
Abstract
The rise of surrogacy in India over the last decade has helped individuals across the world to realize their parenting aspirations. In the macro-context of poverty in India and the hierarchical and patriarchal family set-up, concerns are expressed about coercion of women to participate in surrogacy. While the ethical issues engulfing surrogacy are widely discussed, not much is known about the role women play in the decision-making to participate in surrogacy. The paper aims to addresses this gap and is based on a part of a larger ethnographic study conducted at a surrogacy clinic in Anand, Gujarat, India. We explored experiences of forty-one surrogate mothers using in-depth interviews and analysed the narratives to identify women’s own perceived role in the decision-making to participate in surrogacy. Narratives describing the decision-making process were identified and treated as a preliminary unit of analysis. We examined the use of singular and plural pronouns like “I,” “me,” and “mine” versus “we,” “us,” and “our,” along with the use of active and passive voice to determine whether women assumed responsibility for the decision to participate in surrogacy or they attributed the decision to others. Findings unravelled the complexities of the decision-making process and indicated that eighty-five percent of the women played an active role in the decision-making to participate in surrogacy, albeit with new avenues of exploitation in the commercial market space and raised serious bioethical concerns.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Use of assisted reproductive technology (ART) and gestational surrogacy (henceforth surrogacy) has undergone phenomenal growth in India over the last decade. India has emerged as a global surrogacy hub with its liberal approach to surrogacy offering a safe haven to same-sex and heterosexual couples as well as single individuals seeking domestic or transnational surrogacy services (Chang 2009; Sengupta 2010). In response to wide-ranging critiques, India prohibited provision of surrogacy services to foreign nationals in 2015 (Ministry of Health and Family Welfare 2015) and later proposed a full ban on commercial surrogacy, permitting only altruistic surrogacy through the Surrogacy (Regulation) Bill 2016. The bill intends to prevent women from entering surrogacy as a forced choice to escape poverty; yet fails to acknowledge that in Indian families, hierarchical relationships and familial obligations may push women in altruistic surrogacy to help kin experiencing infertility. Gupta (2000) reported that prior to the boom of commercial surrogacy, surrogate mothers in India were always related to the couple seeking their services, indicating the possibility of their subjugation at a familial level. Egg donors in Delhi, India, were found to be pressured for egg donation to close relatives experiencing infertility (Gupta and Richters 2008). A study by the Centre for Social Research (2012) covering three towns and two metropolitan areas in India reported that the husbands coerced Indian surrogate mothers for participation in paid surrogacy, though the report did not present empirical data to validate the claim. The agency of surrogate mothers in India continues to be debated amidst a paucity of empirical evidence.
The move to regulate the burgeoning surrogacy industry in India is a welcome step, though the voices of surrogate mothers are missing in the formation of policy intended to safeguard them. A lacuna in the policy discourse is the agency of surrogate mothers; it is crucial to understand how Indian women arrive at the decision to offer paid surrogacy services and to understand their agency throughout their surrogacy journey. Concerns about socio-economic injustice through which domestic and transnational surrogacy arrangements have thrived in India, although valid, often fail to acknowledge ways in which women exercise agency in seemingly oppressive conditions. A non-Eurocentric understanding of the ethics of decision-making and autonomy is critical to form a context sensitive policy for regulation of surrogacy services in India. This paper aims to address the gap based on an in-depth ethnographic study conducted with surrogate mothers in Gujarat, India.
A Macro Context of Surrogacy in India
The right to reproduce has a long history of political control marked by inequalities of class, gender, nation, race, and sexuality. The neo-liberal globalized market has led to increased yet differential access to ART services in India. Health insurance companies do not cover the costs incurred for ART services, limiting its access to the wealthy and marginalizing the reproductive rights of the poor (Mulay and Gibson 2006; Sarojini 2010). Many Indian women lack access to high standards of reproductive care during their own pregnancies but receive it when they gestate babies for others (Jaiswal 2012). The Indian surrogacy industry is thus condemned as a form of neo-colonial exploitation in a globalized world (Vora 2009). Surrogate mothers are often at an educational and economic disadvantage and are resource-poor compared to the clients seeking their services, thereby making them vulnerable. Women may not entirely be aware of the complexities of the surrogacy process and the short-term and long-term impact of participation on their health (Centre for Social Research 2012; Pande 2009; Unnithan 2010; Vora 2009).
In the context of the colonial history of India, surrogate mothers are likely to view medical practitioners in an authority position, are dependent on them for information, and lack legal representation. As medical professionals become a common party representing both the commissioning parents and the surrogate mothers, in matters of conflict the interests of the paying party are likely to prevail (Deonandan, Green, and Van Beinum 2012; Qadeer 2010). ART clinics in India routinely transfer more than one embryo to the recipient surrogate mothers and tend to gloss over the risks of multiple gestations—selective reduction of foetuses and consequent abortion in some cases, complications during pregnancy and childbirth, and preterm delivery (Qadeer and John 2009). Indian clinics offering surrogacy services, however, assert that surrogacy creates an avenue for the surrogate mothers to alleviate poverty and can be an empowering experience (Saravanan 2010; Vora 2010).
