
Abstract
To establish the design requirements for an MR-compatible haptic hand-controller, this paper measures magnitudes and frequency bands of three mechanical motion and interaction components during the performance of neurosurgical tasks on a cadaveric brain. The hand-controller would allow the performance of virtual neurosurgical tasks within the bore of a high field magnet during image acquisition, i.e., functional MRI. The components are the position and the orientation of a surgical tool, and the force interaction between the tool and the brain tissue. A bipolar forceps was retrofitted with a tracking system and a set of force sensing components to measure displacements and forces, respectively. Results showed working positional, rotational, and force frequency bands of 3, 3 and 5 Hz, respectively. Peak forces of 1.4, 2.9 and 3.0 N were measured in the Cartesian coordinate system. A workspace of 50.1 × 39.8 × 58.2 mm3 and orientation ranges of 40.4°, 60.1° and 63.1° for azimuth, elevation, and roll angles were observed. The results contribute in providing information specific to neurosurgery that can be used to effectively design a compact and customized haptic hand-controller reflecting characteristics of neurosurgical tasks.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Statement of the problem
Magnetic resonance imaging (MRI) can be used to image various types of tissues, and has an established value in neurological disease due to its remarkable soft tissue contrast [1, 2]. Furthermore, in addition to anatomical imaging, MRI also allows for functional brain imaging, i.e., fMRI. When a region of brain is activated to a given stimulus, increased blood flow occurs to the region. This change in blood flow may result in a mismatch such that the venous system contains oxygen rich blood, i.e., the basis of fMRI or BOLD effect [3]. Using fMRI, a brain can be mapped to different regions, each of which has a different functionality. This mapping is presented by color-coding to show not only the region of brain, but also the amount of activity in that region. Functional MRI can be used to identify, for example, language or speech processing areas in the intact human brain [4]. One way to examine brain activities, in fMRI, is to ask the subject to perform a physical task. This is possible by moving a hand-controller (joystick) located inside the MR bore that emulates an actual task in a virtual environment. The subject, however, is positioned supine on a table. A requirement for such a hand-controller is the capability of transferring essential information of the task environment, such as workspace and force to provide a sense of telepresence to the subject [5]. Several haptic interfaces have been used in a wide variety of applications such as medical robotics, tele-ultrasound, virtual reality, tele-surgery, and micromanipulation and assembly [6–11]. However, none of them has specifically been constructed for neurosurgical applications, emulating the workspace and interaction forces during the performance of real neurosurgical tasks.
This work is the preliminary stage of an ongoing work in Project neuroArm that focuses on the development of an MR-compatible haptic interface to study surgeon’s regional brain activities and evaluate surgical performance. The haptic interface will include two main elements: a haptic hand-controller and a virtual reality graphical interface to provide a more close-to-real environment for the surgeon. The surgeon grasps the surgical tool attached to implement of the hand-controller (while lying supine), looks at the graphical interface, and conducts the surgical task depicted in the graphical interface. Due to the confined space available inside the bore of magnet and the fact that subject cannot have large range of motion as it induces image artifacts, knowing minimal required workspace of the hand-controller during performance of microsurgical tasks is crucial. Furthermore, neurosurgery is very much dependent on touch [12], and therefore in addition to providing motions similar to real neurosurgical tasks, the fidelity of mimicked forces, applied to the surgeon’s hand, must represent real forces encountered during real surgery. Therefore, in this pilot study, the workspace and force components of neurosurgical maneuvers are quantified during conventional neurosurgery performed on a cadaveric head.
This paper reports the design requirements of a haptic interface in terms of the operational workspace and the force generating capabilities matched to neurosurgical tasks. The quantified information consists of both frequency and magnitude contents. The workspace and force components were measured during conventional (freehand) neurosurgery performed on a cadaveric head to allow the hand-controller reflecting characteristics of real surgical tasks. A tracking system and a novel force-sensing component were employed to measure the displacements and forces, respectively. The instrumented bipolar forceps was the developed version of the forceps by which the authors measured the tool-tissue interaction forces [13, 14]. Experiments were conducted on a cadaveric brain to perform 35 neurosurgical tasks over 1000 s of neurosurgery.
