
Abstract
Background
The 2014 Veterans Choice Act and subsequent 2018 Veteran’s Affairs (VA) Maintaining Systems and Strengthening Integrated Outside Networks Act (MISSION Act) are legislation which clarified Veteran access to healthcare provided by non-VA clinicians (community care). These policies are of particular importance to Veterans living in rural areas, who tend to live farther from VA medical facilities than urban Veterans.
Objective
To understand Veterans’ experiences of the MISSION Act and how it impacted their access to primary care to inform future interventions with a focus on reaching rural Veterans.
Design
Qualitative descriptive design.
Participants
United States (US) Veterans in Northwestern states engaged in VA and/or community care.
Approach
Semi-structured interviews were conducted with a purposive sample of Veterans between August 2020 and September 2021. Interview domains focused on barriers and facilitators of healthcare access. Transcripts were analyzed using thematic analysis.
Key Results
We interviewed 28 Veterans; 52% utilized community care as their primary source of care and 36% were from rural or frontier areas. Three main themes emerged: (1) Veterans described their healthcare experiences as positive but also frustrating (billing and prior authorization were noted as top frustrations); (2) Veterans with medical complexities, living far from healthcare services, and/or seeking women’s healthcare services experienced additional frustration due to increased touch points with VA systems and processes; and (3) financial resources and/or knowledge of the VA system insulated Veterans from frustration with healthcare navigation.
Conclusions
Despite provisions in the MISSION Act, Veteran participants described persistent barriers to healthcare access. Patient characteristics that required increased interaction with VA processes exacerbated these barriers, while financial resources and VA system knowledge mitigated them. Interventions to improve care coordination or address access barriers across VA and community care settings could improve access and reduce health inequities for Veterans—especially those with medical complexities, those living far from healthcare services, or those seeking women’s healthcare.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
INTRODUCTION
Inequities in accessing healthcare between urban and rural Veterans are well documented.1,2,3 In order to improve access, the Veteran’s Health Administration (VA) implemented the Veterans Access, Choice And Accountability Act Of 2014, which expanded Veterans’ access to non-VA clinicians (known as community care) when a specific service was not available in a VA medical facility or Veterans faced wait time/travel delays.4 In 2018, the VA Maintaining Systems and Strengthening Integrated Outside Networks Act (MISSION Act) replaced this 2014 act.5 The MISSION Act increased access to covered services not provided by the VA and expanded Veterans’ ability to use community care. In an effort to address geographic barriers to healthcare access, this expansion was open to Veterans living more than a 30-min drive from VA primary care, mental health, and non-institutional extended care services; those with a 60-min average drive time for VA specialty care; and those having to wait either more than 20 days for an primary care appointment at a VA medical facility, mental health, and non-institutional extended care services or 28 days for specialty care.5, 6 The MISSION Act is of particular importance to the five million Veterans living in rural areas, nearly one-quarter of all US Veterans.7 These Veterans often live farther from VA medical facilities than their urban counterparts, which contributes to disproportionate barriers to accessing care.8, 9
Despite additional community care options available to rural Veterans through the MISSION Act, access barriers persist. Veterans’ gender, employment and socioeconomic status, and disability status often contribute to further health inequities, which exacerbate these existing barriers.10, 11 A 2021 survey of VA Medical Center directors found that accessing community care was problematic for Veterans seeking orthopedic, dermatologic, neurologic, mental health, and pain management care.12 Though Veterans can use community care if VA wait times exceed the length established in the MISSION Act, community wait times are not always shorter. In fact, despite provisioning an expanded network of community clinicians for Veterans experiencing long wait times,13 wait times for community primary care appointments have increased at all VA facilities post-MISSION Act.14 Furthermore, rural Veterans may not have a community provider available in their area. One VA medical facility in the Northeast reported increased issues coordinating and communicating with healthcare providers following the MISSION Act, leaving Veterans primarily responsible for connecting their own care.15
Additional impacts of the MISSION Act on care access, and interventions to mitigate them, are largely unknown.16 Therefore, we conducted a qualitative study with Veterans across the Pacific Northwest to understand healthcare accessibility as well as barriers and facilitators to receipt of healthcare post-MISSION Act. Our approach was designed to understand Veterans’ experiences of the MISSION Act and how it impacted their access to primary care in order to inform future interventions, focusing on reaching rural Veterans.
