
Abstract
Acromioclavicular (AC) joint injuries are common in competitive and recreational athletes. These injuries are a significant cause of pain and instability, especially with overhead activities. Injuries are generally classified using the Rockwood Classification system, based on the degree of ligamentous injury to the AC joint and the coracoclavicular (CC) ligaments. In general, Rockwood type I and II injuries are managed nonoperatively, while types IV and VI are usually treated surgically. However, there is debate on the optimal treatment of type III and V injuries. Various surgical techniques have been described, including reconstruction with internal fixation, coracoacromial ligament transfer, reconstruction with suture fixation, anatomic coracoclavicular ligament reconstruction (ACCR), and arthroscopic-assisted techniques. The current review article describes the diagnosis and therapy of this injury with regard to the athlete and additionally presents the differences in treatment approaches between the United States and Germany (Europe).
Zusammenfassung
Akromioklavikular(AC)-Gelenkverletzungen sind bei Leistungs- und Freizeitsportlern eine häufige pathologische Veränderung. Diese Verletzungen sind eine wesentliche Ursache für Schmerzen und Instabilität, insbesondere bei Überkopfaktivitäten. Die Verletzung wird i. Allg. nach Rockwood klassifiziert, basierend auf dem Grad der Kapsel-Band-Verletzung des AC-Gelenks und der korakoklavikulären Bänder (CC). Grundsätzlich werden Rockwood-Verletzungen vom Typ I und II konservativ behandelt, während die Typen IV und VI i. Allg. chirurgisch behandelt werden. Die optimale Behandlung von Typ-III- (oft auch von Typ-IV-)Verletzungen wird jedoch kontrovers diskutiert. Es wurden verschiedene chirurgische Techniken beschrieben, darunter die Rekonstruktion mit interner Fixation, der Korakoakromialligamenttransfer, die Rekonstruktion mit Nahtfixation, die anatomische Rekonstruktion der korakoklavikulären Bänder (ACCR) und arthroskopisch assistierte Techniken. Im vorliegenden Übersichtsartikel werden die Diagnostik und Therapie dieser Verletzung im Hinblick auf den Sportler dargestellt und zusätzlich die Unterschiede zwischen einem US-amerikanischen und einem deutschen (europäischen) Behandlungskonzept gezeigt.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
The review describes acromioclavicular (AC) joint injuries in athletes, including the epidemiology, clinically relevant pathoanatomy, and biomechanics, and discusses the available conservative and surgical treatment options. We specifically outline both the senior U.S. author’s preferred technique of anatomic coracoclavicular ligament reconstruction (ACCR) and the German approach, which consists in arthroscopic-assisted techniques.
Epidemiology
Acromioclavicular (AC) joint injuries in athletes most commonly result from a direct impact on the shoulder’s superolateral acromion with the arm in adduction. Patients typically describe a blow to their shoulder when colliding with another player or the ground.
It is essential to consider the type of sport an athlete competes in, as these injuries are especially prominent in contact sports, accounting for up to 41% of shoulder injuries [16, 17, 23, 27, 29, 36]. In addition, AC joint injuries are more common during in-season competition than in practice, related to high-speed, full-contact collisions [23]. Understanding the prevalence of AC joint injuries in different sports helps assist orthopedic surgeons in diagnosis and treatment. In contact sports such as American football, rugby, and ice hockey, the rates of AC joint injuries can be as high as 41% [12, 16, 17, 23, 27, 29, 36].
In contact sports, physicians should have a high index of suspicion for an AC joint injury following a player’s lateral shoulder sustaining a direct blow from an opponent or after being driven into the playing surface. In American football, AC joint sprains are one of the most common shoulder injuries, and players are 14 times more likely to sustain sprains during in-season games than during practice [12]. In elite collegiate football players, AC separation accounted for up to 41% of shoulder injuries [27]. Offensive skill position players (quarterback, wide receiver, running back, tight end) had a higher incidence of AC injuries than defensive players [27]. Rugby and Australian Rules football players experience similar forceful collisions and tackles to American football players. In rugby players, AC joint injuries are the most common in-match shoulder injury, accounting for 32% of shoulder injuries [19, 23].
Injuries of the AC joint are among the most common overall injuries in ice hockey and lead to a significant amount of time lost by athletes [16, 24, 31, 42, 43, 47, 63]. In addition to contact with an opponent or the ground, ice hockey players frequently injure their AC joint through contact with the hockey rink boards.
Although much less common, it is vital to be aware that AC joint injuries can present in noncontact athletes (soccer, basketball, baseball, cycling, etc.) too [24]. The mechanism of injury in these sports is more commonly due to a fall onto the shoulder or outstretched arm. However, noncontact injuries have also been noted to occur as a result of noncontact excessive loading of the joint, as demonstrated by a study of professional golfers that reported that 53% experienced pain in the AC joint [36].
Classification system
The classification system of AC joint injuries is based on radiographic and clinical examination findings, as shown in Table 1. Historically, Tossy et al. and Allman grouped AC joint injuries into three grades, which were further modified into the six types described in the Rockwood classification system [1, 60, 64].
