
Abstract
Background
Obesity is commonly associated with increased sympathetic tone, changes in heart geometry, and mortality. The aforementioned translates into a higher and potentially modifiable mortality risk for this specific population.
Objectives
The aim of the study was to analyze the extent of changes in the heart ventricular structure following rapid weight loss after bariatric surgery.
Setting
Academic, university-affiliated hospital.
Methods
We retrospectively reviewed all the patients that underwent bariatric surgery at our institution between 2010 and 2015. Data analyzed included demographics, BMI, and associated medical problems. Preoperative and postoperative echography readings were compared looking at the heart geometry, cardiac volumes, and wall thickness.
Results
Fifty-one patients who had bariatric surgery and had echocardiography before and after the surgery were identified. There were 33 females (64.7%). The mean age was 63.4 ± 12.0 years with an average BMI of 40.3 ± 6.3. The mean follow-up was 1.2 years after the procedure. At 1 year follow-up 25 patients (49%, p = 0.01) showed normal left ventricular geometry. The left ventricular mass (229 ± 82.1 vs 193.2 ± 42.5, p<0.01) and the left ventricular end diastolic volume (129.4 ± 53 vs 96.4 ± 36.5, p = 0.01) showed a significant modification following the procedure. There was a significant improvement in the interventricular septal thickness (p = 0.01) and relative wall thickness (p < 0.01) following surgery.
Conclusion
The patients with obesity present a significant cardiac remodeling from concentric remodeling to normal geometry after bariatric surgery. The decrease in BMI has a direct effect on improvement of the left ventricular structure. Further studies must be carried out to define the damage of obesity to diastolic function.
Graphical Abstract

Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The World Health Organization recognizes obesity as one of the most underestimated public health problems [1, 2]. The number of deaths related to its many complications keeps rising exponentially. The highest ranked cause of death in patients with obesity is cardiovascular disease, commonly associated with alterations in cardiac structure and hemodynamics [2]. The heart of a patient with obesity sustains many changes in order to adapt to the challenges of metabolic syndrome by undergoing remodeling, resulting in left ventricle hypertrophy, dilation and atrial changes, and leading eventually to heart failure [3, 4]. Similarly, increased left ventricular wall thickness (LVWT), chamber size, left ventricle mass (LVM), and systolic and diastolic dysfunction, all of which are prevalent abnormalities in patients with obesity, have been proven to be independent risk factors for cardiovascular disease [3, 5, 6]. The aforementioned plus an increase in sympathetic activity translates into a higher and potentially modifiable mortality risk for this specific population [7, 8].
Bariatric surgery has been recognized as the most effective and durable intervention in patients with severe obesity and metabolic syndrome. In addition to the reduction in BMI, it has shown remarkable effects in the control and resolution of obesity-related medical problems, such as diabetes, hypertension, and dyslipidemia [9, 10]. In the same fashion, growing evidence suggests that weight reduction also has an impact on heart geometry, especially by reducing LVM and improving LV dimensions [11,12,13]. However, other authors have not been able to show a significant improvement in heart function after weight loss, which is why the literature remains inconclusive [14].
The aim of this study is to analyze the extent of changes in the heart ventricular function, structure, and dimensions following bariatric surgery.
Methods
After the institutional review board (IRB) approval, we retrospectively reviewed our prospectively collected electronic database of all the patients who underwent bariatric surgery from December 2010 to December 2015 at our institution. All the patients that had bariatric surgery and also had an echocardiogram before and after the surgery were included. All the other patients were excluded. Echocardiogram parameters were obtained based on the comprehensive guidelines and recommendations from the American Society of Echocardiography in adults. [15] We do not routinely obtain echocardiograms before and after bariatric surgery at our institution. However, as part of the preoperative evaluation and clearance, the cardiologists might request echocardiograms, based on patients’ associated medical problems and risk factors.
