
Abstract
Building on the health belief model (HBM), this research tests, over six months, how the exposure to COVID-related information in the media affects fear, which in turn conditions beliefs about the severity of the virus, susceptibility of getting the virus, and benefits of safety measures. These health beliefs ultimately lead to social distancing and panic buying. As a first contribution, we find that fear is not directly triggered by the objective severity of a crisis, but rather formed over time by the way individuals are exposed to media. Second, we show that fear affects behaviors through the components of the HBM which relate to the risks/benefits of a situation. Last, we find that critical thinking about media content amplifies the “adaptive” responses of our model (e.g., health beliefs, social distancing) and reduces its “maladaptive” responses (e.g., panic buying). Interestingly, we note that the beneficial effect of critical thinking about media content disappears as the level of fear increases over time. The implications of these findings for policymakers, media companies, and theory are further discussed.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
As of March 2022, COVID-19 resulted in more than six million deaths worldwide (World Health Organization, 2022). The ripple effect of the pandemic has been colossal. For instance, unemployment rates soared in April 2020 at 14.7%, the highest in the USA since the late 1940s (Bureau of Labor Statistics, 2020). Similarly, unemployment rates in Canada peaked to 13.7% in May 2020 (Statistics Canada, 2021). In addition to these economic outcomes, there were significant unquantifiable human consequences related to this crisis. Even though lockdowns can help curb the spread of the virus, research notes their detrimental effects on individuals’ anxiety and mental health (Pew Research Center, 2020). Although the situation has improved in the last years, people are now learning to live with the omnipresence of COVID. Despite the vaccines, this virus is unlikely to disappear as new variants (e.g., Omicron) keep emerging (CDC, 2022; Das et al., 2021). Living with COVID will likely become the “new normal” with seasonal propagation waves that will require cyclical preventive measures. Given the constant evolution of the virus, the effectiveness of vaccines could greatly vary, and the implementation of physical preventive measures (e.g., social distancing, hand washing, and mask wearing) will remain relevant in years to come.
Policymakers have an important role to play in managing the consequences of the new COVID variants or the next pandemic (Das et al., 2021). We argue that policymakers would be in a better position to manage the next waves if they have a deeper understanding of the processes that lead individuals to adopt adaptive (e.g., social distancing) or maladaptive (e.g., panic buying) behaviors. We focus on the prediction of social distancing and panic buying because of their importance for policymakers at the beginning of a pandemic or a new variant (see Table 1 for the definitions of our core italicized concepts). At its outbreak, social distancing is among the most effective measures to curb a virus’s propagation and to reduce the number of deaths and hospitalizations (e.g., Matrajt & Leung, 2020). Then, for effective management of a pandemic, policymakers need to ensure that people stay calm and do not succumb to any form of panic. In this research, we pay special attention to panic buying given its implications for consumers and retailers (e.g., Islam et al., 2021).
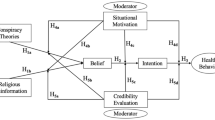
To predict our two core behaviors, we propose a framework (Fig. 1) that combines the health belief model (HBM; Keller & Lehmann, 2008) with elements from marketing-related literatures, such as crisis in marketing (e.g., Khamitov et al., 2020) and health communication (e.g., Austin et al., 2015; Pinkleton et al., 2010; Radanielina Hita et al., 2018). We anchor our framework by starting with the HBM, which has been widely used in prevention and medical contexts (e.g., Chin & Mansori, 2019; Keller & Lehmann, 2008). The HBM predicts that people are more likely to adopt healthy behaviors when they develop appropriate beliefs related to the susceptibility of getting a disease, severity of getting a disease, and benefits of a preventive measure (Table 1). Despite the popularity of the HBM to predict behaviors in a private health context (e.g., cancer prevention), it has rarely been applied to an ongoing public health crisis. In this research, we extend the HBM by adding three crucial components. To the best of our knowledge, these variables have never been combined with the HBM, and these additions are necessary given the particularities of the pandemic.

Conceptual framework
First, the severity of a pandemic keeps changing according to its different propagation waves and their levels (e.g., top, decreasing, bottom). We incorporate this key notion because it affects the measures put in place by policymakers and the attention given by media (Das et al., 2021). Second, people’s responses to a pandemic are largely explained by their exposure to mass media content and their ability to critically assess such content. As a result, we add to the HBM two key variables from the communication literature: media exposure (e.g., de Vreese & Neijens, 2016) and critical thinking about media content (e.g., Austin et al., 2015; Pinkleton et al., 2010; Radanielina Hita et al., 2018). Third, pandemics are characterized by a high level of fear of the virus (Peters et al., 2013); in our model, this emotion activates the HBM, which ultimately leads to our core behaviors. Building on the above, our core contribution is to propose a unique theoretical assemblage that is specifically designed for a global health crisis. Importantly, this framework is tested with six surveys, collected over six months (May to October 2020), with a homogenous population (Quebec, Canada). We explain our framework by dividing it into three distinct parts, which correspond to three specific contributions for theory and policymakers.
As a first contribution, we focus on the role of mass media in transmitting governments’ information about crisis severity and in creating a sense of fear (Campbell et al., 2020; Olagoke et al., 2020). Although governments have accurate information about the severity and propagation of a pandemic, such an information is not necessarily the direct cause leading to fear. We rather argue that people’s fear is mainly conditioned by their exposure to media (traditional and online) and the COVID-related information obtained through this exposure. Here, we posit that media exposure mediates over time the effect of crisis severity on fear of COVID; this sequence corresponds to the longitudinal process “crisis severity/propagation wave → media exposure → fear.” Since the HBM has rarely been applied to a global health crisis, this sequence adds two key components (i.e., crisis severity and media exposure) that have been under-researched in the HBM literature.
As a second contribution, we explain the fear-based processes that lead to our two behaviors. We argue that fear of COVID is the emotional drive that conditions both adaptive and maladaptive behaviors through its specific effects on health beliefs (Earl & Albarracín, 2007; Meadows, 2020); this logic is reflected in the longitudinal processes “fear→ components of the HBM → social distancing, panic buying.” Although fear is an important consideration to account for in a pandemic, there is surprisingly little HBM research on the matter. For instance, the meta-analyses and reviews on the HBM do not consider fear as a potential driver (e.g., Jones et al., 2014; Sulat et al., 2018). We address this gap by proposing two different processes depending on the behaviors. For social distancing, all three beliefs—reflecting both the threat of the virus (i.e., severity and susceptibility) and the benefits of the measure—should play a mediating role. For panic buying, only the beliefs associated with the threat of COVID should play a mediating role in the sequence of interest.
After integrating media exposure and fear into the HBM, our third contribution refers to the evaluation of media content. It is not sufficient to account for mere “media exposure” to add a strong “media and communication” component to the HBM; we also need to account for people’s ability to critically assess media content (Austin et al., 2006, 2015; Pinkleton et al., 2010). Different media have different views on the pandemic, and individuals need to distinguish between false and truthful information. Accordingly, we examine the beneficial effects that critical thinking about media content may have on our model. In terms of main effects, we argue that critical thinking should amplify adaptive responses (e.g., social distancing), and mitigate maladaptive ones (i.e., panic buying). Importantly, we argue that critical thinking moderates the paths involving the notion of fear (i.e., “media exposure → fear” and “fear → HBM components”). The amplifying effect of critical thinking is expected to decrease as the levels of media exposure or fear increase. Understanding the beneficial effect of critical thinking is important for policymakers and media companies because this skill can be taught and learned.
Research background
Two behaviors of interest for policymakers
In this section, we justify the selection of our two behaviors and present the HBM. When a pandemic erupts, policymakers are primarily concerned about 1) slowing down the virus and 2) ensuring that individuals do not get overwhelmed by panic. Accordingly, we focus on predicting two key outcomes: social distancing and panic behavior.
When no vaccine is available, social distancing is the most effective measure to slow down the propagation of the virus; it is the most adapted initial response for societies and individuals (Das et al., 2021; Greer, 2013). The concept of social distancing comprises a set of simple precautionary measures that share the common goal of limiting community transmission of a virus (World Health Organization, 2021). At a societal level, policymakers can implement measures such as quarantines, travel limitations, and workplace closures. In this research, our focus is on the individual level, which includes measures such as physical distancing with any unrelated individual as well as avoiding public places (Greer, 2013). Other forms of physical measures include hand washing and mask wearing, and all these measures aim to create a distance or barriers between people and the virus (World Health Organization, 2021).
It should be noted that vaccination is often viewed as the preventive measure of choice to counter a pandemic (World Health Organization, 2021). Unfortunately, the development of vaccines can take months before being available, and their effectiveness may decrease over time, as new variants emerge (Centers for Disease Control and Prevention, 2022). Accordingly, some form of social distancing and other physical preventive measures keep their relevance over time, and they almost always accompany vaccination efforts.
Along with social distancing, policymakers are also concerned that people do not succumb to panic. Here, panic buying is one of the most observable movements of collective fear, and this behavior reflects well a population’s state of mind (Ahmadi et al., 2021; Omar et al., 2021). Policymakers hope that people will not fall into such a trap, and that they will keep trusting governments. Consistent with recent marketing research, panic buying is described as a specific form of stockpiling of food and non-food items, which is driven by impulsiveness and insecurity about the future (Ahmadi et al., 2021; Herjanto et al., 2021; Omar et al., 2021). In line with this literature, we define panic buying as an impulsive buying behavior that leads consumers to stockpile food and non-food items in times of uncertainty to face a potential threat. Because panic buying threatened retailers’ operations in times of crisis, it is viewed as a maladaptive response (Ahmadi et al., 2021).