A consensus statement from the ISAKOS Upper Extremity Committee in 2014 recommended that type III injuries be divided into type IIIA and IIIB based on function, pain, scapular motion, and cross-body adduction x‑rays [4]. The authors described type IIIA injuries as stable injuries without persistent pain or limitation in function. By contrast, patients with persistent pain, scapular dyskinesis, and radiographic findings consistent with type IIIB injuries may warrant earlier surgical intervention.
Physical examination
The athlete should be examined standing or sitting without supporting their injured shoulder, because the arm’s weight can accentuate deformity. A thorough shoulder examination should begin with the cervical spine, as cervical radicular symptoms can mimic shoulder pathology. All patients should undergo a thorough neurovascular assessment to rule out a brachial plexus or vascular injury. A visual inspection should evaluate for any signs of deformity, swelling, bruising, or asymmetry compared with the contralateral shoulder. In high-grade AC joint injuries, the distal clavicle can protrude through the trapezial fascia and tent the skin, creating a visible prominence. The AC joint and CC interspace should be palpated for tenderness or instability. Palpation should also include the sternoclavicular joint, clavicle, and glenohumeral joint for concomitant fractures, displacement, or injuries.
Following palpation, the examiner should fix the lateral clavicle with their thumb and index finger and provoke an anterior-to-posterior translation, always in comparison with the opposite healthy shoulder, to get an impression of horizontal instability. Horizontal instability with an anterior-to-posterior force suggests injured AC ligaments, while vertical (superior–inferior force) instability indicates CC ligament injury. Reduction of displaced injuries can be attempted by stabilizing the clavicle and placing an upward force on the ipsilateral elbow. Additionally, by having a patient shrug their shoulder, the integrity of the deltotrapezial fascia can be assessed. The integrity of the deltotrapezial fascia is important when distinguishing between type III and V AC joint injuries, as this motion will reduce type III but not type V injuries [51].
The two most widely described provocative tests are the cross-arm adduction test and the O’Brien active compression test. A simple way to perform the cross-body adduction test is to ask the patient to reach across their body and touch their contralateral shoulder. The examiner should palpate the AC joint during this maneuver and assess for pain, tenderness, or overriding of the distal clavicle on the acromion. A distal clavicle that overrides the acromion with a cross-body adduction maneuver may suggest a type IIIB injury that warrants more aggressive treatment [4]. The O’Brien test is performed by flexing the affected shoulder to 90°, with 10° of adduction and maximal internal rotation. A downward force is then applied to the arm, and pain in the AC joint is considered a positive test. Both assess for provoked pain over the AC joint, with the cross-arm adduction test being the most sensitive (77%) and the O’Brien test being the most specific [8].
Imaging
Athletes with history and physical examination findings suggestive of AC joint injury should have standardized shoulder radiographs to diagnose and classify the injury. Variation in individual anatomy and variations of the techniques of x‑ray technicians make bilateral radiographs and comparison with the healthy side essential for diagnosis.
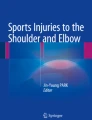
Figure 1 represents a standard radiographic series in a patient with a type V AC joint injury, including anteroposterior (AP), axillary, and bilateral Zanca views. The AP views should be taken with one-third penetration bilaterally to evaluate vertical CC displacement. An axillary view can demonstrate posterior displacement of the distal clavicle, which is helpful in diagnosing type IV injuries. In this case, very subtle posterior displacement is seen; however, given the significant increase in CC distance, we classified this as a type V injury. By tilting the x‑ray 10–15° in the cephalic direction with one-half the standard penetration strength, the Zanca view is the most accurate view to assess the AC joint [38].

Radiographic imaging of type V acromioclavicular joint injuries. a Anteroposterior view, b axillary view, c cross-body adduction view, d bilateral Zanca view: right (R) demonstrates increased coracoclavicular distance compared to contralateral left side (L)
Specialized views can be useful in classifying the type of AC joint injury. The cross-body adduction view (Basmania/Alexander) can help discern between type IIIa and IIIb injuries [4]. The modified bilateral Alexander views can quantify dynamic posterior translation of an unstable AC joint [46]. Historically, an AP stress view has been used to help differentiate type II and III injuries; however, it is rarely used in current practice as it can be quite uncomfortable.
Advanced imaging, including magnetic resonance imaging and computed tomography scans, can provide additional information and rule out concomitant injuries. Magnetic resonance imaging is helpful to evaluate for other soft tissue injuries such as long head of biceps lesions, labral tears, or rotator cuff tears. Tischer et al. showed that patients with AC joint injuries could concurrently present with superior labral anterior posterior (SLAP) lesions (14.3%), rotator cuff tears (3.9%), and fractures (5.2%) [59]. Computed tomography scans can be useful in providing greater detail of nondisplaced lateral clavicular or acromial fractures not identified on plain radiographs.
