
Abstract
Summary
This study determined the incidence of hip fractures in Gwangju city and Jeonnam province of Korea in 2011 and compared it with the rates in the same area in 1991 and 2001.
Introduction
This study determined the incidence of hip fracture in Gwangju city and Jeonnam province in Korea in 2011 and compared it with the rates in the same area in 1991 and 2001, with the aim of identifying any changes in 2011.
Methods
Korea Health Insurance Review Agency patient data from Gwangju city and Jeonnam province for the period 2011 January 1 to December 31 was analyzed. All claims and records of patients ≥50 years of age with a diagnosis of fracture of the neck of the femur, pertrochanteric fracture, and hip fracture-related surgeries including open reduction and internal fixation, closed reduction and osteosynthesis, total hip replacement, or bipolar hemiarthroplasty were analyzed. Population figures were obtained from the Korea National Statistical Office. Age- and sex-specific annual incidences were calculated. The 2011 data was compared with published data from 1991 to 2001.
Results
There were 1590 hip fractures in 2011, representing a crude incidence of 14.0/10,000. The incidence was 9.7/10,000 in males and 17.5/10,000 in females. The number of hip fractures and fracture incidence was 247 and 3.3/10,000 in 1991 and 1152 and 13.3/10,000 in 2001, respectively. There was a fourfold increase of fracture incidence between 1991 and 2001. Thereafter, the number of fractures increased only by 5.2 %. However, the number of arthroplasties done increased significantly.
Conclusions
The incidence of fractures increased considerably between 1991 and 2001, with less increase in the ensuing 10 years.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Osteoporosis is a significant public health problem as the proportion of the elderly in society increases [1]. Hip fracture is the most valid epidemiologic marker of osteoporosis and is associated with a high degree of both morbidity and mortality. As global population continues to age, the number of patients with hip fractures is expected to increase. According to a World Health Organization report, the worldwide number of hip fractures resulting from osteoporosis is expected to increase threefold by the middle of this century, from 1.7 million in 1990 to 6.3 million by 2050 [1], as hip fracture incidence rates increase exponentially with aging [2]. Asia is predicted to bear an increasing burden of this rise, but the incidence rates of hip fractures for Asian people are reportedly lower than those for Whites living in northern Europe and North America [3–7]. In 1990, 26 % of all hip fractures occurred in Asia, and this is predicted to rise to 37 % by 2025 [8]. By the year 2050, more than 50 % of all hip fractures are projected to occur in Asia [9]. However, this dramatic increase in hip fracture rate cannot be accounted solely by increase in the aged population, as several reports from Asian and Western countries suggest that age-specific incidence is also rising [10–12].
As the aged population increases in Korea, the numbers of patients with osteoporosis and osteoporotic fractures are also estimated to increase. In 2000, the proportion of elderly (>65 years old) in Korean population was 7.4 %, and it is expected to reach 15.1 % by 2020 [13]. Moreover, bone mineral density has a strong negative correlation with age in the Korean middle-age population [14].
In Korea, Rowe et al. reported the first epidemiological study on incidence of hip fractures at our institute. They included the hip fracture data of Gwangju city and Jeonnam province in 1991 [15]. In 2001, Rowe et al. [16] again reported the hip fracture incidence of the same area. During the decade from 1991 to 2001, the hip fracture incidence increased four times in this region of Korea [16].
The purpose of this study was to determine the incidence of hip fracture in Gwangju city and Jeonnam province in 2011 and the changes in their incidence since 2001. Also, we tried to analyze the difference in distribution of hip fracture incidence in rural and urban areas and the changes in methods of surgical treatment during 20 years.
Materials and methods
Patients ≥50 years of age living in Gwangju city and Jeonnam province, Korea, who sustained a fracture of the hip during year 2011, were investigated. Data from the Health Insurance Review Agency (HIRA) of Korea for the period 2011 was analyzed. In Korea, 97.0 % of the population is obligated to enroll in the National Health Insurance Program. Every clinic or hospital in Korea submits patient data regarding the diagnosis and treatment to HIRA. The remaining 3 % of the population is under Medical Aid Program. Thus, nearly information of entire population about the volume and burden of disease can be obtained from this centralized database, with the exception of procedures that are not covered by insurance, such as cosmetic surgery. Many epidemiological analyses have been published from this database [17–19]. The cumulative and anonymized data were delivered by the Ministry of Health, the official institute holding the HIRA of Korea. Thus, data protection was fully guaranteed. Given the anonymous and mandatory nature of the data, the requirement for informed consent was not necessary.