The data collected included patient’s common demographics (age and gender), BMI, and associated medical problems (hypertension, diabetes mellitus type 2, hyperlipidemia, gastro esophageal reflux disease, and obstructive sleep apnea). The preoperative and postoperative echocardiography readings were compared. All the preoperative echocardiograms were abnormal. Abnormal echocardiograms were defined as those with at least one measurement out of the standard normality range. The data used for comparison from echocardiography readings included heart rate, aortic root diameter, left atrial systolic diameter, left ventricular mass, posterior wall thickness, relative wall thickness, inter-ventricular septal thickness, left ventricular systolic volume, left ventricular end systolic diameter, left ventricular end diastolic diameter, left ventricular end systolic volume, and left ventricular ejection fraction. Primary measures were taken from the two-dimensional views in accordance with the recommendations of the American Society of Echocardiography.
Data Analysis
The data was collected from the patient chart review and imported into JMP software (SAS Institute Inc., NC, USA), which was then used to apply variable formatting and change variable names to conform to the conventions needed for R (software R, version 3.3.1 (2016-06-21), R Foundation for Statistical Computing, Vienna, Austria). Data was described using mean and standard deviation for continuous variables and counts and percentages for categorical variables.
Outcomes of clinical characteristics and postoperative results were described using the chi-square, Fisher exact, and t-tests. Sample sizes for individual variables reflect missing data. All the analyses were performed on a complete-case basis. All the tests were two-tailed and performed at a significant level of 0.05. Statistical software R, version 3.3.1 (2016-06-21), was used for all the analyses.
Results
From 1129 bariatric patients reviewed, 51 patients who had bariatric procedures and had an echocardiography before and after the surgery were identified. We observed a predominant female population, which composed 64% (N = 33) of our included patients. The average age for females was 63.4 ± 12.0 years. The average BMI was 40.3 ± 6.3 at the time of bariatric surgery and 31.8 ± 5.8 at 1-year follow-up. Laparoscopic sleeve gastrectomy (LSG) was the most prevalent surgery at 51.0% (N = 26), followed by LRYGB 23.5% (N = 12), 15.6% gastric bands (N = 8), and 9.8% revisions (N = 5). Type 2 diabetes mellitus was diagnosed in 76.4% (N = 39) of our patients with a resolution of 30.7% at follow-up. Hypertension was found in 84.3% (N = 43) with a resolution of 30.2% at follow-up. The mean follow-up was 1.2 years post-procedure (Table 1).
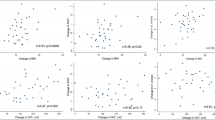
At 1-year follow-up, 25 patients showed normal left ventricular geometry (p = 0.01). The left ventricular mass and the left ventricular end diastolic volume showed significant modification following the procedure (p < 0.05 and p = 0.01, respectively). Comparably, there was a significant modification in the interventricular septal thickness and relative wall thickness following surgery (p = 0.01 and < 0.01, respectively). Although not statistically significant, volume measures as left ventricular systolic volume and left ventricular end systolic volume also showed considerable improvement. Similarly, dimension measurements such as left ventricular end systolic diameter and left ventricular end diastolic diameter showed extensive improvements (3.1 ± 0.7 vs 3 ± 0.7, p = 0.9, 95% Cl, and 4.8 ± 0.7 vs 4.6 ± 0.6, p = 0.1, 95% Cl, respectively) (Table 2). Finally, the percent total weight loss (%TWL) was 22.9 ± 17.4%.
Discussion
The plasticity of pathologic changes observed in heart geometry with different levels of weight loss has been a topic of discussion for over a decade [16]. Many of the cardiovascular alterations seen in patients with obesity, regardless of age, are related to excess body fat and its consequent increase in volume and overload, resulting in eccentric or concentric hypertrophy [17, 18]. The present study shows that the heart is able to regress many of the adaptive changes it undergoes as compensation for the overload state caused by the obesity disease following bariatric surgery and sustained weight loss. Throughout the years, many authors have been trying to show and describe the many metabolic improvements accomplished for this specific population after bariatric surgery [19, 20]. In previous studies, we reported the benefits of rapid weight loss, including remission of hypertension and diabetes, marked reduction of cardiovascular risk, improvement of chronic kidney disease, and regression of hepatic steatosis [9, 10, 21]. The vast majority of these alterations correlate to each other, creating a net of changes that ultimately affect the remodeling of the heart.
