
Abstract
Background
In obese patients (OP), the best intraoperative ventilation strategy remains to be defined. Dynamic lung compliance (Cdyn) and dead space fraction are indicators of efficient ventilation at an optimal positive end-expiratory pressure (PEEP). Herein, we investigated whether intraoperative dynamic lung compliance optimization through PEEP manipulations affects the incidence of postoperative hypoxemia (SpO2 < 90%) in OP undergoing laparoscopic bariatric surgery (LBS).
Methods
This was a single-center, prospective, randomized controlled study conducted from July 2013 to December 2015. After obtaining institutional review board approval and informed consent, 100 OP undergoing LBS under volume-controlled ventilation (tidal volume 8 mL/kg of ideal body weight) were randomized according to the PEEP level maintained during the surgery. In the control group, a PEEP of 10 cm H2O was maintained, while in the intervention group, the PEEP was adapted to achieve the best dynamic lung compliance. Anesthesia and analgesia were standardized. The patients received supplemental nasal oxygen on the first postoperative day and were monitored up to the second postoperative day with a portable pulse oximeter.
Results
Demographics were similar between groups. There was no difference in the incidence of hypoxemia during the first 2 postoperative days (control: 1.3%; intervention: 2.1%; p = 0.264).
Conclusions
The incidence of postoperative hypoxemia was not reduced by an open-lung approach with protective ventilation strategy in obese patients undergoing LBS. A pragmatic application of a PEEP level of 10 cm H2O was comparable to individual PEEP titration in these patients.
Trial Registration
Clinicaltrials.gov identifier, NCT02579798; https://clinicaltrials.gov/ct2/show/NCT02579798
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Pulmonary atelectasis, which occurs in 85–90% of healthy adults within minutes of general anesthesia (GA) induction, remains the main cause of increased intrapulmonary shunt during and after surgery [1, 2]. Compression of lung tissue, absorption of alveolar air, and impairment of surfactant function have all been implicated; however, many other factors can also contribute, such as the increased abdominal pressure during laparoscopic procedures or the supine position [3]. Obese patients (OP) are more likely to develop intraoperative atelectasis [5] as they exhibit a greater decrease in functional residual capacity (FRC) during GA; an exponential relationship between increasing body mass index (BMI) and decreasing FRC has been observed [4, 5].
Atelectasis is one of the main causes of postoperative hypoxemia (PH) and may predispose to postoperative adverse outcomes, such as respiratory failure, pneumonia, and mortality [6]. Preventing these complications is a recognized measure of any hospital’s quality of care [7, 8].
Several strategies have been found to be effective [9,10,11,12,13,14] in reducing atelectasis during GA in obese patients. Among intraoperative ventilation strategies, the optimal level of PEEP remains controversial. PEEP improves intraoperative lung function (lung compliance, oxygenation), especially in combination with recruitment maneuvers [1,2,3,4,5,6, 9,10,11,12,13,14,15,16,17,18,19,20]. However, the use of high levels of PEEP may result in hemodynamic instability [15] and pulmonary overdistension [21,22,23,24,25,26]. In a recent review, Fernandez-Bustamante et al. suggested to titrate the level of PEEP to maximize dynamic lung compliance (Cdyn) [7].
The primary objective of our study was to test the hypothesis that lung compliance optimization through PEEP manipulations could reduce the incidence of postoperative hypoxemia (IPH) in patients undergoing laparoscopic bariatric surgery compared with a pragmatic level of PEEP fixed at 10 cm H2O.
Methods
Our study was a prospective, randomized controlled study, approved by the Institutional Ethics Committee. Written informed consent was obtained from all participating subjects. This manuscript adheres to the applicable Enhancing the Quality and Transparency of Health Research (EQUATOR) guidelines.
Patients were included according to the following criteria: age over 18 years, ASA score (American Society of Anesthesiologists) II or III, body mass index (BMI) > 35 kg/m2, and elective laparoscopic bariatric surgery (gastric bypass or sleeve).