Scholars are increasingly questioning the portrayal of poor women in the third world as victims of varying contexts and passive acceptors of subjugation lacking agency. In a review of popular discourse on surrogacy in the United States during 2002 to 2012, Fixmer-Oraiz (2013) revealed that altruism was promoted as an exclusively western trait through a discourse that presented intended parents as having philanthropic motivations of alleviating the poverty of the Indian surrogate mothers or presented U.S.-based domestic surrogate mothers as entering surrogacy “out of the love for others.” On the contrary, the surrogate mothers in India were portrayed as victims of poverty who mitigated financial constraints through a conscious decision to participate in paid surrogacy. A narrative of “mutually beneficial” surrogacy endeavour easily dismissed any concerns regarding the vulnerability of women. Recent ethnographic studies of surrogacy in India have revealed the agentic role of the surrogate mothers. In a study based in Gujarat, India, Pande (2009) highlighted “everyday forms of resistance”—discursive practices surrogate mothers engaged in to remediate the stigma and resist subordination during surrogacy. Surrogate mothers created symbolic moral boundaries to distance themselves from sex work and child selling, downplayed choice, denied disposability by considering themselves special, and made claims over the baby through labour of gestation and shared bodily fluids—like blood and breast milk. Forde (2016) and Deomampo (2013) reported that participation in surrogacy was a conscious decision for the women in Mumbai and most of them were far from the image of victimized women—neither economically desperate nor pushed into surrogacy by their in-laws. Instead, women asserted their participation in surrogacy to their disapproving husbands.
Agency of the Relational Selves
Individualistic conception of agency frames agents as individual actors and when applied in the settings where self is constructed in relation to the others does not yield a coherent account of the actions agents engage in. The cultural psychology perspective to individual development (Shweder et al. 2006) formed the theoretical framework for the ethnographic work presented here. It allowed framing of agency in a relational context wherein surrogate mothers in the context of their family relations were viewed as relational agents. A large body of literature in cultural psychology is devoted to the understanding of the self as a relational agent and is summarized by Shweder et al. (2006) as:
-
self in relation to others determines the individual experiences and the self cannot be abstracted from the social context
-
self is experienced by accommodating with others and creating and fulfilling obligations to become part of various interpersonal relations
-
such an interdependent sense of self calls for agency in the form of high degrees of self-control directed towards personal desires and goals and emotions that may conflict with expectations of others, self-discipline, adjustment, and attending to the situational demands.
Exercise of agency is thus situational and dynamic—it may vary depending on the social standing of the agent in a specific situation, gender, the relative place of the agent in the social hierarchy, and the duties and obligations of the relationship in question. Menon (2011) suggested that fulfilling duties and the expectations of others might generate a sense of satisfaction among Hindu Indians and agency thus takes the form of catering to the needs of significant others. Ganesh (1999) viewed Indian women as active constructors of their own realities through negotiation skills which are central to the “capacity to adjust.” Ethnographic explorations of two cohorts of Hindu Gujarati women—a younger cohort situated in Gujarat and an older cohort located in Canada—by Raval (2009) indicated that women engaged in negotiation within the context of their familial roles when faced with conflicts, rather than manifesting resistance or passive acceptance of role-based social ideals. Personal desires in conflict were rarely self-centred, revolved around the needs or well-being of their children, and were resolved by thinking through the situational demands for optimizing the benefits for their children. Chaudhary (2012) states that interconnectedness may allow for flexibility in relationships where Indian women negotiate their agency within familial and social spaces. She suggests that a representation of Indian women as a homogeneous category is problematic in the context of their regional, linguistic, ethnic, religious, social, familial, and life-stage diversity, and women’s experiences must be studied with keen attention to their subjective position in the familial and social hierarchy.
Pande (2010) highlighted that unlike other parts of the world, surrogacy in India is a particularly stigmatized form of work; it is equated with sex work, due to the long absence of the women from the marital household for surrogacy and due to the stigma of bearing children outside of wedlock. Consequently, most women prefer to maintain secrecy about their surrogacy endeavour. Such secrecy may further compromise the well-being of surrogate mothers in the absence of a robust monitoring system for the ART industry. Women enter surrogacy unprotected by stringent regulatory measures, have limited education and few opportunities to participate in organized labour, and live in poverty. Their context is particularly limiting compared to the women Menon (2011) and Raval (2009) studied. In this context of stigma, secrecy, and especially oppressive conditions under which women enter surrogacy, it is extremely crucial to study their agency and decision-making process.
Methodology
The findings presented here are derived from a larger ethnographic study exploring psychosocial experiences of surrogate mothers in Anand, Gujarat, India. The study explored the experiences of forty-one surrogate mothers through participant observation and in-depth interviews at a surrogacy clinic over a period of nine months during 2012–2013. Participation in surrogacy required the women to live in the geographical boundaries of the clinic or at one of the two surrogate hostels for almost a year as they underwent the surrogacy regimen. Shared living with the fellow surrogate mothers and close contact with the medical practitioners, albeit temporary in nature, created a community with its own distinct ideologies, shared beliefs, practices, and language. The ethnographic approach was used to capture the essence of this “community of interest”—people who have experienced a common phenomenon of interest and who may or may not interact regularly (Angrosino 2007).
Gaining Access to the Field
In ethnographic research, access is negotiated and renegotiated at multiple levels of the research project (Gobo 2008). Gaining access to the field was a cyclic process at two levels, that of the settings and the individuals. Official permission from the infertility specialist was the stepping stone for the fieldwork, and later access was navigated through surrogacy hostel matrons and the surrogate mothers. The “participant-as-observer” role was adopted, wherein the researcher was completely immersed in the field to observe the daily routines of surrogate mothers and was known to them as conducting research with prior permission and their consent. In the initial months of fieldwork, the researcher introduced herself and her research interests to the surrogate mothers in small groups and to anyone else who expressed interest in the researchers’ presence using a detailed consent form (Gujarati/Hindi). The consent form explained the purpose and duration of the study, what participation in research entailed, and the associated risks, confidentiality and rights of participants during participation. Voluntary participation was repeatedly stressed while seeking the participation of the women. Prior to each interview, the consent form was re-explained to the individual surrogate mothers and a copy of the form was shared for detailed reading and future reference. The women were particularly interested in knowing how the researcher planned to use the audio recordings, whether the recordings would be shared with other people, whether the researcher was planning to write anything about them in the newspapers, and whether their real names would be revealed. The researcher spent considerable time explaining the plan to manage and use the information shared, showed them dummy transcripts with pseudonyms, and assured them of confidentiality.
