
Abstract
The objective of this study is to examine the costs attributable to robotic-assisted laparoscopic hysterectomy from a broad healthcare sector perspective in a register-based longitudinal study. The population in this study were 7670 consecutive women undergoing hysterectomy between January 2006 and August 2013 in public hospitals in Denmark. The interventions in the study were total and radical hysterectomy performed robotic-assisted laparoscopic hysterectomy (RALH), total laparoscopic hysterectomy (TLH), or open abdominal hysterectomy (OAH). Service use in the healthcare sector was evaluated 1 year before to 1 year after the surgery. Tariffs of the activity-based remuneration system and the diagnosis-related grouping case-mix system were used for valuation of primary and secondary care, respectively. Costs attributable to RALH were estimated using a difference-in-difference analytical approach and adjusted using multivariate linear regression. The main outcome measure was costs attributable to OAH, TLH, and RALH. For benign conditions RALH generated cost savings of € 2460 (95% CI 845; 4075) per patient compared to OAH and non-significant cost savings of € 1045 (95% CI −200; 2291) when compared with TLH. In cancer patients RALH generated cost savings of 3445 (95% CI 415; 6474) per patient when compared to OAH and increased costs of € 3345 (95% CI 2348; 4342) when compared to TLH. In cancer patients undergoing radical hysterectomy, RALH generated non-significant extra costs compared to OAH. Cost consequences were primarily due to differences in the use of inpatient service. There is a cost argument for using robot technology in patients with benign disease. In patients with malignant disease, the cost argument is dependent on comparator.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hysterectomy is the most common major gynecological procedure in Denmark with an annual volume of 180 per 100,000 women [1]. The indications for hysterectomy range from benign conditions such as abnormal uterine bleeding, fibroids, and endometriosis, as well as pre-malignant and malignant conditions such as uterine and cervical cancer [2]. Historically, open abdominal hysterectomy (OAH) was the preferred surgical modality with evidence gradually emerging that conventional laparoscopy [total laparoscopic hysterectomy (TLH)] was a safe alternative to OAH. Although worldwide recognition of the laparoscopic approach within both benign and malignant gynecology, routine use was mainly adopted at highly specialized centers for, e.g., endometriosis or gynecological cancer [3], while open abdominal hysterectomy (OAH) remained the most frequently used method in most countries at the time of the present study period [4].
Robotic-assisted laparoscopy is the latest innovation in the field of minimally invasive surgery [3, 5] and has been adopted within many specialties including the gynecological field. It has been claimed that the introduction of robotic-assisted laparoscopy has revolutionized the surgical approach since the proportional share of patients who are offered minimally invasive surgery has raised substantially [6]. Use of the robot technology shares patient-related advantages well known from conventional laparoscopy; shortened hospital stays, reduced blood loss, and fewer complications [2, 4, 6,7,8,9,10,11,12,13,14]. In addition, robotic-assisted laparoscopy has been claimed to improve the ergonomics of the surgeons compared to laparoscopy and open surgery and to have the advantage of a faster learning curve [12, 15, 16]. However, the literature is not definite in terms of these benefits when compared to laparoscopy alone [4, 6, 8, 9, 12,13,14,15, 17, 18]. Disadvantages such as limited availability of skilled technical staff, longer operation time, and substantial capacity costs have also been pointed out [5,6,7, 13,14,15, 17, 19,20,21,22,23].
Studies comparing the costs of robot-assisted laparoscopic hysterectomy (RALH) with the costs of OAH or TLH have demonstrated higher costs for robot-assisted procedures in the range of $ 1936 to $ 5059 when looking only at costs related to the operation and hospital admission [8, 15, 17, 19, 20]. It has been suggested that a broader cost perspective including the costs of complications, readmissions, and comorbidity as well as a longer follow-up period that goes beyond the index admission may reduce the additional costs of the robot technology [8, 24,25,26].
To date, most evidence concerning the costs of RALH derives from small-scale, non-controlled and in some cases highly selected populations, and commentators argue that there is insufficient evidence to draw definitive conclusions about the cost consequences of using the robot technology [5, 9, 23, 27]. Furthermore, it is unknown if derived cost consequences such as readmissions and service use in the primary sector could be affected.