Treatment
The severity of injury typically guides treatment for AC joint injuries in athletes on a case-by-case basis. In general, lower-grade injuries such as type I and II are treated conservatively. Higher-grade injuries such as IV, V, and VI are typically treated surgically. Much debate exists regarding the optimal treatment for type III injuries, as many studies have shown acceptable outcomes with nonoperative treatment in these patients [3, 41, 52, 57, 58, 61]. In deciding a treatment plan, it is important to consider what sport the athlete will be returning to, hand-dominance, position requirements, the season of sport, and the patient’s goals. The ultimate goal of treatment is a pain-free and fully functional return to play.
Type I and II
Rockwood type I and II AC joint injuries are predominantly treated nonoperatively, although this is primarily based on case series (level IV evidence) and expert opinion (level V evidence). Based on the athlete, their sport, and their current pain level, our institution’s practice is to allow athletes to return to play the same day. If the athlete is in considerable pain, we consider injection with a local anesthetic. Athletes with a considerable amount of pain and whose sport does not necessitate an immediate return to play may also undergo a brief period of immobilization in a sling for comfort, typically for 3–10 days [10, 38]. Activity modification, rest, cryotherapy, and anti-inflammatories can help with pain and swelling during the acute phase of injury and the initial period of immobilization.
In the first week following injury, physical therapy can assist in regaining range of motion, beginning with closed-chain scapular exercises and introducing open-chain exercises once the patient can maintain forward elevation without pain [10]. Progression is made toward isotonic strength exercises followed by sport-specific training [10, 38, 56]. For athletes undergoing more conservative treatment, we allow athletes to return to play when they no longer experience pain and demonstrate a normal range of motion, strength, and a lack of scapular dyskinesis.
Type III
Our institution’s opinion is to treat type III AC joint injuries nonoperatively, which is supported by a review of the current literature [3, 41, 52, 57, 58, 61]. One important consideration is whether the athlete is in-season. Trainer et al. recommended that in-season athletes who demonstrate normal motion and controlled pain with type III injuries can immediately return to sport upon receiving an intra-articular injection with a local anesthetic [61]. If immediate return to sport is not required, optimal nonsurgical management remains similar to type I and II injuries, except for an extension of sling immobilization to 3–4 weeks [44, 48, 54]. The subsequent rehabilitation is similar to type I and II injuries. Some consider athletes of throwing or overhead sport to be special cases that may warrant surgery due to the high demand on their shoulder girdle [22]. However, a previous study on Major League Baseball pitchers demonstrated comparable nonoperative and operative symptoms [41]. Even so, there are special circumstances where we still consider operative treatment for high-end athletes.
The ISAKOS Upper Extremity Committee considered that unstable type IIIB injuries demonstrate scapular dysfunction resistant to physical therapy, and an overriding clavicle after 3–6 weeks indicates surgical treatment [4]. Even in high-level athletes with IIIA injuries, surgery may be indicated if there is residual pain, loss of function, or inability to return to pre-injury level of play after 3–6 months of functional rehabilitation [38, 61].
Type IV–VI
The practice at our institution is that all acute, high-grade type IV, V, and VI AC joint injuries constitute an indication for surgical repair [4, 17, 34, 55]. Surgical repair aims to restore stability and range of motion, decrease pain, and allow the athlete to return to sport at a pre-injury level. A recent systematic review showed that the rate of return to pre-injury level of play after surgery was 86.2% in type V injuries and 89.6% after type IV injuries [28]. However, the failure rate for surgical repair is as high as 21%, and 10% of patients require revision [20]. Additionally, it can be challenging to differentiate between type III and V injuries, which can make it more difficult to determine whether surgery is indicated. It is important to discuss the benefits and risks of surgery with each patient, as some athletes decide on a personal basis that the risks outweigh the benefits.
Surgical techniques
A plethora of surgical techniques have historically been described for surgical repair of AC joint injuries. Techniques include, but are not limited to, open reduction and internal fixation (ORIF), distal clavicle excision, Weaver–Dunn, modified Weaver–Dunn, and anatomic coracoclavicular ligament reconstruction (ACCR). The primary author’s (A.D.M) preferred method of reconstruction is ACCR, to restore the native anatomy and stability to the joint.
Non-anatomic historical repair techniques
Historically, joint injuries were surgically managed through ORIF. This approach used various screws, pins, Kirschner wires, plates, and hook plates for reduction and fixation. The migration of pins and wires was a serious complication and contributed to the abandonment of these methods [35, 50, 53]. Hook plates are commonly used in Europe and have been used successfully to treat AC joint injuries and distal clavicle fractures [15]. However, the plate is typically removed at 8–16 weeks, necessitating an additional procedure.
Other non-anatomic repairs for AC joint injuries include distal clavicle excision, the Weaver–Dunn, and the modified Weaver–Dunn. These techniques have failed to stabilize the AC ligament complex. Based on the results of previous biomechanics and review studies, anatomic reconstruction techniques have been demonstrated to be more favorable than non-anatomic techniques [3, 40, 62].
