow-up study on transphyseal ACL reconstruction in Irish adolescents with no cases of leg length discrepancy or angular deformity. Ir J Med Sci 189, 1323–1329 (2020). https://doi.org/10.1007/s11845-020-02259-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11845-020-02259-7