The health belief model
The HBM is the cornerstone of our research, and we posit that its core components can predict our two behaviors of interest. Substantial empirical evidence has supported the predictive ability of the HBM for a variety of preventive and medical behaviors, such as cancer screening or the adoption of a medical treatment (see Chin & Mansori, 2019; Jones et al., 2014; Sulat et al., 2018 for reviews). Although the HBM is typically used to predict health interventions for specific targets in a private context (e.g., the elderly, youth), we argue that it can also be employed in the context of a public and ongoing global pandemic.
Three beliefs of the HBM are relevant for the prediction of our two behaviors (Birmingham et al., 2015; Fall et al., 2018). Specifically, (1) susceptibility of getting COVID represents an individual belief about the likelihood of getting infected by the virus; (2) severity of getting COVID is defined as a belief about the medical and social seriousness of contracting the virus for oneself and others; and (3) benefits of social distancing reflect an individual belief about the advantages of engaging in social distancing to reduce the threat of the virus for oneself and others. The combination of susceptibility and severity forms the “costs” that people try to minimize by accounting for the “benefits” of a measure (Glanz et al., 2008). At its core, the HBM includes divergent considerations (i.e., threats/costs vs. opportunities/benefits) that individuals try to weigh when making health decisions.
Our research is not simply a replication of the HBM with new behaviors, in a new context. We add to the HBM new conceptual elements to capture the particularities of the current pandemic (Fig. 1), which is characterized by high levels of severity, media influence, and fear. This research proposes a new theoretical assemblage that captures the fear-based process leading to social distancing and panic buying in the context of a heavily mediatized pandemic. Thus, we incorporate into the HBM new conceptual aspects that relate to the severity of a crisis (e.g., Khamitov et al., 2020), media involvement (e.g., Austin et al., 2015; Radanielina Hita et al., 2018), and the role of fear (e.g., Meadows, 2020). The linkage between these variables and the HBM are explained in detail when we formulate our hypotheses in the next section.
Our framework is developed in a longitudinal manner (Bauer et al., 2006; Singer & Willett, 2003) by using a mix of repeated variables (level 1) and trait variables measured at baseline (level 2; see Table 1). Our multi-level framework has implication for theory development. Indeed, our initial hypotheses propose longitudinal, within-individual processes (in contrast with cross-sectional, between-individuals processes) through which predictors, mediators, and outcomes travel together over time, as we see next. Such a longitudinal approach is recommended to better understand individual responses to crises (Khamitov et al., 2020), and to establish causal inferences in the HBM literature (Sulat et al., 2018).
Development of hypotheses
The process “crisis severity/propagation wave → media exposure → fear of COVID”
Crisis severity
Consistent with recent research on crises and pandemics (Campbell et al., 2020; Islam et al., 2021), the variable “severity” is our logical starting point. The severity of a pandemic is the triggering variable that conditions “macro” considerations (e.g., economic contraction, uncertainty, scarcity), which then influence marketers’ and policymakers’ decisions (Das et al., 2021). For instance, governments were much more active in managing COVID compared to SARS-1 (2002–2003), which was less costly and deadly. Being one of the most studied variables in the crisis literature (Khamitov et al., 2020), severity is one of the first factors considered by all actors (policymakers, marketers, consumers) before taking actions.
We define the severity of the COVID crisis as the loss in terms of human lives and the efforts required by the population to face the crisis (Khamitov et al., 2020; Laufer et al., 2005). Here, the severity of the COVID crisis is estimated by referring to four indicators, or proxies. The number of deaths captures the “loss” dimension of severity (Das et al., 2021; Islam et al., 2021). The “effort” dimension is assessed by three other proxies: the number of hospitalizations, confinement orders, and deconfinement orders. The hospitalizations capture the pressure of a pandemic on the healthcare system. In turn, the order of confinement (vs. deconfinement) represents temporary policies requesting people to decrease (vs. allowing people to increase) their contacts with others. Such orders include the closure of schools, retailers, and workplaces.
By referring to these proxies, we determine the level of severity for each month of interest. To capture the longitudinal aspect of crisis severity, we refer to the notion of propagation wave, defined as the oscillating pattern (top, decreasing, bottom, increasing, and so forth) showing the spread and severity of a virus over time. Pandemics are characterized by a series of waves, and this notion is widely used to qualify the severity of a pandemic (World Health Organization, 2021). People are particularly restricted at the top of a wave and much less constrained at the bottom of it (see Table 2 for our assessment per month).
The role of media exposure
Governments possess accurate information about the severity of a pandemic. However, they are not well equipped to quickly bring this information to the population; mass media typically plays this crucial role. In marketing, crises typically affect only specific customers that a firm can contact by using personal information. Because of the localized nature of most crises in marketing, prior research did not see the necessity of integrating the role of mass media (Cleeren et al., 2017; Khamitov et al., 2020). This situation is different for a global pandemic in which policymakers rely on mass media to alert and update the population. We address this issue by examining the effects of crisis severity on media exposure.
We define media exposure as the extent to which viewers have encountered and engaged with messages about COVID in all types of media (de Vreese & Neijens, 2016; Slater, 2004). There are different ways to measure media exposure by using aggregated archival data or individual perceptions. Given the purpose of our research, we rely on self-reported measures in which consumers assess the extent to which they watched, read, and shared COVID-related information (de Vreese & Neijens, 2016; Slater, 2004); using perceptual, panel data is a common way to test longitudinal processes (Bauer et al., 2006). Although such perceptions have limitations,Footnote 1 they are regularly used in communication; about 94% of communication research used self-reported measures of media exposure (de Vreese & Neijens, 2016). Given the centrality of media exposure in our model, we elaborate on three of its core attributes.
First, we use a generic measure of media exposure that includes exposure to all types of media: traditional, online, or social. Given the convergence of media on different platforms (traditional or online), consumers now use a blend of media to get information. In this context, it can be challenging to dissociate the influence of different media source when measuring exposure (Ohme et al., 2016). Second, we directly ask the participants to remember and report their active exposure to different media (de Vreese & Neijens, 2016). Accordingly, the current research does not account for involuntary exposure to information and unconscious processes. We rather measure consumers’ perception of their willful exposure to COVID-related information and their level of engagement with this information (i.e., sharing it). Third, our measure of media exposure does not reflect the evaluation that consumers make about media content. This evaluative part is discussed later when we introduce critical thinking (H4-H6).
H1 Governments critically need the support of mass media to make their populations aware of and careful about the pandemic. The current research pays special attention to the notion of fear, which has been prevalent in the current pandemic. Here, fear of COVID refers to an intense and unpleasant emotion that is triggered by the anticipation of getting infected by the virus (Ruiter et al., 2014; Tannenbaum et al., 2015). In H1, the level of propagation wave affects over time the extent to which consumers expose themselves to media feeds about COVID, which in turn generates fear. H1 argues that fear is not directly created by the characteristics of a crisis (e.g., severity, level of wave) as described by governments. It is rather created over time by the way that individuals expose themselves to media and the content they have collected through this exposure. Because of the deadly nature of the disease, COVID-related information should create some fear (Olagoke et al., 2020). For instance, Sacerdote et al. (2020) reported that major media were overwhelmingly negative when reporting on COVID even when the cases were declining. This situation made the population fearful even if the initial wave was decreasing.
H1
The effect of propagation wave (i.e., crisis severity) on fear of COVID is mediated over time by media exposure. Specifically, H1 involves the longitudinal indirect effect: level of propagation wave → media exposure → fear.
The process “fear of covid → HBM components → behaviors”
Understanding the longitudinal effects of fear of COVID is important for policymakers. Fear creates an urge to reduce the threat at the origin of the emotion (Campbell et al., 2020). This urge, in turn, motivates the target audience to revise their beliefs and behaviors to protect themselves from the threat (Meadows, 2020; Tannenbaum et al., 2015). On the one hand, this intense emotion can be functional in the context of a pandemic when it leads to appropriate actions (e.g., social distancing). On the other hand, it can also produce maladaptive responses (e.g., panic buying) if individuals do not have the resources to correctly assess the threat. Although prior research has highlighted the action-oriented nature of fear (Campbell et al., 2020; Meadows, 2020), its longitudinal mechanisms leading to behavioral responses, in the context of a pandemic, still need to be documented.
The link between fear and health beliefs is surprisingly under-researched (Ort & Fahr, 2018). Indeed, fear is absent from meta-analyses and systematic reviews about the HBM (Carpenter, 2010; Jones et al., 2014; Sulat et al., 2018). To fill this gap, fear is viewed as the emotional drive that leads to the formation of health beliefs, which in turns leads to our two behaviors. As their level of fear increases, individuals become highly motivated to appraise the pandemic, and to develop appropriate health beliefs that correspond to their assessment (Meadows, 2020; Tannenbaum et al., 2015). Based on these explanations, we can reasonably expect that fear of COVID will lead to the formation of the three health beliefs of interest. Depending on the beliefs that are activated, individuals then develop a propensity to engage in social distancing and/or panic buying. We suggest two slightly different processes depending on the behavior.
