
Abstract
To validate the proxy version of the Quality of Life after Brain Injury (QOLIBRI) questionnaire to utilize caregivers for comparison and to evaluate the correspondence between patients’ self-perceived and caregivers’ perception of patients’ Health-Related Quality of Life (HRQoL). Ninety-two patients with severe TBI and their main caregivers were enrolled. Patients’ and caregivers’ HRQoL was assessed by the Patient-QOLIBRI (Pt-QOLIBRI) and the Proxy-QOLIBRI (Pro-QOLIBRI), respectively. The Pro-QOLIBRI is a modified version of the QOLIBRI to investigate caregivers’ perception of patients’ HRQoL (Pro-QOLIBRIpatient-centered), and their degree of satisfaction and botheredness (Pro-QOLIBRIcaregiver centered). The patients’ disability and their social reintegration was investigated by means of Glasgow Outcome Scale Extended and Community Integration Questionnaire. Pro-QOLIBRI has good internal consistency and homogeneity. There was also positive correlation between the level of satisfaction measured by Pro-QOLIBRI but not by Pt-QOLIBRI, and the disability severity and social integration of the patients. The comparison between the Pt-QOLIBRI and Pro-QOLIBRI confirmed the usefulness of the Pro-QOLIBRI, especially the caregiver-centered version, to predict the social reintegration of survivors. To our knowledge this is the first study that correlates the HRQoL of survivors, as self-perceived and as perceived by the caregivers with social reintegration.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Health-related quality of life (HRQoL) following traumatic brain injury (TBI) has been defined as “a person’s perspective on his or her subjective health condition, functioning and well-being in the domains of physical, psychological (emotional and cognitive), social and daily life” [1–3]. To assess HRQoL in terms of both satisfaction and botheredness as self-perceived by survivors of TBI, the Quality of Life after Brain Injury (QOLIBRI) questionnaire, i.e., both the extended and the short forms, was validated in persons with TBI [1–5]; results of the Italian validation of the QOLIBRI [6] shows statistically significant correlations with physical, neuropsychological, and social disability.
A relevant factor, which should be considered in the field of severe TBI, is impaired self-awareness [7–11], namely, the ability to be aware of one’s own thoughts, feelings, and mental states [12], which implies that one actively identifies, processes, and stores information about the self [13]. Impaired self-awareness consists of a partial or total reduction of the ability in recognizing problems due to the brain damage. Since low self-awareness can impair a patient’s capacity to estimate and self-report the individual’s post-TBI abilities, the reliability of tools that evaluate self-perceived quality of life by means of self-report scales in persons with TBI may be accordingly questionable [14].
Indeed, Sasse and coll [15] studied a population with prevalent mild TBI, and reported that a lower SA is associated with higher estimates of HRQoL, particularly in the cognitive domain. Conversely, in our recent study on more severe TBI, persons with low SA after TBI are less satisfied than patients with adequate SA (Formisano et al., submitted).
The primary aim of this study was to validate the proxy version of the QOLIBRI (i.e., the Pro-QOLIBRI). The secondary aim was to utilize caregivers for comparison, and to evaluate the correspondence between patients’ self-perceived Quality of Life (QoL) and caregivers’ perception of patients’ QoL.
Finally, we wish to verify the hypothesis that both patients’ and proxies’ HRQoL could be related to some TBI severity and disability indicators as well as to their social reintegration.
Materials and methods
Participants
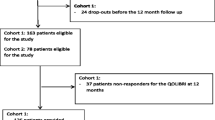
We enrolled 92 patients with severe TBI (75.0 % males and 25.0 % females) who had a Glasgow Coma Scale (GCS) [16] score equal to, or less than 8 in the first 24 h after coma onset. They were selected from a larger population of patients who had undergone TBI, and were enrolled in a multicenter national and international study (Appendices 1 and 2). All the patients had been discharged from the Santa Lucia Foundation Rehabilitation Hospital in Rome.
Each patient’s main proxy/caregiver was also enrolled. The population of caregivers included 69 females and 23 males (75 and 25 % respectively); 51 (55.4 %) were mothers, 16 (17.4 %) fathers, 14 (15.2 %) partners, and 11 (12.0 %) other relatives.
