
Abstract
The suspension of use of sub-urethral mesh in the UK in 2018 has seen the resurgence of colposuspension in female SUI surgery. Open and laparoscopic colposuspension techniques are well recognised. We present data from 28 robotic-assisted laparoscopic colposuspension (RALCp) procedures, reporting on technique, safety and efficacy. Approval was obtained from the hospital New and Novel Procedures Committee. All patients had urodynamic assessment prior to surgery. Data was prospectively gathered and 24-h pad usage and Urinary Incontinence Short Form Questionnaire (ICIQ-UI-SF) scores were used to assess symptom severity and quality of life. PGII scores were used to assess patient satisfaction after the procedure. Paired T test analysis was conducted. Since May 2019, robotic colposuspension has been performed in 28 patients. The mean age and BMI were 49 and 27 (kg/m2), respectively, with a mean follow-up period of 12 months. 67.9% of patients had pure urodynamic SUI and 32.1% of patients had previous anti-SUI surgery. Average operating time was 127 min, blood loss 20 ml and length of stay 2 days. There was a significant 73% improvement in mean 24-h pad usage (p = 0.001) and an improvement in mean ICIQ-UI-SF scores from 18.1 to 9.4 (p = 0.0001). Day 1 mean pain score was 5/10. This is the largest series of its kind. Robotic colposuspension is safe and feasible with significant improvements seen in quality of life scores and number of pads used per day. It presents a minimally invasive treatment option in female SUI, however needs larger volume evaluation and longer follow-up for further evaluation.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Urinary incontinence is common, debilitating and often underreported. Its prevalence in adult women is reported in the range of 10–40%, and can be severe in up to 17% [1]. Stress urinary incontinence (SUI) relates to the symptom of involuntary loss of urine secondary to raised intra-abdominal pressure (coughing, sneezing, straining), whilst urodynamic SUI is the involuntary loss of urine during the filling phase of cystometry with raised intraabdominal pressure and in the absence of a detrusor contraction [2].
Following its introduction in 1996 [3], the tension-free vaginal tape succeeded Burch colposuspension by 2001 as the most frequently performed procedure for SUI in the UK [4]. At the time it was felt to be simple, cost-effective, consist of a short learning curve and minimally invasive. Studies at the time demonstrated equivalent functional outcomes to Burch colposuspension, with a decreased risk of prolapse at 2–5 years follow-up, traded off by an increased risk of intra-operative bladder injury [4, 5]. The popularity of mid-urethral synthetic tapes was sustained with UK Hospital Episodes Statistics (HES) data analysis between 2000 and 2012, suggesting they had become standard of care. However, there was a noted increase in tape-related complications and an increase in procedures to remove synthetic tapes [6].
Over the last decade, the controversy surrounding the long-term complications of mesh surgery had resulted in significant medical and legal implications for both health boards and the manufacturers of mesh. In 2018, NHS England halted the use of vaginal mesh surgery on the NHS, and in 2019 the FDA banned the use of MESH in pelvic organ prolapse surgery [7]. The suspension of sub-urethral mesh has seen the resurgence of urethral bulking, autologous rectus fascial sling and the Burch colposuspension in female SUI surgery as the remaining first-line alternatives ahead of the artificial urinary sphincter.
Surgical management is considered standard of care for women who have failed conservative management. Historically, open retropubic colposuspension had been considered an effective management of SUI [8], and the traditional Burch colposuspension procedure involved elevating the anterior and paravaginal tissue towards the pectineal ligament on the pelvic sidewall using two to four sutures on each side. 5-year data from long-term follow-up studies have reported cure rates of 63–81% using this technique and equivalence to TVT [9]. A more recent systematic review had shown a slightly higher cure with the synthetic MUS over colposuspension, at a trade-off for higher complications and voiding urinary symptoms [10].
