
Abstract
Purpose
Floppy eyelid syndrome (FES) is a clinical entity characterized by palpebral hyperlaxity and chronic conjunctivitis. Patients’ eyelids evert (“flip inside out”), leading to eye irritation, dryness, grittiness, and tearing. More severe cases can lead to significant ocular complications, such as keratoconus and impaired eyesight. Research has revealed an association between FES and obstructive sleep apnea syndrome (OSAS). OSAS is also one of the most common comorbidities among patients with obesity and an indication for bariatric surgery. This is one of the first studies to explore FES in a group of patients who have undergone bariatric surgery.
Materials and Methods
This was a retrospective study. A total of 88 patients completed a survey by mail or telephone. Additional data on demographics and baseline preoperative clinical information was extracted from the online medical records and the MBSAQIP database.
Results
Thirty-nine patients (44%) recalled having chronic ocular symptoms before their bariatric surgery, among whom six reported palpebral laxity and/or an established diagnosis of FES. The majority of them (67%) rated their symptoms postoperatively as “somewhat” or “significantly improved.” The patients that reported improvement in their ocular symptoms also experienced an improvement in their OSAS severity.
Conclusion
Bariatric surgery might affect the clinical course of FES and the severity of symptoms. Treating OSAS, the underlying mechanism of FES, is a possible mechanism of how bariatric surgery can help patients. It is also critical for bariatric surgeons to consider FES when patients with obesity, particularly those with OSAS, present with chronic eye symptoms.
Graphical Abstract

Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Floppy eyelid syndrome is a palpebral laxity disorder that Culbertson and Ostler first described in 1981 [1]. It is characterized by the presence of a lax (“floppy”) upper eyelid that everts spontaneously during sleep, although the lower lid can be affected too. This nocturnal eyelid eversion and subsequent conjunctival exposure can lead to chronic conjunctivitis [1]. In addition, physical irritation of the ocular surface by eye rubbing and repetitive microtrauma has been proposed as one possible mechanism contributing to the pathogenesis of FES keratoconjunctivitis [2]. Eyelid hyperlaxity has also been associated with a higher risk of severe ocular surface disease symptoms [3], including corneal dryness [4].
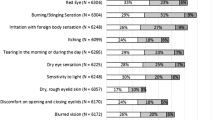
The prevalence of FES among adults has been estimated to fall between 3.8 and 15.8% [3, 4]. However, this disorder remains largely underdiagnosed, and therefore, the aforementioned numbers are likely an underestimation. FES is a syndrome of tarsal papillary conjunctivitis. Hence, patients can present with eye redness, foreign body sensation, tearing, mucus discharge, and/or blurred vision. Symptoms are usually worse in the morning upon waking up and can be either unilateral or bilateral. Notably, symptoms are often more pronounced on the side the patient usually sleeps [5]. Various ocular findings have been associated with FES, including blepharitis, entropion, ectropion, dermatochalasis, corneal scarring/ulceration [6], and keratoconus [7, 8].
Even though the pathophysiology and underlying mechanism of FES are not yet fully elucidated, previous research has revealed an association between FES and obstructive sleep apnea syndrome (OSAS) [9]. FES and OSAS share important risk factors, namely male gender and obesity. The prevalence of OSAS in patients with FES has, in fact, been estimated to be as high as 90–100% [2]. OSAS is a well-known comorbidity of patients with obesity [10] and is one of the indications for bariatric surgery referral, according to the American Society for Metabolic and Bariatric Surgery (ASMBS). Studies exploring the association between FES and obesity have generated mixed results. One study showed an increased lid hyperlaxity in patients with OSAS and high BMI compared to patients with OSAS and low BMI [6]. Another study demonstrated no association between FES and BMI [6]. To our knowledge, this study is one of the first to explore the prevalence of FES in bariatric patients and examine the potential effect of bariatric surgery on FES symptoms. Based on the background described above, our working hypothesis was that bariatric surgery might lead to improvement or resolution of FES.
