
Abstract
The aim of the study was to evaluate the association between circulating (CPCs) and endothelial (EPCs) progenitor cells and left ventricular (LV) remodeling in chronic heart failure (HF). 85 HF patients, ranging 29–89 years, 83.5 % males, 45.9 % ischemic, NYHA functional class II–IV, with a LV ejection fraction ≤40 % were studied. LV ejection fraction, LV end-diastolic and end-systolic (LVESV) volumes, LV mass and tricuspid annular plane systolic excursion (TAPSE) were evaluated, and, when indicated, indexed for body surface area (BSA). CPCs and EPCs number was assessed using flow cytometry. CPCs were defined as CD34+, CD133+ and CD34+/CD133+. EPCs, identified through their expression of KDR, were defined as CD34+/KDR+, CD133+/KDR+ and CD34+/CD133+/KDR+. All EPCs were negatively related to LVESV/BSA (r = −0.24, p = 0.02 for all EPC’s populations), and to LVmass/BSA (CD34+KDR+; r = −0.30, p = 0.005; CD133+KDR+; r = −0.31, p = 0.004; CD34+CD133+KDR+; r = −0.29, p = 0.007). No differences in EPCs levels in relation to cardiovascular risk factors, medications, etiology, age or gender were observed. CPCs number was higher in women, and lower in ischemic patients. In logistic regression analyses, the low EPCs’ number was associated with an increased likelihood of abnormal LVmass/BSA. CPCs proved to be higher and EPCs lower in patients with severely abnormal LVmass/BSA (gr/m2, ≥122 in women and ≥149 in men). Our results suggest a correlation between LV remodeling and progenitor cells. This is noteworthy considering that it has been suggested that bone marrow-derived EPCs participate in cardiac regeneration and function recovery in the setting of progressive HF.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
It has been reported that persistent mobilization of bone marrow progenitor cells correlates with favorable left ventricular (LV) remodeling, as evidenced by prevention of LV dilatation and enhanced contractile recovery in patients with acute myocardial infarction [1, 2]. However, data on the association between mobilization of progenitor cells and LV remodeling in chronic heart failure (HF) patients are few. Among the scant data about this issue, it has been previously suggested that bone marrow-derived endothelial progenitor cells participate in cardiac regeneration and function recovery in the setting of progressive HF [3, 4]. The aim of the present study was to better analyze the relationship between blood levels of progenitor cells and LV remodeling in HF patients. For this purpose, we estimated both endothelial (EPCs) and circulating (CPCs) progenitor cells. From a biological point of view, EPCs and CPCs likely represent different progenitor cell phenotypes with different biological properties. The EPCs circulating pool represents a population of more mature cells that are just “committed” to differentiate into endothelial cells, able to participate mainly in the processes of re-endothelialization and revascularization. CPCs represent a more heterogeneous and undifferentiated cell population, able to evolve in different cell types.
Materials and methods
Study population
Our population consisted of 85 consecutive chronic HF out-patients, referred to our Heart Failure service in the period 2008–2011. All participants gave informed written consent, and the study protocol was approved by the local ethics committee. All clinical data, echocardiographic evaluation and blood sample collection were performed for each patient on the day of recruitment visit. The median age was 67 years (range 29–89); 71 (83.5 %) patients were men. The New York Heart Association (NYHA) functional class was II–IV. All participants had a LV ejection fraction (LVEF) ≤40 %. The median QRS duration was 140 ms (range 80–200 ms). Fifty-seven out of 85 patients (67.1 %) showed narrow QRS (≤120 ms), remaining patients had a QRS >120 ms, and a left bundle branch block morphology. The QRS duration was measured from the surface ECG using the widest QRS complex. The QRS duration was scored by two independent observers who were blinded to all other patient data. All patients had to be clinically stable for a period of at least 3 months preceding the enrollment. All patients presented in a normal sinus rhythm. HF etiology was ischemic in 39 patients (45.9 %) and non-ischemic in 46 patients (54.1 %). Forty-eight patients (56.5 %) were hypertensive, 34 (40 %) dyslipidemic, 16 (18.8 %) diabetic and 47 (55.3 %) were smokers.