As in the international validation of the QOLIBRI, we administered the Pro-QOLIBRI with face-to-face interviews, self-reports, or telephone interviews [1].
The study was approved by the local ethics committee.
Inclusion criteria were: (a) diagnosis of TBI according to the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10) criteria (WHO 1992) [17]; (b) outpatient status; (c) time interval from TBI between 3 months and 15 years, in accordance with the inclusion criteria used in the multicenter international validation study of the QOLIBRI [1–4]; (d) score on the Levels of Cognitive Functioning Scale (LCF) >6; (e) being a relative of a patient with TBI; and (f) informed consent of patients and their caregivers.
The exclusion criteria were: (a) a Glasgow Outcome Scale Extended (GOS-E) [18] score <3; (b) spinal cord injury; (c) significant current or previous psychiatric disease or ongoing severe addiction; and (d) diagnosis of terminal illness.
Patients with vegetative state, minimally conscious state plus and minus, and patients with severe cognitive disability were excluded, since as inclusion criterion, the enrolled patients should be able to understand and answer the questions of the QOLIBRI questionnaire.
Quality-of-life evaluation
Patients’ and caregivers’ HRQoL were assessed with the Patient-QOLIBRI (Pt-QOLIBRI) [1–3] and the Pro-QOLIBRI, respectively.
The Pt-QOLIBRI was administered to all patients with the support of a trained psychologist when needed. Similarly, the Pro-QOLIBRI was administered to the main caregivers of the enrolled patients.
The Pt-QOLIBRI consists of 47 items and divided into two sections (A and B). Section A concerns the level of satisfaction, and consists of four subscales: cognition (seven items), self (seven items), daily life and autonomy (DLA) (seven items), social relationships (six items), and an overall section (six items), which provide a summary of the HRQoL issues investigated by each QOLIBRI subscale.
Section B concerns the discomfort/bother domain and consists of three subscales: emotions (five items), physical problems (four items), and physical conditions (four items). In Section B, there is also one item that provides a summary of discomfort conditions investigated in this section.
The Pro-QOLIBRI is a modified patients’ version of the QOLIBRI, which was developed to investigate caregivers’ perception of patients’ HRQoL (Pro-QOLIBRIpatient-centered) and their level of satisfaction and degree of botheredness (Pro-QOLIBRIcaregiver-centered).
As Pt-QOLIBRI, the Pro-QOLIBRI consists of 47 items and divided into two sections (A and B). Section A concerns the level of satisfaction, and consists of four subscales: cognition (seven items), self (seven items), daily life and autonomy (DLA) (seven items), social relationships (six items), and an overall Section (six items), which provide a summary of the HRQoL issues investigated by each QOLIBRI subscale.
Section B concerns the discomfort/bother domain, and consists of three subscales: emotions (five items), physical problems (four items), and physical conditions (four items). In Section B, there is also one item that provides a summary of discomfort conditions investigated in this section.
Unlike the Pt-QOLIBRI, each item of Pro-QOLIBRI was administered in two versions: the first “Patient-centered” (i.e., “In your opinion how much is your son/daughter/father…. satisfied with the ability to express themselves?”) and the second “Caregiver-centered” (i.e., “how much are you satisfied with the ability of your son/daughter/father…. to express themselves?”).
The Pro-QOLIBRI and Pt-QOLIBRI items are rated on a five-point Likert scale: 1 (Not at all), 2 (Slightly), 3 (Moderately), 4 (Quite), and 5 (Very). Section B also provides an additional response (“Not applicable”) considered as “Not at all” in the statistical analysis, in agreement with the international validation of the QOLIBRI [1–4]. According to the International and Italian validation of the QOLIBRI [1–4, 6], the scores in Section B (discomfort/bother) were reversed to give the QOLIBRI subscales the same direction, that is, the best situation was associated with higher scores, as in Section A (level of satisfaction). For each QOLIBRI subscale, a score was calculated by summing each item and was presented as a percentage (0–100 %) of the maximum possible score; missing data were imputed using horizontal mean imputation.