The chronic volume overload and hypertension in patients with obesity usually leads to compensatory mechanisms, which modify the structure of the heart. These modifications typically induce left ventricular enlargement, hypertrophy, and, as result, significant changes in the hemodynamic function of the heart [22].
The metabolic effects of bariatric surgery seem to improve the hemodynamic parameters by decreasing the inflammatory state that induces ventricular hypertrophy. Excessive weight loss can lead to a significant reduction in LV dimensions after 3–36 months and even after 10 years [22]. This is consistent with our study that showed a significant improvement in cardiac geometry at 12 months of follow-up. However, the beneficial cardiac geometry changes after metabolic surgery are likely multifactorial and not only related to the weight loss. In fact, %TWL seems to be lower than expected, probably due to the older age of the study population (63 ± 12 years old), the inclusion of lower weight loss procedures (gastric banding and revisional surgery) and, possibly, the short=term follow=up (1 year). Cardiac remodeling following bariatric surgery is influenced by the reduction in gastric size, anatomical gut rearrangement, vagal manipulation, and enteric gut hormone changes [22].
In the study conducted by Garza et al. on 57 patients who underwent gastric bypass, the authors found a significant change in echocardiographic parameters after a mean follow-up of 3.6 years. The authors also showed that neither LV nor RV function change significantly after weight loss, but the structural changes following weight loss led to an improved RV end diastolic area which could prevent the progression to RV dysfunction [23]. This study also included a control group of patients who did not undergo bariatric surgery. The control group, on the other end, presented a worsening trend of the same echocardiographic parameters during the study period. Although a shorter follow-up time was assessed in our study, these results support the heart geometry improvement that we found in our group of patients.
Rocha et al., in her study of 23 patients with obesity, reported a decreased width of the ventricular septum and LV posterior wall, and an increase in LV diastolic dimension [4]. In a similar manner, we were able to demonstrate a considerable and statistically significant reduction in the posterior wall thickness, relative wall thickness, and interventricular thickness, evidencing a solid remodeling through regression of concentric hypertrophy. These favorable changes are probably due to the progressive regulation of the sympathetic tone and the normalization of the cardiac load that happens after bariatric surgery, allowing heart cavities to return to their original dimensions [24]. LV mass was related to changes in both BMI and visceral adiposity as reported by Shin and colleagues, contributing to the observed changes in our population [16]. Equally important, the atrial cavity has been acquiring an important role in the pathophysiology of cardiovascular adaptations of heart geometry [25]. Previous publications have shown that there is a correlation between periatrial pericardial fat accumulation and left atrial diameter, increasing the rate of cardiac arrhythmias as atrial fibrillation [25, 26]. In this study, we were able to show how bariatric surgery also modifies the atrial cavity, evidencing a significant improvement in the left atrial cavity, correlated with a decrease of the left atrial systolic diameter. The change in the atrial cavity potentially corresponds in part to the decreased periatrial fat and the decreased atrial diameter, which is potentially the result of a decrease in the overload state of this population. In light of this information, the necessity to further study the direct correlation between the specific atrial changes and their subsequent effects and arrhythmogenic potential becomes paramount. Taking into account the aforementioned variables prevalently altered in patients with obesity, our population is immediately placed at an even higher cardiovascular risk. The structural changes in heart geometry acquired after bariatric surgery allow the heart to return to its normal hemodynamic and electrophysiological state. Therefore, this suggests heart geometry is a key component to explain the marked reduction in cardiovascular risk evidenced in previous studies [9, 27].