METHODS
This qualitative descriptive study was conducted by a multidisciplinary team with expertise in rural health, primary care, implementation science, qualitative methods, and Veteran/patient engagement. Study activities were conducted by Oregon Rural Practice-based Research Network (ORPRN) in partnership with the VA Veterans Rural Health Resource Center in Portland, Oregon (VRHRC-P). Data collection occurred during two time periods, May to September 2020 and August to September 2021, though each participant was only interviewed once. The separate interview periods resulted from funding mechanism structures and an effort to expand participation to other Northwestern states. The study was approved by the Veterans Affairs Portland Health Care System (VAPORHCS) and Oregon Health & Science University (OHSU) joint Institutional Review Board (eIRB#20,843).
Setting
Participants were recruited from VA Veteran Integrated Service Network (VISN) 20, which includes Washington, Oregon, Idaho, Alaska, Montana (one county), and California (one county). VISN 20 covers 135 counties and approximately 23% of the US land mass; it covers 17% of the total US populated area, the largest percentage of all VISNs.17 VISN 20 has six VA medical centers, two tertiary sites, 20 community-based outpatient clinics, and one mobile clinic. VISN 20 currently serves 194,949 Veterans and 79% of counties report health professional shortages within their areas.17 VISN 20 is largely rural, with four out of the five market regions having a greater proportion of Veterans living in rural areas (42.7–54.3%) than the national average (32.5%).18
Participants
Participants were purposively sampled through direct outreach to Veteran-serving community organizations, including Veterans of Foreign Wars, American Legion, and Veteran Service Officers (VSOs). We leveraged ORPRN’s extensive network of clinic partners to facilitate connections to Veterans living in rural areas, seeking care at rural facilities, and Veteran groups serving rural regions. Participants were eligible if they (1) identified as a Veteran, (2) were located in VISN 20, and (3) used community care either for primary or specialty care. We sought variation across multiple characteristics: age, sex, state, rurality, dominant source of care (VA primary or community care primary, or both) and geographic region. As the MISSION Act primarily impacted those in rural areas, participants from non-urban areas were prioritized using Rural Urban Commuting Area (RUCA) codes designated as frontier (10), rural (7–9), or micropolitan (4–6) as compared to urban (1–3) by zip code.19
Data Collection
The study team developed a 12-question, semi-structured interview guide that explored factors impacting Veterans’ access to and experience with healthcare. Interview domains focused on barriers and facilitators and general impressions of accessibility, and explored variation by geographic site/care setting.20 Prior to data collection, the guide was reviewed by the research team and the study Advisory Board, which consisted of Veterans living in rural areas, VSOs, VA clinicians, and non-VA clinicians serving Veteran populations. As data collection progressed, the interview guide was iteratively refined based on coding of preliminary interviews.
Telephone or Zoom videoconference interviews were conducted by team members with qualitative interview training and experience (MP, NR, CB). Interviews lasted 44 min on average (range 30–60), were digitally recorded with the participant’s verbal consent prior to the interview, and professionally transcribed. Members of the study team validated and de-identified interview transcriptions, renaming them using a participant identification number. Data was monitored for saturation (e.g., participants presented no new information), at which point recruitment stopped.21
De-identified transcripts were uploaded to ATLAS.ti for data management and analysis. During the 2020 interviews, analysis and data collection occurred concurrently using Braun and Clarke’s approach to thematic analysis.22 An initial code book was developed using a combination of deductive and inductive codes. The code book was tested on a subset of transcripts, coded by a second analyst to ensure reliability and iteratively, and refined through analytic team meetings that included qualitative analysts (EK, NR, MP), the principal investigator (MD), and a medically trained Veteran. In 2020 and 2021, all interview transcripts were then coded by independent qualitative analysts using the finalized code book (EK, NR, CB). The qualitative analysis team identified emergent themes through reviewing, coding, and engaging in a dialogue-based refinement process.22 The full study team and Advisory Board reviewed and member-checked all themes.23
RESULTS
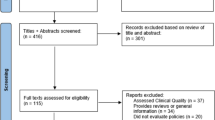
We interviewed 28 Veterans living in Oregon, Washington, Idaho, and California. As summarized in Table 1, participants were distributed across frontier (21%), rural (14%), micropolitan (43%), and urban (21%) RUCA code regions. About half of participants (52%) used community care primarily, with the remainder (48%) primarily using VA care and community care for specialty care. Most (89%) lived more than 30 min from a VA primary care location. Nearly a third (32%) of our sample identified as female.