Nonetheless, the adoption of the robot technology throughout both privately and publicly financed health care systems seem to accelerate and evidence on both the cost consequences and the clinical effects are warranted [3, 7, 17, 19, 28]. The objective of this study was to examine the costs attributable to RALH from a broad health care sector perspective.
Methods
Study design
The study was a register-based longitudinal study of consecutive women (n = 7670) undergoing hysterectomy for benign or malignant disease between January 2006 and August 2013. The women were followed from 1 year before to 1 year after the surgical procedure. The study is a further analysis of data collected in relation to a Health Technology Assessment of robot-assisted surgery for several procedures including hysterectomy [29].
Study population
Consecutive women were identified in The Danish National Patient Register [30] using procedure codes for OAH and open radical hysterectomy (ORH) (KLCD00, KLCD30), TLH and laparoscopic radical hysterectomy (LRH) (KLCC11, KLCD01A, KLCD01, KLCD01B, KLCD04, KLCD31), and further linked to the robotic attributable codes (KZXX00, ZPW00002). To support comparability of the patients, a restriction was made to women who received the surgical procedure at a hospital where all surgical techniques were offered at the time of surgery.
The study population was stratified according to indication for surgery based on the diagnosis of action from the National Patient Registry. The registry records version 10 of the The International Classification of Diseases (ICD-10). Malignant disease was identified as all diagnostic codes starting with “C” and benign disease was identified by all other codes. In total, 38 women were defined by ‘Carcinoma in situ’ and ‘Tumour without invasion’ and therefore reclassified from malignant to benign disease. For malignant disease, the women were further grouped into the more advanced procedure, radical hysterectomy, or simple hysterectomy based on the procedure codes. Sixteen women undergoing laparoscopic radical hysterectomy did not have a robotic procedure code and were manually given one because this procedure is not undertaken by conventional laparoscopy in Denmark.
Setting
The surgical procedures were all performed in a public hospital setting. As for the oncological operations, these were undertaken at centers that were highly specialized within gynecological cancer surgery.
Cost and data sources
In Denmark, all use of health care is recorded in national administrative registries and all residents in Denmark have a unique personal identification number that can be used to link individual registries [30]. Costs were considered from a health care system perspective and included primary care use (general practitioners, medical specialists, therapists, and other privately practicing specialists) and secondary care use (all cause inpatient admissions, procedures, and outpatient visits). Information on use of primary care was derived from The Danish National Health Service Register and was valued using the national collectively bargained tariffs [31]. Information on use of secondary care was obtained from The Danish National Patient Register and valued using tariffs of the national Diagnosis-Related Grouping system (DRG) and the Danish Outpatient Grouping System (DAGS) [30].
The DRG tariffs for the index hysterectomy cover the activity from the day of admission to the day of discharge (preparation, surgery, remobilization and discharge) whereas follow-up visits and other events after discharge, e.g., caused by complications, are separately reimbursed. The 2014 tariffs for the three surgical techniques are: standard benign OAH and TLH € 5289 and standard benign RALH € 8624, standard malignant OAH and TLH € 7263 and standard malignant RALH € 14,029. The higher tariffs of RALH are attributable to more costly instrument kits, robot maintenance costs and longer operating time.
Costs were adjusted for inflation using the general consumer price index and reported in Euros for the price year 2014.
Sensitivity analysis
Several sensitivity analyses were conducted to test the robustness of findings to alternative methodological choices. First, length of stay after the surgical procedure was included in the regression model to compensate for the lack of individual-level variation in the DRG tariff for the hysterectomy. Second, potential misclassification of surgical procedure was tested by conversion of all conventional laparoscopic procedures into robot-assisted procedures (this could have happened if the first robot-assisted procedures were misclassified as conventional laparoscopic procedures due to not knowing the new procedure code).
Statistics
Analyses were undertaken separately for the groups of benign disease, malignant disease + simple hysterectomy, and malignant disease + radical hysterectomy. Summary statistics were used to describe patient characteristics: Pearson’s Chi-square test for categorical variables and analysis of variance (ANOVA) for continuous variables.