The age and sex distribution of entire Korean population for the study period was obtained from the census data of Korea National Statistics Bureau [13].
Only fractures of the femoral neck and intertrochanteric fractures were included. Subtrochanteric fractures were excluded, as they are usually caused by high-energy trauma. All records of claims of outpatient visits or hospital admissions of patients ≥50 years of age with a diagnosis of femur fracture (International Classification of Diseases (ICD)-10 diagnostic code: S72), fracture of the neck of the femur (S72.0, S72.00), pertrochanteric fracture (S72.1, S72.10) and hip fracture-related operation (open reduction and internal fixation; ICD-10 procedure code: N0601), closed reduction and osteosynthesis (N0991), total hip replacement (N0711), or hemiarthroplasty (N0715) from January 1 to December 31, 2011, were analyzed from the HIRA claims database. Age- and sex-specific annual incidences were calculated using the population of the aforementioned locales. The data of 2011 was compared with the data of previous studies [15, 16].
Statistical analyses
To assess the change in annual rates of hip fractures in each age group, generalized linear models were used. Specifically, Poisson regression models are generalized linear models with the logarithm as the (canonical) link function and the Poisson distribution function as the probability distribution. Poisson regression assumes that the response variable has a Poisson distribution and assumes that the logarithm of its expected value can be modeled by a linear combination of unknown parameters. Poisson regression is also appropriate for rate data. Hip fracture rates were calculated as the number of hip fractures in a region, representing the number of fractures divided by person-years. More generally, event rates can be calculated as events per unit time, which allows the observation window to vary for each unit. In these examples, exposure is respectively unit area, person-years, and unit time.
To explore the possible impact of distribution of population in rural and urban areas on hip fracture, Spearman’s correlation coefficient was calculated. The analyzed variables were the proportion of rural population and change in hip fracture rates by age group.
Data were analyzed using the SPSS 19.0 (SPSS, Chicago, IL, USA). Between-group comparisons were conducted using the Pearson chi-square test. For all analyses, a p value <0.05 was considered statistically significant.
Results
The total population of Gwangju city and Jeonnam province with ≥50 years of age in 2011 was 1,135,037, of whom 622,628 were female and 512,769 were male, giving a sex ratio of 1.21:1. These individuals accounted for 33.6 % of the total population of this area. The numbers of people with ≥50 years of age were 20.6 % in 1991 and 24.7 % in 2001 (Table 1, Fig. 1).

a The total population change of Gwangju and Jeonnam province in 1991, 2001, and 2011. b The population change in people ≥50 years of age
The total number of hip fractures was 1590 in 2011 (Table 1), and the incidence of hip fracture was 14.0/10,000 population ≥50 years of age. The total number of hip fractures and incidence was 247 and 3.3, respectively, in 1991 and 1152 and 13.3, respectively, in 2001. From 1991 to 2001, the hip fracture incidence increased by 306 %. The increase from 2001 to 2011 was 5.2 % (Table 1). The difference of incidence rate of hip fractures among male and female was increased to 7.8 in 2011 (male 9.7, female 17.5) compared to 3.9 in 2001 (male 11.2, female 15.1) and −0.6 in 1991(male 3.7, female 3.1) (Table 1).
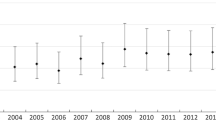
The age-specific incidence showed a decrease in hip fracture incidence in people aged 50s, 60s, and 70s but an increase in people with ≥80 years of age, from 62.8 in 2001 to 78 in 2011. The increase in hip fracture incidence was more pronounced in males than females. In males ≥80 years of age, the hip fracture incidence was 92 in 2011, 60.3 in 2001, and 21.7 in 1991 (p < 0.001). In females ≥80 years of age, the incidence was 73 in 2011, 63.7 in 2001, and 13.0 in 1991 (p < 0.001) (Fig. 2).

a Number of hip fracture changes according to age. b Incidence changes of males. c Incidence changes of females
There were significant differences between the incidences of hip fracture in urban and rural areas. In urban area (Gwangju, Mokpo, Yeosu, and Suncheon cities), the incidence was 15.7/10,000. The rural incidence was 12.8/10,000. During the 20 years from 1991 to 2011, the incidence of hip fractures displayed a similar urban/rural pattern (Table 2). The risk of hip fracture was increased 1.26 times in urban dwellers compared to rural dwellers during the 20-year period.