Materials and Methods
We sought to obtain retrospective data from patients who underwent bariatric surgery at Beth Israel Deaconess Medical Center (BIDMC) between January 1, 2016, and December 31, 2021. All patients were 18 years or older at the time of the surgery. A survey packet, including the prospective agreement, the survey questionnaire, and a pre-stamped envelope for returning the completed material to the researchers, was mailed to the patients. The survey was prepopulated, and unique identifier codes were used to ensure anonymity. Telephone follow-up was conducted for patients that had neither returned a completed survey nor refused participation. The survey elicited information about patients’ demographics, self-reported eye symptoms preoperatively, and postoperative symptom evolution (Table 1). Additional clinical information, including baseline (preoperative) comorbidities (Table 2), was abstracted from the Metabolic and Bariatric Surgery Accreditation and Quality Improvement (MBSAQIP) database.
While we extensively reviewed the existing literature and the work of researchers that have studied FES, we found no standardized questionnaires for this particular group of patients. Therefore, we decided to structure our survey in a way that could help us collect key anamnestic details and findings that may suggest the diagnosis of FES. We asked patients to reflect on the 6 months prior to their weight loss surgery and to respond whether they had, more often than not, symptoms suggestive of FES, including eye redness, grittiness, dryness, and mucus discharge. We also asked about the localization of symptoms (unilateral versus bilateral) and when these were more pronounced (upon waking up/throughout the day/towards the end of the day). We included more direct questions as well, asking patients whether they had ever noticed (or had been told) their eyelids were “floppy” and whether they were diagnosed with FES prior to surgery. Finally, we asked patients to reflect on how their eye symptoms have changed after their weight loss surgery (significantly improved/somewhat improved/no change/somewhat worsened/significantly worsened). The full questionnaire is included in Fig. 1.


Questionnaire
Results
In total, 88 patients completed the survey, 31 by mail and 57 by phone. An additional 24 patients could not be contacted due to changes in their contact information that were not updated on our records, while 7 refused participation. The respondents’ demographics and baseline (preoperative) comorbidities can be seen in Tables 1 and 2, respectively. The mean age was 48.4 years. The mean body mass index (BMI) was 44.7 preoperatively and 33.3 postoperatively (ΔΒΜΙ = − 11.4, mean % excess weight loss (%EWL) = 57.8). The mean weight reduction was 27.3 kg (60.2 lbs). Thirty-nine patients recalled having at least one ocular symptom, more often than not, in the period immediately prior to their bariatric surgery, with more than half of these patients (24 patients) reporting seeing an ophthalmologist for their ocular symptoms. Among these 39 patients, three had noticed and/or had been told that their eyelids felt “loose”/flipped over (Fig. 2) during sleep, two had both noticed/had been told that their eyelids felt “loose” and had been diagnosed with FES, and one had been diagnosed with FES, without self-reporting having “loose” eyelids. As this is a retrospective study, patients recall that having “loose,” floppy eyelids and/or a diagnosis of FES was the strongest information we could rely on to assume that these patients possibly had the syndrome. Of these six patients, three were women, and three were men.

Flipped eyelid
Five patients reported suffering from OSA before their surgery; four also used a sleep apnea machine. Regarding their postoperative state, three patients evaluated both their OSA and their ocular symptoms as “significantly improved,” one as both conditions “somewhat improved,” and one responded that there had been no change in the severity of their OSA, while their eye symptoms had “significantly worsened” (Table 3). One patient, who had no prior diagnosis of OSA, reported no change in their ocular symptoms (Table 3). Notably, a patient commented that his desire to improve his FES symptoms was one of the reasons he decided to have bariatric surgery, as their physician advised. Of the remaining 33 patients who recalled chronic ocular symptoms before surgery but had not observed eyelid laxity nor had a diagnosis of FES, 19 responded that they had seen no change in their symptoms after surgery. Four evaluated them as “somewhat improved” and three as “significantly improved.” In contrast, four other patients reported that their ocular symptoms have “somewhat worsened,” and one patient reported them as “significantly worsened.” Two patients did not fill out the survey section regarding their postoperative outcomes. Although many of these patients describe symptom profiles that could be attributed to FES, it would be precarious to assume so. In many cases, the symptoms could be due to dry eye syndrome or a particular subset of this named Sjögren’s syndrome.