For frequency, we determined the operational bandwidth of all interactions to successfully stereotype forces in the entire frequency range and precisely mimic forces [15]. One way to find the effective frequency range for the design of the hand-controller is to implement spectral analysis over the acquired force signals to extract both dominant frequencies and frequency range of interest. For a hand-controller with single-axis actuators, it is necessary to determine a single range of frequency to properly mimic tool-issue interaction forces and hand motions. There exist different dimensional reduction methods in the frequency and time domains, which transforms a 3-axis signal to a 1-axis signal. Common techniques for signal dimensional reduction can be, (i) algebraic addition of time domain signal components, (ii) vectorial magnitude of signal components, and (iii) principal component analysis [15]. However, these methods can result in the loss of spectral contents of the signal and adding DC components to the frequency domain after Discrete Fourier Transform (DFT) analysis. To alleviate this problem, Landin et al. [16] suggested preserving the spectral contents by spectral match, which preserves the spectral energy at each frequency. To implement this method, the DFT of each signal is calculated and energy components at each frequency are added as the vectorial magnitude. Therefore, the vertical axis is the sum of squared Energy Spectral Density (ESD) at each frequency.
Results of this study will help to address challenges in the design of a hand-controller that can be used inside a magnet bore for evaluating brain activity as it relates to the performance of neurosurgical tasks. It is believed that implementing the results in the design of this haptic hand-controller will allow surgeons to experience a virtual environment similar to real neurosurgery. The challenges addressed are (i) confined space within magnet bore, (ii) workspace required to perform the tasks, and (iii) fidelity of interaction. Other challenges, outside the scope of this paper, include MR-compatibility and/or MR-safety to be addressed in the design process [17, 18]. This paper is also an extension to the studies previously conducted by the authors [19] to quantify positional and surgical force data (magnitude and working frequency) during four cases of robot-assisted neurosurgical operation using the neuroArm surgical manipulators [5, 20].
This paper is organized as follows. Experimental setup and task procedure are described in Sect. 2, followed by results and discussions in Sect. 3. Conclusions are outlined in Sect. 4.
Design of experiment
Test setup
The operation room setup is illustrated in Fig. 1. As observed, a six Degree-of-Freedom (DOF) electromagnetic tracker device (Polhemus Fastrak®, USA) was attached to the proximal end of the bipolar forceps. The tracking system consisted of a main processor that was connected to both receiver and transmitter. The receiver measures the magnetic field generated by the transmitter. Both processor and transmitter were positioned underneath the operating table during the experiment, and the receiver was attached to the bipolar forceps proximal end with velcro and secured by a zip tie (see insets in Fig. 1). The tracker measured the position and orientation of the bipolar forceps proximal end with respect to the reference coordinate system while the surgeon was conducting surgical tasks. The position and orientation were then transferred to the coordinate system attached to the point considered in the middle of the forceps tips, i.e., {xyz} (see Fig. 2).

Surgeon conducting neurosurgical tasks on the cadaveric brain tissue

a Instrumented bipolar forceps is a novel design to measure the interaction forces between the surgical tool and the brain tissue. b Strain gauges S1 to S4 measure the force components along x and y directions, and S5 and S6 measure the forces along z axis
A bipolar forceps (Codman & Shurtleff Inc., MA, USA) was equipped with six strain gauges (three strain gauges on each prong). Configuration of the strain gauges S1 to S6 is depicted in Fig. 2. For each prong, two strain gauges are placed in opposite to each other, and the third pair is located on the bottom of the forceps prong. As observed in Fig. 2, combination of S1 to S4 measures the force components along x and y, and the force component in z direction is measured by S5 and S6 for each prong. Each strain gauge is arranged in a quarter bridge configuration. The output signal of the bridge is then amplified and filtered by a signal-conditioning box. Amplifier’s gain and bias were adjusted such that, along each axis, the polarity of the force signal depends on the direction of the force applied to the forceps tips.