The concept of cardiac plasticity has been addressed and studied by multiple scientists. Three predominant mechanisms that would induce heart modifications have been suggested starting for the physiologic myocardial growth propitiated by normal demand [28, 29]. The other two types of changes are associated to pathological states, hypertrophic remodeling as a result of hemodynamic stress, and cardiac atrophy as an adaptation to ventricular unloading [28]. This concept has been applied with the purpose of medically treating the effects of the heart modifications caused by chronic conditions as hypertension, obesity, myocardial infarction, and valvular heart disease. However, multiple medications are needed in order to compensate for the impact of heart geometry in systemic hemodynamics (blood pressure, volume overload, heart rate) [30]. There is no universal medical intervention to address them as a whole. However, bariatric surgery propitiates the changes needed to help reshape heart geometry in order to return to a normal or close-to-normal structure and, consequently, function, hemodynamic, and electrical status [31]. The fact that almost 50% of our population returned to completely normal heart geometry at 1-year follow-up speaks to the plasticity of the human heart and the potential for adaptation when subjected to the appropriate conditions. To the best of our knowledge, this is one of the first studies observing the effects of bariatric surgery on cardiac geometry and plasticity not only reporting improvement but also normalization of cardiac structure after bariatric surgery.
The ejection fraction was available and reviewed in our population, and no statistical significance was found after bariatric surgery. This result was expected given the fact that more than 90% of our patients had preserved ejection fraction before bariatric surgery. In order to acquire statistical significance for the aforementioned analysis, a larger patient population would be needed, and additional variables should be included. Our findings correlate to current literature, reporting that the most common phenotype of heart failure affecting the population with obesity is heart failure with preserved ejection fraction (HFpEF) [32,33,34]. Despite having an increased risk of myocardial infarction, thus increasing the risk of systolic function impairment, this population has a higher risk of developing heart failure independent of ischemic cardiac injury [35]. The aim of our study was to analyze the extent of changes in the heart ventricular structure following rapid weight loss after bariatric surgery, hence the reason why ejection fraction was not directly addressed in the present study. However, we are currently working on analyzing cardiac function in the population with obesity in depth, and we will be presenting our results in the near future.
We acknowledge that the small number of patients, the selection of the population by the availability of preoperative and postoperative echocardiograms, and the fact that all echocardiograms are abnormal before surgery represent weaknesses of our study. These factors, in addition to the short follow-up, limit our ability to perform a meaningful correlation analysis between variables and cardiac geometry changes and, also, to report the long-term effect of our findings. Our study, however, presents several strengths. This is a single institution series, and as such has the benefit of consistency in the preoperative, intraoperative, and postoperative phases of the care of the patients with obesity. Secondly, the series is from a well-established and experienced practice. Differently from other studies, we include a higher percentage of sleeve gastrectomies (51%). Finally, we believe that the evidence presented supports the demonstration of cardiac structural changes in the elderly with several associated medical problems, reinforcing the benefit of metabolic surgery in this patient population.
Understanding the multiple factors involved in the resolution of metabolic syndrome in patients with obesity after bariatric surgery and their impact in heart geometry modification, it is imperative to conduct further and prospective studies to better understand the direct impact of all these factors in the normalization of heart dimensions and its repercussions on heart function.
Conclusion
In conclusion, our results suggest that there is a significant cardiac remodeling from concentric remodeling to normal geometry after bariatric surgery. Bariatric surgery greatly impacts the plasticity of the human heart by propitiating the necessary conditions for structural cardiac re-adaptation. Studies have to be carried out to further define the extent of the damage of obesity to the heart dimensions and function, and the beneficial effects of bariatric surgery.
References
Centers for Disease Control and Prevention. Adult obesity causes & consequences. Overweight Obes. 2018:1–6. https://doi.org/10.1037/e534682011-001.
World Health Organization. Controlling the global obesity epidemic. World Heal Organ. 2015;7:1–2.
Kardassis D, Bech-Hanssen O, Schönander M, et al. The influence of body composition, fat distribution, and sustained weight loss on left ventricular mass and geometry in obesity. Obesity. 2012;20:605–11. https://doi.org/10.1038/oby.2011.101.
Rocha IE, Victor EG, Braga MC, et al. Echocardiography evaluation for asymptomatic patients with severe obesity. Arq Bras Cardiol. 2007;88:52–8. https://doi.org/10.1590/S0066-782X2007000100009.