Echocardiographic protocol
Echocardiographic studies were performed using a high-quality echocardiograph (Vivid 9, GE, USA) equipped with a 5S probe. All measurements were performed by the same expert cardiologist according to the American Society of Echocardiography recommendations, [5] and parameters, when necessary, were indexed by body surface area (BSA). The following echo M-mode, bi-dimensional and pulsed Doppler parameters were evaluated: LV end-diastolic and end-systolic volumes (LVEDV and LVESV, respectively); LVEF estimated with the biplane Simpson’s method. Tricuspid annular plane systolic excursion (TAPSE) was estimated by two-dimensional echo-guided M-mode recordings from the apical 4-chamber view, the cursor placed at the free wall side of the tricuspid annulus. Relative wall thickness was defined as (posterior wall thickness + interventricular septal wall thickness)/internal diameter, and LV mass was calculated according to the formula of Devereux [6–8]. Concentricity was defined as LV mass divided by LVEDV. LVmass/BSA (gr/m2) was considered severely abnormal when, as previously indicated, [7] its value was ≥122 in women and ≥149 in men.
Flow cytometric analysis of CPCs and EPCs
CPCs and EPCs’ number was assessed contemporarily using flow cytometry, as previously described [9, 10]. Briefly, 200 μl of peripheral venous blood was incubated for 20 min in the dark with:
-
fluorescein isothiocyanate (FITC)-labeled monoclonal antibodies against human CD34 (BD Pharmingen, San Diego, California, USA);
-
allophycocyanin (APC)-labeled monoclonal antibodies against human AC133 (Miltenyi Biotec, Bergisch Gladbach, Germany);
-
Phycoerythrin (PE)-labeled monoclonal antibodies against human VEGFR2-KDR (R&D Systems Inc, Minneapolis, USA);
-
allophycocyanin-cyanine7 (APC-Cy7)-labeled monoclonal antibodies against human CD45 (Becton–Dickinson, San Jose, USA); and
-
LDS751, a nucleic acid dye (Molecular Probes, Invitrogen, Eugene, Oregon, USA).
Mouse isotype-identical antibodies served as controls (Becton–Dickinson, San Jose, CA, USA). Red blood cells and platelets were subsequently lysed by NH4Cl lysing solution (Autolyse solution; BioSource International, Camarillo, USA). For analysis, 300,000 cells within the leukocyte gate were acquired using a FACSCanto analyzer (Becton–Dickinson, San Jose, USA), and data were processed using BD FacsDiva software. Circulating EPCs were identified through their expression of CD34, KDR, and CD133, and were considered as endothelial progenitor cells CD34+/KDR+, CD133+/KDR+ and CD34+/CD133+/KDR+.
Using a modification of the International Society of Hematotherapy and Graft Engineering (ISHAGE) guidelines, [11] CPCs were defined as cells forming a cluster with low side scatter and low-to-intermediated CD45 staining and positive for CD34+, CD133+ and CD34+/CD133+.
NT-proBNP determination
NT-proBNP was measured with a chemiluminescent immunoassay kit (Roche Diagnostic Laboratory, Indianapolis, IN, USA) on an Elecsys 2010 analyzer.
Statistical analysis
Statistical analysis was performed using the SPSS (Statistical Package for Social Sciences, Chicago, IL, USA) software for Windows (Version 18.0). Values are presented as median and range or by mean and standard deviation as appropriate. The Chi square test was used to identify statistically significant differences between categorical variables. The Mann–Whitney test for unpaired data was used for comparisons between groups. The Spearman’s test was used to identify significant correlations between numerical variables. A multiple logistic regression analysis was used to test the independent association between EPCs number and the likelihood of an abnormal LVmass/BSA. All odds ratios (OR) are given with their 95 % confidence interval.