Patients’ social reintegration evaluation
The CIQ (Community Integration Questionnaire) [19] is focused on the social reintegration of the person over the past month. It is composed of three parts: familiar integration, social integration, and work integration. A different score is computed for each of the three areas, with a maximum total score of 29, obtained by summing the three areas.
Data analysis
The Kruskall–Wallis χ2 for equality-of-medians rank test and the Cuzick non-parametric test for trend between ordered groups were performed. Spearman rho correlation (with Bonferroni correction) was performed to correlate QOLIBRI subscales with severity indicators, such as GOS-E and coma length. We assumed that the two QOLIBRI scales were: (a) functionally unitary if ρ > 0.80; (b) shared a common construct if ρ = 0.60–0.79; and (c) were mostly unique, but had something in common, if ρ = 0.40–0.59. Internal consistency was assessed using Cronbach’α. The following values are widely accepted in the social sciences: a cutoff of α = 0.70 for a set of items to be considered as acceptable for a scale and α > 0.90 for clinical application. The most important measure that a set of items must meet to constitute an acceptable survey construct is Loevinger’s homogeneity coefficient (H). Indeed, to evaluate the homogeneity of the Pro-QOLIBRI scales, Loevinger’s H coefficient was used and a cutoff of 0.5 was chosen to indicate strong homogeneity [20]. Data analysis was carried out using Stata/SE 13.1 (StataCorp, College Station, Texas, USA).
Results
The socio-demographic and clinical characteristics of the patients are reported in Table 1.
For each subscale of Pro-QOLIBRI, no statistically significant difference is found between male’s and female’s scores.
Internal consistency was assessed for each version of the Pro-QOLIBRI (patient-centered and caregiver-centered) (see Table 2). In Section A of the questionnaire (level of satisfaction), the only low value of Cronbach’s α regards the Patient-centered Cognition subscale (α = 0.32). The other individual subscale scores exceed α = 0.80, ranging from 0.85 for social relationship (patient-centered scale) to 0.91 of DLA (caregiver-centered scale). In Section B, both Emotions individual scores exceed Cronbach’s α = 0.70 as well as the Physical Problems score (caregiver-centered).
Results indicate that the Pro-QOLIBRI scores generally have good internal consistency as well as good internal homogeneity. Indeed, all individual scale scores in Section A (level of satisfaction) exceed Loevinger’s H = 0.50 (Table 2). No individual item score in Section B (level of discomfort) shows strong homogeneity, but both Emotions individual items and Physical Problems item scores (caregiver-centered) exceed Loevinger’s H = 0.40, showing medium-strong homogeneity according to Mokken [20].
Finally, the Physical Condition score (patient-centered) shows Loevinger’s H = 0.37, which indicates a clinically useful scale. The Loevinger’s Hs are supportive of strong scale homogeneity.
Results indicate that the Pro-QOLIBRI scale has good internal homogeneity.
Consistent with the results of internal consistency and homogeneity, all Pro-QOLIBRI individual items in Section A positively correlate with each other with a statistically significant Spearman rho coefficient (Table 3) ranging from ρ = 0.5235 for cognitionpatient-centered vs social relationshipcaregiver-centered to ρ = 0.8859 (social relationshippatient-centered vs social relationshipcaregiver-centered).
As expected, all Pt-QOLIBRI sub-scores correlate with each other within each scale (p < 0.01 in all the cases) as do the Pro-QOLIBRI sub-scores of both patient-centered and caregiver-centered versions (p < 0.01 in all cases). Instead, regarding the correlation between Pt-QOLIBRI and Pro-QOLIBRI sub-scores, only a few correlations are found. In particular, in the Satisfaction domain, significant differences are found between the Pt-QOLIBRI and Pro-QOLIBRIpatient-centered vs Pro-QOLIBRIcaregiver-centered sub-scores. Indeed, among the 50 possible correlations between the five Pt-QOLIBRI subscales and both Pro-QOLIBRI versions sub-scores, 27 are statistically significant (54 %), 19 are between the Pt-QOLIBRI and the Pro-QOLIBRIpatient-centered version, and only 8 are between the Pt-QOLIBRI and the Pro-QOLIBRIcaregiver-centered version (Fisher’s Exact Test: p = 0.004) (see Table 3). In this domain, the highest statistically significantly correlated subscales are the social relationshippatient-centered, Overall and Selfcaregiver-centered version.