The researcher invested time in befriending surrogate mothers and matrons at the hostels as well as receptionists, nurses, and medical practitioners at the clinic. This involved casual talks with several people, asking them questions pertinent to plan fieldwork, participating in the daily routine at the hostels, and a lot of self-disclosure. At the later stages of fieldwork, the participant role also involved providing emotional support and comfort to the surrogate mothers experiencing health complications and miscarriages. Adopting a “participant-as-observer” role was a continuous process—both planned and spontaneous—that established the researcher’s credibility as a trustworthy person, which greatly aided and shaped the research process.
Sample and Sampling Techniques
Stratified purposive sampling, along with a combination of techniques like maximum variation, snowball, and opportunistic sampling was used to select women at varied stages of the surrogacy treatment. Synergetic processes of data collection and analysis allowed continuous refinement of the research focus to explore emergent themes. Theoretical saturation marked by the repetitive occurrence of similar patterns in the data gathered from women at various stages of surrogacy marked sampling saturation at forty-one. The interviewing process was completed when interactions with women ceased to provide additional insights about the phenomenon. The emerged sampling distribution is presented in Table 1.
Tools for Data Collection
A brief structured survey captured background details of the women. Qualitative data were generated through observations, semi-structured in-depth interviews with the surrogate mothers, interactions with the medical practitioners and hostel matrons, and opportunistic discussions with the family members of the surrogate mothers and a commissioning mother. Thematic analysis was used to search for patterns in the data and to interpret it for generating explicit and implicit meanings. A combination of inductive and deductive analysis was used.
Profile of the Surrogate Mothers
The mean age of the women was thirty-one years with an age range of twenty-two to thirty-nine years. The majority (90%) were currently married, 5 percent were separated, and another 5 percent were widowed. More than half of the women (64%) lived in nuclear households, followed by 24 percent living with extended family members and 12 percent living in a joint family. The average family size was five, generally with two dependent members, mostly children. Representation of Hindus was highest (66%), followed by Christians (29%) and Muslims (5%). Overwhelming 61% of the women belonged to scheduled castes and other disadvantaged classes. Educational attainment was low, with 22 percent of the women with no literacy, 19 percent with primary education, 37 percent with secondary education, and 10 percent with higher secondary schooling. Another 12 percent had completed a diploma or graduate studies. Women were either unemployed (32%) or engaged in agricultural work (17%) or odd jobs (32%). The few (19%) who worked in the organized employment sector were poorly paid. The average monthly family income for a five-member family was INR 5900. This socio-economic profile of the women confirms the macro context of poverty, where poor educational attainments had led to limited livelihood opportunities for women largely from the marginalized sections of the society.
Results
Ahearn (2001) and Duranti (2004) suggest that a keen attention to language and linguistic forms can elucidate micro and macro processes of agency. All languages have multiple ways of representing and mitigating agency and offer linguistic framework choices to speakers to mention or omit the agent responsible for an event. There is cross-linguistic evidence on the use of impersonal, passive-like, and passive constructions as a means of agency mitigation and to avoid blaming specific parties; of course, not all passive constructions can be assumed to purely serve the purpose of agency mitigation, nor are they the only way of mitigating agency. While linguistic anthropologists have demonstrated that languages of the world differ in the ways they express agency and delve deep into the analysis of how language and agency are intertwined (Duranti 2004); here we limit linguistic analysis of the women’s narratives to identifying their own perceived role in the decision-making to participate in surrogacy. Based on Roland’s (1988) concept of the “expanding self”—when a predominant “we-self” experienced by the Indians comes in contact with global civilizational forces and social change, it grows in individuation—we explored narratives of women for the degree of individuation reflected and the complexities they experienced in the decision-making process.
Interviews began with a generative question asking women to narrate their surrogacy journey; an interview guide was used to understand their experiences, including those during decision-making to participate in surrogacy, unfolding of events, and the dilemmas and feelings women experienced. Narratives describing the decision-making process were identified and treated as a preliminary unit of analysis. We examined the use of singular pronouns like “I,” “me,” and “mine,”, as well as plural pronouns like “we,” “us,” and “our” by the women, along with the use of active and passive voice to determine whether women assumed responsibility for the decision to participate in surrogacy or they attributed the decision to others. The assumption was that the women who played a key role in the decision-making were more likely to use singular pronouns and active voice in their narrations of the process. Further, we undertook a thorough within-case-analysis of the data gathered from multiple sources: in-depth interviews, conversations, observations, and field notes to examine re-occurrences, inconsistencies, and temporality in the decision-making process. The extent of control women displayed in the decision-making process and contextual details and events shared by the women informed interpretations to form three mutually exclusive categories of women: those who engaged in predominantly individual decision making, those who engaged in mutual decision making, and those for whom spouses took the decision for participation in surrogacy. The decisions were rarely straightforward, and the results are organized in two sections: the role of women in decisions to participate in surrogacy, and the complexities of the decision-making process. The words of the woman were recorded verbatim and then translated into English.
Role of Women in the Decision to Participate in Surrogacy
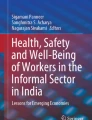
The majority of the women (68%) played a lead role in making the decision and convinced their reluctant spouse about participation in surrogacy. Seventeen percent of the women experienced it as a mutually initiated endeavour wherein both women and their spouse were favourable towards participation, and 15 percent of the women initiated surrogacy on the request or insistence of their spouse (Figure 1).