Urology has been an early adopter of minimally invasive surgery (MIS). Open surgery has given way to minimally invasive surgery; ranging through endoscopic techniques, laparoscopy and robotic-assisted laparoscopic surgery. The benefits of MIS over open surgery are well established ranging from less blood loss, shorter length of stay, reduced pain scores and faster recovery [11]. Laparoscopic colposuspension was increasingly described as an established MIS technique in centres with expertise for female SUI and was considered more cost-effective than the open approach [12]. Furthermore, some proponents described single-port laparoscopic Burch colposuspension; however, this has not become popularised [13]. However, working in the confined space of the pelvis results in a more technically demanding procedure, coupled with other disadvantages of laparoscopy such as the amplification of tremor, limited range of movement, two dimensional vision impairing accurate depth perception and steep learning curve. The 10–15x magnification, three-dimensional vision, absence of tremor and versatile instruments with significantly increased range and plane of movement confers a significant advantage for robotic surgery over laparoscopy [11]. Robotic surgery within urology has now become widely adopted for both oncological pelvic, renal, reconstructive and transplant urology that the transition to female urology is becoming popular [14,15,16,17].
We present data from 28 robotic colposuspension procedures, reporting on technique, early safety, and short-term outcomes.
Patients and methods
An application for the development of the Robotic colposuspension programme was placed through the New and Novel procedures committee of the Hospital for approval, and written informed consent was obtained from patients. The surgical team establishing this procedure included members with a high volume of open and robotic pelvic surgery expertise combined. Since May 2019, 28 robot-assisted colposuspension procedures for SUI were performed, and data collated in a prospective database. All patients underwent pre-operative urodynamic assessment, pad usage assessment and had to complete the PGII, ICIQ-UI-SF, and ICIQ-OAB questionnaire as standard.
Patient demographics including age, BMI, ASA grade were recorded and analysed. Pad usage and ICIQ-UI-SF were used to characterise degree of SUI and bother caused. Intra-operative data including operative time, estimated blood loss (EBL) and complication. All patients received a specialist nurse review at 1-week post-discharge, and were required to complete a postop questionnaire at their clinic visits to assess functional outcome. Post-operative catheter was removed within the first 5 days of the procedure by a nurse specialist in an outpatient setting. Paired T test analysis for pad usage and ICIQ-UI-SF was conducted using SPSS v23.
Technique
Robotic colposuspension was performed via a trans-peritoneal 4 port approach (Fig. 1) using the da Vinci Si Surgical System (Intuitive Surgical, Sunnyvale, CA, USA).

Standard port positions for robotic-assisted Burch colposuspension (RALCp)
The patient was placed in a 25o Trendelenburg tilt. In this trans-peritoneal approach, a pneumoperitoneum was obtained using a supraumbilical open/Hasan technique. Along with the 12-mm camera port, two 8-mm robotic ports were inserted under vision approximately 8 cm inferolateral to the umbilical port, and a 5-mm assistant port was inserted 5 cm superior to the left anterior superior iliac spine. The robot docked, and only two robotic arms were utilised. The initial dissection was carried out using the robotic bipolar forceps and scissors.
The bladder was dropped from the anterior abdominal wall and the symphysis pubis identified (Fig. 2). The Retzius space was dissected and the paravesical/paravaginal tissue, urethrovesical angle and lateral bladder contour were identified. Coopers ligament was then identified (Fig. 3) and cleared along the superior aspect of the pubic ramus. A foley catheter helped delineate the bladder neck and assistant Hegar dilators inserted in the vagina helped to delineate the vagina and stay lateral to the urethra. Endowrist robot needle drivers were then used to place 0 Ethibond sutures through the paravaginal tissue lateral to the mid-urethra and bladder neck, the obturator shelf and Cooper’s ligament (Fig. 4). The sutures were tied intracorporeally as the assistant elevated the ipsilateral vaginal fornix to prevent excessive tension. Three sutures were placed on each side (Fig. 5), and following the procedure a vaginal examination was carried out to ensure no vaginal stitches present. A cystoscopic assessment was performed to ensure no sutures had been passed into the bladder. No drain was left.