A difference-in-difference (DiD) analytical strategy was used to estimate the cost attributable to the use of the robot technology. First, the cost of hysterectomy was estimated as the difference in health care costs between the year following surgery and the year preceding surgery to cancel out, e.g., chronic comorbidity. Second, the cost attributable to robot technology was estimated as the differences in average health care costs for the surgical techniques of RALH versus TLH, and RALH versus OAH, respectively, to cancel out significant influence of e.g. time trends. Differences are reported as arithmetic means with 95% confidence intervals based on bootstrapping (a method sampling from the empirical distribution of data instead of assuming a particular probability distribution) with 5000 replicates due to the skewed nature of the data.
Multivariate linear regression was used to adjust the DiD estimator for characteristics that could mask risk selection to surgical technique. The choice of variables was based on a review of the literature of patient characteristics associated with choice of surgical method and included: age, comorbidity (characterized by Charlson’s comorbidity index [32]), and cancer severity (classified according to the TNM-classification [33]). As a substantial number of cases lacked TNM registrations, a dummy variable was created for missing values to maintain cases in the model. Finally, regional variation at the organizational level was included by region id [29]. Due to the hierarchical data structure, robust standard deviations were estimated. Results are reported as means with 95% confidence intervals. All tests were two-sided and p values less than .05 were considered significant. All statistical analyses were performed using Stata 13.0.
Results
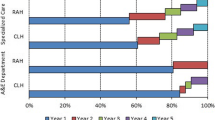
A total of 7670 women who underwent hysterectomy at six hospitals around Denmark were included. The majority underwent OAH (63%), followed by almost equal proportions of TLH and RALH (19 and 18%, respectively). More than half of the population underwent surgery for malignant disease (52%). While one-third of the women undergoing TLH were operated for malignant disease (34%), and half of the women undergoing OAH were operated for malignant disease (53%), the majority (69%) of women operated with robot-assisted laparoscopy underwent surgery for malignant disease. Patient characteristics are detailed in Table 1.
Patient costs from each surgical technique are illustrated over time in Figs. 1 and 2. Primary care costs were small compared to secondary care costs in both patients operated for malignant and benign disease, while costs in secondary care were higher in patients undergoing surgery for malignant disease than in patients undergoing surgery for benign disease. In benign disease, total health care costs were high following OAH because of high inpatient costs as compared to RALH and TLH. Also in patients with malignant conditions OAH resulted in the highest health care costs primarily due to high outpatient costs both prior to and following surgery.

Time series graphics for the unadjusted mean costs (€) in patients with benign conditions. Month zero marks the time of hysterectomy

Time series graphics for the unadjusted mean costs (€) in patients with malignant conditions (simple hysterectomy only). Month zero marks the time of hysterectomy
Table 2 shows the service use and the corresponding unadjusted costs related to hysterectomy for women with benign disease. RALH was associated with the shortest length of stay (bed days) following surgery thus contributing to the lowest inpatient costs, but the most outpatient visits, resulting in the highest outpatient costs. OAH was associated with a longer hospital stay and higher inpatient costs than its two minimally invasive counterparts. The results of the multivariate analyses are shown in Table 4. It is demonstrated that RALH was associated with the lowest health care costs when compared to TLH and OAH, respectively. For benign conditions, the adjusted analysis did not change the conclusions made from Table 2. As it appears in Table 4 RALH generated significant cost savings of € 2460 (95% CI 845; 4075) when compared to OAH and non-significant cost savings of € 1045 (95% CI −200; 2291) when compared to TLH.
Table 3 shows the service use and corresponding unadjusted costs for women with malignant disease. In women undergoing simple hysterectomy, RALH seemed to incur the shortest length of stay following surgery although the difference between the two was only 0.6 day. Yet, TLH incurred the lowest inpatient, outpatient and total health care costs. OAH generally led to a substantially longer length of stay as well as more outpatient visits, thereby contributing to considerably higher costs following surgery as compared to RALH and TLH.
In women undergoing radical hysterectomy, use of robotic-assisted surgery was associated with the lowest outpatient costs, however, the highest inpatient and total health care costs when compared to OAH.