Exclusion criteria were the following: restrictive [total lung capacity (TLC) < 65%] or obstructive [Tiffeneau ratio (FEV1/FVC ratio) < 69%] pulmonary disease; increased intracranial pressure; active smoking; current pregnancy; history of heart failure (New York Heart Association class III or IV) or coronary artery disease; urgent surgery; allergy to any drug used in the study. Patients with a higher incidence of postoperative atelectasis (i.e., history of obstructive sleep apnea syndrome) were not excluded from the study.
The anesthetic management was standardized for each patient. Drugs were administered according to the ideal body weight [IBW (kg) = height (cm)—100 (for men) and 105 (for women)], except for muscular relaxants for which the corrected IBW (IBW + 40% overweight) was used (see annex 1 for the complete anesthetic protocol).
Preoxygenation was obtained by vital capacity maneuvers with a fraction of inspired oxygen (FiO2) of 1.0 and a 10 cm H2O CPAP until an end-tidal SpO2 > 90% was obtained in Ramp positioned patients. Anesthesia was induced with propofol, sufentanil, and rocuronium and maintained with desflurane (6–8%) to keep entropy values between 40 and 60.
Patients were ventilated in volume control mode with a mixture of 50% oxygen and 50% air, a tidal volume (VT) of 8 mL/kg IBW, and an inspiratory-expiratory ratio (I/E) of 1:2 [7]. The initial respiratory rate of 10 breaths/min was adjusted to maintain end-tidal carbon dioxide partial pressure between 35 and 45 mmHg. Plateau pressure (Pplat) was limited to 30 cm H2O and inspiratory peak pressure (PIP) to 40 cm H2O. Recruitment maneuvers (RM) were applied whenever the SpO2 < 95%, using to the protocol described by Whalen et al. [10].
For the laparoscopic procedure, a carbon dioxide pneumoperitoneum was performed with a maximal intra-abdominal pressure of 15 mmHg.
Lactated Ringer’s solution was administered at a rate of 3 mL kg−1(IBW) h−1 throughout the procedure. During surgery, hypotension (decrease in MAP greater than 25% from baseline) was treated with a bolus of 250 mL of 3% modified fluid gelatin (Geloplasma, Fresenius Kabi GmbH, Germany) if pulse pressure variation was greater than 13% (IntelliVue MP40™, Philips Medical Systems, Andover, USA) (fluid challenge) or by intravenous bolus administration of vasoactive drugs (5 mg ephedrine or 50 mcg neosynephrine) if pulse pressure variation was lower than 13%. Urinary losses were compensated with lactated Ringer’s solution at a ratio of 1 to 1 and blood losses were compensated with a 3% modified fluid gelatin at a 1:3 ratio.
At the end of surgery, patients’ trachea was extubated when the following criteria were met: hemodynamic stability (heart rate and mean arterial pressure; a maximum variation of 20% around the baseline value was accepted); normothermia (temperature > 36 °C); VT > 5 mL/kg (IBW); and minimal respiratory frequency of 11 breaths/min.
All patients were transferred to the PACU in head-up sitting position with supplemental nasal oxygen (3 L/min). If the SpO2 was < 90%, a ‘Venturi’ mask with 35% FiO2 was applied. For patients using CPAP preoperatively, CPAP was used as soon as they could cooperate. When leaving the PACU, all patients received supplemental nasal oxygen (3 L/min) during the first postoperative day (D1) and were monitored with a portable pulse oximeter (oxytrue®A, Bluepoint medical, Selmsdorf, Germany) up to the second postoperative day (D2). The invasive arterial catheter could not be maintained after the patient had left the recovery room.
At the 30th postoperative day (POD), the medical record of each patient was reviewed to collect possible postoperative complications.
Study Protocol
In the control group, a 10-cm H2O level of PEEP was applied throughout the surgical procedure and recruitment maneuvers (RM) were applied whenever SpO2 < 95% (Fig. 1).

