
Abstract
Recent research suggests that the human gastrointestinal microbiota is greatly involved in yielding, storing and expending energy from the diet; therefore, it may be a further factor in linking diet to obesity. The gut microbial composition is affected by diet throughout the human lifespan, and is highly dynamic and efficient in response to dietary alterations in particular to dietary fibre intake. Short-chained fatty acids (SCFA) are the bi-product of fibre fermentation and have both obesogenic and anti-obesogenic properties. The production of specific forms of SCFAs depends on the microbes available in the gut and the type of fibre ingested. The gut microbiome associated with healthy lean individuals has a higher microbial biodiversity and a greater Bacteroidete to Firmicute ratio compared to the obese individuals associated with microbiome. These gut microbial associations are similar to those seen in individuals with high and low dietary fibre intakes, respectively. Metabolites generated by Bacteroidetes and Firmicutes include the three main SCFA related to obesity, namely butyrate, acetate and propionate. However, neither Bacteroidetes nor Firmicutes is purely causative or purely preventative of obesity. More research is crucial in linking the various types of fibre with particular SCFA production and the microbiome it promotes before suggesting that dietary fibre modulation of the gut microbiome can treat obesity. However, the long-term dietary trend plays the principal role in assembling the diversity and abundance of gut microbes; thus, a sustained diet high in fibre may help prevent obesity by promoting a microbiome associated with a lean phenotype.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The world is currently facing a detrimental obesity epidemic with statistics showing a doubling in numbers over the past 35 years. Six hundred million people worldwide were classified obese in 2014, of which 41 million were young children (< 5 years) [68]. Obesity has been a major problem in the developed world, but has gradually also been established as a key issue in developing countries. According to the Global Burden of Disease 2013 Obesity Collaboration, the high increase in the prevalence of obesity worldwide has slowed down over the past 10 years. However, this is more evident in developing countries [44]. Obesity is frequently accompanied by metabolic health consequences that carry a high economic burden on the health system. Nonetheless, obesity is believed to be preventable. The traditional way of explaining the driver of obesity is the disruption in energy balance, whereby calories consumed are greater than calories expended. Therefore, The World Health Organization (WHO) established the "WHO Global Strategy on Diet, Physical Activity and Health" which attempts to strategically plan how to induce lifestyle changes globally to halt the increasing obesity numbers by 2025. However, this has been a relatively unsuccessful intervention to date.
After attempts by numerous researchers worldwide to clarify the cause of the current obesity epidemic, it has become clear that diet and physical activity alone cannot be blamed. It has consequently been suggested that individual predisposition to obesity is affected by both environmental and genetic interactions. The FTO gene was first identified as an obesity-related gene in 2007 by Jonsson et al. which revealed its association with obesity in Caucasians [29]. This was later established in succeeding studies [43]. The risk allele, FTO rs9939609, is caused by a single-nucleotide polymorphism in the FTO gene and is associated with increased BMI and body weight (+ 1.5 kg/risk allele) [29]. Moreover, a recent genome-wide epigenetic and transcriptome analysis of adipocytes from 105 Caucasian men, found novel candidate genes for obesity with functional roles in the fat supply pathways controlled by epigenetic modifications: HAND2, HOXC6, PPARG, SORBS2, CD36 and CLDN1. PPARG plays a crucial role in adipogenesis and differentiation, and was found to be further hypermethylated in omental visceral adipose tissue (OVAT) compared to subcutaneous tissue (SAT) [31]. This was noteworthy as co-morbidities linked to obesity have a greater association with OVAT than SAT [24, 64]. Furthermore, this was the first epigenome-wide study conducted in the hunt for obesity-related methylation patterns of genes.
Other studies have proven time and again, in both human and rodents, that expression of genes encoding inflammatory proteins in adipocytes correlate with adiposity [11, 42]. Research on inflammatory protein-coding genes was conducted in an attempt to explain an increased concentration of systemic inflammatory markers observed in an obese population compared to a lean population in the 1960s. Today, systemic low-grade inflammation is considered a ‘hallmark’ of obesity that can lead to severe damage to human organs and tissues including the pancreas, skeletal muscle, the liver, peripheral vascular system and the central nervous system. This in turn can contribute to the progression of various metabolic diseases such as type II diabetes mellitus (T2DM), non-alcoholic fatty liver disease, cardiovascular disease, some cancer categories and other diseases with aberrant metabolic pathways [30]. Although there are several molecular causes that link obesity and disease, inflammation is thought to be one of the major players. Studies to date have mainly focused on adipose tissue and its pro-inflammatory potential in obesity [11, 42], but for the purpose of this review, the link between the gut microbiome and inflammation will be emphasised. Recent obesity research suggests that the human gastrointestinal microbiota is significantly involved in yielding, storing and expending energy from the diet [19], and that the microbial composition of the gut in obese individuals is linked to a more permeable gut barrier [28]. Thus, food choice and intestinal bioavailability facilitated by microbial species typical of the obese gastrointestinal tract as well as a highly permeable gut barrier may prove to be additional contributing factors to the pathophysiology of obesity.
The gastrointestinal microbiome
The human gut is populated by a large variety of microbial communities that play major roles in human health and disease [25]. These include eukaryotes, archaea, bacteria and viruses [27], whereof four bacterial phyla have been identified as dominant in the human gut: Bacteroidetes, Firmicutes, Actinobacteria and Proteobacteria [71]. It was previously thought that there were ten times more commensal bacteria than human cells in the body [51], but recently, it has emerged that the ratio of bacteria to human cells is more likely closer to 1:1 [55]. In spite of the ratio being lower than initially expected, it still implies that these microbial populations serve a rather key role in human biological processes and are crucial for human life. The gastrointestinal tract contains bacteria that are protective, as well as bacteria that can be harmful to the human body. Crosstalk and cross-regulation between the host and the gut microbiota build a homeostatic stability of microbes. Any instability in the gut microbiome can contribute to health issues, such as obesity and irritable bowel disease. Such an imbalanced gut microbiome has been designated the term ‘dysbiosis’ [18]. It is well known that gut microbial composition is affected by a variety of factors such as age [34, 47], genetics [10, 48], host milieu [48], and nutritional intake [20, 65, 69]. With respect to the latter, diet has an impact upon the composition as well as the function of the microbiota. This review will consider the feasibility of modifying the gut microbial signature associated with obesity by dietary fibre to promote a gut microbiome associated with health.