The multivariate analyses showed different results depending on whether RALH was compared to TLH or OAH (Table 4). The adjusted analysis did not change the conclusions made from Table 3; however, the magnitude of the cost estimates did change. In women with cancer undergoing simple hysterectomy, use of robotic-assisted surgery generated significant excess costs of € 3345 (95% CI 2348; 4342) when compared to TLH and significant cost savings of € 3445 (95% CI 415; 6474) when compared to OAH. In women undergoing radical hysterectomy, open access surgery was the only available comparator to RALH since neither of the hospitals performed this procedure as conventional laparoscopy. In this case, use of robotic-assisted surgery was found to generate non-significant increased costs of € 7282 (95% CI −7079; 21,644).
None of the sensitivity analyses were found to change the results noticeably. Potential misclassification of surgical procedure showed the largest impact on the results, with RALH generating significant cost savings of € 4631 (597; 8665) when compared to OAH in cancer patients undergoing simple hysterectomy, corresponding to a cost saving of € 1186 more than the one depicted in Table 4.
Discussion
Main findings
Our study demonstrates that the use of robot technology for hysterectomy is potentially cost saving from a broad health care sector perspective. This seems to apply for both benign and malignant disease when compared to open surgery whereas when compared to laparoscopic surgery, the use of robot technology for simple hysterectomy in malignant disease seems to increase costs.
Interpretation in light of other evidence
The existing literature indicates that RALH is more costly when compared to OAH [5, 7, 23] and TLH [5, 8, 15, 17, 19,20,21, 23] whereas only one study suggests that the use of robot technology could be cost neutral [25]. The present study appears to be the first that includes a 1-year follow-up and covers the entire health care sector in relation to consequences of hysterectomy. Our results are in agreement with previous findings of higher costs of RALH when compared to TLH in malignant conditions [8, 19, 25]. However, divergence is noticed for benign conditions where most studies have demonstrated additional costs related to RALH compared to TLH [14, 17, 19, 20, 22].
Sarlos et al. estimated the surgical costs of RALH for benign conditions at € 4067 and the corresponding estimate of TLH at € 2151. The analysis did, however, only include costs generated in the operating room, while no potential cost consequences of post discharge follow-up or readmissions were included [15]. Lönnerfors et al. included the costs of complications and readmissions until four months after surgery and demonstrated similar costs of RALH ($ 7016) and TLH ($ 7059) when ignoring the purchase cost of the robot [13]. In the light of the present results, this suggests that the longer the follow-up, the less the additional cost of using the robot technology.
The total costs of health care for RALH patients were higher than the total costs of health care for TLH and OAH patients. This indicates that patients selected to robotic surgery had more severe disease, either related to the gynecological disease or comorbidity, and did not represent the easiest cases. This is somewhat counterintuitive to the fact that robotic surgery is a relatively new technology in Denmark. As an example; one of the centers started out their robotic program in 2010 by operating patients with endometriosis. These patients represent a group with a high demand for outpatient visits both before and probably also after surgery due to physical and psychological symptoms. By using the DiD design, time invariant costs cancel out and by further adjusting for baseline covariates we seek to control residual risk selection. It should, however, be noted that potentially relevant covariates such as psychological health and body mass index (BMI) were unobserved and thus not controlled for. If these are associated with selection into RALH and higher health care costs after RALH, our results potentially overestimate the cost implications of using robot technology.
Our findings should be viewed and interpreted in the perspective of the national implementation of minimally invasive cancer surgery in Denmark and additionally, aspects regarding complexity of the surgical procedure and its re-imbursement should be discussed in this regard. First, Denmark has succeeded in centralization of gynecological cancer surgery to highly specialized centers; for, e.g., endometrial cancer six centers since 2006 (four centers for high-risk endometrial cancer since 2012) and for cervical cancer five centers until 2012 and since then four centers. All centers report all surgical and pathological data to a national database, with reporting being compulsory and published annually in an official report. Hence, trends and activities are carefully monitored and discussed at national multidisciplinary meetings and in the board of the Danish Gynecological Cancer Group with members being responsible for updating the national guidelines. Most gynecological cancer cases were performed as open procedures until the years 2008–2010. Before this period only three centers performed TLH and only in low-intermediate risk endometrial cancer whereas high-risk endometrial cancer and cervical cancer was operated by open surgery. In 2008, the first center acquired a robot and introduced TLH including pelvic lymphadenectomy when indicated, as a routine procedure. In 2010 the second and in 2012 the third center introduced a robotic program with similar set up as described. All three centers went directly from performing most cases as open procedures to perform most cases as robotic procedures. The remaining centers had limited access to robotic surgery until 2012–2013 but were also the centers performing TLH routinely in low-intermediate risk endometrial cancer while saving the limited robotic surgical capacity to more complex procedures. The more complex procedure as, e.g., radical hysterectomy was gradually introduced at all centers when the access to robotic surgery increased; however, it was never performed by conventional laparoscopy. Likewise, para-aortic lymphadenectomy was performed as open procedure and not performed by robotic access in Denmark until after the study period. Hence, as it appears that, although conventional laparoscopy was available at all centers and used within benign gynecology, it never gained nationwide currency within gynecological cancer surgery as a routine procedure.