Anatomic coracoclavicular reconstruction—U.S. technique
A variety of ACCR techniques aim to restore the native CC ligaments anatomically. Jones et al. were the first to describe an open technique that created two tunnels in the clavicle to recreate the footprints of the trapezoid and conoid, which were then recreated using a semitendinosus autograft [26]. Semitendinosus, anterior tibialis, allo- or autografts have been described as suitable grafts for this repair [32]. The senior author (A.D.M) further developed this technique to augment the AC ligaments and CC ligaments with tendon graft (Fig. 2; [7, 39]). In this technique, two bone tunnels are drilled in the clavicle at the approximate insertion site of the trapezoid (anterolateral) and conoid (posteromedial) ligaments. A soft-tissue allograft (semitendinosus or peroneus longus) is then passed under the coracoid and pulled through their respective tunnels to restore the native anatomy of the CC ligaments. Both graft limbs are then fixed with two interference screws while maintaining a reduced AC joint. The longer limb of the graft exiting the lateral tunnel is then sutured to the acromion to reinforce the AC joint. The excess graft material is then used to recreate the superior and posterior AC ligaments.

Representative image of anatomic coracoclavicular ligament reconstruction technique (left shoulder). Interference screw is used to fix the tendon allograft in the posteromedial clavicular tunnel
The biomechanical importance of both the AC and CC ligaments in preventing vertical and horizontal translation has been well documented [11, 18, 25, 30], and this technique has subsequently been shown in biomechanical cadaveric studies to more effectively restore native tendon properties [9, 21, 32, 40]. In addition to favorable biomechanical evidence, this technique has yielded positive patient satisfaction rates and significant clinical and radiographic improvement [2, 5, 7, 13, 45, 49].
Arthroscopic-assisted coracoclavicular reconstruction with additional AC cerclage—the German way
Compared to the U.S., German orthopedic surgeons do not have the same access to allografts as needed for the ACCR. Therefore, a different approach has been developed during the past few years. Since we know that there is accompanying glenohumeral injury in up to 18.2% of all AC joint injures, the arthroscopic-assisted techniques have become one of the techniques most frequently used by specialized orthopedic shoulder surgeons in Germany [59].
In addition to CC reconstruction, the importance of addressing the AC capsule has become more evident. The AC cerclage has thus become one of the standard procedures addressing the horizontal instability component.
Glenohumeral approach for CC reconstruction
Yang et al. have described this approach [65], which is usually performed in a beach-chair position. A standard posterior portal is used, and a 30° scope is inserted, enabling an additional examination to exclude injuries to the glenohumeral joint and treat them simultaneously if necessary. A working portal in a low anterior–lateral position is established in an outside–in technique to allow the instruments to reach the base of the coracoid process. To access the coracoid base, dissection is performed using a shaver or electrocautery device. The subscapularis tendon serves as the direct visual guide passing the rotator cuff interval. The debridement should focus on the lateral part of the coracoid process so as to avoid neurovascular injury. Once the coracoid process is reached, the scope can be switched to a trans-supraspinatus lateral viewing portal directly posterior to the long head of the biceps tendon for better visualization. To perform a safe reconstruction, the inferior part of the coracoid base has to be clearly visualized [6].
Clavicle and coracoid drilling
With the undersurface of the base of the coracoids clearly visualized, the drill guide is placed under the base of the coracoid. Care is taken to make sure the guide is centered under the coracoid in order to avoid implant break-out. There are several techniques available for CC reconstruction, which basically differ in the diameter of the tunnel drilled through the clavicle and coracoid. Based on the implant used, there is a range of 2.4–4 mm of tunnel diameters (Fig. 3). Some surgeons prefer reconstructing both CC ligaments using two implant systems (e.g., AC-TightRope, Arthrex GmbH, Munich, Germany).

a Preoperative panorama view with high-grade acromioclavicular (AC) joint dislocation (right shoulder, Rockwood type V). b Anteroposterior view 6 weeks after coracoclavicular reconstruction using a single stand system (blue circle indicates the drill hole of the AC cerclage). c Y-view of AC joint shows an anatomic position with no loss of reduction. L left, orange line distance and dislocation, R right
The drill guide is directed over the lateral clavicle approximately 25–40 mm medial to the AC joint (depending on whether one or two implants are used), followed by a small 2–3-cm incision centered over the posterior aspect of the clavicle. Depending on the tunnel size, a drill (cannulated or not) is used and brought through all four cortices of the clavicle and coracoid. The drill guide is then removed, and through a shuttling maneuver, the implant(s) is put in place. The AC joint is then reduced, and the sutures are knotted to hold the reduced AC joint in its anatomic position. Maziak et al. proposed performing a small overreduction, as there might be some loss of reduction in postoperative rehabilitation [37].
Additionally, an AC cerclage is carried out to address the horizontal instability and reconstruct the AC ligaments/capsule. Several techniques for this have been described. The most important aspect is to add a cerclage, as Dyrna et al. reported in their study by testing different cerclage techniques [14].