Study design and three key times: PEEP = positive end-expiratory pressure; CPAP = continuous positive airway pressure; Cdyn = dynamic lung compliance; PS = pressure support; T1 = time 1, after induction/intubation, flat patient, without pneumoperitoneum; T2 = time 2, after pneumoperitoneum inflation and implementation anti-Trendelenburg; T3 = time 3, after pneumoperitoneum exsufflation, flat patient
In the study group, starting with the same baseline level (10 cm H2O), PEEP was adapted to achieve the best Cdyn determined by the ventilator (Aisys® CS [2], GE Healthcare, Madison, WI, USA). This maneuver was repeated at 3 time points (Fig. 1: T1, T2, T3). The best Cdyn was achieved by first increasing the level of PEEP by 2 cm H2O. If the Cdyn value increased after 6 respiratory cycles, PEEP was further increased by another 2 cm H2O. Conversely, if the Cdyn value decreased after 6 respiratory cycles, PEEP was decreased by 2 cm H2O. The PEEP levels were limited to the maximum allowed values for the current Pplat or Pip. A recruitment maneuver was applied whenever SpO2 < 95% [10].
Measurements
Measurements performed preoperatively (ambient air) included heart rate (HR), mean arterial blood pressure (MAP), SpO2, arterial pH, PaCO2, and PaO2. Parameters measured intraoperatively were HR, MAP, SpO2, arterial pH, PaCO2, and PaO2, end-tidal CO2, PaO2/FiO2 ratio, Cdyn, anatomical dead space ratio (VD/VT), and the number of recruitment maneuvers (RM). These variables were measured after induction of anesthesia in flat positioning, without pneumoperitoneum (T1), after pneumoperitoneum inflation and anti-Trendelenburg positioning (T2), and after pneumoperitoneum exsufflation, in flat positioning (T3). Volume of fluids administered and the need for fluid challenges and/or vasopressors were also recorded.
Study Outcomes
The primary endpoint was the incidence of postoperative hypoxemia (IPH) defined as the percentage of time spent with a SpO2 < 90% during the first (D1) and the second postoperative day (D2). The secondary endpoints included pulmonary dynamic compliance (Vt/Ppeak-PEEP), anatomical dead space ratio (VD/VT = (1-etCO2/PaCO2), and PaO2/FiO2 ratio. The tertiary endpoints included the number of RM (n), the need for fluid (n), the volume of colloid (mL), the use of vasopressors during surgery (n), and the incidence of complications at the 30th postoperative day (n).
Statistical Analysis
No power analysis was performed, as the incidence of our primary endpoint for the study population was not reported in the literature. We elected to recruit 100 patients and then modify our sample size according to our results if required. Subjects were randomized using a computer-generated random table with block sizes of 10. Patients were blinded to the group allocation. The anesthetist in charge of the patient was not blinded, but data collection and statistical analysis were blinded.
As the distribution of continuous variables was not homogenous (Kolmogorov-Smirnov test), groups were compared with the Mann-Whitney U test and data expressed as median and interquartile range. Categorical variables were compared using Chi-square and data presented as percentage. Two-way analysis of variance for repeated measurements was used to compare PEEP, PaO2/FiO2, Cdyn, and VD/VT between both groups. Statistical programs used were Minitab 16 (Paris, France) and the R version 3.2.1. For all analyses, a p value < 0.05 was considered significant.
Results
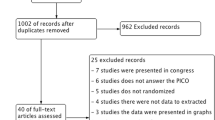
Of the 208 consecutive OP screened for eligibility, from July 2013 to December 2015, 100 were randomized (50 in the control group, 50 in the intervention group) and included in the analysis (Fig. 2). There was no statistical difference between groups, except for the genre (Table 1).

CONSORT diagram: recruitment, inclusion, exclusion and randomization
Incidence of postoperative hypoxemia was not different between groups (Table 2). Mean SpO2 on D2 was not different between groups, although it was higher in the control group on D1. Notably, all but three patients presented with at least one episode of hypoxemia during the study postoperative period.
