
Abstract
Background
In the setting of a national audit of acute stroke services, we examined the delivery of thrombolytic therapy for ischaemic stroke and whether current practice was achieving safe outcomes and consistent delivery for patients.
Method
Data obtained from the recent national stroke audit was compared against previous Irish audit, the most recent SSNAP UK stroke audit and the Safe Implementation of Thrombolysis in Stroke-Monitoring Study (SITS-MOST) study.
Results
Thrombolysis was provided in 27 acute hospitals throughout Ireland during the period assessed with 82% (22/27) providing 24/7 access, the remaining sites using redirect policies. Decision to thrombolyse was made by stroke trained consultants in 63% (17/27) of units, with general physicians and emergency medicine consultants covering the other units. Thrombolysis rate for non-haemorrhagic stroke was 11% (n = 80/742, CI 95% ±2.23) versus a 1% rate in the 2008 audit. Sites receiving patients through a redirect policy had the highest thrombolysis rate, an average of 24%. Nearly 30% of cases were thrombolysed on the weekend. Eighty-three percent of cases were managed in a stroke unit at some time during admission versus 54% of the national total cases. Thirty-seven percent of patients were ≥80 years old. The mortality rate was 11.3% versus the national mortality rate for non-thrombolysed ischaemic strokes of 10% (p > 0.5), and this is comparable to the SITS-MOST 2007 study 3-month mortality rate of 11.3% (p > 0.5).
Conclusion
Stroke thrombolysis is being effectively and safely provided in acute stroke services in Ireland despite regular involvement of non-specialist staff. There is still potential to improve thrombolysis rate.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The evidence for thrombolysis of acute ischaemic stroke was established by the NINDS trial in 1995 [1], and a conditional licence for the therapy was granted by the European Union (EU) in 2001. The licence was made permanent following the publication of the Safe Implementation of Thrombolysis in Stroke-Monitoring Study (SITS-MOST) and extended to 4.5 h following the publication of the European Cooperative Acute Stroke Study (ECASS) III [2, 3].
Ireland lagged behind other countries in the development of organised stroke services. In 2008, the first Irish National Audit of Stroke Care (INASC 2008) was published [4]. A review of 2173 cases revealed that only 1% of patients received thrombolytic therapy, compounded by the fact that there was only one stroke unit in existence in the whole country.
In response in 2010, the Irish health service implemented the national stroke programme with the stated aim of developing rapid access to best-quality stroke services and reducing death and disability due to stroke [5]. These aims were targeted through a number of measures including infrastructural change, limited specialist recruitment, and guideline development, which facilitated a national programme for thrombolysis therapy. Unfortunately, this coincided with a financial collapse and severe economic recession in the country, which severely limited the extent of new resource, which could be allocated to develop services. A further challenge was in the distribution of population and acute hospitals across Ireland. Outside the largest cities of Dublin, Cork, Galway, and Limerick, populations are quite dispersed. For example, population density in County Dublin is 1459/km2 compared with a population density of <50/km2 in 16 of the remaining 25 counties in the Republic of Ireland [6]. These areas are supported by a large number of smaller hospitals who are typically unable to provide 24-h cover by specialist stroke services. This means that conventional means of delivering thrombolysis by stroke specialists is often impossible.
A combination of strategies, under the guidance of the National Clinical Programme for Stroke, was employed to deliver thrombolysis therapy to the entire country including developing a training programme for general physicians to identify and thrombolyse potentially eligible patients, application of a redirect policy in certain areas to allow ambulance paramedics to divert suitable patients to hospitals providing thrombolysis, and introduction of a limited stroke telemedicine service in other areas. In 2015, we repeated a national study to determine the effectiveness of these interventions on thrombolysis practice and safety in Ireland [7].
Methods
The Irish audit of acute hospital services (NSA 2015) had two components, an audit of the organisational aspects of stroke care in acute hospitals and a clinical audit of stroke care involving the review of clinical case notes for a selected national sample of patients with stroke, with audit protocol approved by a national stroke audit steering group. The data were obtained by the use of validated surveys adapted from the INASC 2008-validated proforma, which, in turn, was based on the Royal College of Physicians London (RCPUK) National Sentinel Stroke Audit 2004 Organisational Audit proforma and National Sentinel Stroke Audit 2006 Clinical Audit proforma. Modifications and additional questions were added to allow comparison of results with those from the larger UK SSNAP database and with European Stroke Organisation Guidelines. A copy of the audit proforma is included in the supplementary appendix.