Complications
Nonsurgical complications include chronic AC joint instability, cosmetic deformity, joint arthrosis, and distal clavicle osteolysis [17, 38, 55]. Persistent pain, instability, scapular dyskinesis, or inability to return to pre-injury form may necessitate surgical intervention. Failure of prolonged nonoperative treatment and ultimate surgery can significantly prolong an athlete’s return to play. Complications related to surgery include failure of surgical repair, surgical site infection, clavicular/coracoid fracture, graft failure, loss of reduction, and persistent pain [17].
Rehabilitation
The goal of postoperative physical rehabilitation is a safe and timely return to the pre-injury level of activity. Our current rehabilitation protocol focuses on periscapular control and four phases of progression [33]. Phase 1 begins with an extended period of platform brace immobilization for 6 weeks to allow for pain control and to unload the arm’s weight from the AC joint [10]. Phase 2 progresses to range-of-motion exercises and early strengthening when the patient is pain-free. This begins with passive- and active-assisted range of motion before progressing to closed-chain and periscapular exercise, with care taken to unload the arm’s weight and reduce AC joint stress. Phase 3 advances to a dynamic strengthening of the shoulder girdle and periscapular muscles. This phase continues with closed-chain exercises before the patient can progress to kinetic chain and open-chain exercises to promote scapular stability. Phase 4 is the final phase and integrates sports-specific training following kinetic chain exercises. Throwers begin with short, low-velocity throws before slowly progressing as tolerated. For overhead athletes such as tennis players, ground strokes should be initiated before progression to higher-energy, overhead serves. Throughout the rehabilitation process, it important to progress along these phases as a continuum, understanding that every athlete will heal differently and may require more or less time at each phase. Return-to-sport guidelines are largely determined on a case-by-case basis, but return to contact sports typically takes 4–6 months following completion of phase 4.
An appropriate algorithm to identify patients who benefit from conservative or operative treatment is essential (Fig. 4). However, it is important to discuss treatment options with an athlete individually and also take the type of sports into consideration when recommending a specific therapy.

Algorithm of treatment options for injuries of the acromioclavicular (AC) joint
Practical conclusion
-
Acromioclavicular (AC) joint injuries are common in competitive and recreational athletes and are a significant cause of pain and instability.
-
The classification of AC joint injuries is based on radiographic and clinical findings using the Rockwood classification system.
-
Rockwood type I and II injuries are managed nonoperatively, while types IV and VI are usually treated surgically; there is debate on the optimal treatment of type III and V injuries.
-
Several surgical techniques have been described, including reconstruction with internal fixation, coracoacromial ligament transfer, reconstruction with suture fixation, anatomic coracoclavicular ligament reconstruction, and arthroscopic-assisted techniques.
References
Allman FLJ (1967) Fractures and ligamentous injuries of the clavicle and its articulation. J Bone Joint Surg Am 49:774–784
Baran S, Belisle JG, Granger EK, Tashjian RZ (2018) Functional and radiographic outcomes after allograft anatomic coracoclavicular ligament reconstruction. J Orthop Trauma 32:204–210. https://doi.org/10.1097/BOT.0000000000001079
Beitzel K, Cote MP, Apostolakos J, Solovyova O, Judson CH, Ziegler CG, Edgar CM, Imhoff AB, Arciero RA, Mazzocca AD (2013) Current concepts in the treatment of acromioclavicular joint dislocations. Arthroscopy 29:387–397. https://doi.org/10.1016/j.arthro.2012.11.023
Beitzel K, Mazzocca AD, Bak K, Itoi E, Kibler WB, Mirzayan R, Imhoff AB, Calvo E, Arce G, Shea K (2014) ISAKOS upper extremity committee consensus statement on the need for diversification of the Rockwood classification for acromioclavicular joint injuries. Arthroscopy 30:271–278. https://doi.org/10.1016/j.arthro.2013.11.005
Berthold DP, Muench LN, Beitzel K, Archambault S, Jerliu A, Cote MP, Scheiderer B, Imhoff AB, Arciero RA, Mazzocca AD (2020) Minimum 10-year outcomes after revision anatomic coracoclavicular ligament reconstruction for acromioclavicular joint instability. Orthop J Sports Med 8:2325967120947033. https://doi.org/10.1177/2325967120947033