Identification of pubic symphysis

Identification of Cooper's ligament

Paravaginal tissue stitched to Cooper's ligament

Position of sutures on one side
Post-operatively the patients are placed on an enhanced recovery pathway. They are sat out on day 0 and encouraged to mobilise by day 1. A normal oral diet is encouraged as tolerated. Patients are trialled without catheter once mobile, and aimed to be discharged at day 1 or 2.
Results
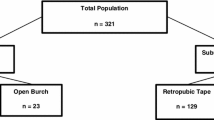
At the time of the study, 28 patients had undergone RALCp. The cohort’s mean age was 49 years. They had a mean BMI 27kg/m2 and a median American Society of Anaesthesiologists (ASA) score of 2. The mean follow-up period was 12 months (range 1–21 months). All patients underwent urodynamic assessment prior to surgery. Four patients (14%) had a history of a neurological condition; two with multiple sclerosis, and two with spinal bifida. The mean number of 24-h pads pre-operatively was 4.9 (range 2–16). Pure SUI was seen in 19 (67.9%), with mixed incontinence and concomitant detrusor overactivity accounting for the remaining 9 patients. All patients with mixed urinary incontinence had historically received intravesical Botulinum toxin A for the overactive bladder component. Ten (35.7%) patients had previously had anti-SUI procedures with urethral bulking (n = 9), one of whom also had a previous TVT that had failed to confer sustained symptomatic relief.
The transperitoneal approach accounted for 80% of the procedures. An extraperitoneal approach was utilised in patients with ‘virgin’ lower abdomens. Mean total operative time was 126 min, with 20ml blood loss. The mean length of stay was 2 days.
Overall, there was a 73% improvement in mean daily pad usage from 4.9 pre-operatively to 1.3 post-operatively, and a 45% improvement in mean ICIQ-UI-SF score from 18.1 pre-operatively to 9.4 post-operatively. These translated to statistically significant improvements in pad usage (p = 0.001) and ICIQ-UI-SF score (p = 0.001) using the paired t testing. These results are depicted in Fig. 6. There were no significant improvements in ICIQ-OAB scores. The average PGII score was 2.63, which ranges from 1 (very much better) to 7 (very much worse). Out of those with mixed incontinence, three patients continued to have intravesical Botox injections. One patient went on to have further urethral bulking treatment, despite significant improvement in incontinence from 16 to 3 daily pads.

Graph comparing pre-operative and post-operative pad usage and ICIQ-UISF scores
There was one intra-operative complication and two post-operative complications. The lone intra-operative complication was a serosal bowel injury that was repaired intracorporeally. Of the two post-operative complications, one patient failed trial without catheter post-operatively. This patient began clean intermittent self-catheterisation three times a week, and stopped intermittent catheterisation by 4 weeks post-operatively. Another patient had a post-operative urinary tract infection that was treated successfully with a 7-day course of oral antibiotics.
Discussion
We present our early experience of a novel minimally invasive surgical approach to a well-established surgical technique for female SUI. Statistically significant improvements were seen in both pad usage and ICIQ-UISF scores suggesting good early functional outcome in these patients with this approach. Transient bladder dysfunction was seen in one patient. This is in keeping with the positive outcomes reported in the literature for open Burch colposuspension [5, 8, 18].
Trials have looked at the benefit of laparoscopic surgery compared with open surgery in colposuspension. A Cochrane review of these trials found no difference in the overall cure rates between the open and the laparoscopic group (RR 0.95; 95% CI 0.80–1.11), with only one small trial demonstrating outcomes favouring the MIS group—although this did not reach statistical significance. Generally, laparoscopic colposuspension reported shorter operating times by 15–30 min compared to open and shorter length of stay, quicker return to normal activity and shorter time to successful trial without catheter. There were no statistically significant differences in complications post either approach (14% vs 12%; RR 1.18; 95% CI 0.64–2.16). Similarly, no difference in prolapse events or voiding dysfunction post operatively was found between open and laparoscopic colposuspension [8].