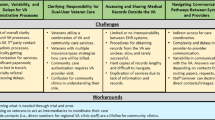
Three main themes emerged: (1) Veterans described their healthcare experiences as positive, but expressed frustrations with navigating VA systems and processes; (2) Veterans with medical complexities, those living far from healthcare services, and/or those seeking women’s healthcare services experienced additional frustration due to increased touch points with VA systems and processes; and (3) financial resources or knowledge of the VA system insulated Veterans from frustration with system navigation. We describe each theme in depth with illustrative quotes below.
Veterans Described Their Healthcare Experiences as Positive, but Expressed Frustrations with Navigating VA Systems and Processes
Overall, when asked about their care experiences, Veterans (1) spoke about their clinical encounters in both VA and community care settings, and (2) talked about navigating the administrative aspects of obtaining VA-covered care. The clinical encounter anecdotes were primarily positive; participants were generally satisfied with care they received. Veterans described providers as “remarkable” (Veteran 11) and the VA system as full of “wonderful people” (Veteran 11) and as a “modern” and “highly rated institution” (Veteran 21).
However, the tone shifted when describing navigating the administrative aspects of obtaining care covered by VA benefits. As an integrated healthcare system, the VA functions as both healthcare provider and insurer, with specific processes required to authorize access to community care. Participants often described these experiences as frustrating, leaving them with a “chip on their shoulder” due to difficulty getting accurate information to access necessary care (Veteran 10). One participant described this frustration:
It’s . . . the bureaucracy, finding your way through the labyrinth, trying to get something done is really hard. But if you can talk to somebody who actually is going to do something for you one way or another, that’s really pretty good. Getting there sometimes is kind of hard. (Veteran 9)
Two processes that consistently caused the most frustration were billing/reimbursement and care authorization. Many Veterans shared stories of billing challenges even after seeking prior authorizations and approvals. Veteran participants described “spend[ing] at least five hours on the phone” trying to determine if their care was covered and being told “at least two different things” (Veteran 10) regarding coverage. Other Veterans described situations where they were required to pay for services provided by the VA they previously understood would be covered. For example, one participant described various challenges with billing and payment/reimbursement for care:
If it’s a prescription or something, then I usually have to do a copay. And then, we do this dance where they keep sending me these bills, and I say, ‘I’m not supposed to pay this.’ And then they threaten to garnish my wages, so I go down there and pay it. And I pay the cashier. And then a month or two later they send me a check for the amount I went down and paid. (Veteran 6)
Participants described the care authorization process as similarly challenging due to long wait times for information and that it was “difficult to know what was going on.” One participant reported that getting enrolled in care, a process that took over six months, was “the single most difficult thing I’ve ever done in my life.” (Veteran 10). Similar to billing, participants explained that every person they talked to would tell them different information, making it impossible to confirm authorization.
Some Veterans described spending multiple hours on the phone in advance of every appointment. Not only did these challenges result in extra effort, but many participants described the additional burden that navigating reimbursement and authorizations placed on non-VA clinic staff, VSOs, and friends and family members helping them navigate the system. For example, one participant stated:
I couldn’t do it if I was employed because I spend at least four hours on the phone. My nurse practitioner, her receptionist, I know her by name. . . . I’ve sent her flowers because she has spent four hours a day just leaving the phone on speaker with the VA while they transfer her from place to place to place to place. Nobody is on the same page. (Veteran 25)
Veterans with Medical Complexities, Those Living Far from Healthcare Services, and Those Seeking Women’s Healthcare Services Experienced Additional Frustration due to Their Need for Increased Touch Points with VA Systems and Processes
We highlight challenges described by each of these populations below.
Increased Medical Complexity Amplifies Fragmented Care and Number of Interactions
Veterans with multiple medical conditions described engaging with more clinicians than those without, compounding the number of times they engaged with VA policies and processes. These Veterans often needed to utilize both the VA and the community care system to fully address their medical needs, a process they described as fragmented. Providers in these systems have limited avenues open to communicate with each other, leaving the burden of communication on the Veteran.