Discussion
This is the first study to our knowledge that explores FES in a group of bariatric patients. FES is an important and relatively common cause of ocular irritation. Nevertheless, it can be easily misdiagnosed in clinical practice. As discussed above, even though FES has not been linked directly to obesity, it is strongly associated with OSAS, with the majority of patients with FES suffering from OSAS.
The mechanism of FES is not well understood. One hypothesis to explain the association between FES and OSAS is that chronic sleep fragmentation, microtrauma [11], and alternating states of tissue ischemia and reperfusion [12], as seen in OSAS, can lead to overexpression of elastolytic proteases (e.g., matrix metalloproteinases) and subsequently loss of elastin and hyperlaxity of the palpebral tissue [13]. In addition, a case–control study revealed that FES patients were more likely to suffer from conditions related to metalloproteinase dysfunction (e.g., hernias, dermatologic, or rheumatological diseases), suggesting that they might represent a unique phenotype among patients presenting with OSA [14]. As many of these proteases depend on cofactors such as metal ions, it is worth mentioning that none of the six patients with FES had any nutritional deficiencies, according to their medical records. All six took standard multivitamin supplements, as noted in their medication list. Furthermore, a decrease in cortical arousability and reflex response to noxious stimuli can be seen in patients with OSAS. This feature may exacerbate mechanical injury to palpebral tissue during sleep as the patient can often tolerate significant mechanical stress that would have normally prompted the individual to wake up and reposition [7]. Interestingly, the use of continuous positive airway pressure (CPAP) therapy in patients with OSAS resulted in an improvement of their FES symptoms when these were also present [2, 15]. This reinforces the likely causal relationship between OSAS and FES.
OSAS is highly prevalent among populations with obesity and is an indication for bariatric surgery for patients with a BMI of 35 or higher. Weight loss surgery has been shown to improve or lead to complete resolution of OSAS, with postsurgical remission in as many as 80% of the cases [16]. This raises the question of whether bariatric surgery has an effect on FES symptoms. Although the design of our study does not allow us to reach definitive conclusions, our findings can be considered hypothesis-generating. Additional research is needed to examine whether improvement of FES is one of the benefits a patient can anticipate after their weight loss surgery (WLS). Improvement of FES could indirectly be linked to bariatric surgery by improving OSA severity.
A correlation might also exist between FES and leptin hormone levels. A case series showed that plasma leptin levels were elevated in FES patients, implying that hyperleptinemia might play a role in FES pathogenesis [17]. Although leptin is primarily produced by adipocytes, the stomach is another identified production site [18]. In this context, bariatric surgery, which alters the stomach anatomy, might affect FES through mechanisms related to leptin. More data are warranted.
The small number of patients with potential or diagnosed FES we identified in this study does not allow for further correlation analysis. However, the relationship between bariatric surgery and FES, as well as risk factors and predictive markers, are likely to be further elucidated as research continues to shed light on the pathophysiology of FES. We also hope that this effort will help raise awareness about FES among medical professionals. Many specialists, including ophthalmologists, sleep physicians, and bariatric surgeons, should keep a high level of suspicion and refer these patients to appropriate resources for further evaluation and treatment.
Limitations
We acknowledge that our study presents a number of limitations. First of all, due to our retrospective design, the risk of recall bias cannot be excluded. We relied on a self-reported diagnosis of FES and/or history of eyelid laxity, but we cannot exclude nor confirm the presence of FES among the rest of the patients reporting chronic eye symptoms. Furthermore, there is a risk of selection bias, as we were not able to contact all patients due to changes in contact information that were not updated properly in our patient records. Finally, our survey included patients from a single WLS center in Boston, and the patients who responded had all undergone sleeve gastrectomy. Therefore, the generalizability of our findings is limited.
Conclusions
FES is a common yet underdiagnosed condition that can be associated with significant ocular symptoms. Therefore, it is critical to consider FES when patients with high BMI, particularly those with OSA, present with nonspecific ocular symptoms, such as eye irritation. The present study explores the possible effects of bariatric surgery on FES symptoms. Further research, including prospective studies with patients with an established diagnosis of FES, is needed and will allow for more definitive conclusions.