First, we argue for the longitudinal sequence: fear → severity, susceptibility, and benefits → social distancing. This sequence highlights the role of all three HBM components in predicting social distancing (Chin & Mansori, 2019; Sulat et al., 2018; Tannenbaum et al., 2015). Fear on its own is not sufficient to predict this prevention measure, and it needs to go through all the beliefs related to its costs (i.e., severity and susceptibility) and benefits. As long as consumers perceive that COVID could have severe consequences for them, that they are susceptible to getting the virus, and that the benefits of social distancing are important, they should engage in social distancing. Accordingly, the effect of fear on social distancing should be mediated in parallel by all three HBM components. Formally:
H2
The effect of fear of COVID on social distancing is mediated over time by the three components of the HBM. Specifically, H2 involves three parallel longitudinal indirect effects:
-
Fear of COVID → severity of getting COVID → social distancing;
-
Fear of COVID → susceptibility of getting COVID → social distancing;
-
Fear of COVID → benefits of social distancing → social distancing.
Our other mediation effect links, in a longitudinal manner, the variables: fear → severity, susceptibility → panic buying. We argue that only two of the HBM components—those related to the costs of COVID—are relevant in explaining the effect of fear on panic buying. If consumers perceive the virus as causing severe consequences and if they feel susceptible to getting it, they should engage in panic buying. Here, recent research explains that panic buying is driven by negative motivations, such as urgency or insecurity about the future (Ahmadi et al., 2021; Omar et al., 2021)—which seem related to the beliefs about severity and susceptibility. For these reasons, we expect that severity and susceptibility are relevant, parallel mediators in explaining the sequence between fear and panic buying. The belief about the benefits of social distancing refer to a different behavior; as a result, it does not play a role in H3.Footnote 2
H3
The effect of fear of COVID on panic buying is mediated over time by the two components of the HBM. Specifically, H3 involves two parallel longitudinal indirect effects:
-
Fear → severity of getting COVID → panic buying;
-
Fear → susceptibility of getting COVID → panic buying.
The beneficial effects of critical thinking about media content
So far, we account for the effect of media exposure and fear without considering viewers’ ability at evaluating media content. Given that different media have different views on the pandemic, our model also integrates individuals’ ability to critically think about media content (Austin et al., 2006, 2015; Pinkleton et al., 2010; Radanielina Hita et al., 2018). Policymakers are concerned about this issue; the effectiveness of their policies relies on people’s ability to distinguish truthful from false information.
Critical thinking about media content is an individual, inquiry-based competence that captures viewers’ ability to analytically assess the information heard in the media before accepting it as believable (e.g.: Pinkleton et al., 2010; Radanielina Hita et al., 2018). It is viewed as a core component of the broader concept of media literacy (National Association for Media Literacy Education (NAMLE), 2020).Footnote 3 Critical viewers actively reflect on media content and seek more information before developing their own opinion. After being exposed to content of all types (traditional or online), they think twice about the intent of the media and its credibility. Critical thinking is viewed as an individual trait (e.g.: Radanielina Hita et al., 2018), and it constitutes a level 2 variable in our model (see Table 1). This competence was originally intended to increase youth’s understanding of persuasive commercials and to prevent risky behaviors on their part. We are not aware of any research examining, in a longitudinal manner, the effects of critical thinking to promote health behaviors during an ongoing global pandemic.
A critical orientation operates by activating viewers’ logic-based processing to help them resist persuasive appeals, which could take advantage of people’s lack of understanding (e.g.,Austin et al., 2006 ; Pinkleton et al., 2010 ; Radanielina Hita et al., 2018). Extending this logic to our context, we argue that critical thinking has different effects on the components of our models depending on their nature as adaptive or maladaptive. On the one hand, we predict that critical thinking amplifies all the adaptive responses of our models—such as fear, the HBM components, and social distancing. Critical thinkers can recognize the extreme danger associated with COVID. As a result, they become fearful, develop appropriate health beliefs, and engage more intensively in social distancing. On the other hand, critical thinking should decrease panic buying because of its maladaptive nature. Individuals with a strong critical orientation should recognize that this behavior is somewhat unreasonable and unproductive (Ahmadi et al., 2021; Herjanto et al., 2021).
H4
Critical thinking about media content (level 2 variable) has positive effects over time on (a) fear of COVID, the three HBM components, and on social distancing. In turn, (b) critical thinking has a negative effect on panic buying over time.
We also expect critical thinking to moderate the paths involving fear. We focus on these paths because prior research suggests that critical thinking could mitigate the emotional route of the persuasion process (Austin et al., 2006; Pinkleton et al., 2010; Radanielina Hita et al., 2018). For the path “media exposure → fear,” we expect that the amplifying effect of critical thinking (H4) will decrease as the level of media exposure increases. On the one hand, we should find the amplification effect of critical thinking for individuals who were less exposed to media and less informed about the crisis. In the context of low media exposure, individuals who possess lower critical thinking could dismiss the danger of the crisis and feel little fear. On the other hand, heavy users of media should experience a higher level of fear regardless of their level of critical thinking. The pandemic has been described as dangerous in most media; well-informed consumers should feel afraid irrespective of their critical thinking.
H5
Critical thinking about media content (level 2 variable) interacts with media exposure to predict fear of COVID over time. As the level of media exposure increases, the amplifying effect of critical thinking is reduced.
We expect the same pattern of interaction for the three paths “fear → three HBM components.” Again, we expect that the amplifying effect of critical thinking mainly holds at low levels of fear. In a situation of low fear, consumers with low critical thinking may not understand the importance of developing appropriate health beliefs about the pandemic (Austin et al., 2006; Pinkleton et al., 2010; Radanielina Hita et al., 2018). However, as the fear increases, all consumers develop appropriate health beliefs, regardless of their level of critical thinking. Their high level of fear becomes the main driver conditioning their beliefs; critical thinking has little effect when consumers feel vivid fear.
H6
Critical thinking about media content (level 2 variable) interacts with fear of COVID to predict over time a) severity of getting COVID, b) benefits of social distancing, and c) susceptibility of getting COVID. As the level of fear increases, the amplifying effect of critical thinking on these health beliefs is reduced.
Method
Sample and study design
We conducted a longitudinal study over a six-month period in Quebec, Canada. We collaborated with the firm Delvinia, which operates an online panel called “Asking Canadians.” The panel consists of about one million Canadians, with 22% Quebecois. This panel matches the characteristics of the population on a set of relevant variables such as age, sex, language, income, education, and regions (Statistics Canada, 2021). The data collection comprised six measurement periods. At the beginning of each month, from May to October 2020, participants were asked to think about the last month and answer questions related to our variables.
For the first measurement period, Delvinia sent the link to 14,702 panelists, from whom the firm obtained 2333 first clicks, for an initial response rate of 15.87%. We excluded incomplete questionnaires and participants who missed the attention checks. In addition, Delvinia used an in-house procedure to eliminate “straightliners” and “racers” (about 5%). After eliminating these participants, the baseline data included 881 complete questionnaires, for a final response rate of 5.99%. Although lower, this level of responseFootnote 4 appears reasonable compared to recent response rates (10%–15%) (Chen, 2021; Wielgos et al., 2021).
After time 1, we obtained the following numbers of participants (and response rates): 631 (71.6%), 378 (59.9%), 190 (50.3%), 123 (64.7%), and 84 (68.3%) for times 2–6, respectively. In prior work using repeated surveys (e.g., Bolander et al., 2017; Palmatier et al., 2007), the response and attrition rates varied greatly according to different factors, such as the type of participants (consumers vs. employees), the intervals between surveys (ranging from two weeks to a year), and the number of measurement periods (ranging from three to 24). Among the reviewed articles, the response rate across periods tended to vary between 55% (Palmatier et al., 2007) and 80% (Grégoire et al., 2018). After balancing these considerations and the costs of collecting data, we consider that our response rates across periods are generally satisfactory. Research firms, such as Delvinia, typically aim for an average response rate of 60% (50% being the lowest acceptable threshold). Accordingly, the response rates appear high for times 2 and 6 (71.6% and 68.3%), satisfactory for times 3 and 5 (59.9% and 64.7%) and acceptable for time 4 (50.3%).
In our sample, 49.5% were female; the mean age was 48 years (SD = 11.23); and 76.7% were francophone. In terms of locations, 52.2% came from Montreal, 19.1% from Quebec City, and 28.7% from other areas. To assess the possibility of non-response bias (Hulland et al., 2018), we compared the socio-demographics (i.e., gender, region, and language) and the scores of our key variables between a random sample of early and late participants (for time 1). We did not find any significant differences on any of these variables (p’s > .09 and χ2 > .05).
Longitudinal designs in marketing
Longitudinal surveys are rare in marketing; Hulland et al. (2018) report that only 7.9% of the surveys published in JAMS, between 2006 and 2015, use longitudinal designs. Similarly, Khamitov et al. (2020) find that only 3.8% of the methods are longitudinal surveys in the service failure literature. A longitudinal design fits our research well since we are interested in testing longitudinal, within-individual processes (Bolander et al., 2017; Rindfleisch et al., 2008). Longitudinal designs are appropriate to capture the evolution of self-reported and internally oriented variables, which are consistently measured over time. This method is also adapted to capture the particularities of a phenomenon that evolves over time, such as a pandemic. As documented in Table 2, our research covers most of the first propagation wave (April to July 2020) and the beginning of the second wave in Quebec (August and September 2020).