Women’s perception of the role they played in the decision-making to participate in surrogacy (n=41)
Of the 68 percent women who played a lead role in initiating surrogacy, all but two cited resistance by their spouse for one or more reasons (Figure 2).

Reasons for spousal resistance for women’s participation in surrogacy (n=26)
In line with the previous findings of Pande (2009), women revealed that surrogacy was equated in public opinion with sex work and child selling and was perceived as an immoral and stigmatized form of work, resulting in spousal resistance. Non-sexual reproduction was unimaginable for surrogate mothers and their spouses until agents and/or medical practitioners briefed them about the biomedical process involved in surrogacy. Women and their spouses anticipated stigma for moral transgression because of the prolonged absence of the woman from the household during surrogacy and because of conception outside marriage, as well as the woman’s economic contributions being viewed as showing the incompetence of the man as a primary provider for family. Men anticipated a role reversal due to the absence of their wives during the period of institutionalization for surrogacy and resisted it for the possible distortion of family life. Health concerns were articulated less frequently as a reason for spousal resistance, indicating the possibility of trivialization of the risks involved in surrogacy. Men viewed the earnings of women and the associated power gains as a threat to their authority within the family; nevertheless, women persuaded their husband and family about participation in surrogacy. Decision-making for participation in surrogacy therefore involved significant work on the part of women, wherein they invested effort in convincing their reluctant spouses and, at times, extended family members over a few months or a couple of years.
The narratives of women who appeared to play a primary role in the decision-making revealed their resolve. Rukshar (thirty-six years), a former nursemaid at a maternity clinic, shared her journey from an initial disbelief about the authenticity of surrogacy and the profits involved when she first heard of it from a fellow passenger on a bus ride (former surrogate) to her firm resolve to participate in surrogacy. In her words:
At that time I thought, how can a child be conceived like that? I was illiterate; therefore, I could not understand it…Then I asked my husband, “Is that true?” He said, “It is possible, I have read such an article in the newspaper.” Later one day, I saw in the news that one mother became a surrogate for her daughter who could not conceive. Eventually, the thought struck me, that it is possible. Then I decided, I will become (a surrogate). At least once, I will become (a surrogate) certainly.
Rukshar then visited the clinic alone to enquire about surrogacy only to learn that spousal consent was mandatory for participation. She convinced her reluctant husband to visit the clinic and delayed her participation for a year on his insistence until their son completed his grade ten exam, and she maintained secrecy about her surrogacy endeavour, anticipating the resistance of extended family members. Within a year of her first surrogate delivery, Rukshar convinced her husband and the medical practitioner for repeating surrogacy to make the most out of her reproductive potential before she reached menopause. With the money earned, she aspired to own a home, to change the destiny of her son by providing him with an engineering college education, and to accumulate savings for her daughter’s wedding.
Hiteshi (35 years), a former housemaid and a second-time surrogate mother, shared that she was unhappy living in poverty and was inspired when she witnessed the newly acquired affluence of her sister-in-law (brothers’ wife) through participation in surrogacy.
My sister-in-law became (a surrogate). Seeing her standard of living, even I felt that I should become (a surrogate) once. Then I decided, I must embrace this path (of surrogacy) to happiness …
Hiteshi decided to try it, but her husband resisted, worried that with the income earned Hiteshi would be independent, would buy a home, and might desert him or even ask for a divorce. Hiteshi then took a soft stance, stating that the money earned through surrogacy would be spent eventually, that she would always depend on him, and that both of them could live happily together through the money earned. Ultimately tired of trying to persuade him, Hiteshi separated and started living with her parents; she agreed to reunite only against his signature on the consent form for her participation in surrogacy.
These and many other similar narratives of women demonstrate the predominant use of singular pronouns in Gujarati—“hun” (I), “me” (I), “mane” (me)—and in Hindi—including “main” (I) and “mujhe” (me). The use of verbs in active voice coupled with singular pronouns and the sequence of events convincing their spouses for participation in surrogacy revealed the primary role women (68%) played in the decision-making process.
The narratives of seventeen percent of women indicated that they did not experience spousal resistance to participation in surrogacy. These women also used plural pronouns in combination with singular pronouns while describing their experiences, indicating a mutual decision to participate in surrogacy between them and their spouse. The plural pronouns used in Gujarati included “ame” (we), “aapde” (we), “amane” (to us). A first-time surrogate mother, Prerna (22 years)—a professional nurse—donated eggs twice to meet her immediate financial needs when she and her husband, along with their toddler, moved out of the joint family household to set up their own separate living space. Her neighbour introduced them to the clinic, and during her egg donation stints, she and her husband grew familiar with the clinic, gained confidence in the authenticity of surrogacy, and decided to participate. Prerna narrated her experience as follows:
A couple of times we donated eggs, so we had experienced it all. My husband would accompany me, and he too understood everything. Therefore, we didn’t especially take a decision as such. My husband and I were doing back and forth visits here (clinic) therefore we knew everything, that the pregnancy through medication was possible. Therefore, we didn’t discuss it much. Then my husband said, “If you want to go, it’s your will. I am not refusing you.” Therefore, there wasn’t much of a discussion or deliberation. Then I was willing and he (husband) was desirous too. Therefore, I came into surrogacy.