Cdyn was significantly higher in the study group compared to the control group at all time points (Table 3). The level of PEEP and the VD/VT ratio was similar between the two groups. The PaO2/FiO2 ratio increased progressively throughout the procedure in both groups, without any significant difference between the groups.
There was no difference in the number of RM at any time point (3 vs 3, 6 vs 2, and 2 vs 0) between the groups. Twenty-two patients in the control group and 27 patients in the study group received a fluid challenge (p = 0.317). The total volume of colloid (mL) was 375 mL (250–500) in the control group and 500 mL (250–500) in the study group (p = 0.613). Twenty patients in the control group and 23 in the study group received at least one vasopressor bolus (p = 0.544).
Incidence of postoperative complications was low (3 in each group). There was no pulmonary complication in both groups.
Discussion
In the conditions of our study, Cdyn optimization through PEEP manipulations did not reduce the IPH when compared to a fixed 10 cm H2O PEEP. To our knowledge, this study was the first to assess the effect of Cdyn optimization on the IPH up to postoperative day 2.
Although postoperative hypoxemia episodes may have important clinical consequences in obese patients [6], only one study has so far assessed the incidence of postoperative hypoxemia in patients undergoing laparoscopic bariatric surgery during the immediate postoperative period. In this study, Defresne et al. [27] reported IPH on D1 ranging from 2.1 to 2.5%, which is similar to our results. Notably, these authors used a protective ventilation protocol combining ‘Ramp’ position, recruitment maneuvers using a 10 cm H2O CPAP, low tidal volume, and 10 cm H2O PEEP. The observed low IPH might be a result of the beneficial interaction between all the protective strategies used in both studies. Indeed, protective ventilation approaches during general anesthesia could improve postoperative pulmonary function and arterial oxygenation up to 5 days postoperatively [28].
In our study, combining different protective ventilation maneuvers was associated with a low incidence of RM to keep a SpO2 > 95%. The optimal modalities and systematization of RM remain a matter of debate in the literature [29,30,31]. Because RM can cause adverse effects including temporary desaturation, decreased preload, hypotension, arrhythmias, and barotrauma [7], we elected to perform RM only when SpO2 was < 95%. Defresne et al. [27] showed that when added to a protective mechanical ventilation strategy combining low tidal volume and high PEEP, RM does not improve FRC and arterial oxygenation.
In our study, individual PEEP manipulation to optimize Cdyn resulted in a mean level of PEEP of 10 cm H2O. Interestingly, these results confirm those of Coussa’s et al. and Talab’s et al. [1, 11] who concluded that 10 cm H2O was an optimum level of PEEP to reduce atelectasis and maintain oxygenation in obese patients during surgery. This might explain why the level of PEEP manipulated to achieve the best Cdyn was similar to that used through a pragmatic approach as recommended by the PROBESE study [32]. Although Cdyn was significantly higher in the study group, the difference compared to the control group was probably not clinically relevant.
Individual titration of PEEP to a respiratory mechanical target such as Cdyn represents a compromise of regional overdistention and collapsing-reopening of lung units [32]. As such, our methodology is in accordance with Maisch’s et al. [23] and Fernandez-Bustamante et al. [7] who suggest that the optimal level of PEEP is the pressure level with the highest compliance value in conjunction with the lowest VD/VT ratio [7, 23].
PaO2/FiO2 ratios increased throughout the surgery in both groups. This could be the result of a gradual recruitment rather than the consequence of pulmonary overdistension as the Cdyn measured before and at the end of surgery was similar.
The need for fluid challenges and the use of vasopressors were not different between groups. Nevertheless, almost half of our patients required a fluid challenge or vasopressors. Our results confirm that the use of high levels of PEEP require more frequent interventions to treat hemodynamic instability [15].
Our study presents several limitations. Firstly, the study was not powered for the primary objective, as the IPH after laparoscopic bariatric surgery was not known when the protocol was designed. However, based on our results, no difference could be expected between both strategies even if a much higher number of patients were recruited.