The clinical outcomes of patients were studied during the specified 6-month period (1 January 2014–31 March 2014 and 1 July 2014–30 September 2014) with a primary diagnosis of stroke (ICD code, I61, I63, I64). Subjects with classification I60 (subarachnoid haemorrhage) were not studied as these patients are predominantly redirected to neurosurgery centres in Ireland under defined protocol.
The data was compared with the findings of the previous Irish audit (INASC 2008), the Sentinel Stroke National Audit Programme (SSNAP) UK acute organisational audit 2014, and the SITS-MOST including data specifically related to the UK [2, 4, 8], Ireland not having participated to any large extent in SITS-MOST.
Results
Organisation of service
Twenty-seven hospitals were identified as managing acute stroke patients in Irish hospitals in 2015, a reduction from the 37 sites identified in the 2008 audit (Fisher’s exact test, p = 0.001). Twenty-six (97%) of the sites had 24/7 coverage for thrombolysis either through on-site access or through an emergency service redirect policy. Twenty-four-hour emergency non-contrast CT imaging was available in all sites. Eighty-five percent of sites had access to a senior stroke trained specialist, increased from 32% in the previous audit (Table 1). The decision to thrombolyse was taken by a specialist (predominantly geriatricians) in 17 (63%) sites, general physicians in eight (30%) sites, and emergency department consultants in two (7%) sites. Thrombolysis was delivered in the emergency department in 22 (82%) sites, in a high dependency bed (e.g. ICU/CCU) in four (15%) sites, and in a stroke unit in one site.
Access to specific components of hyperacute care is still lower than the UK (Table 2). Stroke units were in 78% (21/27) of sites versus 99% (165/167) in the SSNAP UK (p < 0.1). Specialists were available in 83% (23/27) versus 99% (181/183) of sites in the UK (p < 0.001). When assessed against the European Stroke Organisation Guidelines for key features for primary stroke centres providing hyperacute care, 22% (6/27) of sites meet recommended requirements (Table 3).
Clinical outcomes
Of the total audit sample of 874 cases from 2014, 80 patients received thrombolysis, which represents a thrombolysis rate for non-haemorrhagic stroke of 11% (n = 80/742, confidence interval 95% ±2) versus a 1% rate in the 2008 audit. The highest thrombolysis rates were achieved in sites, which received patients via a redirect policy, with an average rate of 24% (37/154). Higher rates were also observed in centres with a stroke specialist versus general physicians (excluding redirect sites), 10.5 versus 5%, respectively (p < 0.1). The median age was 73 (range 36–93), and 36% of patients were ≥80 years old, with 84% (67/80) described as independent pre-stroke and 6% living in residential care pre-admission. These were similar to the non-thrombolysed ischaemic stroke patients (Table 4).
Following on from treatment with thrombolysis, 83% (66/80) of cases were managed in a stroke unit at some time during admission versus 51% (406/793) of the remaining national total cases (p < 0.001). Half of thrombolysed patients (40/874, 4.6% of total cases) are initially managed in high dependency beds (ICU/HDU), compared with less than 2% of all stroke patients being initially managed in a high dependency bed in the UK (p < 0.001).
The mortality rate for thrombolysed strokes to discharge was 11.3% (CI ±6.9) versus the national mortality rate for non-thrombolysed ischaemic strokes of 10% (CI ±2.3) (chi-square test, p > 0.5). Similar numbers of patients were discharged to residential care, 7.5% of thrombolysed cases versus 7.1% of non-thrombolysed cases (chi-square test, p > 0.5).
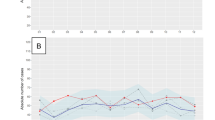
Of the 645 non-thrombolysed ischaemic strokes, 32% (207/645) had a precise time of onset. Almost two thirds (63%, 131/207) of this group presented within 3.5 h and the majority (71%) by ambulance. Of those with a precise time of onset, presenting within 3.5 h, 45% (59/131) had a normal CT scan (Fig. 1). However, median time to scan from hospital presentation for the non-thrombolysed ischaemic patients was 172 min (IQ 87–875 min). With regard to a 24/7 service, 28.8% of patients were thrombolysed during the weekend as compared with 18.4% in the UK SITS-MOST patients (p < 0.05). Just under a quarter (24%) of the thrombolysed patients presented in out of periods in hours (8 pm–8 am), compared with 78% (503/645) of the non-thrombolysed strokes presented to ED during normal working hours (8 am–8 pm).