Prerna’s narrative, as well as being indicative of the mutual role she and her spouse played in the decision-making, also exemplifies the complexity of the process. Her husband’s revelation that he was not against Prerana’s participation in surrogacy appears to have shaped their joint decision; however, throughout her narrative another consistently reoccurring theme is that her husband refused to take responsibility of any adverse outcomes of the surrogacy. This theme consistently appeared in other interviews, where husbands hesitated due to concerns that extended family members and society would accuse them of risking their wife’s life for monitory profits. In effect, the clinic through the legal agreement and the spouses through verbal discourse completely shifted the responsibility of any adverse outcomes of surrogacy on to the women.
Sargam (twenty-eight years), a homemaker, was a second-time surrogate mother with a young son. Her husband earned INR 3000 per month as a driver. When Sargam first heard of surrogacy, she was interested in participating, but her son was barely two years old. Her husband could not believe the authenticity of surrogacy and resisted her participation for the fear of stigma and in the absence of childcare support. Eventually, after meeting a medical practitioner at the clinic, he agreed to Sargam’s participation in surrogacy.
I felt, if we give away one child, we get so much money, what’s the problem in doing it then? It could make our life, our son’s life. (I) could provide him with a good education. At first, he (husband) argued with me that such things can’t be done. He said, “who will take care of our young son?” A year or two passed. When my son became three years old, I asked him (husband) again. He told me, “Let’s find out the details first.” We then came to the hospital… Both of us then decided that we should do this work. Then the medication began. (We thought that) if (we) earn some money it will come handy for our son.
Sargam’s narrative was neither assertive nor passive; she took initiative for participation in surrogacy and patiently waited for the right time when her husband was ready for participation in surrogacy. She also involved their distant relative—matron at the surrogate hostel—to build the confidence of her husband about the authenticity of surrogacy to convince him for the preliminary visit to the clinic.
The narratives of six women describing the decision-making process were predominantly passive and also indicated that their surrogacy was initiated by others. Such narratives revealed a range of women’s experiences, from others’ insistence on their participation in surrogacy to, in a rare case, grave threats for a share of the money earned through surrogacy. Though relatively small in numbers, these narratives indicate the need for developing a robust regulatory mechanism to prevent women from being pushed into surrogacy by others and to safeguard their interests.
Suman (thirty-two years), a first-time surrogate mother, revealed how she was bullied by her extended family members to participate in surrogacy. Suman’s husband had lost his leg in an accident, was unemployed, and was bullied by his siblings. In the absence of any earnings, Suman struggled to send her sons to school. Reluctant to offer financial support, extended family members suggested that Suman should participate in surrogacy. After persistent nagging by her in-laws, Suman had enrolled her sons in a boarding school and became a surrogate. She shared:
These people (relatives) brought me here. They assured me nothing will go wrong, (I) need not worry, I must demonstrate courage for (the well-being of) my children. I was sent here. I said, (to my brother-in-law) “send your wife.” He said, “no, we are scared.” They persuaded me for the last two years. Ultimately, I came here now.”
Suman’s narrative of participation in surrogacy initiated by others is laced with predominant use of passive voice. She further added that after her embryo transfer, extended family members started demanding money from her. Her experiences revealed not only exploitation in the context of family but also implications for the mental health of women. In her words:
My sister-in-law’s (husband’s sister) son often comes here drunk and asks for money; I told him, “I don’t have any money.” He therefore threatened me, saying, “I will abort it, my mother helped you get it, and I will get it aborted.” When I get my payment of 25,000 rupees, I will give him 10,000 for getting me here. My family members are such that they can kill for money.”
Narratives of women were closely scrutinized for any incongruence and subtle indications of participation in surrogacy against their will. Although women took ownership of the decision, at times their narratives indicated feelings of lack of choice and of compulsion to participate in surrogacy. Ramila’s narrative is one such example. Ramila (twenty-six years) was a homemaker and lived with her husband, two children, and parents-in-law in a small town. Her husband, the sole breadwinner of the family, drove a rickshaw and earned a meagre monthly income of INR 6500 to support the six-member family. He suffered from a prolonged illness, had mortgaged their home, and was in debt. Ramila shared:
My husband’s brother told (him); that’s how (we) came to know. Then he (husband) asked me, “Should we go—we have debts?” Therefore, I came. We had problems, therefore I agreed. I didn’t think—came because of the debt.”
Later Ramila shared that after an initial failed embryo transfer, her husband encouraged her for a second attempt, stating it would be successful whenever she was destined to conceive. Ramila was determined not to undergo a third trial if she failed to conceive again; but her second attempt was successful. When asked about a second surrogacy, Ramila exclaimed she could never think of doing it again. Although Ramila stated that her husband “asked” her for participation in surrogacy, whether Ramila was in any position to decline such a request from her husband is questionable. In addition, her life context also exposed her glaring poverty in which surrogacy may have seemed to her as a last and only resort for escape.