For longitudinal designs, a major threat for internal validity is the presence of intervening events (Bolander et al., 2017; Rindfleisch et al., 2008). Such a threat is important in the current COVID context, as the situation was changing almost daily. To account for this threat, our analyses integrate the level of propagation wave associated with each period. In addition, the endogeneity related to the COVID situation is somewhat reduced by the fact that we study a specific population with localized media habits (Quebec).
Common method bias (CMB)
We used three sets of remedies to account for CMB. First, we implemented two procedural remedies. As a first remedy of this sort, our model contains three types of variables that are measured in different manners (Fig. 1 and Table 1), including one objective variable of level 1 (i.e., propagation wave), eight perceptual variables of level 1 (our seven core variables and job insecurity), and three variables of level 2 (critical thinking, age, and gender). These three types of variables involve different sources of variance. As a second procedural remedy, the merits of longitudinal data in minimizing CMB has regularly been noted by survey researchers (e.g., MacKenzie & Podsakoff, 2012; Rindfleisch et al., 2008). Most of these researchers argue that panel data is an effective strategy to reduce CMB, which tends to be stable across time (Jakobsen & Jensen, 2015).
Second, in terms of statistical remedy, we conducted a series of post hoc analyses with a marker variable (MacKenzie & Podsakoff, 2012). See our Post Hoc Analyses and Web Appendix F that show that the presence of a marker (i.e., neo-racism) does not affect our results.
Third, this research relies on linear mixed modeling (LMM), which enables the estimation of both fixed and random effects. To account for the violation of the assumption of independence in longitudinal designs, we specify random effects for the residuals of the repeated dependent variables (West et al., 2007). We use a special application of LMM for repeated measure in SPSS 23.0 that models “repeated covariance type” specifying “the covariance structure for the residuals” (IBM SPSS Statistics, 2021). In sum, the estimation of this covariance structure represents a remedy that accounts for the correlated nature of our repeated variables.
Measurements and scales
Crisis severity and propagation wave (level 1)
To assess crisis severity and propagation wave per period, we collected four proxies from the Institut National de Santé Publique du Québec (2021). According to our definition, we use the number of deaths to capture the “loss” dimension and the number of hospitalizations, confinement orders, and deconfinement orders to capture our population’s “efforts” (Table 2). By referring to these four proxies, we associate each period with a level of crisis severity and propagation wave. We use three levels for crisis severity per period (high, moderate, and weak), which correspond to four levels of propagation wave (i.e., top, decreasing, bottom, growth). Both April and May were on top of wave 1, June was the decreasing period of wave 1, July and August were the bottom of waves 1 and 2, and September was the beginning of the growth of wave 2. In our analyses, we use two operationalizations for propagation wave. First, we account for the individual effects of each period; we use August as the reference category because it corresponds to a time of relative normality with a low level of severity. Second, we transform “propagation wave” into an ordinal and continuous variable by associating the value “3” with the top of a wave, “2” with the middle of the wave (i.e., decreasing or growth), and “1” with the bottom of the wave.
Repeated variables (level 1)
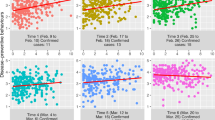
Most of our repeated constructs (level 1) rely on a seven-point Likert scale (1 = strongly disagree and 7 = strongly agree), unless otherwise indicated. Most of our measures are established by and adapted to a COVID context. The scales and their psychometric properties are presented in Web Appendix A. The means per period for our seven core repeated variables are presented in Fig. 2. Overall, we measure six times these seven variables for a total of 42 variables, to which we add six measures for job insecurity (a control variable). Web Appendix B shows the correlation matrix including these 48 variables and critical thinking about media content (a total of 49 variables).

Evolution of our repeated variables according to the periods (observed means)
To measure media exposure, we used a three-item scale adapted from the original work of de Vreese and Neijens (2016). The items were measured on a seven-point scale, with 1 = never and 7 = all the time. This scale includes items such as “I watch television programs/shows about COVID-19.” The index was reliable for the six periods with alphas from .73 to .86.
Fear of COVID was measured using a three-item scale adapted from Birmingham et al. (2015). The scale includes items such as “Thinking about getting COVID-19 makes me afraid.” This index was reliable over time with alphas ranging from .93 to .97.
The three components of the HBM were all measured with established scales adapted from prior work (Fall et al., 2018). Susceptibility of getting COVID was measured using a three-item scale including “I am at risk for COVID-19” (alphas ranging from .76 to .85). In turn, severity of getting COVID was measured using a three-item scale including “Getting COVID-19 would make my daily activities more difficult” (alphas ranging from .85 to .93). Finally, benefits of social distancing were measured using a four-item scale including “Practicing social distancing will prevent me from getting COVID-19” (alphas ranging from .88 to .95).
For social distancing, we used a three-item scale developed by Greer (2013). This scale includes items such as “I avoid public places” (alphas ranging from .64 to .75). To capture panic buying, we developed a five-item scale that combined the items of two scales capturing the notions of food hoarding (Janssens et al., 2019) and urgency buying (Beatty & Ferrell, 1998). This newly developed scale comprises items such as “I buy food items that I did not plan to buy” and “I buy too many products (other than food) more than I need when I go shopping.” The index is reliable with alphas ranging from .83 to .89.
We controlled for job insecurity, which was repeatedly measured over time. Given that economic hardships may exacerbate fear during a major crisis, it seemed important to control for variables that reflect participants’ economic stress as the economic downturns deepens or lengthens. This four-item scale adapted from past research (Vander Elst et al., 2014) includes items such as “Because of the coronavirus pandemic, I now feel insecure about the future of my job” (alphas ranging from .90 to .92).
Critical thinking about media content (level 2)
Critical thinking about media content is an individual difference (level 2) that was measured only at baseline.Footnote 5 This variable was measured with a four-item scale adapted from prior research (e.g., Austin et al., 2013; Radanielina Hita et al., 2018), including items such as “It is important to think twice about what you hear in the media.” This construct is reliable, and its descriptive statistics are within typical ranges (alpha = .78; M = 5.67; SD = 1.09). Finally, in terms of other individual differences measured at time 1 (level 2), we also controlled for age (measured in years) and gender.
Measurement validation
We took a series of measures to validate our scales. First, we performed six cross-sectional CFAs, one for each period. Second, we conducted four longitudinal CFAs to establish the equivalence of our repeated constructs across periods. Third, we conducted additional tests for panic buying because of the novelty of this scale. Given space constraints, we only summarize our results here. Please see Web Appendices A and C for details.
All our six cross-sectional CFA models, one for each period, provide acceptable fit indices (see Web Appendix A). The average variance extracted (AVE) was close to or greater than .5 for all constructs for each period. All alphas and composite reliabilities were close to or above .7 for all constructs for all periods. All the loadings were significant and substantial.
We conducted four longitudinal CFAs (see Web Appendix C) to establish the equivalence of our repeated constructs across periods 1–4 (e.g., Steenkamp & Maydeu-Olivares, 2021). We used only the first four waves for these analyses because the periods 5 and 6 have a limited number of participants (respectively, 123 and 84). As presented in Web Appendix C, all four unconstrained models represent a good fit with the data. Then, we constrained to equality the loadings of a given item in all four structures/periods and conducted a chi-square difference test between both models (constrained vs. unconstrained). None of the differences was significant for any of the models. Overall, these results indicate that our repeated constructs achieve configural and metric invariances across periods.
Given the novelty of the topic, we conducted additional tests for panic buying (see Web Appendix C). First, in terms of face validity, we note that our items are highly consistent with items used in recently developed scales (see Table C2). We also conducted a CFA with panic buying and a scale measuring social anxiety. Overall, this model fits the data well. Consistent with theory, both constructs are significantly correlated, which provides evidence of convergent validity. However, they are also distinct; when we constrain their correlation to equality, we note a significant increase in chi-square, which provides evidence of discriminant validity.
Results
Linear mixed modeling (LMM)
Our analyses are conducted with a multi-level framework by using LMM for three key reasons (Diggle et al., 2002). First, LMM allows combining the fixed effects of variables that are measured at different levels (level 1 or 2). This analysis allows the incorporation of individual differences that are measured at baseline (level 2) and repeated responses that are nested within individuals (level 1). Second, as previously noted, LMM accounts for the correlated and dependent nature of our longitudinal data by specifying random effects for the residuals (West et al., 2007). Third, LMM accounts for missing responses at each period, and it relies on all the observations collected over time (i.e., 2269 observations through six measurement periods). In our LMM analyses, we control for job insecurity (level 1) and the three trait variables (level 2): gender, age, and critical thinking. All variables are standardized. We also control for propagation wave by using one of our two operationalizations. Finally, we specify a random intercept for all the analyses using LMM.