Results
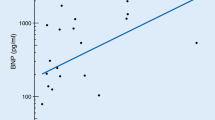
Demographic and clinical characteristics of the study population are reported in Table 1. All EPC’s populations were negatively and significantly related with LVESV/BSA (r = −0.24, p = 0.02 for all EPC’s populations), and a tendency towards significance was observed for LVEDV/BSA (r = −0.19, p = 0.08 all EPC’s populations). Moreover all EPCs’ populations were negatively and significantly related to LVmass/BSA (CD34+KDR+; r = −0.30, p = 0.005; CD133+KDR+; r = −0.31, p = 0.004; CD34+CD133+KDR+; r = −0.29, p = 0.007). In a logistic regression analysis, the low EPCs’ number was associated with an increased likelihood of abnormal LVmass/BSA, even after adjusting for age, gender, cardiovascular risk factors and statin use [OR 95 % CI CD34+KDR+ 1.12 (1.02–1.22), p = 0.01; CD133+ KDR+ 1.13 (1.03–1.25), p = 0.01; CD34+CD133+KDR+ 1.14 (1.03–1.27), p = 0.01]. No significant correlations were observed between CPCs and echocardiographic parameters. To further analyze the behavior of progenitor cells, we compared patients with or without severely abnormal LVmass/BSA (≥122 gr/m2 in women and ≥149 gr/m2 in men). CPCs proved to be significantly higher and EPCs significantly lower in patients with severely abnormal LVmass/BSA (Table 2). There was no significant correlation between EPCs and CPCs levels. According to left ventricular mass/BSA cutoff, significant differences in LVESV/BSA, LVEDV/BSA, concentricity and ischemic etiology were detected (Table 3), while age, gender, NYHA class and ejection fraction did not differ between patients with and without severely abnormal LVmass/BSA. Evaluating cardiovascular risk factors and therapies, a significantly higher proportion of diabetic patients and of statin use was observed in patients without severely abnormal LVmass/BSA with respect to patients with an abnormal LVmass/BSA [diabetes: 10/26 (38.5 %) vs. 6/59 (10.2 %), p = 0.002; statin use 16/26 (61.5 %) vs. 23/59 (38.9 %), p = 0.04.] No significant differences of EPC levels in relation to cardiovascular risk factors, medications, etiology, age or gender were observed (data not shown). On the contrary, CPCs’ number was significantly higher in women with respect to men [CD34+ 288 (150–693) vs. 230 (47–1129) cells/106 events, p = 0.04; CD34+/CD133+ 267 (150–690) vs. 207 (47–1139) cells/106 events, p = 0.02; CD133+ 267 (150–690) vs. 207 (47–1129) cells/106 events, p = 0.02] and significantly lower in patients with an ischemic etiology [CD34+ 182 (80–497) vs. 258 (47–743) cells/106 events, p = 0.04; CD34+/CD133+ 173 (57–493) vs. 233 (47–690) cells/106 events, p = 0.05; CD133+ 173(57–497) vs. 240 (47–690) cells/106 events, p = 0.04]. In addition, a significant and negative correlation between CPCs’ number and age was observed (r = −0.23, p = 0.03 for all CPC’s populations). NT-ProBNP levels were significantly and positively related with age (r = 0.25, p = 0.02), and, albeit not significantly, inversely related with CD34+KDR+ EPCs (r = −0.19, p = 0.07).
Discussion
This study evaluated the relationship between the degree of ventricular remodeling and blood levels of progenitor cells, measuring both EPCs and CPCs, in chronic HF patients. All EPCs populations were negatively related to LVESV/BSA and LVmass/BSA, and the presence of a lower number of EPCs was associated with an increased likelihood of abnormal LV mass/BSA. These data suggest a correlation between higher number of circulating EPCs and a less severe pathological state, with more preserved LV function and a lower degree of ventricular remodeling. A possible explanation for these findings, specifically for the relationship between LVESV/BSA or LVmass/BSA and EPCs, can be inferred from the role of afterload in determining ventricular end-systolic volume [12], with increased afterload inducing pathological cardiac hypertrophy [13]. A possible role of afterload in influencing progenitor cells might be considered.