Initially, during the interview, Pooja (thirty-nine years), a mother of two and a first-time surrogate mother, shared that she willingly took up surrogacy to secure her children’s future. However, later she revealed that her husband had never allowed her to take up any paid job until he learnt of the enormous monetary gains possible through surrogacy. Despite being subtly pushed to overcome her initial hesitation for participation in surrogacy, Pooja defended her husband as “trusting” and therefore allowing her participation in surrogacy. In her words,
My husband told me, “You should go.” He immediately agreed. He is very trusting. In fact, I was reluctant to come (laughs). (I was) Thinking family members would gossip about me, and I had never taken any injections and I would have to (laughs), that is why I was reluctant. Then he said, “It’s not a bad (work), if anyone says anything, I am answerable.” Then he said, “You must go.” Therefore, I came. He never allowed me to take up (paid) work … stating he did not need my earnings (laughs). But now this because of hardships (of poverty)…
The surrogacy agents, largely former surrogate mothers, egg donors, or staff at the ART clinic, played a crucial role in recruiting women for surrogacy and received one-time compensation from the clinic after successful delivery. Over half of the surrogate mothers (51%) revealed that in the initial interactions, agents focused on the vulnerability of women through topics such as living in rental homes, limited income to educate children, health ailments of family members, alcohol addiction and/or unemployment of the spouse, debt, lack of access to profitable livelihood options, and inability to accumulate wealth despite persistent hard work. Agents then presented surrogacy as a lucrative solution to these limiting life circumstances, ensuring large sums of money in relatively shorter duration and eventually a secure future for their family (49%). Women and their spouses were persuaded to at least visit the ART clinic once to understand surrogacy (51%). Shalini (thirty-four years), a professional nurse, had undergone two unsuccessful embryo transfers and, at the time of the interview, was awaiting results of the third embryo transfer. She narrated how she was introduced into surrogacy by an agent:
I wanted to become a surrogate, but I was scared; therefore, I refused. The night shift lady told me everything. I said I want to come (for surrogacy). Then, she brought me (here). Then I refused, but she explained to me a lot saying, “You will be able to get your own home.” My in-laws would tell me every day, “Leave the home, it is our home.” Therefore, I decided to do this.
Shalini’s quote demonstrates how agents used persuasive power, focused on her limiting life circumstances, and posed surrogacy as the way out of the personal difficulties she faced.
Overall, despite the macro-context of poverty, where poor educational levels limited economic opportunities for men and women, a majority of women (85%) appeared to have control over the decision to participate in surrogacy. Experiences of fifteen percent of women indicated that both family members and surrogacy agents could subtly push women into surrogacy against their will, highlighting the need for a robust monitoring mechanism to prevent it. While agents pursued women to explore participation in surrogacy by stressing limiting life-contexts, family members—after knowing the profits involved—construed participation in surrogacy as a moral obligation of women towards family.
The Complexities of the Decision-Making Process to Participate in Surrogacy
Women’s narratives indicated that the decision to participate in surrogacy was rarely straightforward. Not only women, but their husbands, family members and surrogacy agents participated in decision-making, and different people took the lead at various times during decision-making. Kalika (thirty-five years), a first-time surrogate mother, was one of the most expressive participants in the study. Her reflections on her surrogacy journey indicated the fluidity of the decision-making process. Her hopes for a better life and her concerns over her health and safety during surrogacy were intertwined and left her indecisive about the participation in surrogacy. Eventually, Kalika, embedded in her familial context, prioritized the needs of her children and family and participated in surrogacy. The key events from her detailed narrative are presented sequentially in Figure 3, along with the key persons who played a lead role during decision-making.

Complexities in the decision to participate in surrogacy
The shifting positions of various persons during decision-making, as presented in Figure 3, are noteworthy. At the outset, Kalika’s “sister turned surrogacy agent” directly contacted Kalika’s husband, encouraging him to send Kalika for surrogacy. She possibly viewed him as a primary decision-maker in the family and was aware that the clinic did not accept women for surrogacy without spousal approval. Only at his outright refusal did she contact Kalika and highlight surrogacy as the only solution to her difficult life circumstances.
Kalika, convinced of the economic potential of surrogacy, was assertive with her husband about her desire to participate in surrogacy and challenged his fear of stigma. Even when he turned down her surrogacy proposal, Kalika did not give up and approached her sister for help. Initially, to avoid resistance from her husband, Kalika proposed that her sister could sign the consent form instead of her husband for Kalika’s participation in surrogacy. However, when her sister insisted that spousal consent was mandatory for participation, Kalika sought her help to convince husband. This was indicative of the alliances women may form in the familial setting to utilize collective power in pursuit of their own goals either to seek approval of the male family members or to override the decisions taken by men. Despite Kalika’s ability to assert and her success in convincing her spouse for a preliminary visit to the clinic, she was excluded from the visit. Her husband made it clear that he held the authority to make the decision. At this point, Kalika graciously accepted her husband’s lead, patiently waiting for his approval. This indicates that Kalika did acknowledge the power of her husband over crucial family decisions and chose to “negotiate” her goals when “assertion” did not work.
Kalika’s husband, during his inquiry at the clinic, ascertained the non-sexual nature of surrogacy. On returning home he shared with Kalika that there was nothing immoral in surrogacy and that death during surrogacy was the rarest possibility—a matter of her fate. Though initially taken aback, Kalika made up her mind to participate in surrogacy and requested her husband to seek the approval of her mother-in-law. Interestingly, while Kalika tried “assertion” with her husband, she insisted on “approval” of her mother-in-law and this time formed an alliance with the husband to convince her, indicating a highly contextual expression of agency through careful management of intimate hierarchical interpersonal relationships to attain personal goals. Mother-in-laws typically hold a powerful position in Indian families. Menon (2004; 2011) has reported the typical life-cycle of Hindu women, wherein young married women in their conjugal families gradually moved up the ladder of power position as they aged. A large body of literature on women’s autonomy and reproductive decision-making in India has indicated that extended family members, especially mother-in-laws, greatly influence the fertility decisions of young couples (Char, Saavala, and Kulmala 2010). Kohli (2016) shared that daughters-in-law in northern India accepted the dominance of mothers-in-law as a form of love and care, to ensure support for themselves and their children. Kalika thus appears to exercise agency in relation to the existing power structures of her family rather than resisting it.
The situation became only more complex when Kalika’s confidence wavered after obtaining the approval of her mother-in-law. What seemed a distant dream so far had now become a reality, forcing her to weigh the benefits and costs of engaging in surrogacy. She was worried over possible health consequences and labour pains, but her sister assured her of a caesarian section delivery. Thought of separation from her children and husband for nine months during surrogacy rattled Kalika, who had never lived alone. She was also concerned about the well-being of her children in her absence. Kalika then doubted her ability to manage the surrogacy endeavour and refused to participate in surrogacy.