The human microbiome project
Joshua Lederberg was the first researcher to propose the term human microbiome to describe an ecological community made up of different microbial species that are mutually dependent on each other and are co-habiting within the human body [35]. Due to the highly evolutionary conserved nature of the 16S rRNA coding genes in prokaryotes, 16S rRNA technology is the main method applied to investigate phylogenetic associations and structures among commensal microbiota as well as for quantifying microbes. Most of the original research of the microbial communities associated with the human body including the gut microbiome was conducted using microbiological cultures employing 16S rRNA gene sequencing. However, many microbes cannot be grown in culture. Thus, the diversity of microbes was previously miscalculated causing an incomplete image of the phylogenetics. Due to the limitations associated with previous 16S rRNA technology and the aspiration to investigate the host-microbe interactions, it is now more common to perform gene sequencing of material taken straight from environmental samples, such as faecal samples [46]. In 2008, the US National Institute of Health (NIH) established the Human Microbiome Project (HMP) to investigate and identify the microbial species present in the human body and to identify the differences between the microbiome in healthy and diseased individuals [27]. Genome sequences were generated by the HMP. The HMP developed better cultivation techniques and protocols with a view to identify correlations between the human microbiome and disease as well as to identify a healthy microbiome. This involved characterising the human microbiome to an extent that would allow for research to study the differences in the microbiome upon variations in extrinsic and intrinsic factors such as nutritional and genetic factors, respectively. The second phase involved linking specific microbial signatures with disease and health [46]. For the purpose of this review, merely a subdivision of the human microbiome will be considered, that is the gut microbiome.
The HMP developed a single standardised 16S rRNA sequencing method to make sure all sequencing centres involved in the project would be using the same procedures. The 16S rRNA gene has nine variable regions that are the most useful for forming taxon units, whereof variable region 3 to 5 (V35) was the region elected for sequencing. This standardisation ensured uniformity in the high-throughput data production and improved taxonomic classification and operational taxonomic unit (OTU). An evaluation of whole-genome sequencing (WGS) between the four centres involved in the HMP project demonstrated great uniformity of target sequencing depth and positive outcomes. In conclusion, the HMP managed to create a publicly accessible microbiome reference library that is dependable. This has allowed researchers progress more rapidly in the field of microbiome and health.
The healthy gut microbiome: a first characterisation
In 2012, the HMP finally delivered a first characterisation of the gut microbiota in healthy adults in a US population. The microbiome was characterised from self-collected stool samples of 242 screened and phenotyped individuals. One hundred twenty-four classified and characterised communities were sequenced using 16S rRNA and WGS [28]. Microbial diversity is based on two aspects: (1) the overall abundance of each microbial species and (2) the overall diversity in species [51]. The gut microbiome showed a considerably higher microbial diversity when analysing stool samples compared to samples taken from other cavities in the human body. There were no taxa found to be existent in 100% of the subject population. This confirmed the colossal variety in microbial species found in the gut. On the other hand, there were many pathways that were evident in all individuals. Therefore, indicating a functional overlap among different taxa as certain pathways exhibited a non-dependency of any particular taxa [28]. Bacteroides were identified as the most universally abundant taxa and the subclass Bacteroides thetaiotaomicron was established in 46% of the subjects. Prevotella copri was the most abundant at a genus level. However, none of these were evident in all subjects. Nonetheless, as already stated, the metabolic pathways were consistent throughout the subjects. These included pathways that are involved in vital biological functions in the human body, such as mRNA translation, ATP production and glucose break down [28]. Therefore, it is evident that microbial interactions with human host cells and other microbes are vital for a healthy gastrointestinal milieu and an overall healthy body. Furthermore, temporal monitoring of intra- and inter-individual microbial diversity and metabolic capacity revealed greater variation between individuals. This was evident in both the composition of microbes as well as the metabolic function of the microbes present [28].
The worldwide obesity epidemic has motivated researchers to identify what environmental influences affect human energy balance. Although lifestyle interventions including dietary approaches have been reasonably successful in prompting initial weight loss, as much as 80% of successful diet cases regain the weight within 12 months, often regaining even more weight than pre-initial weight loss [3]. Therefore, alternative weight loss methods are necessary. Consequently, a novel theory has arisen involving modulation of the gut microbiome. Defining an obese gut microbial signature could drive the development of future personalised therapeutics to fight obesity. Hypothetically, personalised drug and/or dietary treatment could be applied to manipulate an individual’s gut microbial composition and abundance to promote a more health supportive microbial structure.
Gut microbial signature in obese humans
The Bacteroidetes and the Firmicutes are the main favourable bacterial communities found in the human gut. Ley et al. showed that the human gut microbiome has a decreased Bacteroidetes to Firmicutes ratio in an obese population compared to a lean population, and that this ratio increases upon weight loss. Furthermore, an escalation in numbers of Bacteroidetes was associated with loss of adiposity as a result of dietary restrictions. The caloric intake, however, was not associated with Bacteroidete quantity, indicating that the microbes which inhabit the gut are directly linked with adiposity [37]. Turnbaugh et al. confirmed this in a study of female weight concordant monozygotic (MZ) and dizygotic (DZ) twin pairs of European and African descent. Twin studies can be highly valuable when evaluating the impact of genes versus environment on the microbial structure in the human gut. Several regions of the bacterial 16S rRNA from faecal samples were sequenced, and the highest similarity in microbial community organisation was seen within twin pairs for all regions of the 16S rRNA. Unrelated individuals showed a significantly lower correlation in microbial composition. There were, on the other hand, several microbial genes that were very common across the board. Using the words of Turnbaugh, these microbes make up the so-called core microbiome, and any deviation from the ‘core’ are signs of dysbiosis and is related to obesity or disease (see Fig. 1). On the other hand, no single microbial phylotype existed at high levels in the entire sample size. However, some vital metabolic functions were highly evident in the entire sample population. Thus, various species must have the same function. This would explain the combination of large diversity in species and low diversity in metabolic functions across the participants. Bacteroidete and Firmicute numbers were altered in obese participants, decreased and increased, respectively. High functional diversity was associated with high Bacteroidete numbers, typically seen in lean individuals. However, a low functional diversity was associated with a Firmicute-enriched microbiome, typically seen in obese individuals. Furthermore, an overall poor microbial diversity was associated with obesity [63].