There is also a statistically significant positive relationship between the level of satisfaction measured by all the Pro-QOLIBRI subscales and the social integration of the patients assessed by CIQ, which ranges from ρ = 0.4323 for cognitionpatient-centered to ρ = 0.6845 for DLAcaregiver-centered; that is, the higher the patients’ score on the CIQ scale (indicating they were more integrated), the higher their caregivers’ QOLIBRI score (i.e., they were more satisfied).
All individual Pro-QOLIBRI item scores correlate with GOS-E, although the correlation is weaker than with the CIQ. Moreover, the GOS-E weakly correlates with Cognitionpatient-centered (ρ = 0.3384). As expected, the correlation between the caregiver’s level of satisfaction, measured by the Pro-QOLIBRI, and coma length is negative: (the longer the duration of coma, the less satisfied the caregiver), but this negative correlation is not statistically significant (Table 4).
According to the non-parametric analysis performed with the Kruskall–Wallis test, the median scores in Section A of the Pro-QOLIBRI (level of satisfaction of the caregiver) for the five subscales increase with the outcome level of the patients evaluated by the GOS-E (Table 5); that is, the more favorable the patient’s outcome and the higher the median level of the caregiver’s satisfaction. Performing the non-parametric test for trend across ordered groups [21], we observe a significant increasing trend for the median scores of each QOLIBRI subscale.
According to the Spearman correlation, all Pro-QOLIBRI individual item scores in Section B (level of discomfort) are significantly correlated with each other (Table 6), ranging from ρ = 0.4090 for Physical Problemspatient-centered vs Emotionscaregiver-centered to ρ = 0.9350 for Physical Condition (patient vs caregiver). In the bother domain (which includes four subscales), only 8 of the 32 possible correlations (25 %) are significantly correlated among the Pt-QOLIBRI and both versions of the Pro-QOLIBRI; 6 of them regarded the Physical Problems items, which correlate for both the patient-centered and the caregiver-centered versions with the following subscales: limitations, physical problems, and overall of the Pt-QOLIBRI items. In Section B, higher correlations are also found among the subscales of the same version of the Pro-QOLIBRI (patient-centered and caregiver-centered).
According to Table 7, statistically significant positive correlations between the level of discomfort measured by the three Pro-QOLIBRI items scores (emotions, limitations, and physical problems) and the social integration of the patients assessed by CIQ are demonstrated, except for the physical problems items score, which ranges from ρ = 0.4919 for physical problems (patient-centered) to ρ = 0.6275 for the overall Condition (caregiver-centered). Only the Pro-QOLIBRI Physical Problems item and the Summary Discomfort Condition (caregiver-centered) correlate with GOS-E, but more weakly than with CIQ. As in Section A, the correlation between the caregiver’s level of bother and the patient’s coma length is negative but not statistically significant.
As for Section A, the median scores in Section B of the Pro-QOLIBRI (level of bother/discomfort of the caregiver) for the individual items scores increase slightly with the improved outcome of the patients evaluated with the GOS-E (see Table 5), except for the scores on the physical conditions items.
According to the Spearman correlation analysis, the only statistically significant correlations between the Pt-QOLIBRI and the GOS-E are found with Daily Life and Autonomy (DLA) in the Satisfaction domain and with the overall subscales in the satisfaction and bother domain. Instead, the Pro-QOLIBRIpatient-centered correlates with the GOS-E for all subscales except cognition in the satisfaction domain, and correlates only with the limitations subscale in the bother domain. In addition, the Pro-QOLIBRIcaregiver-centered is significantly correlated with the GOS-E for all subscales except Emotion and Physical Problems in the bother domain (see Table 8). With regard to social reintegration, none of the Pt-QOLIBRI subscales correlate with the Community Integration Questionnaire (CIQ); conversely, all the Pro-QOLIBRI subscales correlated with the level of social reintegration except for physical problems in the bother domain, which again seems to be the subscale least correlated with the level of social reintegration and with disability outcome severity (GOS-E) (Table 8).