There was no significant seasonal difference in hip fracture incidence in 2011 and 1991, although there were significantly more hip fractures in 2001, especially in the winter season (p < 0.001). During the 20 years from 1991 to 2011, the risk of hip fracture was highest in winter. Comparing winter with autumn, the risk was 1.32 times higher in winter than autumn (p < 0.001).
There were significant changes in the treatment method during this 20-year span. In 2011, there were more arthroplasties in the treatment of femoral neck fracture or intertrochanteric fracture compared with 1991 and 2001 (femoral neck fracture, p = 0.050; femoral intertrochanteric fracture, p < 0.001; Fig. 3).

a Changes of treatment in femoral neck fracture. b Changes of treatment in femoral intertrochanteric fracture
Discussion
The incidence of hip fracture did not increase during the last 10 years in Gwangju city and Jeonnam province. The fracture incidence in people aged in their 50s, 60s, and 70s decreased but increased in people ≥80 years of age. Especially, in male ≥80 years of age, there was an increasing tendency of hip fracture. These changes of hip fracture incidence in Korea, as well as some other countries, could reflect economic and population changes. Korea has a rapid growing economy and is becoming an increasingly aged society. In 1991, the hip fracture pattern did not show patterns similar to more developed countries like Japan. But, in 2001, the pattern became similar to these countries. A study performed in Tottori province in Japan reported an increasing trend of hip fracture incidence from 1986 to 2006 [3, 20]. The authors included hip fracture data from patients aged 35 to 50 years. The authors also commented that the age- and gender-specific incidence of hip fracture in Tottori prefecture had not plateaued. However, in the present study, the age-specific hip fracture incidence in 2011 showed a trend of decrease in people aged in their 50s, 60s, and 70s, while increasing in people ≥80 years of age. In Korea, several epidemiological studies of hip fracture incidence have been done in Jeju Island. One study [21] reported a 101 % increase in the number of hip fractures from 151 in 2002 to 304 in 2011. The crude incidence of hip fractures in those ≥50 years of age increased from 126.6/100,000 to 183.7/100,000. A study of the 5-year change of hip fracture incidence in Korea from 2001 to 2004 [17] reported a 4.7 % increase in women ≥50 years of age from 250.9/100,000 persons in 2001 to 262.8/100,000 in 2004. However, the rate in similarly aged men decreased 15.5 % from 162.8/100 000 in 2001 to 137.5/100,000 in 2004. The present results are qualitatively similar, but the actual fracture incidence was lower. This may be because proportionally more people ≥50 years of age live in Gwangju city and the Jeonnam area than in entire country, with the proportion of people ≥80 years of age also being higher in these two locales. Another study of Korean hip fracture incidence showed that the lower rate of increase with time could be correlated with increasing prescription of bisphosphonate in Korea [18]. We agree with this view. The current data suggest that the changed increase involves people aged in their 50s, 60s, and 70s. Concerning the variation of urban and rural areas, people in rural area are more apt to do heavy labor work like farming and are more likely to be exposed to sunlight than urban dwellers. Both factors could increase bone strength.
Although no significant seasonal influence in the rate of hip fracture was apparent during the 20 years from 1991 to 2011, winter was the most dangerous season for hip fracture and autumn was the safest season.
For the treatment of hip fracture, in the femoral neck fracture, the proportion of arthroplasty showed a small increase (p = 0.050). Recently, Lee et al. [19] reported the increasing arthroplasty as a treatment of hip fracture in Korea. The authors suggested that increasing awareness of proper treatment among surgeons might be the underlying cause of increase in tendency of hip fracture. However, there was a steep increasing trend of hip arthroplasty for the patients with femur intertrochanteric fracture (p < 0.001). Until recently, the gold standard for the treatment of intertrochanteric fracture is internal fixation with compression hip screw or proximal intramedullar nail devices [22]. Arthroplasty may be chosen in cases with severe comminuted intertrochanteric fracture. In our study, as the hip fracture was more prevalent in more aged population, such as people ≥80 years of age, the number of comminuted intertrochanteric fractures could be increased. Surgeons may tend to choose arthroplasty for more comminuted intertrochanteric fractures.
Conclusion
The increasing tendency of hip fracture was reduced in 2011 compared to 2001, except in people ≥80 years of age. Hip fracture prevention remains a heightened concern in very old people.