Living Far from Healthcare Contributed to Additional Travel Costs and Cumbersome Reimbursement Processes
Several participants living in rural or frontier areas described additional challenges in navigating VA policies and processes. One participant described the inconvenience of switching addresses in the VA system:
When we moved to [frontier town] . . . I attempted to get us switched over to being able to see a provider in [nearby town] instead, and the paperwork process is just out of this world. . . . And the turnaround times, in the mail or for phone calls, I felt were really unreasonable. Like if we don’t hear from you in two days you have to restart this process. . . . So that was a huge barrier for us. (Veteran 27)
Participants living far from care options also described travel costs such as gas, lodging, and taking time off work. While the VA reimburses appointment travel costs, the process was described as onerous and, following policy change, now occurs after the appointment. One participant described it as cumbersome, particularly if you were not computer savvy:
Well, they paid everything—travel pay is so hard to do online, and I put in the travel pay, and it wasn’t on the proper letterhead. So I probably lost at least $300 or $400, just because of that. And I’ve been so dang busy, and I haven’t followed up on it. . . . And you have to sign in securely, which is a hassle sometimes if you’re not computer literate. (Veteran 18)
Another participant described the added burden from the reimbursement for travel shifting from pre to post-appointment:
I think for me, when we are living with less income it’s really difficult to get to specialty appointments when the reimbursement doesn’t come until later. . . . I think gas money is huge, huge, huge barrier to people who [don’t] live very near town. (Veteran 27)
Seeking Women’s Healthcare Services Is Challenging due to Lack of Qualified Providers and the Male-Centeredness of VA Care
Participants identifying as female frequently reported that navigating women’s-specific healthcare further complicated factors described in previous sections. One participant reported that she had had “eight or nine providers” (Veteran 4), none of them staying more than six months. Another commented that the VA often sidelined women’s healthcare and that men get taken more seriously:
[Women] are treated differently than our male counterparts. It’s automatically assumed the male is the Veteran. We’re kind of forgotten about. . . . Care is geared more towards males. It seems like they get a lot more care. They get taken more seriously. We just, I don’t know, personally I feel at times that we get pushed off to the side and not get taken seriously. (Veteran 4)
Further compounding these challenges, participants identifying as female self-reported a high incidence of military sexual trauma, and often struggled to use VA health services. Multiple participants strongly associated the VA with their service and military sexual trauma. One participant (Veteran 4) described that finding a VA provider equipped to provide mental health services for military sexual trauma was difficult and that “[it] can be a challenge. Not everyone has worked with clients that have endured [military sexual trauma].”
While the factors in this section are detailed separately, many participants experienced multiple simultaneously. Those experiencing several factors described compounding impacts, partly due to the exponential increase in touch points and care coordination to fully meet their healthcare needs. One Veteran with multiple chronic conditions who lived in a rural area described the process of navigating care as “exhausting,” adding, “I’m not sure the VA always considers the disabilities of their patients when they do the scheduling.” (Veteran 3).
Financial Resources or Knowledge of the VA System Insulated Veterans from Frustration with System Navigation
Participants described variation in the levels of system navigation frustration. For some, increased financial resources and knowledge of the VA system allowed them to optimize their healthcare options, decreasing care barriers and increasing satisfaction. In contrast, those with fewer financial resources or less knowledge of the VA system described more challenges and frustration.
Financial Resources
Veterans who described having more financial resources, such as secondary coverage and more discretionary income, were able to better absorb the costs associated with navigating the multiple layers of policy and process. Those with fewer resources, such as those who were low income or only had VA insurance coverage, were not. Waiting for reimbursement for travel or other services was not a burden for Veterans with more disposable income, as they were more likely to be able to absorb these costs. Similarly, those with more income were more able to pay out-of-pocket costs associated with seeking faster care. Veterans with secondary insurance coverage through an employer or spouse were more likely to get services covered through a broader network of providers. One participant described using employer-sponsored insurance to receive care faster and easier, saying, “I have medical insurance through my employer and so sometimes I just use that....I just go with whatever, I pay my copay, and do it. That’s easy and quick and works.” (Veteran 7).