Discussion
The comparison between the Pt-QOLIBRI and Pro-QOLIBRI confirms the utility of the Proxy-QOLIBRI, especially the caregiver-centered version, at least for predicting the social reintegration of persons with TBI.
This emphasizes that a similar relationship between patients’ and caregivers’ viewpoints has been reported in other neurological disorders [22–24].
In the present study, we first aim to validate the proxy version of the QOLIBRI in an Italian sample of caregivers of persons with TBI. The statistical analysis demonstrates the internal consistency of the Proxy-QOLIBRI as well as its high relationship with patients’ outcome in terms of both severity of disability and social reintegration.
As expected, higher disability as outcome in patients corresponds with worse quality of life of the persons with TBI as perceived by their caregivers, as emerged from the correlation between most Pro-QOLIBRIcaregiver-centered scores and patients’ GOS-E and CIQ scores. These data suggest that, coherently with the QOLIBRI already largely used to assess HRQoL in patients with TBI, the Proxy-QOLIBRI can also be used in the field of TBI to assess the same variables perceived by caregivers.
Another aim of the study is to verify the hypothesis that both patients’ and proxies’ HRQoL could be related to some severity indicators and functional outcome of patients and their social integration, or restricted social participation, according to the bio-psychosocial model (ICF). Indeed, since the HRQoL reflects patients’ perspectives about their subjective health condition, functioning and well-being [1], the high number of statistically significant correlations between the Pt-QOLIBRI and the Pro-QOLIBRIpatient-centered version scores might demonstrate the reliability of the self-perceived quality of life of patients and the great ability of caregivers to empathize with patients, as previously reported [25]. However, given that the Pt-QOLIBRI and Pro-QOLIBRIpatient-centered overlap, utilizing the Pro-QOLIBRIpatient-centered to assess patients’ HRQoL might be redundant; therefore, we suggest using both the Pt-QOLIBRI and the Pro-QOLIBRIcaregiver-centered to evaluate not only the quality of life of patients, but also the quality of social reintegration of the whole family system.
The present study also demonstrates how different caregivers’ HRQOL can be from patients’ HRQoL based on the lower scores on both the satisfaction and bother sections of the Pro-QOLIBRIcaregiver-centered version with respect to the Pt-QOLIBRI. Indeed, in line with a previous study [15], it is also likely that in our sample of patients, self-awareness issues may have compromised their ability to congruently estimate their quality of life, especially regarding social post-TBI consequences. This hypothesis is supported by the low number of correlations between the Pt-QOLIBRI and the GOS-E scores (except for Daily Life and Autonomy in the Satisfaction section and overall bother), as well as with respect to the CIQ scores (no correlations between Pt-QOLIBRI and CIQ). However, partially divergent data emerged in another study by our group, which also demonstrates that patients with low self-awareness are able to self-report on their HRQoL (Formisano et al., submitted) and thus, as in previous studies [25], the proxy report need could be challenged.
Conversely, the high number of statistically significantly correlations found between Pro-QOLIBRIcaregiver-centered and both GOS-E and CIQ, demonstrates that the caregivers’ perception is different from that of the patients, that is, the worse the patients’ outcome severity, the worse the HRQoL of their caregivers, suggesting the usefulness of the Pro-QOLIBRIcaregiver-centered to evaluate the social impact of TBI on the whole family system.
This study also demonstrates that HRQoL, as assessed by the Proxy-QOLIBRI, is not only related to the disability severity of patients, but also to their social reintegration. Indeed, to our knowledge, this is the first study that correlates the quality of life of persons with TBI as self-perceived and as perceived by the caregiver, with social reintegration measured by a specific tool such as the CIQ.
The validation of the Proxy QOLIBRI sheds new light on the reduced ability of persons with TBI to perceive their social disability more than they perceive their subjective quality of life [1–3], as reported in the previous studies (Formisano et al., submitted).
In a recent study [26], a causal relationship is demonstrated between low self-awareness and perspective-taking difficulties in a population of persons who had suffered a TBI; Theory of Mind (ToM), and perspective-taking are also impaired in persons after TBI, even those with adequate levels of SA, with a statistically significant correlation between the ToM deficit and caregivers’ HRQoL [27].