Coordinate systems
Orientation of the bipolar forceps is defined by three components: azimuth (\(\psi\)), elevation (\(\theta\)), and roll (\(\varphi\)). As shown in Fig. 3, the three angles state the current orientation of the frame {xyz} with respect to the world coordinate system {XYZ}. Three displacements (x,y,z) were also considered along X, Y and Z axes to represent the displacement of forceps tips with respect to the frame {XYZ}. In general, the position and the orientation of the bipolar forceps tips are introduced by three translational (x, y, z) and three rotational (\(\psi\), \(\theta\), \(\varphi\)) components. The transition coordinate systems (X′, Y′, Z′) and (X″, Y″, Z″) represent directions of {XYZ} after the rotation by azimuth angle (\(\psi\)) about \(Z\) axis and the elevation angle (\(\theta\)) about Y′ axis, respectively.

Coordinate system attached to the forceps tips, {xyz}, with respect to the world frame {XYZ}
Test procedure
A cadaver head was obtained through the Body Donation Program within the Department of Anatomy at the University of Calgary. A set of neurosurgical tasks were completed by an experienced surgeon as the primary surgeon (GS), and one assistant surgeon. The instrumented bipolar forceps was used by the primary surgeon to perform 35 neurosurgical tasks (320 trials) over 1000 s of practicing on a cadaver. Cadaveric brain was practiced to quantify the position and orientation of a bipolar forceps as well as the interaction force between the forceps tips and the brain tissue. After a frontotemporal craniotomy on the cadaver head, an incision was made on the dura, exposing brain tissue. The surgeons then began performing the surgical tasks surrounding different brain structures, including dissection of arachnoid sylvian tissue (23 trials), dissection of middle cerebral artery (17 trials), coagulating temporal stem (34 trials), coagulating pia arachnoid (13 trials), coagulating pia arachnoid along superior temporal gyrus (12 trials), dissection of corpus callosum (22 trials), crunching third cranial nerve (10 trials), dissection of inter-hemispheric fissure (19 trials) and coagulating choroid plexus (22 trials).
Analysis of data
Time domain analysis
Typical position and orientation components of the bipolar forceps tip over a period of 100 s of surgery are illustrated in Fig. 4a, b, respectively. For this typical time interval, ranges of the forceps tip motion (difference in maximum and minimum positions) were 13.2, 21.1, and 15.9 mm along the X, Y and Z axes. Moreover, the forceps ranges of orientation (difference in maximum and minimum orientations) were 11.9° (\(\psi\), azimuth), 22.1° (\(\theta\), elevation) and 9.3° (\(\phi\), roll). The interaction force components and total force are also shown in Fig. 4c.

Typical ranges of a linear displacements (x, y, z), b angular displacements (\(\psi ,\,\theta ,\,\phi\)), and c interaction force components (F x , F y , F z ) and resultant force (F) over 100 s of neurosurgery
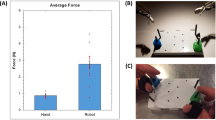
Table 1 presents mean values and standard deviation (SD) of position, orientation, velocity, and force components of the bipolar forceps over a period of 1000 s of surgery. For the practiced cadaver, results indicated that the bipolar forceps travelled within a workspace of 50.1 × 39.8 × 58.2 mm3 along X, Y and Z axes. Results also showed, a range of 40.4°, 60.1° and 63.1° for the azimuth (\(\psi\)), elevation (\(\theta\)), and roll (\(\phi\)) angles, respectively. Peak values of the forceps orientations are also presented in Table 1. Moreover, peak force components of F x = 1.4 N, F y = 2.9 N and F z = 3.0 N along X, Y and Z axes were observed.