Secondly, evaluation of hypoxemia episodes through portable oximeter was performed during a relatively short postoperative period. The incidence of postoperative hypoxemia tended to be higher on D2 than on D1, but it should be noted that the patients did not receive supplemental oxygen up to D1 according to our institutional practices. The mean hospitalization duration was short in our population (4 days).
Thirdly, our results are limited to laparoscopic bariatric surgery in obese patients and may not apply to other surgical procedures and populations. Such ventilatory approach required the use of an anesthetic machine allowing the determination of Cdyn which is the case for most modern ventilators.
In conclusion, IPH was not reduced by an open lung approach with protective ventilation strategy aiming at optimizing Cdyn in obese patients undergoing laparoscopic bariatric surgery. A pragmatic application of a PEEP level of 10 cm H2O was comparable to an individual PEEP titration in these patients.
Presentation: Preliminary data for this study were presented as a poster presentation at the Euroanaesthesia meeting, 28–30 May 2016, London.
Data Availability
Data are available upon reasonable request to the corresponding author.
References
Coussa M, Proietti S, Schnyder P, et al. Prevention of atelectasis formation during the induction of general anesthesia in morbidly obese patients. Anesth Analg. 2004;98(5):1491–5.
Magnusson L, Spahn DR. New concepts of atelectasis during general anaesthesia. Br J Anaesth. 2003;91(1):61–72.
Duggan M, Kavanagh BP. Pulmonary atelectasis: a pathogenic perioperative entity. Anesthesiology. 2005;102(4):838–54.
Pelosi P, Croci M, Ravagnan I, et al. The effects of body mass on lung volumes, respiratory mechanics, and gas exchange during general anesthesia. Anesth Analg. 1998;87(3):654–60.
Eichenberger A, Proietti S, Wicky S, et al. Morbid obesity and postoperative pulmonary atelectasis: an underestimated problem. Anesth Analg. 2002;95(6):1788–92. table of contents
Imberger G, McIlroy D, Pace NL, et al. Positive end-expiratory pressure (PEEP) during anaesthesia for the prevention of mortality and postoperative pulmonary complications. Cochrane Database Syst Rev. 2010;9:56–67. https://doi.org/10.1002/14651858.CD007922.
Fernandez-Bustamante A, Hashimoto S, Serpa Neto A, et al. Perioperative lung protective ventilation in obese patients. BMC Anesthesiol. 2015;15(1):56.
Shander A, Fleisher LA, Barie PS, et al. Clinical and economic burden of postoperative pulmonary complications: patient safety summit on definition, risk-reducing interventions, and preventive strategies. Crit Care Med. 2011;39(9):2163–72.
Futier E, Constantin J-M, Pelosi P, et al. Intraoperative recruitment maneuver reverses detrimental pneumoperitoneum-induced respiratory effects in healthy weight and obese patients undergoing laparoscopy. Anesthesiology. 2010;113(6):1310–9.
Whalen FX, Gajic O, Thompson GB, et al. The effects of the alveolar recruitment maneuver and positive end-expiratory pressure on arterial oxygenation during laparoscopic bariatric surgery. Anesth Analg. 2006;102(1):298–305.
Talab HF, Zabani IA, Abdelrahman HS, et al. Intraoperative ventilatory strategies for prevention of pulmonary atelectasis in obese patients undergoing laparoscopic bariatric surgery. Anesth Analg. 2009;109(5):1511–6.
Almarakbi WA, Fawzi HM, Alhashemi JA. Effects of four intraoperative ventilatory strategies on respiratory compliance and gas exchange during laparoscopic gastric banding in obese patients. Br J Anaesth. 2009;102(6):862–8.
Reinius H, Jonsson L, Gustafsson S, et al. Prevention of atelectasis in morbidly obese patients during general anesthesia and paralysis: a computerized tomography study. Anesthesiology. 2009;111(5):979–87.
Pelosi P, Ravagnan I, Giurati G, et al. Positive end-expiratory pressure improves respiratory function in obese but not in normal subjects during anesthesia and paralysis. Anesthesiology. 1999;91(5):1221–31.