As a self-awareness deficit may limit the reliability of persons with TBI, whereas differences between patients’ self-related HRQoL and caregivers’ perception may be influenced by the reliability of the caregivers’ judgment, it should be emphasized that the emotional distress of caregivers may also influence their judgment about the HRQoL of individuals with TBI [28–30]. Therefore, future studies should focus on the high burden of the family members of persons with TBI and the reliability of their perceived quality of life [31]. Further studies are also needed to confirm the usefulness of associating the Pro-QOLIBRI with the Pt-QOLIBRI in investigating the social disability, adjustment and reintegration of persons with TBI and their caregivers.
The usefulness of the Pro-QOLIBRI in clinical practice and in the development of more effective health and social networks for people with severe brain injury has to be emphasized.
Indeed, as it is well known, TBI is a family affair [32]; consistently, the present study suggests the usefulness of evaluating the caregivers’ quality of life in the clinical practice, by means of a specific tool such as Pro-QOLIBRI, to monitor their emotional distress related to the injury of the person they care of. Thus, Pro-QOLIBRI could allow the development of a structured psychologic support of the caregivers, as well as effective health and social networks for people with severe brain injury and their significant others [31].
References
von Steinbüchel N, Wilson L, Gibbons H et al (2010) Quality of Life after Brain Injury (QOLIBRI): scale development and metric properties. J Neurotrauma 27:1167–1185. doi:10.1089/neu.2009.1076
von Steinbüchel N, Wilson L, Gibbons H et al (2010) QOLIBRI task force. Quality of life after brain injury (QOLIBRI): scale validity and correlates of quality of life. J Neurotrauma 27:1157–1165. doi:10.1089/neu.2009.1077
Truelle JL, Koskinen S, Hawthorne G et al (2010) Qolibri Task Force. Quality of life after traumatic brain injury: the clinical use of the QOLIBRI, a novel disease-specific instrument. Brain Inj 24:1272–1291. doi:10.3109/02699052.2010.506865
von Steinbuechel N, Wilson L, Gibbons H et al (2012) QOLIBRI overall scale: a brief index of health-related quality of life after traumatic brain injury. J Neurol Neurosurg Psychiatry 83(11):1041–1047. doi:10.1136/jnnp-2012-302361
Muehlan H, Wilson L, von Steinbüchel N (2015) A rasch analysis of the QOLIBRI Six-Item Overall scale. Assessment 23(1):124–130. doi:10.1177/1073191115569844
Giustini M, Longo E, Azicnuda E et al (2014) Health-related quality of life after traumatic brain injury: Italian validation of the QOLIBRI. Funct Neurol 29:167–176
Ben-Yishay Y, Rattok J, Lakin P, Piasetsky EB, Ross B, Silver S et al (1985) Neuropsychological rehabilitation: Quest for a holistic approach. Semin Neurol 5:252–259
Prigatano GP, Fordyce DJ, Zeiner HK, Roueche JR, Pepping M, Wood BC (1986) Neuropsychological rehabilitation after brain injury. Johns Hopkins University Press, Baltimore
Sherer M, Hart T, Nick TG (2003) Measurement of impaired self-awareness after traumatic brain injury: a comparison of the patient competency rating scale and the awareness questionnaire. Brain Inj 17:25–37
Bivona U, Ciurli P, Barba C et al (2008) Executive function and metacognitive self-awareness after severe traumatic brain injury. J Int Neuropsychol Soc 14:862–868. doi:10.1017/S1355617708081125
Ciurli P, Bivona U, Barba C et al (2010) Metacognitive unawareness correlates with executive function impairment after severe traumatic brain injury. J Int Neuropsychol Soc 16(2):360–368. doi:10.1017/S135561770999141X
Keenan JP, Gallup GC, Falk D (2003) The face in the mirror: The search for the origins of consciousness. HarperCollins Publishers
Morin A (2006) Levels of consciousness and self-awareness: a comparison and integration of various neurocognitive views. Conscious Cogn 15(2):358–371. doi:10.1016/j.concog.2005.09.006