Overview of our results
We conducted a first series of models (see Web Appendix D) to test the effects of the six periods—characterized by different levels of propagation wave—on the evolution of our seven core repeated variables (Fig. 2). When operationalized as a nominal variable, the five different periods are associated with different levels of media exposure, which differ from the reference category (August). As shown in Fig. 2, Panel A, the level of media exposure followed the level of a propagation wave; high media exposure at the top of wave 1 (April and May), moderate exposure in the middle of waves 1 (June) and 2 (September), and low exposure in the bottom of waves 1 and 2 (July and August). Interestingly, the periods have limited effect on the six other repeated variables.Footnote 6 As shown in Fig. 2, Panels A and B, the patterns for the other variables tend to be relatively flat. Consistent with these findings, when propagation wave is a continuous variable, we find a strong significant effect of this variable on media exposure but little or nonsignificant effects on the other variables (see Web Appendix D).
Figure 3 provides an overview of the main effects of our framework.Footnote 7 Most main effects are significant and in the expected direction. As previously noted, the main effect of propagation wave/period on media exposure is significant (F = 126.66, p < .001); all the different periods differ from the reference category (Fig. 3). In turn, the continuous version of propagation wave also has a positive effect over time on media exposure (β = .26, p < .001), which in turn enhances fear of COVID over time (β = .25, p < .001). Next, this fear positively affects the three components of HBM over time (all p’s < .001). Then, the three health beliefs positively influence the practice of social distancing over time (all p’s < .001), whereas only “susceptibility of getting COVID” has an impact on panic buying over time (β = .20, p < .001). Finally, critical thinking about media content has a positive effect on most responses (p’s < .001) and a negative effect only on panic buying (β = −.10, p < .001). We formally test our hypotheses next.

Presentation of the main effects
Tests of hypotheses
Mediation analyses (H1-H3)
Our mediation analyses were conducted by using the MLmed macro—i.e., Multi-Level Mediation—which relies on LMM (Rockwood, 2019; Rockwood & Hayes, in press). This macro can handle different types of multilevel mediation analyses, including longitudinal and within-individual mediations. In our research, H1-H3 take this form of mediation—that is, a sequence of three variables of level 1 (Rockwood, 2019). This macro automatically conducts the different linear mixed models necessary to test the longitudinal mediation effects, and it calculates the indirect effects by following the procedures of Bauer et al. (2006). The significance of the indirect effects is determined by using Monte-Carlo simulations (i.e., 10,000 resamples) that produce 95% confidence intervals (CI). MLmed is one of the rare available options to test the significance of longitudinal indirect effects with LMM.
MLmed automatically decomposes indirect effects into the within-individual and between-individuals indirect effects (Bauer et al., 2006). The within indirect effects are the focus of our research.Footnote 8 It should be noted that the within indirect effects reported in Table 3 are systematically lower than the total indirect effects—which contain both the within- and between-individuals indirect effects. We standardized all variables before entering them in MLmed. We also controlled for job insecurity (level 1), propagation wave (level 1), critical thinking (level 2), age (level 2), and gender (level 2) in all our models. In sum (see Table 3), MLmed supports most of our hypothesized mediations (H1-H3); H3a is the only exception.
For H1, the indirect effect “level of propagation wave → media exposure → fear” is significant as the confidence intervals do not contain zero (H1: ind. Effect = .05; CI: .03, .06). In turn, H2 is tested with a single MLmed model that simultaneously incorporates three parallel mediators. Here, the three sequences of interest—i.e., “fear → severity → social distancing” (H2a: ind. Effect = .05; CI: .02, .07), “fear → susceptibility → social distancing” (H2b: ind. Effect = .05; CI: .02, .08), and “fear → benefits → social distancing” (H2c: ind. Effect = .05; CI: .03, .07)—are all significant because the confidence intervals do not contain zero. Finally, H3 is tested with a single MLmed model that simultaneously incorporates two parallel mediators. Only the sequence “fear → susceptibility → panic buying” (H3b: ind. Effect = .05; CI: .02, .08) is significant. The sequence “fear → severity → panic buying” (H3a: ind. Effect = −01.; CI: −.03, .02) does not achieve significance because the confidence intervals contain zero.
We conducted three additional MLmed models to calculate the three indirect paths “media exposure → fear → three HBM components.” Although we do not have hypotheses for these paths, we tested them because they are part of our model. All the three longitudinal sequences—that is, “media exposure → fear → severity” (ind. Effect = .06; CI: .04, .08), “media exposure → fear → susceptibility” (ind. Effect = .07; CI: .05, .09), and “media exposure → fear → benefits” (ind. Effect = .04; CI: .03, .06)—are significant.
H4-H6
We conducted additional LMM models to test H4. As shown in Fig. 3 and Table 4, the direct effects of critical thinking about media content on fear (β = .06, p < .05; model 1), severity (β = .14, p < .001; model 3), susceptibility (β = .05, p < .05; model 5), benefits (β = .17, p < .001; model 7), and social distancing (β = .09, p < .001; model 9) are all positive and significant. H4a is supported. In turn, critical thinking has a significant, negative effect on panic buying (β = −.10, p < .001; model 10), which is consistent with H4b. Overall, these results support H4.
For H5, we examine the interaction “media exposure X critical thinking” in the model predicting fear of COVID (model 2, Table 4). Both media exposure (β = .25, p < .001) and critical thinking (β = .06 p < .05) positively influence fear of COVID. Although the interaction appears in the right direction (β = −.03, p = .13), it does not achieve significance; H5 is not supported.
For H6, we test the interaction “fear X critical thinking” in three different models predicting the three HBM components. Since these three tests follow the same procedure, they are presented together. Please see models 4, 6, and 8 (Table 4) for the results of severity, susceptibility, and benefits, respectively. First, we note main positive effects of fear on the three HBM components (severity: β = .42, p < .001; susceptibility: β = .63, p < .001; benefits: β = .29, p < .001) and main positive effects of critical thinking on the same variables (severity: β = .14, p < .001; susceptibility: β = .05, p < .05; benefits: β = .16, p < .001). Second, the interaction “fear X critical thinking” was significant for severity (β = −.04, p < .05) and benefits (β = −.05, p < .01) but not significant for susceptibility (β = −.01, p > .6). H6ac are supported but not H6b.
We plotted the significant interactions by showing the predicted means of the dependent variables for different values (−1 and + 1 standard deviation) of fear and critical thinking. The patterns of interaction for H6a,c are consistent with our predictions (Fig. 4). In the context of low fear, we note a substantial difference across critical thinking conditions: individuals having low critical thinking about media content perceive an especially low level of severity of COVID (Panel A) and benefits of social distancing (Panel B). In contrast, we note that the effect of critical thinking is reduced as the level of fear increases. Individuals reporting a high level of fear recognize the severity of getting COVID and the benefits of social distancing; the effect of critical thinking for these two variables is reduced for heightened level of fear.

Interaction with critical thinking
Effects of our control variables
Given the particularities of the pandemic (see Table 4), we pay special attention to our control variables. First, age has an amplifying effect on media exposure, severity/COVID, and susceptibility/COVID (all p’s < .05), as well as a negative effect on panic buying (β = −.18, p < .001). Second, we find that women, compared to men, are associated with greater scores on fear and social distancing (all p’s < .01). Third, job insecurity has a positive effect on media exposure, fear, and panic buying (p’s < .05) as well as a negative effect on severity, benefits of social distancing, and practice of social distancing (p’s < .01).
Post hoc analyses
We conducted four additional analyses. First, we replicated the trajectories of perceived media exposure with archival media data. Then, we did three robustness checks; see details in Web Appendices E, F, and G.
Archival data for media exposure
Because individuals’ perceptions of media exposure may not reflect their actual behavior, we complemented this perceptual measure with archival data (Fig. 5). We used two datasets to estimate the press coverage of COVID and the level of word-of-mouth in social media. First, to estimate the press coverage, we used the Eureka database, which tracks million of news items published in Canadian and international press outlets. For our timeframe, there were 215,983 COVID-related articles published in Quebec in 437 generalist news outlets (Fig. 5, Panel A). Second, we estimated the level of electronic word-of-mouth about COVID by examining the reactions to COVID-related posts (i.e., likes, retweets, and comments) on Twitter (Fig. 5, Panel B). As most communications from the government were made through the Premier of Quebec, we focused on his Twitter account (@francoislegault), which has 278,200 followers. This account is much larger than the Government’s official account with only 17,200 followers. As shown in Fig. 5 (Panels A and B), the evolutions of our objective variables (i.e., media coverage, and Twitter-related word-of-mouth) are consistent with the evolution of our variable perceived media exposure (Fig. 2, Panel A). Here, two chi-square tests (all p’s < .001) indicates that the frequencies are generally different from each other in Panels A and B. In sum, there were more media coverage and tweet reactions during the first two months (top of wave 1). These statistics decrease during June and July (middle of wave 1) and reach their lowest level in August (bottom of wave 2). Then, we note a slow increase in September (growth of wave 2).

Objective data about media exposure in Quebec. Note: Results mentioning “COVID” within the text from the local, provincial, and regional generalist press outlets for Quebec (n = 437) during the period of interest (retrieved from Eureka.cc database on July 28, 2021). Note: Total reactions (i.e., likes, comments and retweets) associated to COVID- related posts from the Premier of Quebec, Francois Legault Twitter account (@francoislegault)
Three robustness checks
First, we conducted a series of LMM models in which we account for the effects of the variable “negative evaluation of media content” (Web Appendix E). We did this to test the robustness of the effect of media exposure on fear. Although “negative evaluation of media content” tends to reduce the level of fear, its inclusion does not affect the significance and nature of any of our prior results.