Data Availability
The data supporting this study's findings are available on request from the corresponding author, TZ. The data are not publicly available due to containing information that could compromise the privacy of research participants.
References
Culbertson WW, Ostler HB. The floppy eyelid syndrome. Am J Ophthalmol. 1981;92:568–75.
Salinas R, Puig M, Fry CL, et al. Floppy eyelid syndrome: a comprehensive review. Ocul Surf. 2020;18:31–9.
Ansari Z, Singh R, Alabiad C, et al. Prevalence, risk factors, and morbidity of eye lid laxity in a veteran population. Cornea. 2015;34:32–36 Preprint at https://doi.org/10.1097/ico.0000000000000286.
Chhadva P, et al. Impact of eyelid laxity on symptoms and signs of dry eye disease. Cornea. 2016;35:531–5.
Leibovitch I, Selva D. Floppy eyelid syndrome: clinical features and the association with obstructive sleep apnea. Sleep Med. 2006;7:117–22.
Beis PG, et al. The floppy eyelid syndrome: evaluating lid laxity and its correlation to sleep apnea syndrome and body mass index. ISRN Ophthalmol. 2012;2012:650892.
Ezra DG, et al. The associations of floppy eyelid syndrome: a case control study. Ophthalmology. 2010;117:831–8.
Culbertson WW, Tseng SC. Corneal disorders in floppy eyelid syndrome. Cornea. 1994;13:33–42.
Wang P, et al. Is floppy eyelid syndrome more prevalent in obstructive sleep apnea syndrome patients? J Ophthalmol. 2016;2016:6980281.
Senaratna CV, et al. Prevalence of obstructive sleep apnea in the general population: a systematic review. Sleep Med Rev. 2017;34:70–81 Preprint at https://doi.org/10.1016/j.smrv.2016.07.002.
Schlötzer-Schrehardt U, et al. The pathogenesis of floppy eyelid syndrome: involvement of matrix metalloproteinases in elastic fiber degradation. Ophthalmology. 2005;112:694–704.
Lindsey M, et al. Matrix-dependent mechanism of neutrophil-mediated release and activation of matrix metalloproteinase 9 in myocardial ischemia/reperfusion. Circulation. 2001;103:2181–7.
Cristescu Teodor R, Mihaltan FD. Eyelid laxity and sleep apnea syndrome: a review. Rom J Ophthalmol. 2019;63:2–9.
Nijjar M, Kotoulas S-C, Kerr J, Riha RL. Floppy eyelid syndrome and obstructive sleep apnea: a unique phenotype? Sleep Breath. 2022. https://doi.org/10.1007/s11325-022-02690-3.
McNab AA. The eye and sleep. Clin Exp Ophthalmol. 2005;33:117–25.
Sarkhosh K, et al. The impact of bariatric surgery on obstructive sleep apnea: a systematic review. Obes Surg. 2013;23:414–23.
Taban M, Taban M, Perry JD. Plasma leptin levels in patients with floppy eyelid syndrome. Ophthal Plast Reconstr Surg. 2006;22:375–7.
Muruzábal FJ, Frühbeck G, Gómez-Ambrosi J, et al. Immunocytochemical detection of leptin in non-mammalian vertebrate stomach. Gen Comp Endocrinol. 2002;128:149–52.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics Approval and Consent to Participate
The study was approved by institutional review boards (IRB) at BIDMC. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Conflict of Interest
Dr. Daniel Jones is a member of the advisory board of Allurion Technologies.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Key Points
• Floppy eyelid syndrome (FES) is a common yet underdiagnosed clinical entity.
• FES is related to obstructive sleep apnea, which also affects bariatric patients.
• The present study is one of the first to explore FES among bariatric patients.
• This study aims to raise awareness of FES among bariatric surgeons.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Zoumpou, T., Samuel, S., Torun, N. et al. Floppy Eyelid Syndrome: an Overlooked Comorbidity Among Bariatric Patients. OBES SURG 33, 523–529 (2023). https://doi.org/10.1007/s11695-022-06410-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-022-06410-4