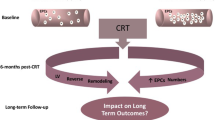
We then evaluated the correlation between LV mass and progenitor cells, dividing patients according to a pre-established cutoff for indexed LV mass, indicating the presence or absence of severely abnormal values [7]. All CPCs populations proved to be higher, and all EPCs lower, in patients with severely abnormal LVmass/BSA. The existence of a relationship between LV mass and progenitor cells is noteworthy, considering that LV hypertrophy is a frequent consequence of hypertension, and is thought to be involved in the subsequent occurrence of congestive heart failure [14, 15]. A relationship between EPCs and LV remodeling had been previously reported only in patients with acute myocardial infarction, and never in chronic HF patients. Previous clinical studies [1, 2] show a reduced mobilization of progenitor cells in the acute phase of myocardial infarction as well as its recovery over 1-year follow-up; a greater reduction of mobilization is associated with more significant impairment of LVEF and greater infarct size. The only study pertinent to our results was performed in 22 chronic HF patients scheduled for cardiac resynchronization therapy [16]. In this study, no relationship between progenitor cells and LV remodeling was observed; however, it was conducted measuring only CPCs, and not EPCs. Two studies [17, 18] reported a reduced number of EPCs in hypertensive patients, but both were conducted without evaluating LV mass and analyzing the presence of hypertrophy only by electrocardiography, whose sensitivity in detecting the presence of cardiac hypertrophy is only 6 to 20 % [19, 20]. In both the cases, the populations under study did not include HF patients. To interpret the different behavior of CPCs and EPCs in relation to left ventricular mass, we should consider that CPCs and EPCs represent different progenitor cells phenotypes with probably a different biological meaning. The CPCs’ population contains stem cells of various lineages, and is a reservoir of haematopoietic, endothelial, neurological and cardiac cells. This “multipotency” of CPCs with respect to EPCs, (which are just committed to the endothelial lineage), and the capacity to shift into a particular type of cells in relation to the stimulus, can explain the differences between the two types of cells. The absence of a correlation between the two types of cells, shown in the results, might suggest an independent role for these cells populations, further supporting their different behavior. In recent years, it has been shown that the most important mechanism by which progenitor cells promote angiogenesis and vasculogenesis is their paracrine function [21, 22]. As progenitor cells become committed to the endothelial lineage, they lose CD133 and acquire KDR; this transition is associated with phenotypic properties more closely related to a mature endothelium, with a possibly different paracrine activity [23]. EPCs possess more pronounced angiogenic properties than CPCs [23], thus a low number of EPCs may be associated with a compromised ability to form new blood vessels, and ability to restore endothelial integrity by vasculogenesis. In this regard, a previous experimental study demonstrates that neoangiogenesis by EPCs prevents apoptosis of hypertrophied myocardium, reduces progressive collagen deposition and scar formation, and improves ventricular function [24]. It might be suggested that patients with reduced EPCs and greater LV mass/BSA may have had a different equilibrium between CPCs and EPCs leading to a worse LV remodeling. Finally, the influence of a technical issue on the different behavior of CPCs and EPCs cannot be excluded. In fact it should be considered that EPCs are very rare in the circulation, and thus CPCs can be more accurately measured due to a higher number with respect to EPCs.
Once patients were divided according to the LV mass/BSA pre-established cutoff, we did not find any difference in relation to patients’ ages. This finding is noteworthy, considering that in keeping with earlier studies [25–27], an inverse relationship between CPCs levels and age was evidenced in our study. The evidence suggests that progenitor cells are subject to age-associated changes, with an impairment of their function at older ages, and these changes may be involved in the dysregulation of endogenous cardiovascular repair mechanisms in the aging heart [28]. CPCs number proved to be significantly higher in women. This had already been observed in the past, and was mainly attributed to sex steroids [29–31]. We found, as previously suggested [32], the existence of a reduced number of CPCs in patients with ischemic heart disease. We cannot analyze in detail the role of therapy, even if a significant higher proportion of statin use was observed in patients without severely abnormal LVmass/BSA. This observation is in accordance with previous findings, concerning the role of statins in increasing the number of progenitor cells [33, 34]. Our results should be taken into account in the light of previous experimental results concerning the capability of bone marrow-derived cells to differentiate in vivo into cells expressing the properties of heart cells, possibly able to help in reconstituting the damaged myocardium. Moreover, it should be considered that previous studies [35, 36], indicate a role for bone marrow-derived progenitor cells in determining a favorable or unfavorable LV remodeling in patients with congestive HF. It is not possible to evaluate, on the basis of our results, the existence of a causal relationship between progenitor cells levels and ventricular remodeling. Nevertheless, it is a matter of fact that the behavior of ventricular remodeling parallels the behavior of progenitor cells, at least in the chronic HF patient population under study. If these results are confirmed by subsequent and more extensive investigations, the evaluation of progenitor cells, together with standard echocardiographic data, and possibly other non-invasive indicators of endothelial function (endothelium-dependent flow-mediated vasodilation (FMD)) could help in the initial evaluation of patients presenting with chronic heart failure, and might be useful in predicting the probability of response to heart failure therapy (e.g. cardiac resynchronization therapy).