Second, we also employed the marker-variable technique as a post hoc remedy to account for the presence of any remaining common method bias (Web Appendix F). We used “neo-racism” as the marker variable. In sum, the presence of this marker does not change the direction, amplitude, or significance of any of our prior results.
Third, we replicated our results with two smaller samples (Web Appendix G). In the first sample, since the number of participants becomes small at times 5 and 6, we replicated all our analyses with only periods 1–4. We have 2065 observations in this first sample (see Tables G1-G3). In the second sample, we use only the 190 participants who completed the four measurement periods for a total of 756 observations (see Tables G4-G6). Despite some minor differences, almost all our hypotheses remain supported with smaller samples.
General discussion
We propose a unique theoretical assemblage that maps the processes that lead to the adoption of social distancing and panic buying, two crucial behaviors that policymakers try to manage in a pandemic. Using the HBM as our cornerstone, we inject to this theory three new conceptual elements that are needed in the context of a pandemic. First, we start our model with the notion of propagation wave, which reflects the severity of a pandemic. Second, we incorporate variables capturing the influence of mass media given their crucial role in a pandemic. Third, we study the adaptive role of fear, which allows the development of health beliefs. Our framework was tested with 2269 observations collected over a six-month period in Quebec. Our hypotheses were tested by using LMM and MLmed (Diggle et al., 2002; Rockwood, 2019). Out of six hypotheses, five are supported (H5 is the exception). Next, we discuss the theoretical implications of the three core processes of our framework.
The crucial role of mass media in communicating crisis severity and generating fear
By adopting a longitudinal approach, we show that the need for information evolves during a pandemic by following the shape of a propagation wave. Indeed, media exposure peaks at the top of a wave, and it fluctuates by following waves’ oscillations. As a core result (H1), we find that media exposure mediates over time the effects of propagation wave on fear of COVID. We conclude that people’s fear is not directly triggered by governments’ objective description of the severity of the virus. Such a fear is rather created over time by the information obtained through media exposure. This result is important for policymakers and media companies; it shows the crucial role that media play in conditioning individual responses to the pandemic.
This first process combines two literatures—crisis marketing and health communication—which have been rarely integrated in the past. The marketing crisis literature typically focuses on crises of a different nature than pandemics (e.g., product harm crisis). For instance, Khamitov et al. (2020) found that little research on crisis (2.3%) had been conducted in a health context. As a typical marketing crisis usually affects a small part of a population, this literature did not see the necessity of studying the role of mass media (Cleeren et al., 2017). We address this issue by testing the relationship between crisis severity and media coverage and by integrating the variable critical thinking about media content (e.g., Radanielina Hita et al., 2018).
The fear-based processes leading to social distancing and panic buying
Our results suggest that fear is adaptive in a pandemic because this emotion leads to the development of appropriate beliefs, which in turn condition adaptive behaviors. The linkage between fear and the development of health beliefs is an under-researched topic (Sulat et al., 2018) that needs to be considered in a pandemic context. In support of H2, we find that the effects of fear on social distancing are mediated by all three health beliefs. As per H3, only “susceptibility” mediates the path between fear and panic buying. This finding is consistent with prior research suggesting that threat appeals combined with perceived susceptibility are effective at generating strong responses (e.g., Tannenbaum et al., 2015).
In contrast to some prior research that shows the ineffectiveness of fear appeals in advertising (Hammond, 2011), we find a beneficial effect of fear, which can be explained by two reasons. First, this effect can occur because the threat of COVID was viewed as being more believable and imminent that the threat suggested in social advertising (cigarettes, HIV-AIDS, alcohol, or car speeding; Hammond, 2011; Earl & Albarracín, 2007). We believe that people are less resistant to believe the threat of a pandemic, given its immediate impact on everybody. Second, our context is different from prior work that examines fear generated by advertising (Keller & Lehmann, 2008; Tannenbaum et al., 2015). In our research, the starting points are “real” indices of the severity of a pandemic (e.g., deaths) rather than scenarioized advertising.
The beneficial effects of critical thinking about media content
Our results suggest that the effects of critical thinking about media content are rich and complex. In terms of main effects, this form of critical thinking simultaneously “amplifies” adaptive responses and “reduces” maladaptive responses (H4). In terms of moderation effects, critical thinking does not influence the path between media exposure and fear; H5 is not supported. However, consistent with H6ac, this competence moderates the linkage between fear and two health beliefs (severity and benefits). The virtuous amplifying effect of critical thinking is especially important among less fearful consumers (see Fig. 4). In the end, our results suggest that less fearful individuals having low critical thinking are especially at risk. They are less likely to develop the beliefs leading to safety measures.
To the best of our knowledge, no research has ever examined the longitudinal effect of critical thinking in the context of an ongoing pandemic. Most of the research on critical thinking about media content uses cross-sectional data (e.g., Austin et al., 2015; Radanielina Hita et al., 2018). Our research is arguably the first to show the long-term beneficial effects of critical thinking to increase adaptive responses during an ongoing pandemic crisis. This last contribution is important because this competence can be taught and learned, as we see next.
Implications for policymakers and marketing
The crucial role of media exposure (H1)
In the context of a pandemic, mass media have much power, as they become people’s main source of information; policymakers only have an indirect influence on their populations. This finding speaks to the importance for policymakers and media companies to collaborate and build strong relationships with one another. As far as possible, governments need to ensure that mass media report accurate information, especially at the peak of a wave. This finding also highlights the danger associated with some media that provide a biased view of the pandemic, which could misguide individuals. Given the dangers associated with unverified information, policymakers need to put in place measures to help individuals develop their ability to identify misinformation. Because of free speech, policymakers cannot easily control media content through regulations. However, they can help people develop stronger critical thinking about media content (as we see next).
In addition, policymakers should capitalize on people’s willingness to listen at the tops of propagation waves. At such moments, effective communication could influence the trajectory of the crisis. For instance, the Twitter account of Quebec’s prime minister was being actively followed during the top of wave 1 when many COVID-related policies and safety measures were implemented. Effective communication at the peak of a wave is even more important in the era of digital communication when policymakers’ voices are just one among many.
Fear-based processes (H2-H3)
Building on the fear-based processes depicted in H2 and H3, we suggest that policymakers and media companies frame their messages by eliciting a reasonable level of fear and by referring to the three components of the HBM (see Appendix H for examples of COVID ad campaigns). Here, the role of media companies is especially important given their influence (see prior point). First, fear appears adaptive in our context; this emotion is the strongest predictor leading to the development of health beliefs. However, it is also important not to go overboard with the generation of fear. Policymakers and mass media need to strike the proper tone. Research on fear appeals suggests that when fear appeals are too extreme, they become ineffective and even counterproductive (Feinberg & Willer, 2011). Second, in framing their messages, mass media need to highlight both the threats associated with the virus (in terms of severity and susceptibility) and the benefits of a protective measures (e.g., social distancing). Our results suggest that a communication needs both components—highlighting the threat and explaining the virtues of a measure—to lead to the adoption of adaptive behaviors. Too much emphasis on the threat is likely to lead to maladaptive behavior, such as panic buying.
The beneficial effects of critical thinking (H4-H6)
An important implication refers to the development of critical thinking about media content. Our findings indicate that fear, health beliefs, and social distancing are positively influenced by consumers’ ability to critically evaluate media content. Additionally, critical thinking leads to less panic buying. In the weeks following the outbreak of the pandemic, scenes of empty shelves were common in the media, which led to a form of panic and “herd” mentality. This example shows the influence of media as a “super peer” (Strasburger & Wilson, 2002). If consumers do not possess a high level of critical thinking, they are more likely to internalize this “super-influence” and give in to panic.
In the prevention literature, critical thinking was developed by media literacy programs delivered offline or via web-based trainings (Austin et al., 2020). Media literacy trainings have been incorporated in a variety of prevention programs (e.g., Food in a Marketing-Driven World, Austin et al., 2020). By getting inspired by these existing programs, policymakers could develop web-based media literacy training to increase the general population’s critical thinking about COVID-related content. By collaborating with national media literacy organizations (National Association for Media Literacy Education (NAMLE), 2020), governments could offer short web lessons about media literacy (e.g., “how to discriminate between accurate/inaccurate information”, etc.). Improved critical thinking should lead to more information seeking behaviors with the purpose of validating the quality of information and debunking false claims.
To maximize the effectiveness of such programs, it is important to adapt the training for different segments of consumers. For instance, our research shows that in the context of low media exposure, people with low critical thinking experience little fear, which could lead to lower adaptive beliefs. For these individuals, their media literacy training should focus on promoting a more systematic processing of information and a more intensive use of trustworthy media. They should become reasonably aware of the dangers of the virus. In turn, when people are highly afraid of the virus, their training should focus on maximizing the cognitive route of decision making so that they will not act on emotion and fear alone.
Limitations and future research
As in all work, our research includes a series of limitations. First, the use of retrospective methods may create recall bias; therefore, future research could test our model with other methods (e.g., social networks). Second, the decision to focus on Quebec makes it difficult to generalize the findings to all populations. Future research could generalize our results to other populations with different attributes (e.g., rural vs. urban, liberal vs. conservative, developed vs. developing). Third, our longitudinal design does not allow establishing causal inference; experiments are more appropriate for this. Fourth, given the collective aspect of the pandemic, it would have been interesting to understand how community-level variables (such as social pressure or social compliance) could have influenced our outcomes, especially social distancing.