As it appears from the description of the robotic implementation process in Denmark, our results from a study period 2006–2013 could be argued to derive from the time course of a robotic learning curve as opposed to results obtained for TLH. TLH was performed as a routine procedure at two large and one smaller center at the time of the first robotic implementation. Further, analyses relying on index tariffs are at present not able to correctly expose the complexity of the surgical procedure performed along with the RALH and TLH, respectively. Hence, explanations for the higher inpatient costs for simple hysterectomy in patients with malignant disease are likely to reflect a combined effect of more expensive instruments, learning curve, and a deliberate selection towards using the robot even in complex cases if open access was the alternative [34, 35].
Regarding radical hysterectomy our analyses suggested, although not significant, higher total costs when using the robot compared to open surgery. Reynisson et al. compared the costs of RALH to the costs of OAH in women with cervical cancer undergoing radical hysterectomy. Based on 231 women with 3-month follow-up after surgery they concluded that robotic surgery can be performed at an equal hospital cost compared to open access, but only after the procedure has been well implemented [7]. It has been shown in other areas of robotic application that operating time, complication rate, and length of stay decrease as the robot technology matures [7, 36, 37] and this will most likely affect the costs.
We have previously described the comparatively slow implementation of robotic surgery for advanced gynecological procedures in Denmark [29]. This limited the inclusion window substantially regarding radical hysterectomy due to the criterion of a center having to offer all three techniques by the time of surgery in order for a patient to be included in this analysis, e.g., only 150 patients had robot-assisted radical hysterectomy. As such, we were not able to rule out that some of the increased costs attributable to advanced robotic surgery in patients with malignant disease merely reflect a learning curve. However, it is noteworthy that the main reason for increased total costs related to robotic-assisted laparoscopic radical hysterectomy (RLRH) was mainly caused by increased inpatient costs one year post surgery and not additional bed days as one would expect if the increased costs reflected re-admissions due to more complications. Hence, although potentially biased due to the small number of included patients, the comprehensive analyses suggested that implementation of robotic-assisted laparoscopy in advanced gynecological cancer procedures leads to reduced admission days and does not seem to cause more re-admissions as compared to open access. In the future, the index tariffs may undergo regulation as instrumental costs may decrease and knowledge concerning admission days is included.
Strengths and weaknesses
We examined costs of RALH compared to both OAH and TLH. Costs related to all health care sectors were included eliminating selection bias and supporting external validity. To our knowledge, the present study is the first to report separate costs related to both benign and malignant conditions. Whether women have cancer or not affects the extent of health care use [38], indicating that the two should be reported separately.
A further strength is the difference-in-difference (DiD) design used in the study. The DiD design serves to minimize the risk of selection bias. External conditions, such as comorbidity, were thus excluded from the analysis. Further, by the DiD design, exogenous factors such as time trends were eliminated when comparing the different surgical techniques.
Our study also has weaknesses. It relied on multivariate regression analysis in combination with a DiD design to handle confounding from selection into surgical techniques. When it comes to choice of surgical modality and surgically related complications, BMI, uterine size, previous surgeries, and the presence of endometriosis may be important confounding factors [2, 17, 27, 39]. Due to our study design, we were not able to control for these confounders. This is a relevant focus in future studies. However, the use of a DiD design will adjust for the confounding effects related to chronic conditions such as extreme BMI values as long as its effect on costs before and after hysterectomy is equal.
There was an uneven distribution of patients with nodal involvement and metastases for women undergoing the different surgical procedures for simple hysterectomy, which could bias the results of Table 3 as more extensive disease might lead to more extensive surgery and more complications. However, when adjusting for confounders in Table 4, possible bias were eliminated.