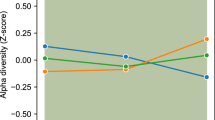
Differences in microbial composition between lean and obese individuals: the lean-associated microbiome has a higher microbial biodiversity and a high Bacteroidete to Firmicute ratio compared to the obesity-associated microbiome
Unfortunately, the studies investigating the microbial composition in obese individuals have given highly inconsistent results. The HMP as well as another large study conducted by MetaHIT (Metagenomics of the Human Intestinal Tract) found no relationship whatsoever between Bacteroidetes/Firmicutes ratio and obesity [4, 28]. However, the HMP revealed similar results to Turnbaugh et al. in regard to microbial diversity with obesity. The microbial signature in obese individuals presented a similar degree of intra-individual variability to healthy individuals, but obesity was associated with an overall poor microbial diversity compared to the lean participants [28]. Nevertheless, a meta-analysis including the four aforementioned studies, HMP, MetaHIT, Ley et al. and Turnabough et al. concluded that neither the Bacteroidetes/Firmicutes ratio nor the gut microbiome community diversity was associated with obesity or BMI. In fact, they noted a greater inter-individual variation among the studies than intra-individual between lean and obese individuals [23]. Turnbaugh and Ley conducted the studies before the HMP and the highly standardised protocols they developed. Thus, the inconsistent results could be due to the varying methods used across the studies. It may also be that there is no single obese gut microbial signature, but several combinations which are associated with obesity. It may be more valid to investigate the gut microbial metabolic pathways rather than the microbial variety and abundance in obese versus lean individuals, or by having a closer look at the microbial composition at a lower taxonomic level.
Human faecal microbiota transplantation
Faecal microbiota transplantation (FMT) is a method whereof microbiota from healthy donors is engrafted into patients suffering from dysbiosis in attempt to establish a homeostatic microbiome. FMT treatment of patients with Clostridium difficile infection (CDI) has eliminated the infection in more than 90–95% of cases and 62–71% of FMT-treated IBD patients have presented with fewer symptoms [18]. It is therefore hypothesised that FMT may be an efficient method to treat other health issues related to dysbiosis, including obesity. There is not enough evidence to date to say that FMT can help treat obesity in humans. However, there are ongoing clinical trials performing FMT from lean to obese patients to investigate the effect of gut bacteria on weight (https://clinicaltrials.gov/). Thus, the future may reveal that FMT is a worthy clinical method to treat obesity and obesity-related disease. Nonetheless, there are some major apprehensions around FMT such as the risk of pathogenic bacterial transfer and ethical acceptance. As to the safety of FMT in humans, only self-limiting side-effects have been documented to date. This included diarrhoea, fever, tiredness and stomach ache [33]. Although FMT is not the traditional obesity cure in humans, mice models have time after time revealed positive results with FMT from lean to obese mice [58].
Gut microbiome and obesity mouse models
Murine models are commonly used for gut microbial research for two main reasons: (1) murine models make it easier to control for extrinsic factors and (2) the anatomy, physiology and genetics between humans and murine are highly similar [45]. Murine models are therefore extremely useful when trying to establish if the gut microbiome is the cause or consequence of disease as well as to advance theories about the mechanistic and functional roles of the microbiome. Both gene knockout and germ-free mouse models have been highly valuable in intervention studies that would not be feasible to execute in humans. On the other hand, it is important to keep in mind the differences between the gastrointestinal system of mice and humans when interpreting the results. Although the gastrointestinal organ arrangement is comparable on an anatomical level, the various sections vary in size relative to the human and mouse dimensions. For instance, the relative mouse cecum is much larger than the relative human cecum, and plays a much larger role in digestion and metabolism than the human cecum. On the other hand, the fermentation of dietary carbohydrates is bound to the large intestine in humans, unlike in mice. Moreover, the mouse intestinal surface area is larger than the human surface area relative to size, as a result of taller villi. These factors in combination allow mice to more efficiently extract nutrients from indigestible food sources than humans. There are also differences on a microscopic and cellular level [45]. Furthermore, the gut microbial species associated with healthy mice and humans also differ on a taxonomic level, 85% of bacterial genera established in the mouse gut have been reported to be non-existent in the human gut [36]. However, mouse models have proven to be very useful in gut microbial studies. Nonetheless, interpretation of results and translation into humans must be done with caution.
Germ-free mice initiated the large interest in gut microbiota and its possible role in obesity after researchers discovered that germ-free mice had lower adiposity than conventional mice and were protected from developing obesity upon exposure to a western diet (devoid of fibres and high in saturated fat and sucrose) [7]. Subsequently, dissimilarity in gut microbial species subdivisions of obese and lean mice was recorded in numerous studies [26, 62]. One study observed that obese mice had as little as half of the Bacteroidete numbers compared to lean mice, but double the amount of Firmicutes [61]. This was similar to what had been reported in some human studies [37, 63].