Artham SM, Lavie CJ, Milani RV, et al. Clinical Impact of left ventricular hypertrophy and implications for regression. Prog Cardiovasc Dis. 2009;52:153–67. https://doi.org/10.1016/j.pcad.2009.05.002.
Brady TM. The role of obesity in the development of left ventricular hypertrophy among children and adolescents. Curr Hypertens Rep. 2016; https://doi.org/10.1007/s11906-015-0608-3.
Thorp AA, Schlaich MP. Relevance of sympathetic nervous system activation in obesity and metabolic syndrome. J Diabetes Res. 2015;2015 https://doi.org/10.1155/2015/341583.
Xiong XQ, Chen WW, Zhu GQ. Adipose afferent reflex: sympathetic activation and obesity hypertension. Acta Physiol. 2014;210:468–78. https://doi.org/10.1111/apha.12182.
Blanco DG, Funes DR, Giambartolomei G, et al. Laparoscopic sleeve gastrectomy versus Roux-en-Y gastric bypass in cardiovascular risk reduction: a match control study. Surg Obes Relat Dis. 2018; https://doi.org/10.1016/j.soard.2018.09.488.
Gutierrez-Blanco D, Romero Funes D, Castillo M, et al. Bariatric surgery reduces the risk of developing type 2 diabetes in severe obese subjects undergoing sleeve gastrectomy. Surg Obes Relat Dis. 2019; https://doi.org/10.1016/j.soard.2018.11.023.
Lakhani M, Fein S. Effects of obesity and subsequent weight reduction on left ventricular function. Cardiol Rev. 2011;19:1–4. https://doi.org/10.1097/CRD.0b013e3181f877d2.
Hinderliter A, Sherwood A, Gullette ECD, et al. Reduction of left ventricular hypertrophy after exercise and weight loss in overweight patients with mild hypertension. Arch Intern Med. 2002;162:1333–9. https://doi.org/10.1001/archinte.162.12.1333.
Cuspidi C, Rescaldani M, Tadic M, et al. Effects of bariatric surgery on cardiac structure and function: a systematic review and meta-analysis. Am J Hypertens. 2014; https://doi.org/10.1093/ajh/hpt215.
Dzenkeviciūte V, Petrulioniene Z, Sapoka V, et al. The effect of weight loss on the cardiac structure and function after laparoscopic adjustable gastric banding surgery in morbidly obese individuals. Obes Surg. 2014;24:1961–8. https://doi.org/10.1007/s11695-014-1294-y.
Mitchell C, Rahko PS, Blauwet LA, et al. Guidelines for performing a comprehensive transthoracic echocardiographic examination in adults: recommendations from the American Society of Echocardiography. J Am Soc Echocardiogr [Internet]. Elsevier Inc; 2019;32:1–64. Available from: https://doi.org/10.1016/j.echo.2018.06.004.
Shin SH, Lee YJ, Heo YS, et al. Beneficial effects of bariatric surgery on cardiac structure and function in obesity. Obes Surg. 2017;27:620–5. https://doi.org/10.1007/s11695-016-2330-x.
Hsuan CF, Huang CK, Lin JW, et al. The effect of surgical weight reduction on left ventricular structure and function in severe obesity. Obesity. 2010;18:1188–93. https://doi.org/10.1038/oby.2010.42.
Luaces M, Martínez-Martínez E, Medina M, et al. The impact of bariatric surgery on renal and cardiac functions in morbidly obese patients. Nephrol Dial Transplant. 2012;27 https://doi.org/10.1093/ndt/gfs529.
Schauer PR, Nissen SE, Kirwan JP, et al. Bariatric surgery versus intensive medical therapy for diabetes — 5-year outcomes. N Engl J Med. 2017; https://doi.org/10.1056/nejmoa1600869.
Sjöström L, Narbro K, Sjöström CD, et al. Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med. 2007;
Cobos MFS, Gomez CO, Funes DR, et al. Ultrasonographic regression of hepatic steatosis after bariatric surgery. Surg Obes Relat Dis. 2018;14:S63. https://doi.org/10.1016/j.soard.2018.09.098.