References
Leone AM, Rutella S, Bonanno G, Contemi AM, de Ritis DG, Giannico MB, Rebuzzi AG, Leone G, Crea F (2006) Endogenous G-CSF and CD34+ cell mobilization after acute myocardial infarction. Int J Cardiol 111(2):202–208. doi:10.1016/j.ijcard.2005.06.043
Wyderka R, Wojakowski W, Jadczyk T, Maślankiewicz K, Parma Z, Pawłowski T, Musiałek P, Majka M, Król M, Kuczmik W, Dworowy S, Korzeniowska B, Ratajczak MZ, Tendera M (2012) Mobilization of CD34+CXCR4+ stem/progenitor cells and the parameters of left ventricular function and remodeling in 1-year follow-up of patients with acute myocardial infarction. Mediat Inflamm 2012:564027. doi:10.1155/2012/564027
Maltais S, Perrault LP, Ly HQ (2011) The bone marrow-cardiac axis: role of endothelial progenitor cells in heart failure. Eur J Cardiothorac Surg 39(3):368–374. doi:10.1016/j.ejcts.2010.04.022
Kucia M, Dawn B, Hunt G, Guo Y, Wysoczynski M, Majka M, Ratajczak J, Rezzoug F, Ildstad ST, Bolli R, Ratajczak MZ (2004) Cells expressing early cardiac markers reside in the bone marrow and are mobilized into the peripheral blood after myocardial infarction. Circ Res 10 95(12):1191–1199. doi:10.1161/01.RES.0000150856.47324.5b
Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, Picard MH, Roman MJ, Seward J, Shanewise J, Solomon S, Spencer KT, St John Sutton M, Stewart W; American Society of Echocardiography’s Nomenclature and Standards Committee; Task Force on Chamber Quantification; American College of Cardiology Echocardiography Committee; American Heart Association; European Association of Echocardiography, European Society of Cardiology (2006) Recommendations for chamber quantification. Eur J Echocardiogr 7(2):79–108. doi:10.1016/j.euje.2005.12.014
Devereux RB, Alonso DR, Lutas EM, Gottlieb GJ, Campo E, Sachs I, Reichek N (1986) Echocardiographic assessment of left ventricular hypertrophy: comparison to necropsy findings. Am J Cardiol 57:450–458. doi:10.1016/0002-9149(86)90771-X
Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, Picard MH, Roman MJ, Seward J, Shanewise JS, Solomon SD, Spencer KT, Sutton MS, Stewart WJ, Chamber Quantification Writing Group, American Society of Echocardiography’s Guidelines and Standards Committee, European Association of Echocardiography (2005) J Am Soc Echocardiogr 18:1440–1463. doi:10.1016/j.echo.2005.10.005
Devereux RB, Pini R, Aurigemma GP, Roman MJ (1997) Measurement of left ventricular mass: methodology and expertise. J Hypertens 15(8):801–809
Cesari F, Caporale R, Marcucci R, Caciolli S, Stefano PL, Capalbo A, Macchi C, Vannucci M, Gensini GF, Abbate R, Gori AM (2008) NT-proBNP and the anti-inflammatory cytokines are correlated with endothelial progenitor cells’ response to cardiac surgery. Atherosclerosis 199:138–146. doi:10.1016/j.atherosclerosis.2007.09.045
Cesari F, Sofi F, Caporale R, Capalbo A, Marcucci R, Macchi C, Lova RM, Cellai T, Vannucci M, Gensini GF, Abbate R, Gori AM (2009) Relationship between exercise capacity, endothelial progenitor cells and cytochemokines in patients undergoing cardiac rehabilitation. Thromb Haemost 101:521–526. doi:10.1160/TH08-10-0644
Sutherland DR, Anderson L, Keeney M, Nayar R, Chin-Yee I (1996) The ISHAGE guidelines for CD34+ cell determination by flow cytometry. International Society of Hematotherapy and Graft Engineering. J Hematother 5:213–226
Carroll JD, Hess OM (2005) Assessment of normal and abnormal cardiac function. In: Zipes DP, Libbey P, Bonow RO, Braunwald E et al. (eds) Braunwald's heart disease: a textbook of cardiovascular medicine (7th edition). Elsevier Saunders, Philadelphia, pp 491–507