Kelley E, Sullivan C, Loughlin JK et al (2014) Self-awareness and neurobehavioral outcomes, 5 years or more after moderate to severe brain injury. J Head Trauma Rehabil 29(2):147–152
Sasse N, Gibbons H, Wilson L (2013) Self-awareness and health-related quality of life after traumatic brain injury. J Head Trauma Rehabil 28:464–472. doi:10.1097/HTR.0b013e318263977d
Teasdale G, & Jennett, B. Assessment of coma and impaired consciousness (1974) A practical scale. Lancet 13:81–84
World Health Organization (1992) International Statistical Classification of Diseases and Related Health Problems. tenth revision. Geneva, Switzerland
Wilson JT, Pettigrew LE, Teasdale GM (1998) Structured interviews for the Glasgow Outcome Scale and the extended Glasgow Outcome Scale: guidelines for their use. J Neurotrauma 15(8):573–585
Willer B, Rosenthal M, Kreutzer JS (1993) Assessment of community integration following rehabilitation for traumatic brain injury. J Head Trauma Rehabil. 8:75–87
Mokken RJ (1982) A non-parametric approach to the analysis of dichotomous item responses. Appl Psychol Meas 6:417–430
Cuzick J (1985) A Wilcoxon-type test for trend. Stat Med 4:87–90
Mellon S, Northouse LL, Weiss LK (2006) A population-based study of the quality of life of cancer survivors and their family caregivers. Cancer Nurs 29(2):120–131
Lulé D, Ehlich B, Lang D, Sorg S, Heimrath J, Kübler A, Ludolph AC (2013) Quality of life in fatal disease: the flawed judgement of the social environment. J Neurol 260(11):2836–2843. doi:10.1007/s00415-013-7068-y
Zucchella C, Bartolo M, Bernini S, Picascia M, Sinforiani E (2015) Quality of life in Alzheimer disease: a comparison of patients’ and caregivers’ points of view. Alzheimer Dis Assoc Disord 29(1):50–54. doi:10.1097/WAD.0000000000000050
Machamer J, Temkin N, Dikmen S (2013) Health-related quality of life in traumatic brain injury: is a proxy report necessary? J Neurotrauma 30(22):1845–1851. doi:10.1089/neu.2013.2920
Bivona U, Riccio A, Ciurli P et al (2014) Low Self-Awareness of Individuals With Severe Traumatic Brain Injury Can Lead to Reduced Ability to Take Another Person’s Perspective. J Head Trauma Rehabil. 29:157–171. doi:10.1097/HTR.0b013e3182864f0b
Bivona U, Formisano R, De Laurentiis S et al (2015) Theory of mind impairment after severe traumatic brain injury and its relationship with caregivers’ quality of life. Restor Neurol Neurosci 33(3):335–345. doi:10.3233/RNN-140484
Guevara AB, Demonet JF, Polejaeva E et al (2016) Association between traumatic brain injury-related brain lesions and long-term caregiver burden. J Head Trauma Rehabil 31(2):48–58. doi:10.1097/HTR.0000000000000151
Bodley-Scott SEM, Riley GA (2015) How partners experience personality change after traumatic brain injury—its impact on their emotions and their relationship. Brain Impairment (3):205–220
Tramonti F, Bonfiglio L, Di Bernardo C et al (2015) Family functioning in severe brain injuries: correlations with caregivers’ burden, perceived social support and quality of life. Psychol Health Med. 10:1–7. doi:10.1080/13548506.2015.1009380
Struchen MA, Pappadis MR, Sander AM, Burrows CS, Myszka KA (2011) Examining the contribution of social communication abilities and affective/behavioral functioning to social integration outcomes for adults with traumatic brain injury. J Head Trauma Rehabil. 26:30–42. doi:10.1097/HTR.0b013e3182048f7c
Lezak MD (1988) Brain damage is a family affair. J Clin Exp Neuropsychol 10:111–123. doi:10.1080/01688638808405098
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Statement of human and animal rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent of patients and their caregivers.
Rights and permissions
About this article

Cite this article
Formisano, R., Silvestro, D., Azicnuda, E. et al. Quality of life after brain injury (QOLIBRI): Italian validation of the proxy version. Intern Emerg Med 12, 187–198 (2017). https://doi.org/10.1007/s11739-016-1536-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11739-016-1536-1