At this juncture, Kalika’s husband, aware of the enormous monetary gains in surrogacy, insisted that Kalika must adhere to her initial decision to participate in surrogacy. He coaxed her into surrogacy, promising that he would take the utmost care of the children and would visit her regularly at the surrogacy clinic. Kalika then made up her mind and attained a surrogate pregnancy in her second attempt of the embryo transfer. It took her considerable time to adjust to the new setting, and at times she even regretted her decision to participate in surrogacy.
Overall, Kalika’s narrative vividly portrays the interpersonal conflicts women must navigate in a hierarchical familial set-up as well as the intrapersonal conflicts they must resolve as agents embedded in the familial context in pursuit of individual goals. The individual goals often were informed by and revolved around the needs of the family. The decision to participate in surrogacy was a complex exercise, the intricacies of which were rarely overt.
Discussion
Building on the existing multidisciplinary work that acknowledges the multiplicity of psychological worlds (Shweder et al. 2006) and critiques of generalized victimization discourse about Indian women (Chaudhary 2012; Ganesh 1999; Mohanty 1988; Raval 2009) this study offers new insights into exercise of agency by Indian women in the context of surrogacy in India. The profile of the women entering surrogacy indicated that sixty-four percent of women had moved out of a joint family to form their own nuclear household. A few even reported marrying by their own choice against the will of their family members, departing from the traditional norm of “arranged marriage.” It was not surprising then to find that the majority of women in this study based in Gujarat—an Indian state with a high international out-migration and diaspora—took the initiative to participate in surrogacy, playing a lead role in the decision-making process. As suggested by Ahearn (2001), for women in this study expression of agency was far from the “exercise of free will” or “resistance.” Most of the women “ascertained facts” to determine the authenticity of surrogacy process without accepting the information they received at face value as evident from the narrative of Rukshar. Despite the reluctance of spouses, women who were determined to participate in surrogacy were able to assert themselves and engaged in “persuasion”—repetitive attempts to convince others for the attainment of their own goals, sometimes over the span of years as in the case of Sargam. At times women also effectively used “selective disclosure,” wherein they revealed their participation in surrogacy to elder family members only after the confirmation of surrogate pregnancy when others could not alter their decision. Char, Saavala, and Kulmala (2010) and Kohli (2016) have reported that Indian women commonly using “secrecy” in the context of reproductive health decisions such as child spacing and abortion when they anticipate the resistance of husband or in-laws. Kalika’s narrative indicates that women carefully choose various forms of agency expression based on their contextual knowledge. For most of them the process was a complex one, full of interpersonal and intrapersonal conflicts and marked by the struggles of striking a balance between traditional gender role ideals and their pursuit of this novel form of work, surrogacy.
The experiences of surrogate mothers are, however, of concern and indicate new avenues of exploitation in the commercial market space and raises serious bioethical concerns. Women were primarily motivated by a strong sense of duty and obligation towards improving life outcomes for their children through the surrogacy income, even at the cost of their life. The concerns about the “safety” of surrogacy processes were limited to sexuality (chastity), and men and women alike trivialized the health risks involved in surrogacy. This poses serious questions about how informed the decisions of women participating in surrogacy are and whether women fully understand and seriously consider the consequences of participation for their health or them. While the Surrogacy (Regulation) Bill 2016 recommends counselling women prior to participation in surrogacy, the contents of such counselling need to be standardized. Even though women were able to assert themselves, sometimes the exercise of agency to pursue their goals was not in the best-interests of the women, as in the case of Rukshar, who convinced her spouse and the medical practitioner to repeat surrogacy within a year of her first surrogate pregnancy. Lack of standardized protocols for surrogacy participation are likely to jeopardize the well-being of surrogate mothers. Lastly, responsibility of any adverse outcomes of surrogacy were shifted to surrogate mothers; the clinic denied any such responsibility through the formal surrogacy contract and spouses reinforced the voluntary participation by women while signing the consent for participation.
Restriction on commercial surrogacy at best can discourage women’s participation in surrogacy out of economic desperation but fails to ensure their well-being under this altruistic guise. The policy instead needs to focus on standardizing surrogacy programmes across India, mandating the inclusion of a rigorous counselling component to promote informed decision-making, and ensuring the physical and mental well-being of the women entering surrogacy.
Conclusion
The study has addressed the paucity of empirical evidence about women’s control over the decision to participate in surrogacy.
Overall, it appeared that the majority of women exercised agency in the context of surrogacy in India. The study indicated that women’s exercise of agency was context sensitive and agency was manifested in the form of ascertaining facts, persuasion, negotiation, selective disclosure, and assertion. The collective voices of women are missing in the policy discourse, and there is a need to create opportunities for the surrogate mothers to participate and shape the Indian surrogacy policy.
References
Ahearn, L.M. 2001. Language and agency. Annual Review of Anthropology 30: 109–137.
Angrosino, M. 2007. Doing ethnographic and observational research. London: Sage Publications Ltd.
Centre for Social Research. 2012. Surrogate motherhood ethical or commercial? New Delhi: Centre for Social Research. http://www.csrindia.org/surrogate-motherhood. Accessed February 23, 2017.
Chang, M. 2009. Womb for rent: India's commercial surrogacy. Harvard International Review 31(1): 11–13. http://hir.harvard.edu/article/?a=1870. Accessed February 23, 2017.
Char, A., M. Saavala, and T. Kulmala. 2010. Influence of mothers-in-law on young couples’ family planning decisions in rural India. Reproductive Health Matters 18(35): 154–162.