It has been suggested that obese mouse gut microbes more effectively absorb energy from food consumed [5, 6]. Backhed et al. observed a 60% rise in adipose tissue within a 2-week period in germ-free mice colonised with gut microbes. This was seen in spite of a lower caloric intake pre-colonisation. The whys and wherefores were put down to a variety of mechanisms including the fermentation of dietary polysaccharides to short-chained fatty acids (SCFA) by the gut microbes which allowed for intestinal absorption and therefore increased calorie intake. The human proteome lacks the glycoside hydrolases necessary to break down dietary polysaccharides; thus, dietary polysaccharides are indigestible in the absence of microbes with a proteome containing this enzyme [56]. Turnbough et al. reported in 2006 that the caecal microbiota in mice with diet-induced obesity (DIO) from exposure to a typical western diet promoted Mollicutes (a clade within the Firmicutes) to thrive as well as to reduce the global microbial diversity. Interestingly, phylogenetically related Mollicutes have been observed in the human gut microbiome [37] as well as reduced microbial diversity in obese human microbiomes [63]. Nonetheless, dietary modulation, both carbohydrate-restricted and fat-restricted diets, caused a reduction in the cecum Mollicute numbers and stimulated weight loss. Furthermore, adipogenesis was higher in germ-free mice with a donated microbiome from mice with DIO than from lean donors. Metagenomic analyses pointed towards an increased capacity of Mollicutes to bring in and process monosaccharides. Western diets tend to be high in simple sugars. Thus, the metagenomic results did give an explanation to the Mollicute explosion. Back et al. also reported that certain microbiota stimulates digestion of simple sugars and that this can lead to adipocyte hypertrophy as monosaccharide absorption prompts the conversion of acetyl-CoA to fatty acids in the liver. Furthermore, Back et al. observed a suppression of fasting-induced adipose factor (Fiaf) in the intestinal epithelium with adipocyte hypertrophy and therefore suggested that the gut microbes promote adipocyte hypertrophy through microbe-gene interactions. Fiaf functions as an inhibitor of lipoprotein lipase (LPL) which in turn is involved in fatty acid uptake into the liver and adipocytes. Fiaf suppression therefore leads to a rise in adipocyte LPL activity as well as amplified lipogenesis in the liver which in turn drive triglyceride storage in adipocytes [5]. These studies point out the potential role of the gut microbiota in controlling energy yield and storage from food taken in. This changes the traditional energy balance equation somewhat. Instead of energy ingested versus energy expended, it may be more accurate to study energy absorbed versus energy expended.
As mentioned earlier, weight regain after dieting is a major concern in humans [3]. A theory that the gut microbiome plays a major role in post-dieting weight regain has recently emerged. Thaiss et al. studied mice of recurrent obesity and found that when exposed to an obesogenic environment (high-fat diet (HFD)), the gut microbial diversity was reduced. Furthermore, upon return to normal weight, the diversity was not fully recovered, but was floating somewhere in between dysbiosis (obese microbial state) and normal state (pre-weight gain). The functional consequence was put down to alterations in gene expression involved in various metabolic pathways, including reduced activity in the isoflavonoid and steroid biosynthesis pathways. It took as much as 21 weeks after weight loss for the microbial composition to return back to the normal composition. This was five times longer than the initial weight gain or dieting stint [58]. Thiass et al. then transplanted the gut microbiome from lean mice that had previously been obese and microbiomes from mice that had never been obese into germ-free mice. The microbiome acceptor mice were then given a HFD. When exposed to a HFD, the mice given the post-obesity microbiome gained significantly more weight than the controls (lean microbiome acceptor mice) as well as exhibited an inferior glucose tolerance. This indicated that the post-dieting microbiome when exposed to a secondary obesogenic environment contributes to an increased vulnerability to weight gain and complications associated with metabolic disorders. The control mice given the HFD also gained weight, but not to the same extent [58].
Gut microbial development in utero and infancy
It was previously thought that the utero environment was sterile, but recent studies have revealed that both the placenta and amniotic fluid contain microbiota [15]. Therefore, the new school of thought is that the neonatal gut is populated by microbes before delivery. Chu et al. investigated if a high-fat diet during pregnancy could alter the neonatal and infant gut microbial composition in early life. Meconium (neonatal stool) sample analyses revealed that the composition varied depending on the quality of the maternal diet during gestation. Mothers with a high-fat gestational diet gave birth to neonates with significantly lower numbers of gut Bacteroides compared to mothers with a control diet (< 35% of caloric intake from fat). Markedly, this gut microbial signature persisted in the babies up to 1.5 months [14]. Backhed et al. evaluated the gastrointestinal microbiome of 98 Swedish mothers and their children from birth to their first birthday. Mode of delivery as well as if the infant was breast-fed or formula fed affected the gut microbial composition, but the main determinant in the maturation of the infants’ gut microbiome was the time of breast-feeding cessation. Subsequent to cessation, there was a distinctive systematic alteration in key bacterial classes which caused the infant gut microbiome to resemble adult gut microbiome [8]. A case study examining the development of the infant gastrointestinal microbiome (n = 60) running over 2.5 years revealed that the phylogenetic diversity steadily expanded over time. On the contrary, key taxa shifted rapidly upon dietary changes. All dietary alterations over the 2.5 years caused alterations in the gut microbiome. The first microbial composition was highly enriched in microbial genes involved in lactate metabolism. However, genes essential for metabolism of solid foods were evident in the infant gut before weaning from milk and starting solid food [32]. The aforementioned studies on gut microbial development in neonates and infants all suggest that diet can alter the gut microbiome.