Non-thrombolysed ischaemic stroke presentation overview
When compared with the SITS-MOST, the thrombolysed patients in the Irish audit were older, with a median age of 71 (36–93) versus 68 (59–75), and were less independent at baseline, 85 versus 93% (p < 0.01). Although formal NIHSS data on arrival were not available in the Irish audit, estimates of severity were drawn from presenting symptoms and may suggest a trend of lower rates of thrombolysis in milder strokes when compared with the SITS-MOST (Table 5).
These results are also in the context of improved stroke services in key areas for all patients presenting with stroke symptoms, with 99% (862/874) of all patients undergoing neuroimaging compared with 93% (2028/2173) in 2008 and 70% (610/874) of all patients being scanned within 24 h compared with 40% (867/2173) in 2008 (p < 0.001). Similarly, access to specialist care improved with 61% of patients under the care of a stroke specialist during their hospital admission compared to 38% in 2008 (p < 0.001).
Discussion
In a relatively short space of time, Ireland has greatly increased patients’ access to thrombolysis therapy, with a tenfold increase in thrombolysis rate from 1 to 11%. This is comparable to other European health services such as the Netherlands, who observed an increase in thrombolysis rate from 6.4 to 14.6% between 2005 and 2012 [9]. Notwithstanding the low baseline, which service providers were comparing against, the estimated national thrombolysis rate of 11%, which was primarily achieved through the reorganisation of services, is now on a par with most developed stroke services internationally [10]. The outcome for these patients should also be viewed through the evidence that more severe strokes tend to present faster and, as such, have a better chance of being thrombolysed. When viewing specific sites’ thrombolysis rates, it is clear that redirect policies will show improved levels of thrombolysis delivery, given the filtering of appropriate cases to that site. It has also been observed that higher rates are shown in redirection services because of a failure to include all strokes in the denominator including the non-redirected patients [11]. The improved rate in our review was offset nationally by the inclusion of all sites in the national figure.
Adopting a policy of expanding the training and responsibility of thrombolysis delivery to general physicians and emergency specialists was a key in achieving this improvement. It appears that this service is being provided in a safe manner within internationally accepted guidelines. However, there is still more to be achieved, noting the numbers of patients presenting with ischaemic stroke within the time window and not receiving the treatment. This raises the question that potential cases are being missed. This may be reflected in the fact that lesser experienced physicians may be slow to thrombolysed milder strokes, as well as inefficiencies in the chain of care such as delays in neuroimaging. Coupling the lower rates of milder strokes receiving thrombolysis and, albeit in a small sample size, the higher dependency of the Irish group versus the SITS group, the observed lack of effect of thrombolysis on dependency may be reflective of a service in evolution [12].
There are also concerns that thrombolysis services provided by general physicians may thrombolyse higher rates of inappropriate patients, and the data available is unable to quantify this at present in Ireland as it is available in the UK for example. Being cognisant of the low sample size, there is a reassuringly comparable mortality rate for thrombolysed cases, coupled with the observation that general physicians are less likely to deviate from guidelines than their more experienced stroke physician colleagues.
There is also evidence that due to limited capabilities of the stroke units within the service, and perhaps compounded by less experienced doctors overcompensating, a high volume of patients utilise high dependency beds. With the new evidence supporting endovascular intervention, the fact that both treatments are directly linked, the emphasis on providing an efficient thrombolysis service is even more apparent [13]. The potential inequity of access is likely to be more evident for endovascular treatment, given the challenges highlighted with regard to population dispersal in Ireland.
Using the SITS-MOST data, which only included cases treated within 3 h of onset and did not include patients over 75 years of age, the inpatient mortality rate of 11.3% was comparable to the SITS-MOST study 3-month mortality rate of 11.3%. The sample size is clearly small in comparison to both the UK and SITS-MOST data. However, the trend appears reassuring and, for outcome measures such as mortality, the NSA 2015 results are comparable to the national Hospital Inpatient Enquiry (HIPE) register of all stroke admissions. The absence of door-to-needle times; rates of symptomatic intracerebral haemorrhage, which are key measures of quality of care; and inconsistent use of assessment tools, such as the NIHSS and the mRS, restrict the interpretation of results against international evidence. The monitoring of door-to-imaging and door-to-needle times was identified as a minimum requirement by the ESO in managing an acute stroke service [14]. These limitations could be offset by better use of the national stroke register, which has been under resourced to date.