Chaudhary, N. 2012. Peripheral lives, central meaning: Women and their place in Indian society. In Cultural dynamics of women's lives, edited by A. Bastos, K. Uriko, and J. Valsiner, 7–30. North Carolina, USA: Information Age Publishing, Inc.
Deomampo, D. 2013. Transnational surrogacy in India: Interrogating power and women’s agency. Frontiers: A Journal of Women’s Studies 34(3): 167–257.
Deonandan, R., S. Green, and A.V. Beinum. 2012. Ethical concerns for maternal surrogacy and reproductive tourism. Journal of Medical Ethics 38(12): 742–745.
Duranti, A. 2004. Agency in language. A companion to linguistic anthropology. Malden, Mass: Blackwell.
Fixmer-Oraiz, N. 2013. Speaking of solidarity: Transnational gestational surrogacy and the rhetorics of reproductive (in)justice. Frontiers: A Journal of Women’s Studies 34(3): 126–257.
Forde, K. 2016. “Good work for good mothers”: Commercial surrogate motherhood, femininity and morality. Asia in Focus (special issue): 5–13. http://www.asiainfocus.dk/wp-content/uploads/2016/11/%E2%80%9CGOOD-WORK-FOR-GOOD-MOTHERS%E2%80%9D-Commercial-Surrogate-Motherhood-Femininity-and-Morality.pdf. Accessed February 23, 2017.
Ganesh, K. 1999. Patrilineal structure and agency of women: Issues in gendered socialization. In Culture, socialization and human development, edited by T.S. Sarawathi, 235–254. New Delhi: Sage Publications India.
Gobo, G. 2008. Doing ethnography. London: Sage Publications.
Gupta, A.J., and A. Richters. 2008. Embodied subjects and fragmented objects: Women’s bodies, assisted reproduction technologies and the right to self-determination. Journal of Bioethical Inquiry 5(4): 239–249.
Gupta, A.J. 2000. New reproductive technologies, women's health and autonomy: Freedom or dependency? New Delhi: Sage Publications India.
Jaiswal, S. 2012. Commercial surrogacy in India: An ethical assessment of existing legal scenario from the perspective of women’s autonomy and reproductive rights. Gender, Technology and Development 16(1): 1–28.
Kohli, A. 2016. Examining middle-class women’s reproductive agency in collective and patriarchal settings of urban northern India. Women’s Studies Journal 30(2): 23–37.
Menon, U. 2011. The three selves of adulthood: Cultural conceptions of self among Oriya Hindu women. Psychological Studies 56(1): 23–35.
Ministry of Health and Family Welfare, Government of India. 2015, November 04. MHFW Circular No.V.25011/119/2015-HR: Commissioning of Surrogacy-Instructions regarding. New Delhi, India. http://www.icmr.nic.in/icmrnews/art/DHR%20notification%20on%20Surrogacy.pdf. Accessed February 16, 2017.
Mohanty, C.T. 1988. Under western eyes: Feminist scholarship and colonial discourses. Feminist Review 30: 61–88.
Mulay, S., and E. Gibson. 2006. Marketing of assisted human reproduction and the Indian state. Development 49(4): 84–93.
Pande, A. 2009. “It may be her eggs, but it’s my blood”: Surrogates and everyday forms of kinship in India. Qualitative Sociology 32(4): 379–397.
Pande, A. 2010. “At least I am not sleeping with anyone”: Resisting the stigma of commercial surrogacy in India. Feminist Studies 36(2): 292–312.
Qadeer, I. 2010. The ART of marketing babies. Indian Journal of Medical Ethics 7(4): 209–215.
Qadeer, I., and M. John. 2009. The business and ethics of surrogacy. Economic and Political Weekly 44(2): 10–12.
Raval, V. 2009. Negotiating conflict between personal desires and others’ expectations in lives of Gujarati women. Ethos 37(4): 489–511.
Roland, A. 1988. In search of self in India and Japan: Toward a cross-cultural psychology. New Jersey: Princeton.
Saravanan, S. 2010. Transnational surrogacy and objectification of gestational mothers. Economic and Political Weekly XLV (16): 26–29.
Sarojini N.B. 2010. Women as wombs. Info Change Agenda 20: 17–22.
Sengupta, A. 2010. The great stem cell debate. Info Change Agenda 20: 34–36.
Shweder, R.A., J.J. Goodnow, G. Hatano, R.A. LeVine, H.R. Markus, and P.J. Miller. 2006. The cultural psychology of development: One mind, many mentalities. In Handbook of child psychology: Theoretical models of human development Vol 1, 6th ed., edited by R.M. Lerner and W. Damon, 716–792. New Jersey: John Wiley & Sons, Inc.
Unnithan M. 2010. Infertility and assisted reproductive technologies in a globalizing India: Ethics, medicalisation and agency. Asian Bioethics Review 2(1): 3–18.
Vora K. 2009. Indian transnational surrogacy and the commodification of vital energy. Subjectivity 28(1): 266–278.
Vora K. 2010. Medicines, markets and the pregnant body: Commercial surrogacy and reproductive labour in a transnational frame. The Scholar and Feminist Online 9: 1–2. http://sfonline.barnard.edu/reprotech/print_vora.htm Retrieved February 23, 2017.
Acknowledgement
This research was supported by The Research Fellowship in Sciences for Meritorious Students, Basic Scientific Research scheme of the University Grants Commission, India.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Naik Africawala, A., Kapadia, S. Women’s Control Over Decision to Participate in Surrogacy. Bioethical Inquiry 16, 501–514 (2019). https://doi.org/10.1007/s11673-019-09931-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11673-019-09931-3