Modulation of gut microbiota by diet
Diet is linked with obesity. However, as the composition of the gut microbiota is influenced by diet, this may be a contributing factor to obesity. Therefore, it may be that the health impact of a so-called bad diet is in fact enabled by the microbiome. The principals behind the role of the microbiome in human metabolism are remarkably multifaceted; thus, it is very hard to accurately interpret data and to reproduce results. However, in theory, dietary manipulation of the microbiota may be a useful therapeutic tool to treat obesity associated with dysbiosis. For obesity to occur, the microbiota is essential. This has been demonstrated in studies that have executed FMT from obese mice to germ-free mice where the germ-free mice have presented an obese phenotype [58]. The gut microbiota has a highly dynamic and efficient response to big dietary alterations, such as changing from a plant-based to meat-based diet or majorly increasing intake of dietary fibre. Only a couple of days have proven sufficient to see changes in microbial diversity and abundance in the gut after dietary change [16, 70]. In spite of the short-term dietary modulation of the gut microbiome observed in various studies, long-term dietary interventions have revealed that the overall long-term dietary trend is what plays the principal role in assembling the diversity and abundance of gut microbes [69]. However, the extent of alterations in gut microbial composition upon diet changes is highly dependent on the microbial community habitating the gut before the dietary change. A prime example of this was a first of its kind study that revealed that there was a greater gut microbial diversity in children from a traditional African rural population in comparison to European children. The African children were breast-fed for 2 years accompanied with solid food, whereas the European children were only breast-fed for 1 year. The results revealed that the differences between the European and African gut microbial composition were increased upon weaning to solid food, indicating that diet is one of the predominant players in modulating the gut microbiome over other environmental factors. The rural diet was principally vegetarian with the occasional chicken and termite meals. All in all, the rural diet was low-fat, low in animal protein, however high in starch, fibre and plant polysaccharides. On the other hand, the European children had a typical western diet, lacking in fibre and rich in calories from fat, animal protein and sugar. Notably, the fibre intake was more than 40% higher in the African population compared to the European children (14.2 g/day and 8.4 g/day, respectively). Although, the four predominant bacteria were similar in the two populations (Actinobacteria, Bacteroidetes, Firmicutes and Proteobacteria), the Firmicute to Bacteriocide ratio significantly differed. The European cohort had 50% more Firmicutes than the African cohort and a much higher Firmicute to Bacteroidete ratio. Furthermore, the microbial richness and biodiversity was much higher in the rural children compared to the western population. Faecal sample analyses also revealed that the short-chain fatty acid (SCFA) concentration was significantly higher in the African population compared to the European population [17]. SCFAs are a product of gut microbial fermentation of complex dietary plant polysaccharides and have been associated with health benefits such as lower body weight and improved glucose tolerance [13]. Consequently, it was hypothesised that the difference in microbial composition was caused by the difference in fibre intake between the cohorts. As discussed previously, the Firmicutes to Bacteroidete ratio and the microbial richness and diversity have also been reported to differ between obese and lean individuals [37, 63]. Therefore, it may be that the European children with lower dietary fibre intakes are predisposed to obesity as the microbial composition, diversity and abundance was similar to that of associated with obesity.
Short-chained fatty acids
The carbohydrates that escape absorption in the small intestine during digestion, including complex dietary plant polysaccharides or dietary fibre, are fermented by gut bacteria in the large colon to produce SCFAs and other monosaccharides. Some branched-chained amino acids (BCAA) are also fermented by the microbiome into branched SCFA (BSCFA), although only a minute part of the SCFA produced are derived from BCAA fermentation. Therefore, the straight and branched SCFA carbon chains (≤ six carbons) are considered one of the principal mechanisms joining nutrition and gut microbiota [57]. Some SCFAs, predominantly butyrate, are utilised by colonocytes as a source of ATP, while propionate and acetate are absorbed in the large colon and travel to the liver where they play key roles in inducing and participating in gluconeogenesis and de novo lipogenesis, respectively [5, 50].
Ninety to 95% of the SCFAs produced from carbohydrate fermentation products are acetate, propionate and butyrate (see Fig. 2), whereof acetate is the most abundant [40]. Many of the Firmicutes and Bacteroidetes are butyrate and propionate producers in the gut, but each bacterium can normally only produce one of the two. Thus, classifying by Firmicutes and Bacteroidetes is not always sufficient, a lower taxonomic level would allow for a better understanding of the consequence of microbial composition on fermentation of non-digestible dietary components [41]. The SCFA balance is highly dependent on the stability and function of the gut microbes. Gut microbes rely on products produced by other gut microbes as well as products produced by the host. These phenomena are called microbial cross-feeding and microbe-host cross-feeding, respectively. The cross-feeding influences both composition and function of the gut microbiome. Thus, a better understanding of the cross-feeding interactions may be vital in developing dietary strategies to treat or prevent obesity or disease related to dysbiosis [53].

Chemical formula of the three most abundant SCFAs produced in the large colon as a bi-product of fibre fermentation
Fernandez et al. compared dietary intakes, faecal SCFA concentrations and gut microbial profiles in two cohorts: healthy lean and overweight/obese. In spite of similar activity levels and dietary intakes, the SCFAs in the faecal samples did differ, the overweight and obese had significantly higher levels. Furthermore, increased numbers of Bacteroides and Prevotella were associated with less SCFA, while an increased ratio of Firmicutes to Bacteroides was associated with higher SCFA concentration. Thus, the obese cohort had higher levels of SCFAs which was associated with an increased Firmicute to Bacteroide ratio which in turn has also been reported in numerous studies of both obese mice and humans [61, 63]. The study suggested that adjustment of microbial fermentation in the large colon plays a major role in the different SCFA concentrations seen in overweight and obese compared to lean individuals, but that alterations were not due to diet [22]. Additionally, to support this, Rahat-Rozenbloom et al. also reported that obese individuals had higher levels of SCFAs in faecal samples than lean individuals, and that this was not due to differences in diet [52]. It was concluded that diet was not the culprit of the increased SCFAs or the altered gut microbial composition as the diet did not differ between the groups of the two studies. However, dietary fibre intake has been associated with many health benefits, including reduced risk of type 2 diabetes mellitus [66], obesity [60] and cardiovascular disease [59]. In spite of the benefits seen with high-fibre intake, studies have revealed that the bi-product of fibre fermentation, SCFAs, promotes an obesogenic microbiome in spite of the reported beneficial roles of SCFAs and appetite control [21]. This may not be the whole story as not all SCFAs promote the same physiological functions.