Hemmes SN, Gama de Abreu M, Pelosi P, et al. High versus low positive end-expiratory pressure during general anaesthesia for open abdominal surgery (PROVHILO trial): a multicentre randomised controlled trial. Lancet. 2014;384(9942):495–503.
Tusman G, Böhm SH, Suarez-Sipmann F, et al. Alveolar recruitment improves ventilatory efficiency of the lungs during anesthesia. Can J Anesth. 2004;51(7):723–7.
Maracajá-Neto LF, Verçosa N, Roncally AC, et al. Beneficial effects of high positive end-expiratory pressure in lung respiratory mechanics during laparoscopic surgery. Acta Anaesthesiol Scand. 2009;53(2):210–7.
Meininger D, Byhahn C, Mierdl S, et al. Positive end-expiratory pressure improves arterial oxygenation during prolonged pneumoperitoneum. Acta Anaesthesiol Scand. 2005;49(6):778–83.
Futier E, Constantin JM, Paugam-Burtz C, et al. A trial of intraoperative low-tidal-volume ventilation in abdominal surgery. N Engl J Med. 2013;369(5):428–37.
Aldenkortt M, Lysakowski C, Elia N, et al. Ventilation strategies in obese patients undergoing surgery: a quantitative systematic review and meta-analysis. Br J Anaesth. 2012;109(4):493–502.
Gattinoni L, Carlesso E, Caironi P. Stress and strain within the lung. Curr Opin Crit Care. 2012;18(1):42–7.
Suter PM, Fairley B, Isenberg MD. Optimum end-expiratory airway pressure in patients with acute pulmonary failure. N Engl J Med. 1975;292(6):284–9.
Maisch S, Reissmann H, Fuellekrug B, et al. Compliance and dead space fraction indicate an optimal level of positive end-expiratory pressure after recruitment in anesthetized patients. Anesth Analg. 2008;106(1):175–81.
Blankman P, Hasan D, Groot Jebbink E, et al. Detection of “best” positive end-expiratory pressure derived from electrical impedance tomography parameters during a decremental positive end-expiratory pressure trial. Crit Care. 2014;18(3):R95.
Carvalho ARS, Jandre FC, Pino AV, et al. Effects of descending positive end-expiratory pressure on lung mechanics and aeration in healthy anaesthetized piglets. Crit Care. 2006;10(4):R122.
Terragni PP, Rosboch G, Tealdi A, et al. Tidal hyperinflation during low tidal volume ventilation in acute respiratory distress syndrome. Am J Respir Crit Care Med. 2007;175(2):160–6.
Defresne AA, Hans GA, Goffin PJ, et al. Recruitment of lung volume during surgery neither affects the postoperative spirometry nor the risk of hypoxaemia after laparoscopic gastric bypass in morbidly obese patients: a randomized controlled study. Br J Anaesth. 2014;113(3):501–7.
Severgnini P, Selmo G, Lanza C, et al. Protective mechanical ventilation during general anesthesia for open abdominal surgery improves postoperative pulmonary function. Anesthesiology. 2013;118(6):1307–21.
Pelosi P, Gama de Abreu M, Rocco PR. New and conventional strategies for lung recruitment in acute respiratory distress syndrome. Crit Care. 2010;14(2):210.
Writing Group for the Alveolar Recruitment for Acute Respiratory Distress Syndrome Trial I, Cavalcanti AB, Suzumura ÉA, et al. Effect of lung recruitment and titrated positive end-expiratory pressure (PEEP) vs low PEEP on mortality in patients with acute respiratory distress syndrome: a randomized clinical trial. JAMA. 2017;318(14):1335–45.
Jo YY, Kwak HJ. What is the proper ventilation strategy during laparoscopic surgery? Korean J Anesthesiol. 2017;70(6):596–600.
Bluth T, Teichmann R, Kiss T, et al. Protective intraoperative ventilation with higher versus lower levels of positive end-expiratory pressure in obese patients (PROBESE): study protocol for a randomized controlled trial. Trials. 2017;18(1):202.