Braun S, Beitzel K, Buchmann S, Imhoff AB (2015) Arthroscopically assisted treatment of acute dislocations of the acromioclavicular joint. Arthrosc Tech 4:e681–e685. https://doi.org/10.1016/j.eats.2015.07.029
Carofino BC, Mazzocca AD (2010) The anatomic coracoclavicular ligament reconstruction: surgical technique and indications. J Shoulder Elbow Surg 19:37–46. https://doi.org/10.1016/j.jse.2010.01.004
Chronopoulos E, Kim TK, Park HB, Ashenbrenner D, McFarland EG (2004) Diagnostic value of physical tests for isolated chronic acromioclavicular lesions. Am J Sports Med 32:655–661. https://doi.org/10.1177/0363546503261723
Costic RS, Labriola JE, Rodosky MW, Debski RE (2004) Biomechanical rationale for development of anatomical reconstructions of coracoclavicular ligaments after complete acromioclavicular joint dislocations. Am J Sports Med 32:1929–1936. https://doi.org/10.1177/0363546504264637
Cote MP, Wojcik KE, Gomlinski G, Mazzocca AD (2010) Rehabilitation of acromioclavicular joint separations: operative and nonoperative considerations. Clin Sports Med 29:213–228. https://doi.org/10.1016/j.csm.2009.12.002
Debski RE, Parsons IM, Woo SL, Fu FH (2001) Effect of capsular injury on acromioclavicular joint mechanics. J Bone Joint Surg Am 83:1344–1351. https://doi.org/10.2106/00004623-200109000-00009
Dick R, Ferrara MS, Agel J, Courson R, Marshall SW, Hanley MJ, Reifsteck F (2007) Descriptive epidemiology of collegiate men’s football injuries: national collegiate athletic association injury surveillance system, 1988–1989 through 2003–2004. J Athl Train 42:221–233
Dyrna F, Berthold DP, Feucht MJ, Muench LN, Martetschläger F, Imhoff AB, Mazzocca AD, Beitzel K (2019) The importance of biomechanical properties in revision acromioclavicular joint stabilization: a scoping review. Knee Surg Sports Traumatol Arthrosc 27:3844–3855. https://doi.org/10.1007/s00167-019-05742-6
Dyrna F, Imhoff FB, Haller B, Braun S, Obopilwe E, Apostolakos JM, Morikawa D, Imhoff AB, Mazzocca AD, Beitzel K (2018) Primary stability of an acromioclavicular joint repair is affected by the type of additional reconstruction of the acromioclavicular capsule. Am J Sports Med 46:3471–3479. https://doi.org/10.1177/0363546518807908
Faraj AA, Ketzer B (2001) The use of a hook-plate in the management of acromioclavicular injuries. Report of ten cases. Acta Orthop Belg 67:448–451
Flik K, Lyman S, Marx RG (2005) American collegiate men’s ice hockey: an analysis of injuries. Am J Sports Med 33:183–187. https://doi.org/10.1177/0363546504267349
Frank RM, Cotter EJ, Leroux TS, Romeo AA (2019) Acromioclavicular joint injuries: evidence-based treatment. J Am Acad Orthop Surg 27:e775–e788. https://doi.org/10.5435/JAAOS-D-17-00105
Fukuda K, Craig E, An K, Cofield R, Chao E (1986) Biomechanical study of the ligamentous system of the acromioclavicular joint. J Bone Joint Surg Am 68:434–440
Gabbett TJ, Domrow N (2005) Risk factors for injury in subelite rugby league players. Am J Sports Med 33:428–434. https://doi.org/10.1177/0363546504268407
Gowd AK, Liu JN, Cabarcas BC, Cvetanovich GL, Garcia GH, Manderle BJ, Verma NN (2019) Current concepts in the operative management of acromioclavicular dislocations: a systematic review and meta-analysis of operative techniques. Am J Sports Med 47:2745–2758. https://doi.org/10.1177/0363546518795147
Grutter PW, Petersen SA (2005) Anatomical acromioclavicular ligament reconstruction: a biomechanical comparison of reconstructive techniques of the acromioclavicular joint. Am J Sports Med 33:1723–1728. https://doi.org/10.1177/0363546505275646
Gstettner C, Tauber M, Hitzl W, Resch H (2008) Rockwood type III acromioclavicular dislocation: surgical versus conservative treatment. J Shoulder Elbow Surg 17:220–225. https://doi.org/10.1016/j.jse.2007.07.017
Headey J, Brooks JHM, Kemp SPT (2007) The epidemiology of shoulder injuries in English professional rugby union. Am J Sports Med 35:1537–1543. https://doi.org/10.1177/0363546507300691
Hibberd EE, Kerr ZY, Roos KG, Djoko A, Dompier TP (2016) Epidemiology of acromioclavicular joint sprains in 25 national collegiate athletic association sports: 2009–2010 to 2014–2015 academic years. Am J Sports Med 44:2667–2674. https://doi.org/10.1177/0363546516643721
Jari R, Costic RS, Rodosky MW, Debski RE (2004) Biomechanical function of surgical procedures for acromioclavicular joint dislocations. Arthroscopy 20:237–245. https://doi.org/10.1016/j.arthro.2004.01.011
Jones HP, Lemos MJ, Schepsis AA (2001) Salvage of failed acromioclavicular joint reconstruction using autogenous semitendinosus tendon from the knee. Surgical technique and case report. Am J Sports Med 29:234–237. https://doi.org/10.1177/03635465010290022001