Index tariffs for gynecological robotic-assisted laparoscopy were introduced in 2008 and the amount of re-imbursement reflects the estimated additional costs for the hospital using, e.g., RALH compared to open or laparoscopic procedures. As an example, the difference in index tariff for a complex robotic surgical procedure (e.g., RALH + pelvic lymphadenectomy) compared to TLH + pelvic lymphadenectomy is approximately 5000 € to cover for the excess costs related to more expensive instrument kits and maintenance of the robot. Separate tariffs for the even more complex procedures such as radical hysterectomy and para-aortic lymphadenectomy have not yet been established in the Danish system and this means that our results averages out the both plain RALH and these more complex procedures.
Limitations regarding generalizability
A limitation in the present study is the use of national average tariffs for the surgical procedure without taking into account the level of technical efficiency that characterizes the operation of the robot, i.e., how efficiently the robot capacity is utilized in terms of equipment and specialised staff [40]. Our results represent the average level of efficiency for the Danish health care system during a period of 7.5 years and the external validity of the results thus strongly depend on how comparable the levels of efficiency are between settings.
An important consideration when examining the costs of RALH is that other surgical methods are compared with a method under development, and thus the position on the learning curve is likely to affect the results [7, 8, 15]. Trials comparing robot-assisted with laparoscopic and vaginal approaches have demonstrated some bias in favor of non-robotic methods as surgeons performing robotic hysterectomies had only limited experience compared to those performing laparoscopic and hysterectomies [14, 21, 41]. Lim et al. provides compelling evidence for the advantages of robot-assisted hysterectomy for benign disorders when performed by surgeons with high-volume experience compared with laparoscopic, vaginal, or open abdominal hysterectomies performed by high-volume surgeons [42]. Also, the cost-efficiency of the robot technology is likely to develop with production volume and specialization, and therefore the cost per future procedure could be overestimated.
Finally, the present study was restricted within a health care perspective and it should be noted that a broader perspective including sick leave and production loss could potentially impact the conclusion. Given that RALH patients had fewer readmissions, they might have recovered more quickly and thus incurred less production loss. Including aspects of societal perspectives is important in future studies.
Conclusion
From a broad health care sector perspective, there seems to be a cost argument for the use of RALH in women with benign conditions whereas in women with malign disease, the cost argument is dependent on comparator. For external validity, it is important to consider how efficiently the robot technology is run, e.g., considering capacity use of equipment, availability of skilled staff and position on the learning curve when comparing to other surgical modalities.
Practical and research recommendations
Today, many hysterectomies are conducted as open surgery. Open access hysterectomy is substantially more costly than RALH and it should, therefore, be considered whether the choice of OAH is founded in evidence for clinical superiority.
The technical efficiency aspect of robot technology with respect to capacity utilization and learning curve position in particular should be examined more closely to estimate long-run consequences of the dissemination of the robot technology.
References
Lykke R, Blaakær J, Ottesen B, Gimbel H, Hysterectomy in Denmark 1977–2011 (2013) Changes in rate, indications, and hospitalization. Eur J Obstet Gynecol Reprod Biol 171(2):333–338
Geisler JP, Orr CJ, Khurshid N, Phibbs G, Manahan KJ (2010) Robotically assisted laparoscopic radical hysterectomy compared with open radical hysterectomy. Int J Gynecol Cancer 20(3):438–442