Fifth, despite our efforts to combine perceptual measures with archival data, future research could benefit from additional objective measures, such as other social media metrics or physio-neurological measures. In turn, one of our post hoc analyses measures a key construct with a single item (i.e., negative evaluation of media content). Given the importance of this construct, future research should use a stronger scale for this notion. In addition, future research should incorporate other outcome of interest including vaccination and mask wearing.
Sixth, it would be important to understand the independent contribution of social vs. traditional media on the components of our model. Future research could capture media exposure separately for traditional and online media. In addition, our perceptual measure of media exposure does not differentiate between “unvoluntary” vs. “voluntary” media exposure, and it does not capture participants’ level of elaboration when processing a message. Further research could benefit from studying these elements.
Seventh, given the relative complexity of our model, we test only one moderator of level 2—that is, critical thinking about media content. Since we tried to inject a “mass media” component to the HBM, the selection of this trait seems logical. However, there is place for the exploration of other moderators, such as perceived efficacy, medical literacy, or political orientation. These moderators would potentially play a role in our model. Eighth, given the current context, further research would benefit from the inclusion of a variable related to misinformation or conspiracy beliefs which could affect individuals’ health beliefs. It would be interesting to analyze the responses to a pandemic by using other theories than the HBM. For instance, theories related to message compliance appear promising.
Notes
Consumers’ perception of their own media exposure may not reflect their actual exposure. To address this limitation, we collected objective media variables (i.e., COVID press coverage and Twitter reactions) over the same period, which will be compared to perceptual media exposure in the results section.
Our model also includes three additional longitudinal processes: “media exposure → fear → HBM components.” Although we test for these indirect effects, we do not present them in the theory section to avoid redundancies. These effects rely on the same logic and main effects that we use to build H1-H3.
Other dimensions of media literacy education include media skills, intercultural dialogue, media participation, and civic engagement (National Association for Media Literacy Education (NAMLE), 2020).
Hulland et al. (2018) note that reporting the initial response rate is not critical when the general purpose of a research study is theory driven. Consistent with this view, the initial response rate of panel data is usually not reported in academic research (e.g., Baehre et al., 2022; Bolander et al., 2021; Lamey et al., 2021). That being said, we gladly do so in this research for the sake of completeness and transparency.
We measured critical thinking over our six periods to validate that this variable is truly a stable individual difference. To do so, we conducted a linear mixed model that examines the effects of the six periods on the evolution of critical thinking. Consistent with a conceptualization as a trait variable, the level of critical thinking remains the same over the six periods; none of the periods differs from the reference category (all p’s > .17).
We also find a significant effect of the first period (April, top of wave 1) on the practice of social distancing. However, this effect is more localized (only the first period) and of lesser importance compared to media exposure.
These different coefficients come from the different LMM models conducted in this research.
The between-individuals indirect effect is calculated by mean-centering all the repeated values, and by conducting traditional mediation analyses (Bauer et al., 2006); this indirect effect reflects a static perspective of the process.
References
Ahmadi, I., Habel, J., Jia, M., Lee, N., & Wei, S. (2021). Consumer stockpiling across cultures during the COVID-19 pandemic. Journal of International Marketing, forthcoming
Austin, E. W., Austin, B., Kaiser, C. K., Edwards, Z., Parker, L., & Power, T. G. (2020). A media literacy-based nutrition program fosters parent-child food marketing discussions, improves home food environment, and youth consumption of fruits and vegetables. Childhood Obesity, 16(S1), S33–S43.
Austin, E. W., Chen, M., & Grube, J. W. (2006). How does alcohol advertising influence underage drinking? The role of desirability, identification and skepticism. Journal of Adolescent Health, 38(4), 376–384.
Austin, E.W., Pinkleton, B., Beam, M. & Porismita, B. (2013). Celebrities and media literacy:
Austin, E. W., Pinkleton, B. E., Chen, Y., & Austin, B. W. (2015). Processing of sexual media messages improve due to media literacy effects on perceived message desirability. Mass Communication and Society, 18(4), 399–421.
Baehre, S., O’Dwyer, M., O’Malley, L., & Lee, N. (2022). The use of net promoter score (NPS) to predict sales growth: Insights from an empirical investigation. Journal of the Academy of Marketing Science, 50(1), 67–84.
Bauer, D. J., Preacher, K. J., & Gil, K. M. (2006). Conceptualizing and testing random indirect effects and moderated mediation in multilevel models: New procedures and recommendations. Psychological Methods, 11(2), 142–163.
Beatty, S. E., & Ferrell, M. E. (1998). Impulse buying: Modeling its precursors. Journal of Retailing, 74(2), 169–191.
Birmingham, W. C., Hung, M., Boonyasiriwat, W., Kohlmann, W., Walters, S. T., Burt, R. W., & Kinney, A. Y. (2015). Effectiveness of the extended parallel process model in promoting colorectal cancer screening. Psycho-Oncology, 24(10), 1265–1278.
Bolander, W., Chaker, N. N., Pappas, A., & Bradbury, D. R. (2021). Operationalizing salesperson performance with secondary data: Aligning practice, scholarship, and theory. Journal of the Academy of Marketing Science, 49(3), 462–481.
Bolander, W., Dugan, R., & Jones, E. (2017). Time, change, and longitudinally emergent conditions: understanding and applying longitudinal growth modeling in sales research. Journal of Personal Selling & Sales Management, 37(2), 153–159.
Bureau of Labor Statistics, U.S. Department of Labor (2020) The Economics Daily: Unemployment rate rises to record high 14.7 percent in April 2020. Retrieved March 9, 2020 from https://www.bls.gov/opub/ted/2020/unemployment-rate-rises-to-record-high-14-point-7-percent-in-april-2020.htm?view_full
Campbell, M. C., Inman, J. J., Kirmani, A., & Price, L. L. (2020). In times of trouble: A Framework for Understanding Consumers’ Responses to Threats. Journal of Consumer Research, 47(3), 311–326.
Carpenter, C. J. (2010). A meta-analysis of the effectiveness of health belief model variables in predicting behavior. Health Communication, 25(8), 661–669.
Centers for Disease Control and Prevention. (2022). What We Know about the Variants. Retrieved on March 14, 2022 from https://www.cdc.gov/coronavirus/2019-ncov/variants/about-variants.html.
Chen, J. (2021). A structural model of purchases, returns, and return-based targeting strategies, A structural model of purchases, returns, and return-based targeting strategies Journal of the Academy of Marketing Science, forthcoming
Chin, J. H., & Mansori, S. (2019). Theory of planned behaviour and health belief model: Females’ intention on breast cancer screening. Cogent Psychology, 6(1), 1–12.
Cleeren, K., Dekimpe, M. G., & van Heerde, H. J. (2017). Marketing research on product-harm crises: A review, managerial implications, and an agenda for future research. Journal of the Academy of Marketing Science, 45(5), 593–615.
Das, G., Jain, S. P., Maheswaran, D., Slotegraaf, R. J., & Srinivasan, R. (2021). Pandemics and marketing: Insights, impacts, and research opportunities. Journal of the Academy of Marketing Science, 49(5), 835–854.
De Cuyper, N., Schreurs, B., Elst, T., Vander, Baillien, E., & De Witte, H. (2014). Exemplification and perceived job insecurity: Associations with self-rated performance and emotional exhaustion. Journal of Personnel Psychology, 13(1A), 1–10.
de Vreese, C. L., & Neijens, P. (2016). Measuring media exposure in a changing communications environment. Communication Methods and Measures, 10(2–3), 69–80.
Diggle, P. J., Heagerty, P., Liang, K. Y., & Zeger, S. (2002). Analysis of Longitudinal Data. Oxford University Press.
Earl, A., & Albarracín, D. (2007). Nature, decay, and spiraling of the effects of fear-inducing arguments and HIV counseling and testing: A meta-analysis of the short- and long-term outcomes of HIV-prevention interventions. Health Psychology, 26(4), 496–506.
Fall, E., Izaute, M., & Chakroun-Baggioni, N. (2018). How can the health belief model and self-determination theory predict both influenza vaccination and vaccination intention? A longitudinal study among university students. Psychology and Health, 23(6), 746–764.
Feinberg, M., & Willer, R. (2011). Apocalypse soon? Dire messages reduce belief in global warming by contradicting just-world beliefs. Psychological Science, 22(1), 34–38.
Glanz, K., Rimer, B. K., & Viswanath, K. (2008). Health behaviour and health education (4th Edition). In Health Behavior and Health Education: Theory, Research, and Practice. John Wiley & Sons.
Greer, A. L. (2013). Can informal social distancing interventions minimize demand for. antiviral treatment during a severe pandemic? BMC Public Health, 13(1), 1–9.
Grégoire, Y., Ghadami, F., Laporte, S., Sénécal, S., & Larocque, D. (2018). How can firms stop customer revenge? The effects of direct and indirect revenge on post-complaint responses. Journal of the Academy of Marketing Science, 46(6), 1052–1071.
Hammond, D. (2011). Health warning messages on tobacco products: A review. Tobacco Control, 20(5), 327–337.