Kaplan LD, Flanigan DC, Norwig J, Jost P, Bradley J (2005) Prevalence and variance of shoulder injuries in elite collegiate football players. Am J Sports Med 33:1142–1146. https://doi.org/10.1177/0363546505274718
Kay J, Memon M, Alolabi B (2018) Return to sport and clinical outcomes after surgical management of acromioclavicular joint dislocation: a systematic review. Arthroscopy 34:2910–2924.e1. https://doi.org/10.1016/j.arthro.2018.04.027
Kelly BT, Backus SI, Warren RF, Williams RJ (2002) Electromyographic analysis and phase definition of the overhead football throw. Am J Sports Med 30:837–844. https://doi.org/10.1177/03635465020300061401
Klimkiewicz JJ, Williams GR, Sher JS, Karduna A, Des Jardins J, Iannotti JP (1999) The acromioclavicular capsule as a restraint to posterior translation of the clavicle: a biomechanical analysis. J Shoulder Elbow Surg 8:119–124. https://doi.org/10.1016/s1058-2746(99)90003-4
Laprade RF, Surowiec RK, Sochanska AN, Hentkowski BS, Martin BM, Engebretsen L, Wijdicks CA (2014) Epidemiology, identification, treatment and return to play of musculoskeletal-based ice hockey injuries. Br J Sports Med 48:4–10. https://doi.org/10.1136/bjsports-2013-093020
Lee SJ, Nicholas SJ, Akizuki KH, McHugh MP, Kremenic IJ, Ben-Avi S (2003) Reconstruction of the coracoclavicular ligaments with tendon grafts: a comparative biomechanical study. Am J Sports Med 31:648–655. https://doi.org/10.1177/03635465030310050301
LeVasseur MR, Mancini MR, Berthold DP, Cusano A, McCann GP, Cote MP, Gomlinski G, Mazzocca AD (2021) Acromioclavicular joint injuries: effective rehabilitation. Open Access J Sports Med 12:73–85. https://doi.org/10.2147/oajsm.s244283
Li X, Ma R, Bedi A, Dines DM, Altchek DW, Dines JS (2014) Management of acromioclavicular joint injuries. J Bone Joint Surg Am 96:73–84. https://doi.org/10.2106/JBJS.L.00734
Lyons FA, Rockwood CAJ (1990) Migration of pins used in operations on the shoulder. J Bone Joint Surg Am 72:1262–1267
Mallon WJ, Colosimo AJ (1995) Acromioclavicular joint injury in competitive golfers. J South Orthop Assoc 4:277–282
Maziak N, Audige L, Hann C, Minkus M, Scheibel M (2019) Factors predicting the outcome after arthroscopically assisted stabilization of acute high-grade acromioclavicular joint dislocations. Am J Sports Med 47:2670–2677. https://doi.org/10.1177/0363546519862850
Mazzocca AD, Arciero RA, Bicos J (2007) Evaluation and treatment of acromioclavicular joint injuries. Am J Sports Med 35:316–329. https://doi.org/10.1177/0363546506298022
Mazzocca AD, Conway JE, Johnson S, Rios CG, Dumonski ML, Santangelo SA, Arciero RA (2004) The anatomic coracoclavicular ligament reconstruction. Oper Tech Sports Med 12:56–61. https://doi.org/10.1053/j.otsm.2004.04.001
Mazzocca AD, Santangelo SA, Johnson ST, Rios CG, Dumonski ML, Arciero RA (2006) A biomechanical evaluation of an anatomical coracoclavicular ligament reconstruction. Am J Sports Med 34:236–246. https://doi.org/10.1177/0363546505281795
McFarland EG, Blivin SJ, Doehring CB, Curl LA, Silberstein C (1997) Treatment of grade III acromioclavicular separations in professional throwing athletes: results of a survey. Am J Orthop 26:771–774
McKay CD, Tufts RJ, Shaffer B, Meeuwisse WH (2014) The epidemiology of professional ice hockey injuries: a prospective report of six NHL seasons. Br J Sports Med 48:57–62. https://doi.org/10.1136/bjsports-2013-092860
Melvin PR, Souza S, Mead RN, Smith C, Mulcahey MK (2018) Epidemiology of upper extremity injuries in NCAA men’s and women’s ice hockey. Am J Sports Med 46:2521–2529. https://doi.org/10.1177/0363546518781338
Mikek M (2008) Long-term shoulder function after type I and II acromioclavicular joint disruption. Am J Sports Med 36:2147–2150. https://doi.org/10.1177/0363546508319047
Millett PJ, Horan MP, Warth RJ (2015) Two-year outcomes after primary anatomic coracoclavicular ligament reconstruction. Arthroscopy 31:1962–1973. https://doi.org/10.1016/j.arthro.2015.03.034
Minkus M, Hann C, Scheibel M, Kraus N (2017) Quantification of dynamic posterior translation in modified bilateral Alexander views and correlation with clinical and radiological parameters in patients with acute acromioclavicular joint instability. Arch Orthop Trauma Surg 137:845–852. https://doi.org/10.1007/s00402-017-2691-1
Mosenthal W, Kim M, Holzshu R, Hanypsiak B, Athiviraham A (2017) Common ice hockey injuries and treatment: a current concepts review. Curr Sports Med Rep 16:357–362. https://doi.org/10.1249/JSR.0000000000000402