Frequency domain analysis
The logged force and position signals in three directions are sampled at 120 Hz that is a proper sampling rate to extract the required frequency range for hand-controller design, especially in the low frequency range where most of tool-tissue interactions occur [15]. To quantify the frequency band of the tool displacement and force, the DFT of each position, orientation, and force signals were calculated, and energy components at each frequency were added as the vectorial magnitude. The vertical axis is therefore the sum of squared ESD at each frequency. Dimensionally reduced periodograms of force signals of each prong are depicted in Fig. 5a, b. The plots show that major frequency contents of different neurosurgical tasks occurred in the frequency range of up to 5 Hz. The Root Mean Square (RMS) analysis of the entire signal also verified that the signal was dominant in this range. Dimensionally reduced periodograms of position and orientation signals are illustrated in Fig. 5c, d, indicating that major frequency contents for position and orientation of different surgery tasks occurred in the frequency range of up to 3 Hz.

Dimensionally reduced periodograms of a force at the right prong, b force at the left prong, c position of the forceps tips, and d orientation of the forceps
Conclusions
This paper reported the bands and magnitudes of the workspace required and the force exerted to the brain tissue during the performance of neurosurgical tasks. Components of the forces and displacements were quantified while an experienced neurosurgeon conducted a variety of neurosurgical tasks using an instrumented bipolar forceps retrofitted by a set of strain gauges (to measure force components) and a position tracker (to measure position and orientation components). Results showed positional, rotational and force frequency bands of 3, 3 and 5 Hz, respectively. Three peak forces were quantified along X (1.4 N), Y (2.9 N) and Z (3.0 N) axes. A workspace of 50.1 × 39.8 × 58.2 mm3 as well as orientation ranges of 40.4° (azimuth), 60.1° (elevation) and 63.1° (roll) were required by the surgical tool, in this case study. The reason to acquire force signals with such a high sampling rate is to ensure covering a wide range of frequency with a high resolution and low noise; however, if a new set of sensory system with different sampling rate is to be chosen, the frequency ranges quantified in this study should not change.
The quantified data provide important information for further utilization in the design of a neurosurgery-specific haptic hand-controller. This will include seamless integration of mechanical design and kinematics, selection of positional sensors and actuators, and devise of the control system. Furthermore, narrowing the desired frequency band facilitates in selecting off-the-shelf sensors and actuators, producing a more economical hand-controller. Future work will focus on implementation of the data in the design of such a hand-controller to reflect characteristics of neurosurgical tasks. Therefore, a surgeon can move the haptic hand-controller and perform neurosurgical tasks, while lying supine and donning a radiofrequency coil within the magnet bore. The brain activity of the surgeon will then be assessed during the performance of tasks using functional MRI technique. Another contribution of this paper is to provide surgeons, as the end-users, a better knowledge of minimum requirements for selecting or designing haptic hand-controllers for robot-assisted microsurgical systems. Moreover, the knowledge of the workspace and forces of microsurgery can also have substantial impact in development of new surgical robots as the slave manipulators, when paired with a haptic device.