Metabolites generated by the Bacteriodetes and Firmicutes include the three main SCFAs related to obesity: butyrate, acetate and propionate. Although, all related to obesity, neither Bacteroidetes nor Firmicutes is purely causative or purely preventative of obesity. Each phylum produces different SCFAs, some of which have opposing effects and functions [12]; thus, highlighting the importance of considering the population ratio of more than one taxon. Al-Lahham et al. demonstrated that propionate plays a role in human energy metabolism by stimulating the expression of the ‘satiety hormone’ leptin [2]. Furthermore, Lin et al. demonstrated that butyrate and propionate protect against diet-induced obesity in mice, but only butyrate and propionate can induce the anorexigenic gut hormone glucagon-like peptide (GLP-1) and peptide YY (PYY). However, butyrate was the most potent hormone stimulator, followed by propionate [38]. On the other hand, increased mice cecal acetate was reported to activate the parasympathetic nervous system and promotes increased secretion of the ‘hunger hormone’ ghrelin and consequently hyperphagia [49]. Therefore, a general classification may perhaps be that acetate is predominantly obesogenic, whereas butyrate and propionate are mainly anti-obesogenic. This highlights the importance of taking the specific SCFAs into account and not only the total SCFAs in studies that are investigating the link between the microbiome and SCFAs in obesity.
Dietary fibre and obesity
The traditional obesity imbalance of too much energy consumed and too little energy expended changes when taking consumption of dietary fibre into consideration. Fibre can be fully fermented in the large colon or only partly fermented, and thus, the energy absorption varies. Furthermore, increased ingestion of fibre reduced the energy absorbed from the energy available in the diet by reducing the fat and protein digestibility [1]. Notably, the inverse relationship between dietary fibre and energy absorption was independent of dietary fat; thus, the same effect of increased dietary fibre was evident with both high- and low-fat diets [9]. Therefore, it may be more correct to say that the obesity imbalance is caused by too much energy absorbed and too little energy expended. Dietary fibre may therefore be helpful for weight management since the energy in fibre-rich foods is less bioavailable. Tucker et al. conducted a study to investigate if changes in fibre intake could influence the risk of gaining weight over time in a female cohort (n = 252) and found that weight decreased by 0.25 kg for each 1 g increase in total fibre consumed. Over 20 months, the women lost an average of 2 kg by increasing their fibre intake by 8 g / 1000 kcal. Tucker et al. concluded that eating more foods high in dietary fibre can significantly reduce the risk of gaining weight in women independent of physical activity levels and dietary fat intake. Fibre and whole grains are nutritionally rich sources containing vitamins, minerals and slow-releasing energy. Moreover, fibre and whole grains contain bio-active non-nutritional compounds secreted by plants termed phytochemicals. Phytochemicals include phenolics, carotenoids, lignans, beta-glucan and inulin. Research has suggested that dietary fibre elicits an array of health properties due to synergistic effects of phytochemicals, high-nutrient content and improvement of digestive operation [39], including beneficial effects on obesity [60]. Thus, the SCFAs produced as a bi-product of microbial fermentation of dietary fibre may not be the only health-promoting component, but other non-nutritional, bio-active components may have additional health-promoting functions.
Subclasses of dietary fibre
Dietary fibre can be categorised into soluble and insoluble fibre, whereof soluble fibre dissolves in water in the large colon and is easily fermentable, and insoluble fibre does not dissolve in water and digestion is therefore limited. Most fibre-containing foods contain both fibre categories [67]. It has therefore become evident that diverse subtypes of fibre elicit different physiological effects. Therefore, although supplementing the diet with resistant starch and dietary fibre does raise intestinal and circulating SCFAs, there may be specific fibre sources that increase the more anti-obesogenic SCFAs. A rat study reported that soluble fibre produces the anorexigenic peptides GLP-1 and PYY after fermentation, both hormones associated with the SCFA butyrate and propionate [1].
Resistant starch, a polysaccharide produced by plants, also falls under the umbrella term dietary fibre. Resistant starch is the starch that bypasses digestion in the small intestine, but is fermented by the gut microbiota in the large colon. Resistant starch can be divided into four subgroups [12]: (1) physically inaccessible starch (RS1), (2) native granules (RS2), (3) retrograded starch (RS3) and (4) chemically modified starch (RS4). A study performed on zebrafish given RS2 or RS4 revealed an increased Bacteroidete to Firmicute ratio in the zebrafish given RS4 [54]. A similar Bacteroidetes to Firmicute ratio which was previously reported in lean human and mice [61, 63]. This indicates that chemically modified starch may be a potential subsidiary tool to modulate the gut microbial composition and promote a lean phenotype.
Conclusion
It has been demonstrated that the human gut microbial composition varies depending on the quality of the maternal diet during gestation [14], if an infant is breast-fed or not [8], the time of solid food introduction [32] as well as short-term and long-term dietary habits in adulthood [16, 70]. Greater SCFA production in the human gut is related to increased microbial richness and biodiversity. Furthermore, microbial diversity differs between obese and lean individuals [37, 63]. These differences are similar to what has been reported between individuals who consume high quantities of dietary fibre versus low quantities of dietary fibre [17]. On the other hand, high SCFA production in the gut has been associated with the obese phenotype. However, dietary fibre intake has been associated with decreased risk of diseases which are generally considered to be obesity-related [59, 66]. Metabolites generated by Bacteroidetes and Firmicutes include the three main SCFAs, that are—butyrate, acetate and propionate [40]. A general classification made in this review based on current literature is that acetate is predominantly obesogenic, whereas butyrate and propionate are mainly anti-obesogenic. This highlights the importance of taking the specific SCFAs into account and not merely the total SCFA content. Furthermore, both Bacteroidetes and Firmicutes produce all three SCFAs [41]. It is therefore necessary to classify the gut microbes at a lower taxonomic level to be able to specify the SCFAs produced by particular microbes. Zebrafish given RS4 revealed an increased Bacteroidete to Firmicute ratio similar to that which has been demonstrated in lean humans. On the other hand, such a ratio was not promoted in zebrafish given RS2 [54]. This implies that not all dietary fibre sources promote the same microbial species. Therefore, an in depth understanding of the effect on microbial composition upon ingestion of different fibre groups is necessary to help explain how a specific metabolic input can alter the gut microbial composition over time. There is not enough evidence to say that the gastrointestinal microbiota can be modulated by dietary fibre to treat obesity. However, the long-term dietary trend plays the principal role in assembling the diversity and abundance of gut microbes [69]; thus, a long-term diet high in fibre may help prevent rather than treat obesity by promoting a microbiome associated with a lean phenotype.