Knowledge of the VA System
Participants with greater VA knowledge about structure and processes were better positioned to navigate the system and understand the actions or workarounds necessary to get their care. Veterans with professional connections to the VA described an increase in their understanding of how to navigate the VA compared to those without. Participants who described getting information from Veteran family members, friends, VSOs, or peer groups who understood their care options relied on these insiders to navigate care. One Veteran highlighted the importance of having a support partner:
I wouldn’t be as well as I am, and [my spouse] wouldn’t, if we wouldn’t have been able to be there and take notes and advocate and have the health literacy needed to navigate it. I would just caution people. You need to find a partner in your healthcare journey. Whether it’s from [the VA] or your personal life, just don’t try and do that on your own because it’s just too much. You’ll get discouraged and not move forward. (Veteran 12)
DISCUSSION
Following the MISSION Act, Veterans from the Northwest not only had positive experiences with VA healthcare, but also described many frustrating aspects to accessing it, particularly billing and prior authorization. These frustrations were amplified for Veterans navigating multiple care systems such as those with medical complexities, living far from healthcare services, and/or seeking women’s healthcare services. Increased financial resources and/or knowledge of the VA buffered these frustrations. These differences in care experiences reflect broader, well-known healthcare inequities such as socioeconomic status, disability status, and gender, and provide an important opportunity to improve equity and access.10, 11
Mixed positive and negative experiences with access to VA healthcare have been described in work conducted prior to the MISSION Act.24 As an integrated system, the VA excels at care coordination within the VA.15, 25, 26 However, care coordination becomes fragmented for Veterans seeing external healthcare providers (e.g., women’s health, multiple providers, community care).15, 26, 27 Indeed, coordination between the VA and community care was previously highlighted as a potential problem, and community care providers have also noted it as an obstacle.28 Resources do exist to address these coordination and access needs, such as the Women Veterans Call Center for women’s health29, but our participants have indicated there is still room for improvement.
The MISSION Act was designed to improve access for Veterans experiencing barriers to care. Yet, Veterans in our study highlighted frustrations with the administrative aspects of accessing care, especially related to billing and prior authorization.6, 12 Moreover, we found that certain sub-groups (e.g., medically complex, living far from healthcare, identifying as female) experienced additional frustration and inequities. This finding is particularly problematic, as a recent study identified that Veterans who were female, lived in rural areas, lived over 40 driving miles to VA care, or had a psychiatric/depression condition, were more likely to receive community care—the same groups reporting additional frustrations with navigating and receiving healthcare in our study.30
Community care is used more often in rural areas than urban ones; therefore, problems in service provision and existing health inequities may be magnified in rural Veteran populations. Our participants living far from healthcare services (likely due to living in rural areas) experienced frustrations beyond billing and prior authorizations due to navigating several care systems. Our recent work suggests that rural Veterans may not experience the benefits of the MISSION Act because of specific barriers, including poor geographic proximity to covered healthcare, wait times, or full patient panels.31 Additionally, Veterans living in rural areas experience poorer health outcomes and health-related quality of life compared to their urban counterparts.15 These complex care needs may require increased care coordination, further exacerbating access issues.27, 32, 33 Conversely, Veterans living in rural areas who received community care reported comparable or better access, coordination, communication, and overall clinician ratings to Veterans living in urban areas who received community care.34 Additional research comparing rural and urban experiences accessing community care following implementation of the MISSION Act is warranted.
We also found that Veterans with more financial resources and VA system knowledge could leverage these supports to better navigate systems and receive satisfactory healthcare. Participants noted family members, friends, peer groups, and VSOs as the places to find information and resources most readily; however, not all had access to these supports. Our results suggest the need for structural solutions, such as formal healthcare navigation programs or system-level interventions to improve the function and coordination of care delivery and coverage and reduce access inequities to increase and simplify the utilization of community care. To ensure equitable access, interventions and implementation strategies may need to be tailored to reach Veteran sub-groups with the increased access barriers identified in our study.
This study has several notable limitations. First, the MISSION Act was implemented in June of 2019 with the COVID-19 pandemic beginning a few months later.9 These co-occurring events likely both impacted how Veterans received healthcare and responded to our outreach. While Veterans may attribute challenges in healthcare like longer appointment wait times, difficulty getting through to call centers, and extended authorization timelines to either the MISSION Act or COVID-19, specific causes and effects could not be disentangled in our dataset. Further exploration of the specific and combined impacts of these two events is needed. Second, our findings are based on qualitative interviews from a subset of Veterans across VISN 20. While efforts were made to obtain a representative sample across age, sex, state, rurality, dominant source of care (e.g., VA primary, community care primary), and geographic region, our sample was not large enough to represent the circumstances of all Veterans. However, we were able to interview Veterans from four states, with 32% of interviewees identifying as female. Additionally, saturation across themes was reached and findings provide important context for future qualitative and quantitative research. Further research is needed to determine if the findings are generalizable to other regions, which may have more racially and ethnically diverse Veteran populations. Despite these limitations, our study provides valuable insight into the healthcare experiences of Veterans.