Advincula AP, Song A (2007) The role of robotic surgery in gynecology. Curr Opin Obstet Gynecol 19:331–336
Martino MA, Berger EA, McFetridge JT, Shubella J, Gosciniak G, Wejkszner T et al (2014) A comparison of quality outcome measures in patients having a hysterectomy for benign disease: robotic vs. non-robotic approaches. J Minim Invasive Gynecol 21(3):389–393
Liu H, Lu D, Wang L, Shi G, Song H, Clarke J (2012) Robotic surgery for benign gynaecological disease (review). Cochrane Collab 2:1–20
Swan K, Advincula AP (2011) Role of robotic surgery in urogynecologic surgery and radical hysterectomy: how far can we go? Curr Opin Urol 21:78–83
Reynisson P, Persson J (2013) Hospital costs for robot-assisted laparoscopic radical hysterectomy and pelvic lymphadenectomy. Gynecol Oncol. 130(1):95–99
Desille-Gbaguidi H, Hebert T, Paternotte-Villemagne J, Gaborit C, Rush E, Body G (2013) Overall care cost comparison between robotic and laparoscopic surgery for endometrial and cervical cancer. Eur J Obstet Gynecol Reprod Biol 171(2):348–352
Reza M, Maeso S, Blasco JA, Andradas E (2010) Meta-analysis of observational studies on the safety and effectiveness of robotic gynaecological surgery. Br J Surg 97:1772–1783
Paley PJ, Veljovich DS, Shah CA, Everett EN, Bondurant AE, Drescher CW et al (2011) Surgical outcomes in gynecologic oncology in the era of robotics: analysis of first 1000 cases. Am J Obstet Gynecol 204(6):551.e1–551.e9
Seamon LG, Bryant SA, Rheaume PS, Kimball KJ, Huh WK, Fowler JM et al (2009) Comprehensive surgical staging for endometrial cancer in obese patients. Obstet Gynecol 114(1):16–21
Seamon LG, Cohn DE, Henretta MS, Kim KH, Carlson MJ, Phillips GS et al (2009) Minimally invasive comprehensive surgical staging for endometrial cancer: robotics or laparoscopy? Gynecol Oncol 113(1):36–41
Lönnerfors C, Reynisson P, Persson J (2015) A randomized trial comparing vaginal and laparoscopic hysterectomy vs robot-assisted hysterectomy. J Minim Invasive Gynecol 22:78–86
Rosero EB, Kho KA, Schaffer JI, Giesecke M (2013) Comparison of robotic and laparoscopic hysterectomy for benign gynecologic disease. Obstet Gynecol 122(4):778–786
Sarlos D, Kots L, Stevanovic N, Schaer G (2010) Robotic hysterectomy versus conventional laparoscopic hysterectomy: outcome and cost analyses of a matched case-control study. Eur J Obstet Gynecol Reprod Biol 150(1):92–96
Gehrig PA, Cantrell LA, Shafer A, Abaid LN, Mendivil A, Boggess JF (2008) What is the optimal minimally invasive surgical procedure for endometrial cancer staging in the obese and morbidly obese woman? Gynecol Oncol 111(1):41–45
Wright JD, Ananth CV, Lewin SN, Burke WM, Lu Y, Neugut AI et al (2013) Robotically assisted vs laparoscopic hysterectomy among women with benign gynecologic disease. JAMA J Am Med Assoc 309(7):689–698
Aarts J, Nieboer T, Johnson N, Tavender E, Garry R, Mol B. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst Rev. 2015;12(8):13–37
Pasic RP, Rizzo JA, Fang H, Ross S, Moore M, Gunnarsson C (2010) Comparing robot-assisted with conventional laparoscopic hysterectomy: impact on cost and clinical outcomes. J Minim Invasive Gynecol 17(6):730–738. doi:10.1016/j.jmig.2010.06.009
Paraiso MFR, Jelovsek JE, Frick A, Chen CCG, Barber MD (2011) Laparoscopic compared with robotic sacrocolpopexy for vaginal prolapse. Obstet Gynecol 118(5):1005–1013
Paraiso MFR, Ridgeway B, Park AJ, Jelovsek JE, Barber MD, Falcone T et al (2013) A randomized trial comparing conventional and robotically assisted total laparoscopic hysterectomy. Am J Obstet Gynecol 208(5):368.e1–368.e7
Sarlos D, Kots L, Stevanovic, von Felten S, Schär G (2012) Robotic compared with conventional laparoscopic hysterectomy: a randomized controlled trial. Obstet Gynecol 120:604–611
Turchetti G, Palla I, Pierotti F, Cuschieri A (2012) Economic evaluation of da Vinci-assisted robotic surgery: a systematic review. Surg Endosc 26(3):598–606
Barnett JC, Judd JP, Wu JM, Scales CD, Myers ER, Havrilesky LJ (2010) Cost comparison among robotic, laparoscopic, and open hysterectomy for endometrial cancer. Obstet Gynecol 116(3):685–693