Hirt MN, Sörensen NA, Bartholdt LM, Boeddinghaus J, Schaaf S, Eder A, Vollert I, Stöhr A, Schulze T, Witten A, Stoll M, Hansen A, Eschenhagen T (2012) Increased afterload induces pathological cardiac hypertrophy: a new in vitro model. Basic Res Cardiol 107(6):307. doi:10.1007/s00395-012-0307-z
McKee PA, Castelli WP, McNamara PM, Kannel WB (1971) The natural history of congestive heart failure: the Framingham study. N Engl J Med 285(26):1441–1446. doi:10.1161/CIRCULATIONAHA.108.815944
Lee DS, Gona P, Vasan RS, Larson MG, Benjamin EJ, Wang TJ, Tu JV, Levy D (2009) Relation of disease pathogenesis and risk factors to heart failure with preserved or reduced ejection fraction: insights from the framingham heart study of the national heart, lung, and blood institute. Circulation 119(24):3070–3077
Goette A, Jentsch-Ullrich K, Hammwöhner M, Trautmann S, Franke A, Klein HU, Auricchio A (2006) Cardiac uptake of progenitor cells in patients with moderate-to-severe left ventricular failure scheduled for cardiac resynchronization therapy. Europace 8(3):157–160. doi:10.1093/europace/euj042
Lee CW, Huang PH, Huang SS, Leu HB, Huang CC, Wu TC, Chen JW, Lin SJ (2011) Decreased circulating endothelial progenitor cell levels and function in essential hypertensive patients with electrocardiographic left ventricular hypertrophy. Hypertens Res 34(9):999–1003. doi:10.1038/hr.2011.68
Huang PH, Huang SS, Chen YH, Lin CP, Chiang KH, Chen JS, Tsai HY, Lin FY, Chen JW, Lin SJ (2010) Increased circulating CD31+/annexin V+ apoptotic microparticles and decreased circulating endothelial progenitor cell levels in hypertensive patients with microalbuminuria. J Hypertens 28(8):1655–1665. doi:10.1097/HJH.0b013e32833a4d0a
Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP (1990) Prognostic implications of echocardiographically determined left ventricular mass in the Framingham Heart Study. N Engl J Med 322(22):1561–1566. doi:10.1056/NEJM199005313222203
Levy D, Labib SB, Anderson KM, Christiansen JC, Kannel WB, Castelli WP (1990) Determinants of sensitivity and specificity of electrocardiographic criteria for left ventricular hypertrophy. Circulation 81(3):815–820. doi:10.1161/01.CIR.81.3.815
Xu S, Zhu J, Yu L, Fu G (2012) Endothelial progenitor cells: current development of their paracrine factors in cardiovascular therapy. J Cardiovasc Pharmacol 59(4):387–396. doi:10.1097/FJC.0b013e3182440338
Drawnel FM, Archer CR, Roderick HL (2013) The role of the paracrine/autocrine mediator endothelin-1 in regulation of cardiac contractility and growth. Br J Pharmacol 168(2):296–317. doi:10.1111/j.1476-5381.2012.02195.x
Friedrich EB, Walenta K, Scharlau J, Nickenig G, Werner N (2006) CD34-/CD133+/VEGFR-2+ endothelial progenitor cell subpopulation with potent vasoregenerative capacities. Circ Res 98(3):e20–e25. doi:10.1161/01.RES.0000205765.28940.93
Kocher AA, Schuster MD, Szabolcs MJ, Takuma S, Burkhoff D, Wang J, Homma S, Edwards NM, Itescu S (2001) Neovascularization of ischemic myocardium by human bone-marrow-derived angioblasts prevents cardiomyocyte apoptosis, reduces remodeling and improves cardiac function. Nat Med 7(4):430–436. doi:10.1038/86498
Cohen KS, Cheng S, Larson MG, Cupples LA, McCabe EL, Wang YA, Ngwa JS, Martin RP, Klein RJ, Hashmi B, Ge Y, O’Donnell CJ, Vasan RS, Shaw SY, Wang TJ (2013) Circulating CD34(+) progenitor cell frequency is associated with clinical and genetic factors. Blood 121(8):e50–e56. doi:10.1182/blood-2012-05-424846