References
Huettel SA, Song AW, McCarthy G (2009) Functional magnetic resonance imaging, 2nd edn. Sinauer, Sunderland
Khanicheh A, Muto A, Triantafyllou C, Weinberg B, Astrakas L, Tzika A, Mavroidis C (2006) MR compatible ERF driven hand rehabilitation device. J NeuroEng Rehabil 2(24):1–11
Logothetis NK (2008) What we can do and what we cannot do with fMRI. Nature 453:869–878. doi:10.1038/nature06976
Binder JR, Frost JA, Hammeke TA, Cox RW, Rao SM, Prieto T (1997) Human brain language areas identified by functional magnetic resonance imaging. J Neurosci 17(1):353–362
Lawrence DA (1993) Stability and transparency in bilateral teleoperation. IEEE Trans Robot Autom 9(5):624–637
Sutherland GR, Latour I, Greer AD, Fielding T, Feil G, Newhook P (2008) An image-guided magnetic resonance compatible surgical robot. J Neurosurg 62(2):286–293
Sutherland GR, Maddahi Y, Gan LS, Lama S, Zareinia K (2015) Robotics in the neurosurgical treatment of glioma. Surg Neurol Int 6(S2):1–8
Zareinia K, Maddahi Y, Ng C, Sepehri N, Sutherland GR (2015) Performance evaluation of haptic hand-controllers in a robot-assisted surgical system. Int J Med Robot Comput Assist Surg 11(4):486–501
Maddahi Y, Greene M, Gan LS, Hirmer T, L’orsa R, Lama S, Sutherland GR, Zareinia K (2014) Performance evaluation of a surgical telerobotic system using kinematic indices of the master hand-controller. Haptics: neuroscience, devices, modeling, and applications. Springer, Berlin, Heidelberg, pp 167–175
Tavakoli M, Patel RV, Moallem M (2003) A force reflective master-slave system for minimally invasive surgery. In: Proceedings of IEEE/RSJ international conference on intelligent robots and systems (IROS 2003), vol 3, pp 3077–3082
Najafi F, Sepehri N (2008) A novel hand-controller for remote ultrasound imaging. J Mechatron 18(10):578–590
Nathoo N, Cavuşoğlu MC, Vogelbaum MA, Barnett GH (2005) In touch with robotics: neurosurgery for the future. J Neurosurg 56(3):421–433
Gan LS, Zareinia K, Yang FW, Maddahi Y, Lama S, Sutherland GR (2015) Quantification of forces during neurosurgical procedures. J World Neurosurg 84(2):537–548
Wang KC, Grant K, Gan LS, Zareinia K, Lama S, Sun Q, Sutherland GR, Maddahi Y (2015) Development of an instrumented surgical setup for quantifying displacement and force in surgical dissection. In: Proceedings of ASME international mechanical engineering congress and exposition. Houston, Texas, USA
Romano JM, Yoshioka T, Kuchenbecker KJ (2010) Automatic filter design for synthesis of haptic textures from recorded acceleration data. In: IEEE international conference robotics and automation (ICRA)
Landin N, Romano JM, McMahan W, Kuchenbecker KJ (2010) Dimensional reduction of high-frequency accelerations for haptic rendering. Haptics: generating and perceiving tangible sensations. Lect Notes Comput Sci 6192:79–86
Chinzei K, Bikinis R, Joules FA (1999) MR compatibility of mechatronic devices: design criteria. Lect Notes Comput Sci 1679:1020–1030
Gassert R, Vanello N, Chapuis D, Hartwig V, Scilingo E, Bicchi A, Landini L, Burdet E, Bleuler H (2006) Active mechatronic interface for haptic perception studies with functional magnetic resonance imaging: Compatibility and design Criteria. In: IEEE international conference robotics and automation (ICRA)
Maddahi Y, Gan LS, Zareinia K, Lama S, Sepehri N, Sutherland GR (2015) Quantifying workspace and forces of surgical dissection during robot-assisted neurosurgery. Int J Med Robot Comput Assist Surg. doi:10.1002/rcs.1679
Sutherland GR, Lama S, Gan LS, Wolfsberger S, Zareinia K (2013) Merging machines with microsurgery: clinical experience with neuroArm. J Neurosurg 118(3):521–529
Acknowledgments
The work was supported by grants from Canada Foundation for Innovation, Western Economic Diversification, and Alberta Advanced Education and Technology. Yaser Maddahi would like to particularly thank the Killam Trusts, whose provision of a Killam Postdoctoral Fellowship provided the requisite time to work on this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were performed with approval from the Conjoint Health Research Ethics Board (CHREB) of the University of Calgary. The cadaver head was obtained through the Body Donation Program, Department of Anatomy at the University of Calgary, Alberta, Canada.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Maddahi, Y., Ghasemloonia, A., Zareinia, K. et al. Quantifying force and positional frequency bands in neurosurgical tasks. J Robotic Surg 10, 97–102 (2016). https://doi.org/10.1007/s11701-016-0561-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11701-016-0561-4