The rationale for adopting robotic minimally invasive surgery in performing colposuspension comes from the now widely accepted benefits to minimally invasive and robotic surgery demonstrated within urological oncology especially. The narrow pelvis is an ideally suited environment to utilise the advantages of magnification, manoeuvrability and dexterity that robotic surgery confers over open and laparoscopic techniques.
There have been isolated case reports in the literature assessing the feasibility of robotic Burch colposuspension. Khan et al in 2007 first reported successful completion of robotic colposuspension using an extraperitoneal approach in two patients with an average operating time of 145 min, blood loss of 15 ml and length of stay of 4.5 days. Both these patients were continent at 1 year, with the group concluding that the robotic approach was an effective modality in female SUI [19]. Since then isolated reports in single patients focusing on technique and modifications can be found in the literature, but larger patient numbers and long-term follow-up of this technique remains lacking [20, 21].
Currently, our series reports on the largest number of colposuspension procedures to be performed robotically. This series has demonstrated good early functional outcomes with a 73% improvement in mean pad use and a 45% improvement in ICIQ-UISF scores. Only one patient had voiding difficulty post procedure, and this was transient—resolved by 4 weeks. We report only two minor post-operative complications, highlighting the safety of the robotic approach.
This study is not without its limitations. Although our database is prospectively recorded, the analysis carried out is retrospective. This series represents data from two surgeons, both with a female urology background, operating with experienced robotic mentors. The effect of the learning curve is not adjusted for in this report. Based on our study design and database recording it is also difficult to adjust for experience of assistants and training time during the analysis of various outcome measures. Nevertheless this study presents positive initial functional outcome indicators and safety profile of the early adoption of robotic-assisted colposuspension for SUI.
Conclusion
This study is one of the largest series in the world of its kind. Robotic colposuspension is safe and feasible with satisfactory early functional outcomes. Significant improvements were seen in quality of life scores and number of pads used per day. Despite the cost constraints, the advantage of robotic surgery over conventional surgery has seen its adoption in a wide spectrum of pathology. The advantage of robotic surgery in pelvic oncology has seen its rapid rise, whereby its use is now considered the norm. Similar benefits can be obtained in benign and functional pelvic surgery and this is an aspect that we believe will grow in the future. As such it is vital that appropriate training, mentoring, standardisation of technique/pathway and rigorous review of outcomes and practice is carried out to ensure the safe transition to robotic skills and maintaining functional outcomes.
Larger volume and longer follow-up are required for further evaluation of this technique. Robotic-assisted laparoscopic colposuspension is safe, feasible and has satisfactory early functional outcomes, presenting a minimally invasive treatment option in female SUI.
References
Hunskaar S et al (2003) Epidemiology and natural history of urinary incontinence in women. Urology 62(4 Suppl 1):16–23
Abrams P et al (2003) The standardisation of terminology in lower urinary tract function: report from the standardisation sub-committee of the International Continence Society. Urology 61(1):37–49
Ulmsten U et al (1996) An ambulatory surgical procedure under local anesthesia for treatment of female urinary incontinence. Int Urogynecol J Pelvic Floor Dysfunct 7(2):81–85 (discussion 85-6)
Ward KL, Hilton P, U.a.I.T.T. Group (2008) Tension-free vaginal tape versus colposuspension for primary urodynamic stress incontinence: 5-year follow up. BJOG 115(2):226–233
Novara G et al (2008) Complication rates of tension-free midurethral slings in the treatment of female stress urinary incontinence: a systematic review and meta-analysis of randomized controlled trials comparing tension-free midurethral tapes to other surgical procedures and different devices. Eur Urol 53(2):288–308
Withington J, Hirji S, Sahai A (2014) The changing face of urinary continence surgery in England: a perspective from the Hospital Episode Statistics database. BJU Int 114(2):268–277
BBC (2018) Immediate stop to NHS mesh operations. https://www.bbc.co.uk/news/health-44763673. Accessed June 2020.