References
Adam CL et al (2014) Different types of soluble fermentable dietary fibre decrease food intake, body weight gain and adiposity in young adult male rats. Nutr Metab 11(1):36
Al-Lahham SH et al (2010) Regulation of adipokine production in human adipose tissue by propionic acid. Eur J Clin Investig 40(5):401–407
Anastasiou CA, Karfopoulou E, Yannakoulia M (2015) Weight regaining: from statistics and behaviors to physiology and metabolism. Metabolism 64(11):1395–1407
Arumugam M et al (2011) Enterotypes of the human gut microbiome. Nature 473(7346):174–180
Backhed F et al (2004) The gut microbiota as an environmental factor that regulates fat storage. Proc Natl Acad Sci U S A 101(44):15718–15723
Backhed F et al (2005) Host-bacterial mutualism in the human intestine. Science (New York, NY) 307(5717):1915–1920
Bäckhed F et al (2007) Mechanisms underlying the resistance to diet-induced obesity in germ-free mice. Proc Natl Acad Sci 104(3):979–984
Bäckhed F et al (2015) Dynamics and stabilization of the human gut microbiome during the first year of life. Cell Host Microbe 17(5):690–703
Baer DJ et al (1997) Dietary fiber decreases the metabolizable energy content and nutrient digestibility of mixed diets fed to humans. J Nutr 127(4):579–586
Benson AK et al (2010) Individuality in gut microbiota composition is a complex polygenic trait shaped by multiple environmental and host genetic factors. Proc Natl Acad Sci U S A 107(44):18933–18938
Braune J. et al. (2017) IL-6 regulates M2 polarization and local proliferation of adipose tissue macrophages in obesity. J Immunol 1600476
Chakraborti CK (2015) New-found link between microbiota and obesity. World J Gastrointest Pathophysiol 6(4):110–119
Chambers ES et al (2015) Effects of targeted delivery of propionate to the human colon on appetite regulation, body weight maintenance and adiposity in overweight adults. Gut 64(11):1744–1754 Available at: http://gut.bmj.com/lookup/doi/10.1136/gutjnl-2014-307913
Chu DM et al (2016) The early infant gut microbiome varies in association with a maternal high-fat diet. Genome Med 8(1):77
Collado MC et al (2016) Human gut colonisation may be initiated in utero by distinct microbial communities in the placenta and amniotic fluid. Sci Rep 6:23129
David LA et al (2014) Diet rapidly and reproducibly alters the human gut microbiome. Nature 505(7484):559–563
De Filippo C et al (2010) Impact of diet in shaping gut microbiota revealed by a comparative study in children from Europe and rural Africa. Proc Natl Acad Sci U S A 107(33):14691–14696
DeGruttola AK et al (2016) Current understanding of dysbiosis in disease in human and animal models. Inflamm Bowel Dis 22(5):1137–1150
DiBaise JK, Frank DN, Mathur R (2012) Impact of the gut microbiota on the development of obesity: current concepts. Am J Gastroenterol Suppl 1(1):22–27
Duncan SH et al (2007) Reduced dietary intake of carbohydrates by obese subjects results in decreased concentrations of butyrate and butyrate-producing bacteria in feces. Appl Environ Microbiol 73(4):1073–1078
Eckburg PB et al (2005) Diversity of the human intestinal microbial flora. Science 308(5728):1635–1638
Fernandes J et al (2014) Adiposity, gut microbiota and faecal short chain fatty acids are linked in adult humans. Nutr Diabetes 4
Finucane MM et al (2014) A taxonomic signature of obesity in the microbiome? Getting to the guts of the matter. PLoS One 9(1):e84689
Gómez-Hernández A et al (2016) Differential role of adipose tissues in obesity and related metabolic and vascular complications. Int J Endocrinol 2016:1–15
Guinane CM, Cotter PD (2013) Role of the gut microbiota in health and chronic gastrointestinal disease: understanding a hidden metabolic organ. Ther Adv Gastroenterol 6(4):295–308
Hildebrandt MA et al (2009) High-fat diet determines the composition of the murine gut microbiome independently of obesity. Gastroenterology 137(5):1716–1724.e2
Human Microbiome Project Consortium, T. (2012a) A framework for human microbiome research. Nature 486
Human Microbiome Project Consortium, T. (2012b) Structure, function and diversity of the healthy human microbiome. Nature 486
Jonsson A et al (2009) Assessing the effect of interaction between an FTO variant (rs9939609) and physical activity on obesity in 15,925 Swedish and 2,511 Finnish adults. Diabetologia 52(7):1334–1338
Katzmarzyk PT et al (2005) Metabolic syndrome, obesity, and mortality. Diabetes Care 28(2)
Keller M et al (2017) Genome-wide DNA promoter methylation and transcriptome analysis in human adipose tissue unravels novel candidate genes for obesity. Mol Metab 6(1):86–100
Koenig JE et al (2011) Succession of microbial consortia in the developing infant gut microbiome. Proc Natl Acad Sci 108(Supplement_1):4578–4585
Kunde S et al (2013) Safety, tolerability, and clinical response after fecal transplantation in children and young adults with ulcerative colitis. J Pediatr Gastroenterol Nutr 56(6):597–601
Lakshminarayanan B et al (2014) Compositional dynamics of the human intestinal microbiota with aging: implications for health. J Nutr Health Aging 18(9):773–786
Lederberg J, Mccray AT (2001) ‘Ome sweet ‘omics—a genealogical treasury of words. Scientist 15(7):8–8
Ley RE et al (2005) Obesity alters gut microbial ecology. Proc Natl Acad Sci U S A 102(31):11070–11075