Lascaris B, Pouwels S, Houthuizen P, et al. Cardiac structure and function before and after bariatric surgery: a clinical overview. Clin Obes. 2018;8:434–43.
Garza CA, Pellikka PA, Somers VK, et al. Structural and functional changes in left and right ventricles after major weight loss following bariatric surgery for morbid obesity. Am J Cardiol [Internet]. Elsevier Inc.; 2010;105:550–6. Available from: https://doi.org/10.1016/j.amjcard.2009.09.057.
Kaier TE, Morgan D, Grapsa J, et al. Ventricular remodelling post-bariatric surgery: is the type of surgery relevant? A prospective study with 3D speckle tracking. Eur Heart J Cardiovasc Imaging. 2014;15:1256–62. https://doi.org/10.1093/ehjci/jeu116.
Owan T, Avelar E, Morley K, et al. Favorable changes in cardiac geometry and function following gastric bypass surgery: 2-year follow-up in the Utah obesity study. J Am Coll Cardiol. 2011;57:732–9. https://doi.org/10.1016/j.jacc.2010.10.017.
Lynch KT, Mehaffey JH, Hawkins RB, et al. Bariatric surgery reduces incidence of atrial fibrillation: a propensity score–matched analysis. Surg Obes Relat Dis. 2019; https://doi.org/10.1016/j.soard.2018.11.021.
Gutierrez-Blanco D, Funes-Romero D, Madiraju SG, et al. Reduction of Framingham BMI score after rapid weight loss in severely obese subjects undergoing sleeve gastrectomy: a single institution experience. Surg Endosc. 2018;32:1248–54. https://doi.org/10.1007/s00464-017-5799-z.
Hill JA, Olson EN. Cardiac Plasticity. N Engl J Med. 2008;358:1370–80. https://doi.org/10.1056/nejmra072139.
Razeghi P, Taegtmeyer H. Hypertrophy and atrophy of the heart: the other side of remodeling. Ann NY Acad Sci. 2006;1080:110–9. https://doi.org/10.1196/annals.1380.011.
Frey N, Katus HA, Olson EN, Hill JA. Hypertrophy of the heart: a new therapeutic target? Circulation. 2004;109:1580–9. https://doi.org/10.1161/01.CIR.0000120390.68287.BB.
Ippisch HM, Inge TH, Daniels SR, et al. Reversibility of cardiac abnormalities in morbidly obese adolescents. J Am Coll Cardiol. 2008;51:1342–8. https://doi.org/10.1016/j.jacc.2007.12.029.
Obokata M, Reddy YNV, Pislaru SV, et al. Evidence supporting the existence of a distinct obese phenotype of heart failure with preserved ejection fraction. Circulation. 2017; https://doi.org/10.1161/CIRCULATIONAHA.116.026807.
Kitzman DW, Shah SJ. The HFpEF obesity phenotype: the elephant in the room. J Am Coll Cardiol. 2016; https://doi.org/10.1016/j.jacc.2016.05.019.
Shah SJ, Kitzman DW, Borlaug BA, et al. Phenotype-specific treatment of heart failure with preserved ejection fraction: a multiorgan roadmap HHS Public Access. Circulation. 2016; https://doi.org/10.1161/CIRCULATIONAHA.116.021884.
Packer M, Kitzman DW. Obesity-related heart failure with a preserved ejection fraction: the mechanistic rationale for combining inhibitors of aldosterone, neprilysin, and sodium-glucose cotransporter-2. JACC Heart Fail. 2018; https://doi.org/10.1016/j.jchf.2018.01.009.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Key points
1. Bariatric surgery and rapid weight loss produce a significant impact on heart geometry.
2. Bariatric surgery results in cardiac remodeling from concentric to normal geometry in patients with obesity.
3. Bariatric surgery improves cardiac plasticity and dynamics in patients with obesity.
Rights and permissions
About this article

Cite this article
Gomez, C.O., Rammohan, R., Romero-Funes, D. et al. Bariatric Surgery Improves Heart Geometry and Plasticity. OBES SURG 32, 1–6 (2022). https://doi.org/10.1007/s11695-022-06016-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-022-06016-w