Bell MC, Torgerson J, Seshadri-Kreaden U, Suttle AW, Hunt S (2008) Comparison of outcomes and cost for endometrial cancer staging via traditional laparotomy, standard laparoscopy and robotic techniques. Gynecol Oncol 111(3):407–411
Teljeur C, O’Neill M, Moran PS, Harrington P, Flattery M, Murphy L et al (2014) Economic evaluation of robot-assisted hysterectomy: a cost-minimisation analysis. BJOG 121(12):1546–1553
Shi G, Lu D, Liu Z, Liu D, Zhou X. Robotic assisted surgery for gynaecological cancer (review). Cochrane Collab. 2014;(1):7–9. doi:10.1002/14651858.CD008640.pub2
Barbash GI, Glied SA (2010) New technology and health care costs—the case of robot-assisted surgery. N Engl J Med 363(8):701–704
CFK Folkesundhed & Kvalitetsudvikling. Health Technology assessment of robot-assisted surgery [Medicinsk teknologivurdering af robotassisteret kirurgi]. 2015
Lynge E, Sandegaard JL, Rebolj M (2011) The Danish national patient register. Scand J Public Health 39(7 Suppl):30–33
Andersen JS, Olivarius NDF, Krasnik A (2011) The Danish national health service register. Scand J Public Health 39:34–37
Charlson ME, Pompei P, Ales K, MacKenzie R (1987) A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 40(5):373–383
National Cancer Institute. Cancer Staging [Internet]. http://www.cancer.gov/cancertopics/factsheet/detection/staging. Cited 8 Nov 2015
Wu J, Wechter ME, Geller E, Nguyen T, Visco A (2007) Hysterectomy rates in the United States, 2003. Obstet Gynecol 110(5):1091–1095
Jacoby V, Autry M, Jacobsen G, Domush R, Nakagawa S (2009) Nationwide use of laparoscopic hysterectomy compared with abdominal and vaginal approaches. Obstet Gynecol 114(5):1041–1048
Steinberg PL, Merguerian PA, Bihrle W, Seigne JD (2008) The cost of learning robotic-assisted prostatectomy. Urology. 72:1068–1072
Mäenpää MM, Nieminen K, Tomás EI, Laurila M, Luukkaala TH, Mäenpää JU (2016) Robotic-assisted vs traditional laparoscopic surgery for endometrial cancer: a randomized controlled trial. Am J Obstet Gynecol 215(5):588.e1–588.e7
Jabaaij L, van den Akker M, Schellevis FG (2012) Excess of health care use in general practice and of comorbid chronic conditions in cancer patients compared to controls. BMC Fam Pract 13:60
Kannisto P, Harter P, Heitz F, Traut A, du Bois A, Kurzeder C (2014) Implementation of robot-assisted gynecologic surgery for patients with low and high BMI in a German gynecological cancer center. Arch Gynecol Obstet 290:143–148
Kruse M, Christiansen T (2011) Register-based studies of healthcare costs. Scand J Public Health 39:206–209
Kilic GS, Moore G, Elbatanony A, Radecki C, Phelps JY, Borahay MA (2011) Comparison of perioperative outcomes of total laparoscopic and robotically assisted hysterectomy for benign pathology during introduction of a robotic program. Obstet Gynecol Int 2011:683703
Lim PC, Crane JT, English EJ, Farnam RW, Garza DM, Winter ML et al (2016) Multicenter analysis comparing robotic, open, laparoscopic, and vaginal hysterectomies performed by high-volume surgeons for benign indications. Int J Gynecol Obstet Int Fed Gynecol Obstet 133(3):359–364
Acknowledgements
We would like to thank Line Stjernholm Tipsmark, DEFACTUM, Central Denmark Region, Denmark, for her valuable contribution on requisition of data and provisional analyses.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This study has been conducted in accordance with The Person Data Act, and approval from The Danish Data Protection Agency has been obtained (journal number 2007-58-0010).
Conflict of interest
All authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Funding
None declared.
Rights and permissions
About this article

Cite this article
Laursen, K.R., Hyldgård, V.B., Jensen, P.T. et al. Health care cost consequences of using robot technology for hysterectomy: a register-based study of consecutive patients during 2006–2013. J Robotic Surg 12, 283–294 (2018). https://doi.org/10.1007/s11701-017-0725-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11701-017-0725-x