Herjanto, H., Amin, M., & Purington, E. F. (2021). Panic buying: The effect of thinking style And situational ambiguity. Journal of Retailing and Consumer Services, 60(5), 1–10.
Hulland, J., Baumgartner, H., & Smith, K. M. (2018). Marketing survey research best practices: Evidence and recommendations from a review of JAMS articles. Journal of the Academy of Marketing Science, 46(1), 92–108.
IBM SPSS Statistics (2021) “Linear Mixed Models” Documentation for SPSS 23.0.0, Retrieved on August 3rd 2021 from https://www.ibm.com/docs/en/spss-statistics/23.0.0?topic=option-linear-mixed-models
Institut National de Santé Publique du Québec. (2021). Données COVID-19 au Québec. Retrieved March 9, 2021 from https://www.inspq.qc.ca/covid-19/donnees
Islam, T., Pitafi, A. H., Arya, V., Wang, Y., Akhtar, N., Mubarik, S., & Xiaobei, L. (2021). Panic buying in the COVID-19 pandemic: A multi-country examination. Journal of Retailing and Consumer Services, 59(3), 1–13.
Jakobsen, M., & Jensen, R. (2015). Common method bias in public management studies. International Public Management Journal, 18(1), 3–30.
Janssens, K., Lambrechts, W., van Osch, A., & Semeijn, J. (2019). How consumer behavior in daily food provisioning affects food waste at household level in the Netherlands. Foods, 8(10), 1–19.
Jones, C. J., Smith, H., & Llewellyn, C. (2014). Evaluating the effectiveness of health belief model interventions in improving adherence: A systematic review. Health Psychology Review, 8(3), 253–269.
Keller, P. A., & Lehmann, D. R. (2008). Designing effective health communications: A meta-analysis. Journal of Public Policy & Marketing, 27(2), 117–130.
Khamitov, M., Grégoire, Y., & Suri, A. (2020). A systematic review of brand transgression, service failure recovery and product-harm crisis: Integration and guiding insights. Journal of the Academy of Marketing Science, 48(3), 519–542.
Lamey, L., Breugelmans, E., Vuegen, M., & ter Braak, A. (2021). Retail service innovations and their impact on retailer shareholder value: Evidence from an event study. Journal of the Academy of Marketing Science, 49(4), 811–833.
Laufer, D., Silver, D. H., & Meyer, T. (2005). Exploring differences between older and younger consumers in attributions of blame for product harm crises. Academy of Marketing Science Review, 7, 1–24.
MacKenzie, S. B., & Podsakoff, P. M. (2012). Common method bias in marketing: Causes, mechanisms, and procedural remedies. Journal of Retailing, 88(4), 542–555.
Matrajt, L., & Leung, T. (2020). Evaluating the effectiveness of social distancing interventions to delay or flatten the epidemic curve of coronavirus disease. Emerging Infectious Diseases, 26(8), 1740–1748.
Meadows, C. Z. (2020). The effects of fear appeals and message format on promoting skin cancer prevention behaviors among college students. Societies, 10(1), 1–12.
National Association for Media Literacy Education (NAMLE). (2020). Core Principles of Media Literacy Education in the United States. Retrieved December 20, 2021 from https://namle.net/wp-content/uploads/2020/09/Namle-Core-Principles-of-MLE-in-the-United-States.pdf
Ohme, J., Albaek, E., de Vreese, H., & C. (2016). Exposure research going mobile: A smartphone-based measurement of media exposure to political information in a convergent media environment. Communication Methods and Measures, 10(2–3), 135–148.
Olagoke, A. A., Olagoke, O. O., & Hughes, A. M. (2020). Exposure to coronavirus news on mainstream media: The role of risk perceptions and depression. British Journal of Health Psychology, 25(4), 865–874.
Omar, N. A., Nazri, M. A., Ali, M. H., & Alam, S. S. (2021). The panic buying behavior of consumers during the COVID-19 pandemic: Examining the influences of uncertainty, perceptions of severity, perceptions of scarcity, and anxiety. Journal of Retailing and Consumer Services, 62(9), 1–12.
Ort, A., & Fahr, A. (2018). Using efficacy cues in persuasive health communication is more effective than employing threats–An experimental study of a vaccination intervention against Ebola. British Journal of Health Psychology, 23(3), 665–684.
Palmatier, R. W., Dant, R. P., & Grewal, D. (2007). A comparative longitudinal analysis of theoretical perspectives of interorganizational relationship performance. Journal of Marketing, 71(4), 172–194.
Peters, G. J. Y., Ruiter, R. A. C., & Kok, G. (2013). Threatening communication: A critical re-analysis and a revised meta-analytic test of fear appeal theory. Health Psychology Review, 7(sup1), S8–S31.
Pew Research Center. (2020). A third of Americans experienced high levels of psychological distress during the coronavirus outbreak. Retrieved March 9, 2020 from https://www.pewresearch.org/fact-tank/2020/05/07/a-third-of-americans-experienced-high-levels-of-psychological-distress-during-the-coronavirus-outbreak
Pinkleton, B., Austin, E., & Van de Vord, R. (2010). The role of realism, similarity and expectancies in adolescents’ interpretation of abuse-prevention messages. Health Communication, 25(3), 258–265.
Radanielina Hita, M. L., Kareklas, I., & Pinkleton, B. E. (2018). Parental mediation in the digital era: Increasing children’s critical thinking may help decrease positive attitudes toward alcohol. Journal of Health Communication, 23(1), 98–108.
Rindfleisch, A., Malter, A. J., Ganesan, S., & Moorman, C. (2008). Cross-sectional versus longitudinal survey research: Concepts, findings, and guidelines. Journal of Marketing Research, 45(3), 261–279.
Rockwood, Nicholas J. (2019). MLMED User Guide: Beta Version 2.0. Accessed at https://njrockwood.com/mlmed/ on August the 4th.
Rockwood, N. J., & Hayes, A. F. (in press). Multilevel mediation analysis. In A. A. O’Connell, D. B. McCoach, & B. Bell (Eds.), Multilevel Modeling Methods with Introductory and Advanced Applications. Information Age Publishing.
Ruiter, R. A. C., Kessels, L. T. E., Peters, G. J. Y., & Kok, G. (2014). Sixty years of fear appeal research: Current state of the evidence. International Journal of Psychology, 49(2), 63–70.
Sacerdote, B., Sehgal, R., & Cook, M. (2020). Why Is All COVID-19 News Bad News? (Vol. No. w28110). National Bureau of Economic Research.
Satirical news and critical thinking about politics (2013). APSA 2013 Annual Meeting Paper. American Political Science Association 2013 Annual Meeting.
Singer, J. D., & Willett, J. B. (2003). Applied longitudinal data analysis: Modeling Change and Event Occurrence. Oxford University Press.
Slater, M. D. (2004). Operationalizing and analyzing exposure: The foundation of media effects research. Journalism & Mass Communication Quarterly, 81(1), 168–183.
Statistics Canada. (2021). Census Profile, 2016 Census. Retrieved March 23, 2021 from https://www12.statcan.gc.ca/census-recensement/2016/dp-pd/prof/index.cfm?Lang=E.
Steenkamp, J. B. E., & Maydeu-Olivares, A. (2021). An updated paradigm for evaluating measurement invariance incorporating common method variance and its assessment. Journal of the Academy of Marketing Science, 49(1), 5–29.
Strasburger, V. C., & Wilson, B. J. (2002). Youth and media: Opportunities for development or lurking dangers? Children, Adolescents, and the Media. SAGE.
Sulat, J. S., Prabandari, Y. S., Sanusi, R., Hapsari, E. D., & Santoso, B. (2018). The validity of health belief model variables in predicting behavioral change: A scoping review. Health Education, 118(6), 499–512.
Tannenbaum, M. B., Hepler, J., Zimmerman, R. S., Saul, L., Jacobs, S., Wilson, K., & Albarracín, D. (2015). Appealing to fear: A meta-analysis of fear appeal effectiveness and theories. Psychological Bulletin, 141(6), 1178–1204.
Vander Elst, T., Van den Broeck, A., De Cuyper, N., & De Witte, H. (2014). On the reciprocal relationship between job insecurity and employee well-being: Mediation by perceived control? Journal of Occupational and Organizational Psychology, 87, 671–693.
West, B. T., Welch, K. B., & Gałlechki, A. T. (2007). Linear mixed models. A practical guide using statistical software. Chapman & Hall/CRC.
Wielgos, D. M., Homburg, C., & Kuehnl, C. (2021). Digital business capability: its impact on firm and customer performance. Journal of the Academy of Marketing Science, 49(4), 762–789.
World Health Organization (2021). Coronavirus disease (COVID-19) advice for the public. Retrieved on March 9, 2021, from https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public.
World Health Organization (2022). WHO Coronovirus (COVID-19) Dashboard. Retrieved on March 15, 2022. https://covid19.who.int/
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Brent McFerren served as Article Editor for this article.
Supplementary Information
ESM 1
(PDF 1352 kb)
Rights and permissions
About this article

Cite this article
Hita, M.L.R., Grégoire, Y., Lussier, B. et al. An extended health belief model for COVID-19: understanding the media-based processes leading to social distancing and panic buying. J. of the Acad. Mark. Sci. 51, 132–152 (2023). https://doi.org/10.1007/s11747-022-00865-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11747-022-00865-8