References
Clark P, Lavielle P, Franco-Marina F, Ramírez E, Salmerón J, Kanis JA, Cummings SR (2005) Incidence rates and life-time risk of hip fractures in Mexicans over 50 years of age: a population-based study. Osteoporos Int 16:2025–2030
Cummings SR, Melton LJ (2002) Epidemiology and outcomes of osteoporotic fractures. Lancet 359:1761–1767
Hagino H, Katagiri H, Okano T, Yamamoto K, Teshima R (2005) Increasing incidence of hip fracture in Tottori Prefecture, Japan: trend from 1986 to 2001. Osteoporos Int 16(12):1963–1968
Maghraoui AE, Koumba BA, Jroundi I, Achemlal L, Bezza A, Tazi MA (2005) Epidemiology of hip fractures in 2002 in Rabat, Morocco. Osteoporos Int 16:597–602
Lau EM, Lee JK, Suriwongpaisal P, Saw SM, De Das S, Khir A, Sambrook P (2001) The incidence of hip fracture in four Asian countries: the Asian Osteoporosis Study (AOS). Osteoporos Int 12:239–243
Ross PD, Huang C (2000) Hip fracture incidence among Caucasians in Hawaii is similar to Japanese. A population-based study. Aging (Milano) 12:356–359
Yan L, Zhou B, Prentice A, Wang X, Golden MHN (1999) Epidemiological study of hip fracture in Shenyang, People's Republic of China. Bone 24:151–155
Gullberg B, Johnell O, Kanis JA (1997) World-wide projections for hip fracture. Osteoporos Int 7:407–413
Cooper C, Campion G, Melton LJ III (1992) Hip fractures in the elderly: a world-wide projection. Osteoporos Int 2:285–289
Kannus P, Niemi S, Parkkari J, Palvanen M, Vuori I, Jarvinen M (1999) Hip fractures in Finland between 1970 and 1997 and predictions for the future. Lancet 353:802–805
Lau EM, Cooper C, Wickham C, Donnan S, Barker DJ (1990) Hip fracture in Hong Kong and Britain. Int J Epidemiol 19:1119–1121
Finsen V, Benum P (1987) Changing incidence of hip fractures in rural and urban areas of central Norway. Clin Orthop Relat Res 218:104–110
Korea National Statistical Office (2003) STAT-Korea, Census. http://www.nso.go.kr/cgi-bin/sws_999.cgi
Lim S, Joung H, Shin CS, Lee HK, Kim KS, Shin EK, Kim HY, Lim MK, Cho SI (2004) Body composition changes with age have gender-specific impacts on bone mineral density. Bone (NY) 35:792–798
Rowe SM, Yoon TR, Ryang DH (1993) An epidemiological study of hip fracture in Honam, Korea. Int Orthop 17:139–143
Rowe SM, Song EK, Kim JS, Lee JY, Park YB, Bae BH, Hur CI (2005) Rising incidence of hip fracture in Gwangju City and Chonnam Province, Korea. J Korean Med Sci 20:655–658
Lim S, Koo BK, Lee EJ, Park JH, Kim MH, Shin KH, Ha YC, Cho NH, Shin CS (2008) Incidence of hip fractures in Korea. J Bone Miner Metab 26(4):400–405
Lee YK, Ha YC, Park C, Yoo JJ, Shin CS, Koo KH (2013) Bisphosphonate use and increased incidence of subtrochanteric fracture in South Korea: results from the National Claim Registry. Osteoporos Int 24(2):707–711
Lee YK, Ha YC, Park C, Koo KH (2013) Trends of surgical treatment in femoral neck fracture: a nationwide study based on claim registry. J Arthroplasty 28(10):1839–1841
Hagino H, Furukawa K, Fujiwara S, Okano T, Katagiri H, Yamamoto K, Teshima R (2009) Recent trends in the incidence and lifetime risk of hip fracture in Tottori, Japan. Osteoporos Int 20(4):543–548
Kim SR, Ha YC, Kim JR, Kim R, Kim SY, Koo KH (2010) Incidence of hip fractures in Jeju Island, South Korea: a prospective study (2002–2006). Clin Orthop Surg 2(2):64–68
Court-Brown CM, Heckman JD, McQueen MM, Ricci WM, Tometta P (2015) Rockwood and green’s fractures in adults, 8th edn. Wolters Kluwer, New York, pp 2075–2130
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None.
Rights and permissions
About this article

Cite this article
Park, KS., Woo, SH., Park, WJ. et al. Change in incidence of hip fracture in Gwangju City and Jeonnam Province, Korea, over 20 years. Arch Osteoporos 10, 38 (2015). https://doi.org/10.1007/s11657-015-0242-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11657-015-0242-3