Conclusion
This review further strengthens the benefits of audit of stroke services [15]. A continued review of thrombolytics in a stroke service is essential, and recording of quality of care metrics in order to facilitate comparison with other jurisdictions is vital. Thrombolysis of ischaemic stroke is still evolving and being refined whether through the time limit it can be safely given, the age profile of patients who receive it, or most recently, the dose that may be effective in certain patient groups [3, 16, 17]. This review highlights that an effective national thrombolysis service is possible with limited investment and appropriate reorganisation and may serve as a template to other jurisdictions with similar challenges.
References
Disorders TNIoN, Group Sr-PSS (1995) Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 333(24):1581–1588
Wahlgren N, Ahmed N, Dávalos A, Ford GA, Grond M, Hacke W et al Thrombolysis with alteplase for acute ischaemic stroke in the Safe Implementation of Thrombolysis in Stroke-Monitoring Study (SITS-MOST): an observational study. Lancet 369(9558):275–282
Hacke W, Kaste M, Bluhmki E, Brozman M, Dávalos A, Guidetti D et al (2008) Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med 359(13):1317–1329
Horgan F, Murphy S, Hickey A, McGee H, O'Neill D (2009) Results from the first Irish National Audit of Stroke Care (INASC)—clinical audit. Cerebrovasc Dis 27:228
Health Do. Changing cardiovascular health: National Cardiovascular Health Policy 2010-2019. Government Publications, 2010–05. Report No.: 0-7557-7639-9
Central Statisitcs Office, Ireland, http://www.cso.ie (accessed 10 June 2017)
McElwaine P, McCormack J, Harbison J. National Stroke Audit 2015. Irish Heart Foundation (IHF) & Health Service Executive, 2016-02. Report No.: 978-1-78602-006-2
Lees KR, Ford GA, Muir KW, Ahmed N, Dyker AG, Atula S et al (2008) Thrombolytic therapy for acute stroke in the United Kingdom: experience from the safe implementation of thrombolysis in stroke (SITS) register. QJM 101(11):863–869
Scherf S, Limburg M, Wimmers R, Middelkoop I, Lingsma H (2016) Increase in national intravenous thrombolysis rates for ischaemic stroke between 2005 and 2012: is bigger better? BMC Neurol 16(1):1–6
Hillmann S, Wiedmann S, Fraser A, Baeza J, Rudd A, Norrving B et al (2015) Temporal changes in the quality of acute stroke care in five national audits across Europe. Biomed Res Int 2015:432497
Price CI, Clement F, Gray J, Donaldson C, Ford GA (2009) Systematic review of stroke thrombolysis service configuration. Expert Rev Neurother 9(2):211–233
McMeekin P, Wildman J, Ford GA, Vale L, Price CI (2015) Relative distributions: a novel method for examining trends between stroke onset and thrombolysis time. Stroke 46(5):1381–1383. doi:10.1161/STROKEAHA.115.008724
Wahlgren N, Moreira T, Michel P, Steiner T, Jansen O, Cognard C et al (2016) Mechanical thrombectomy in acute ischemic stroke: consensus statement by ESO-Karolinska Stroke Update 2014/2015, supported by ESO, ESMINT, ESNR and EAN. Int J Stroke 11(1):134–147
Ringelstein EB, Chamorro A, Kaste M, Langhorne P, Leys D, Lyrer P et al (2013) European Stroke Organisation recommendations to establish a stroke unit and stroke center. Stroke 44(3):828–840
Rudd AG, Irwin P, Rutledge Z, Lowe D, Wade D, Morris R et al (1999) The national sentinel audit for stroke: a tool for raising standards of care. J R Coll Physicians Lond 33(5):460–464
The benefits and harms of intravenous thrombolysis with recombinant tissue plasminogen activator within 6 h of acute ischaemic stroke (the third international stroke trial [IST-3]): a randomised controlled trial. Lancet 379(9834):2352–63
Anderson CS, Robinson T, Lindley RI, Arima H, Lavados PM, Lee T-H, et al. Low-dose versus standard-dose intravenous alteplase in acute ischemic stroke. N Engl J Med 0(0):null
Acknowledgements
The validated data collection tools were used with the kind permission of RCPUK and the SSNAP team, in particular Prof A. Rudd.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Electronic supplementary material
ESM 1
(DOCX 153 kb)
Rights and permissions
About this article

Cite this article
McElwaine, P., McCormack, J., Brennan, C. et al. Thrombolysis for stroke in Ireland: increasing access and maintaining safety in a challenging environment. Ir J Med Sci 187, 275–280 (2018). https://doi.org/10.1007/s11845-017-1661-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11845-017-1661-5