Taguchi A, Matsuyama T, Moriwaki H, Hayashi T, Hayashida K, Nagatsuka K, Todo K, Mori K, Stern DM, Soma T, Naritomi H (2004) Circulating CD34-positive cells provide an index of cerebrovascular function. Circulation 109(24):2972–2975. doi:10.1182/blood-2012-05-424846
Cesari F, Nencini P, Nesi M, Caporale R, Giusti B, Abbate R, Gori AM, Inzitari D (2009) Bone marrow-derived progenitor cells in the early phase of ischemic stroke: relation with stroke severity and discharge outcome. J Cereb Blood Flow Metab 29(12):1983–1990. doi:10.1016/j.ejcts.2010.01.046
Ballard VL, Edelberg JM (2007) Stem cells and the regeneration of the aging cardiovascular system. Circ Res 27 100(8):1116–1127. doi:10.1161/01.RES.0000261964.19115.e3
Herrmann JL, Abarbanell AM, Weil BR, Manukyan MC, Poynter JA, Wang Y, Coffey AC, Meldrum DR (2010) Gender dimorphisms in progenitor and stem cell function in cardiovascular disease. J Cardiovasc Transl Res 3(2):103–113. doi:10.1007/s12265-009-9149-y
Cohen KS, Cheng S, Larson MG, Cupples LA, McCabe EL, Wang YA, Ngwa JS, Martin RP, Klein RJ, Hashmi B, Ge Y, O’Donnell CJ, Vasan RS, Shaw SY, Wang TJ (2013) Circulating CD34(+) progenitor cell frequency is associated with clinical and genetic factors. Blood 121(8):e50–e56. doi:10.1182/blood-2012-05-424846
Fadini GP, de Kreutzenberg S, Albiero M, Coracina A, Pagnin E, Baesso I, Cignarella A, Bolego C, Plebani M, Nardelli GB, Sartore S, Agostini C, Avogaro A (2008) Gender differences in endothelial progenitor cells and cardiovascular risk profile: the role of female estrogens. Arterioscler Thromb Vasc Biol 28(5):997–1004. doi:10.1161/ATVBAHA.107.159558
Theiss HD, David R, Engelmann MG, Barth A, Schotten K, Naebauer M, Reichart B, Steinbeck G, Franz WM (2007) Circulation of CD34+ progenitor cell populations in patients with idiopathic dilated and ischaemic cardiomyopathy (DCM and ICM). Eur Heart J 28(10):1258–1264. doi:10.1093/eurheartj/ehm011
Vasa M, Fichtlscherer S, Adler K, Aicher A, Martin H, Zeiher AM, Dimmeler S (2001) Increase in circulating endothelial progenitor cells by statin therapy in patients with stable coronary artery disease. Circulation 103(24):2885–2890. doi:10.1161/hc2401.092816
Xu H, Yang YJ, Yang T, Qian HY (2013) Statins and stem cell modulation. Ageing Res Rev 12(1):1–7. doi:10.1016/j.arr.2012.03.006
Kissel CK, Lehmann R, Assmus B, Aicher A, Honold J, Fischer-Rasokat U, Heeschen C, Spyridopoulos I, Dimmeler S, Zeiher AM (2007) Selective functional exhaustion of hematopoietic progenitor cells in the bone marrow of patients with postinfarction heart failure. J Am Coll Cardiol 49(24):2341–2349. doi:10.1016/j.jacc.2007.01.095
Barsotti MC, Santoni T, Picoi ME, Mancini N, Massaro F, Grigoratos C, Bortolotti U, Collecchi P, Menicagli M, Scatena C, Felice F, Bevilacqua G, Naccarato AG, Di Stefano R, Balbarini A (2014) Endothelial progenitor cell homing in human myocardium in patients with coronary artery disease. Int J Cardiol 172(2):516–517. doi:10.1016/j.ijcard.2014.01.042
Acknowledgments
All participants gave informed written consent, and the study protocol was approved by the local ethics committee.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Michelucci, A., Cesari, F., Ricciardi, G. et al. Left ventricular mass and progenitor cells in chronic heart failure patients. Intern Emerg Med 10, 329–335 (2015). https://doi.org/10.1007/s11739-014-1149-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11739-014-1149-5