Ley R et al (2006) Microbial ecology: human gut microbes associated with obesity. Nature 444(7122):1022–1023
Lin HV et al (2012) Butyrate and propionate protect against diet-induced obesity and regulate gut hormones via free fatty acid receptor 3-independent mechanisms. L. Brennan, ed. PloS one 7(4):e35240
Liu RH (2003) Health benefits of fruit and vegetables are from additive and synergistic combinations of phytochemicals. Am J Clin Nutr 78(3 Suppl):517S–520S
Louis P et al (2007) Understanding the effects of diet on bacterial metabolism in the large intestine. J Appl Microbiol 102(5):1197–1208
Louis P et al (2010) Diversity of human colonic butyrate-producing bacteria revealed by analysis of the butyryl-CoA:acetate CoA-transferase gene. Environ Microbiol 12(2):304–314
Mengel E. et al (2017) Changes in inflammatory markers in Estonian pubertal boys with different BMI values and increments: a 3-year follow-up study. Obesity
Mizuno TM et al (2017) Negative regulation of hepatic fat mass and obesity associated (Fto) gene expression by insulin. Life Sci 170:50–55
Ng M et al (2014) Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the global burden of disease study 2013. Lancet 384(9945):766–781
Nguyen TLA et al (2015) How informative is the mouse for human gut microbiota research? Dis Model Mech 8(1):1–16
NIH HMP Working Group, TNHW et al (2009) The NIH human microbiome project. Genome Res 19(12):2317–2323
Odamaki T et al (2016) Age-related changes in gut microbiota composition from newborn to centenarian: a cross-sectional study. BMC Microbiol 16(1):90
Org E et al (2015) Genetic and environmental control of host-gut microbiota interactions. Genome Res 25(10):1558–1569
Perry RJ et al (2016) Acetate mediates a microbiome–brain–β-cell axis to promote metabolic syndrome. Nature 534(7606):213–217
Pryde SE et al (2002) The microbiology of butyrate formation in the human colon. FEMS Microbiol Lett 217(2):133–139
Qin J et al (2010) ARTICLES a human gut microbial gene catalogue established by metagenomic sequencing. Nature 464
Rahat-Rozenbloom S et al (2014) Evidence for greater production of colonic short chain fatty acids in overweight than lean humans. Int J Obes 38(12):1525–1531
Ríos-Covián D et al (2016) Intestinal short chain fatty acids and their link with diet and human health. Front Microbiol 7:185
Semova I et al (2012) Microbiota regulate intestinal absorption and metabolism of fatty acids in the zebrafish. Cell Host Microbe 12(3):277–288
Sender R, Fuchs S, Milo R (2016) Revised estimates for the number of human and bacteria cells in the body. PLoS Biol 14(8):e1002533
Sonnenburg JL, Bäckhed F (2016) Diet–microbiota interactions as moderators of human metabolism. Nature 535(7610):56–64
Sonnenburg JL et al (2005) Glycan foraging in vivo by an intestine-adapted bacterial symbiont. Science 307(5717):1955–1959
Thaiss CA et al (2016) Persistent microbiome alterations modulate the rate of post-dieting weight regain. Nature 540(7634):544–551
Threapleton DE et al (2013) Dietary fibre intake and risk of cardiovascular disease: systematic review and meta-analysis. BMJ 347:f6879–f6879
Tucker LA, Thomas KS (2009) Increasing total fiber intake reduces risk of weight and fat gains in women. J Nutr 139(3):576–581
Turnbaugh PJ et al (2006) An obesity-associated gut microbiome with increased capacity for energy harvest. Nature 444(7122):1027–1031
Turnbaugh PJ et al (2008) Diet-induced obesity is linked to marked but reversible alterations in the mouse distal gut microbiome. Cell Host Microbe 3(4):213–223
Turnbaugh PJ et al (2009) A core gut microbiome in obese and lean twins. Nature 457(7228):480–484
Vega GL et al (2006) Influence of body fat content and distribution on variation in metabolic risk. J Clin Endocrinol Metab 91(11):4459–4466
Walker AW et al (2011) Dominant and diet-responsive groups of bacteria within the human colonic microbiota. ISME J 5(2):220–230
Weickert MO, Pfeiffer AFH (2008) Metabolic effects of dietary fiber consumption and prevention of diabetes. J Nutr 138(3):439–442
Wong JMW, Jenkins DJA (2007) Carbohydrate digestibility and metabolic effects. J Nutr 137(11 Suppl):2539S–2546S
World Health Organization (2016) WHO | obesity and overweight. WHO
Wu GD et al (2011) Linking long-term dietary patterns with gut microbial enterotypes. Science (New York, NY) 334(6052):105–108
Wu GD et al (2016) Comparative metabolomics in vegans and omnivores reveal constraints on diet-dependent gut microbiota metabolite production. Gut 65(1):63–72
Xu M-Q et al (2015) Fecal microbiota transplantation broadening its application beyond intestinal disorders. World J Gastroenterol 21(1):102–111
Acknowledgements
The author is grateful to Professor Derek Doherty and Dr. Henry Windle in the MSc. Molecular Medicine course, Trinity College Dublin, for their support during the writing of this review. The author would also like to thank the reviewer for the kind comments that greatly improved this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The author declares that she has no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by the author.
Rights and permissions
About this article

Cite this article
Davis, H.C. Can the gastrointestinal microbiota be modulated by dietary fibre to treat obesity?. Ir J Med Sci 187, 393–402 (2018). https://doi.org/10.1007/s11845-017-1686-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11845-017-1686-9