Mouhsine E, Garofalo R, Crevoisier X, Farron A (2003) Grade I and II acromioclavicular dislocations: results of conservative treatment. J Shoulder Elbow Surg 12:599–602. https://doi.org/10.1016/s1058-2746(03)00215-5
Muench LN, Kia C, Jerliu A, Murphy M, Berthold DP, Cote MP, Arciero RA, Mazzocca AD (2019) Functional and radiographic outcomes after anatomic coracoclavicular ligament reconstruction for type III/V acromioclavicular joint injuries. Orthop J Sports Med 7:2325967119884539. https://doi.org/10.1177/2325967119884539
Norrell HJ, Llewellyn RC (1965) Migration of a threaded steinmann pin from an acromioclavicular joint into the spinal canal: a case report. J Bone Joint Surg Am 47:1024–1026
Rios CG, Mazzocca AD (2008) Acromioclavicular joint problems in athletes and new methods of management. Clin Sports Med 27:763–788
Schlegel TF, Burks RT, Marcus RL, Dunn HK (2001) A prospective evaluation of untreated acute grade III acromioclavicular separations. Am J Sports Med 29:699–703. https://doi.org/10.1177/03635465010290060401
Sethi GK, Scott SM (1976) Subclavian artery laceration due to migration of a Hagie pin. Surgery 80:644–646
Shaw MBK, McInerney JJ, Dias JJ, Evans PA (2003) Acromioclavicular joint sprains: the post-injury recovery interval. Injury 34:438–442. https://doi.org/10.1016/s0020-1383(02)00187-0
Simovitch R, Sanders B, Ozbaydar M, Lavery K, Warner JJP (2009) Acromioclavicular joint injuries: diagnosis and management. J Am Acad Orthop Surg 17:207–219. https://doi.org/10.5435/00124635-200904000-00002
Stucken C, Cohen SB (2015) Management of acromioclavicular joint injuries. Orthop Clin North Am 46:57–66. https://doi.org/10.1016/j.ocl.2014.09.003
Tamaoki MJ, Lenza M, Matsunaga FT, Belloti JC, Matsumoto MH, Faloppa F (2019) Surgical versus conservative interventions for treating acromioclavicular dislocation of the shoulder in adults. Cochrane Database Syst Rev 10:CD7429. https://doi.org/10.1002/14651858.CD007429.pub3
Tamaoki MJS, Belloti JC, Lenza M, Matsumoto MH, Gomes Dos Santos JB, Faloppa F (2010) Surgical versus conservative interventions for treating acromioclavicular dislocation of the shoulder in adults. Cochrane Database Syst Rev 2010:CD7429. https://doi.org/10.1002/14651858.CD007429.pub2
Tischer T, Salzmann GM, El-Azab H, Vogt S, Imhoff AB (2009) Incidence of associated injuries with acute acromioclavicular joint dislocations types III through V. Am J Sports Med 37:136–139. https://doi.org/10.1177/0363546508322891
Tossy JD, Mead NC, Sigmond HM (1963) Acromioclavicular separations: useful and practical classification for treatment. Clin Orthop Relat Res 28:111–119
Trainer G, Arciero RA, Mazzocca AD (2008) Practical management of grade III acromioclavicular separations. Clin J Sport Med 18:162–166. https://doi.org/10.1097/JSM.0b013e318169f4c1
Weinstein DM, McCann PD, McIlveen SJ, Flatow EL, Bigliani LU (1995) Surgical treatment of complete acromioclavicular dislocations. Am J Sports Med 23:324–331. https://doi.org/10.1177/036354659502300313
White LM, Ehmann J, Bleakney RR, Griffin AM, Theodoropoulos J (2020) Acromioclavicular joint injuries in professional ice hockey players: epidemiologic and MRI findings and association with return to play. Orthop J Sports Med 8:2325967120964474. https://doi.org/10.1177/2325967120964474
Williams GR, Nguyen VD, Rockwood CA (1989) Classification and radiographic analysis of acromioclavicular dislocations. Appl Radiol 18:29–34
Yang JS, Voss A, Apostolakos J, Mazzocca AD (2016) Arthroscopic treatment of acromioclavicular joint osteolysis, arthritis, and instability, 5th edn. Rockwood and Matsen’s the shoulder. Elsevier, , pp 757–766
Funding
The University of Connecticut Health Center/UConn Musculoskeletal Institute has received funding and material support from Arthrex Inc. (Naples, FL, USA). The company did not influence the data collection or writing of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
A.D. Mazzocca reports research grants from Arthrex Inc., is a consultant for Arthrex Inc., and receives royalties from Arthrex Inc. B.C. Hawthorne, P. Garvin, J. Messina, A. Cusano, S. Greiner and A. Voss declare that they have no competing interests.
This article does not contain any studies with human participants or animals performed by any of the authors.
Additional information

Scan QR code & read article online
Rights and permissions
About this article

Cite this article
Hawthorne, B.C., Garvin, P., Messina, J. et al. Acromioclavicular joint pathology in athletes. Obere Extremität 17, 12–20 (2022). https://doi.org/10.1007/s11678-021-00675-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11678-021-00675-4