Lapitan MCM, Cody JD, Mashayekhi A (2017) Open retropubic colposuspension for urinary incontinence in women. Cochrane Database Syst Rev 7:CD002912
Ward KL et al (2008) Tension-free vaginal tape versus colposuspension for primary urodynamic stress incontinence: 5-year follow up. BJOG 115(2):226–233
Fusco F et al (2017) Updated Systematic review and meta-analysis of the comparative data on colposuspensions, pubovaginal slings, and midurethral tapes in the surgical treatment of female stress urinary incontinence. Eur Urol 72(4):567–591
Singh I, Hemal AK (2009) Role of robot-assisted pelvic surgery. ScientificWorldJournal 9:479–489
Liu CY (1993) Laparoscopic retropubic colposuspension (Burch procedure). A review of 58 cases. J Reprod Med 38(7):526–530
Gumus II, Surgit O, Kaygusuz I (2013) Laparoscopic single-port Burch colposuspension with an extraperitoneal approach and standard instruments for stress urinary incontinence: early results from a series of 15 patients. Minim Invasive Ther Allied Technol 22(2):116–121
Bradshaw AW et al (2020) Robotic Partial Nephrectomy versus Minimally Invasive Radical Nephrectomy for Clinical T2a Renal Mass: A Propensity Score Matched Comparison from the ROSULA (Robotic Surgery for Large Renal Mass) Collaborative Group. BJU Int 126:114–123
Checcucci E et al (2020) Single-port robot-assisted radical prostatectomy: a systematic review and pooled analysis of the preliminary experiences. BJU Int 126:55
Falagario U et al (2020) Robotic-assisted surgery for the treatment of urologic cancers: recent advances. Expert Rev Med Devices 17:579–590
Gallioli A et al (2020) Learning curve in robot-assisted kidney transplantation: results from the European Robotic Urological Society Working Group. Eur Urol 78:239–247
Norton P, Brubaker L (2006) Urinary incontinence in women. Lancet 367(9504):57–67
Khan MS et al (2007) Robotic colposuspension: two case reports. J Endourol 21(9):1077–1079
Francis SL et al (2015) Robotic Burch colposuspension: a surgical case and instructional video. Int Urogynecol J 26(1):147–148
Bora GS et al (2017) Robotic Burch colposuspension-modified technique. J Robot Surg 11(3):381–382
Funding
No conflict of interest.
Author information
Authors and Affiliations
Contributions
NT: urology trainee. data collection, data analysis, manuscript write-up. DS: urology senior clinical fellow, manuscript write-up. DT: clinical teaching fellow, data collection. TN: female urologist, manuscript review. CA: robotic pelvic surgeon, mentoring + training, manuscript review. HQ: robotic pelvic surgeon, mentoring + training, manuscript review. RI: robotic pelvic surgeon, mentoring + training, manuscript review. RW: regional lead for female urology, study design, manuscript review. JS: lead female urology surgeon, concept design, ethical/novel procedure grant, study design, primary surgeon being mentored and trained to deliver the service, manuscript review.
Corresponding author
Ethics declarations
Conflict of interest
No conflict of interest.
Ethical approval
Obtained from novel procedures committee as per Trust guidelines.
Consent to participate
Obtained from participants.
Consent to publish
Obtained from participants.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Tan, N., Sri, D., Tsang, D. et al. Robotic-assisted laparoscopic colposuspension for female stress urinary incontinence: a prospective series. J Robotic Surg 17, 125–129 (2023). https://doi.org/10.1007/s11701-022-01409-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11701-022-01409-6