Acknowledgements
Assistance with the study: The authors would like to thank the following persons from the Department of Anaesthesiology, CHU Brugmann-HUDERF, Brussels, Belgium, who kindly performed the protocol study in the operating room: Ida Stany M.D., Robert Tircoveanu M.D., Yannick Ciccarella M.D., Jean-Louis Majcher M.D., Christiane Dzechi M.D., and Muj Mulaj M.D.
Funding
This work was supported only by CHU Brugmann-HUDERF departmental sources and the Brugmann foundation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Our study was a prospective, randomized controlled study, approved by the Institutional Ethics Committee. Written informed consent was obtained from all participating subjects. This manuscript adheres to the applicable Enhancing the Quality and Transparency of Health Research (EQUATOR) guidelines.
Conflicts of Interest
The authors declare that they have no conflict of interest.
Ethical and Consent Statement
Ethical and consent statement provided by the Institutional Ethics Committee. Written informed consent was obtained from all participating subjects.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Annex 1: anesthetic protocol
Annex 1: anesthetic protocol
All subjects stopped consuming solid food from 6 h and clear liquids from 2 h before the elective surgery, and received 0.5–1 mg alprazolam and 150 mg ranitidine perorally, 1 h before the procedure as premedication.
Before induction, each patient was placed in ‘Ramp’ position. Basic monitoring was undertaken, including: electrocardiogram, non-invasive blood pressure (NIBP), and pulse oximetry oxygen saturation (SpO2).
An 18-gauge catheter was placed in a vein and a 20-gauge catheter in a radial artery. Further monitoring included entropy, thumb’s adductor neuromuscular monitor, nasopharyngeal temperature probe, and urinary catheter.
Anesthesia was induced by intravenous administration of propofol (2–3 mg/kg IBW) and sufentanil (GEPS model with target concentration of 0.3 ng/mL based on IBW: discontinued 1 h before the end of surgery). The intubation (tube size 8 for women and 8.5 for men) was facilitated by the administration of intravenous rocuronium (0.6 mg/kg corrected IBW). Antibiotic prophylaxis (cefazolin 2 g and metronidazole 500 mg) was also given at the induction.
Anesthesia was maintained with desflurane (6–8%) to keep entropy values between 40 and 60. Every 30 min, a train of 4 (TOF 50 Hz) was performed and a rocuronium bolus (0.15 mg/kg IBW) was administered as needed to maintain a TOF ratio of 0:4.
At the end of surgery, all patients received paracetamol (1 g). Neuromuscular blockade was checked at the thumb’s adductor. The neuromuscular blockade was reversed with 4 mg/kg (corrected IBW) sugammadex when the train-of-four (TOF) ratio reached 2:4.
After attaining a TOF ratio of 4:4 with a sustained tetanic stimulation at 100 Hz over 5 s, patients were placed in ‘Ramp’ position and the administration of desflurane and mechanical ventilation with volume control mode was discontinued in order to switch to mechanical ventilation with pressure support [PEEP of 5 cm H2O and 100% inspired fraction of oxygen (FiO2)].
Anti-emetic prophylaxis was administered to all patients as follows: 40 mg methylprednisolone at the induction and 4 mg ondansetron at the end of the intervention.
Thromboprophylaxis included intermittent pneumatic compression device beginning before surgery and low molecular weight heparin (80 mg/day) beginning 6 h after the procedure.
In the postoperative period, each patient received paracetamol 1 g every 6 h and patient-controlled intravenous analgesia with piritramide was started at the post-anesthesia care unit (PACU) (2-mg bolus every 7 min with a maximum of 30 mg in 4 h).
Rights and permissions
About this article

Cite this article
Van Hecke, D., Bidgoli, J.S. & Van der Linden, P. Does Lung Compliance Optimization Through PEEP Manipulations Reduce the Incidence of Postoperative Hypoxemia in Laparoscopic Bariatric Surgery? A Randomized Trial. OBES SURG 29, 1268–1275 (2019). https://doi.org/10.1007/s11695-018-03662-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-018-03662-x