CONCLUSION
Despite expansion of community care access through the MISSION Act, barriers persist. These barriers were often exacerbated for Veterans with medical complexities, those living far from healthcare services, and those seeking women’s healthcare services because of the need to navigate multiple systems of healthcare, causing specific inequities for these groups. Increased financial resources and knowledge of the VA system insulated many Veterans from barriers and frustrations, making accessing care easier and, therefore, increasing protection from greater morbidity and mortality. Interventions to improve care coordination and address access barriers across VA and community care settings could support equitable access to healthcare for all Veterans—especially those with medical complexities, living far from healthcare services, or seeking women’s health services.
Data Availability:
The datasets during and/or analyzed during the current study available from the corresponding author on reasonable request.
References
Kenzie ES, Patzel M, Nelson E, Lovejoy T, Ono S, Davis MM. Long drives and red tape: mapping rural veteran access to primary care using causal-loop diagramming. BMC Health Serv Res. 2022;22:1075.
Spoont M, Greer N, Su J, Fitzgerald P, Rutks I, Wilt TJ. Rural vs. Urban Ambulatory Health Care: A Systematic Review. Department of Veterans Affairs (US). 2011.
Buzza C, Ono SS, Turvey C, Wittrock S, Noble M, Reddy G, Kaboli PJ, Reisinger HS. Distance is relative: unpacking a principal barrier in rural healthcare. J Gen Intern Med. 2011;26:648-654.
U.S. Department of Veterans Affairs. 10 things to know about the Veterans Choice Program. Available at: https://news.va.gov/39882/10-things-know-veterans-choice-program/. Accessed January 17, 2023.
115th Congress (2017-2018). S.2372: VA MISSION Act of 2018. Washington, D.C: U.S. Government Publishing Office; 2018.
Massarweh NN, Itani KM, Morris MS. The VA MISSION act and the future of veterans’ access to quality health care. JAMA. 2020;324(4): 343-344.
Perry A. Nearly One-Quarter of Veterans Live in Rural Areas, Census Bureau Reports, P.I. Office, Editor. US Census Bureau. 2017.
Cowper Ripley DC, Ahern JK, Litt, ER, Wilson, LK. Rural Veterans Health Care Atlas, 2nd edition FY-2015. Washington, D.C: VHA Office of Rural Health, Department of Veterans Affairs; 2017.
Albanese AP, et al. The VA MISSION Act of 2018: a potential game changer for rural GME expansion and veteran health care. J Rural Health. 2020;36(1):133.
National Academies of Sciences, Engineering, and Medicine. Communities in Action: Pathways to Health Equity. Washington, DC: The National Academies Press; 2017.
Gómez CA, Kleinman DV, Pronk N, Wrenn Gordon GL, Ochiai E, Blakey C, Johnson A, Brewer KH. Addressing Health Equity and Social Determinants of Health Through Healthy People 2030. J Public Health Manag Pract (JPHMP). 2021;7:S249–S257.
Mattocks KM, et al. Understanding VA’s use of and relationships with community care providers under the MISSION Act. Medical Care. 2021;59(6 Suppl 3):S252.
Gurewich D, et al. Did access to care improve since passage of the Veterans Choice Act?: differences between rural and urban veterans. Medical Care. 2021;59(6 Suppl 3):S270.
Govier DJ, Hickok A, Edwards ST, et al. Early Impact of VA MISSION Act Implementation on Primary Care Appointment Wait Time. J Gen Intern Med. 2023;38(4):889-897.
Miller CJ, et al. Veteran Perspectives on Care Coordination Between Veterans Affairs and Community Providers: A Qualitative Analysis. J Rural Health. 2021;37(2):437-446.
Kullgren JT, Fagerlin A, Kerr EA. Completing the MISSION: a blueprint for helping veterans make the most of new choices. J Gen Intern Med. 2020;35(5):1567-1570.
U.S. Department of Veterans Affairs. VISN 20: Norwest Network. Available at: https://www.va.gov/directory/guide/facility.asp?id=1020. Accessed September 15, 2021.
U.S. Department of Veterans Affairs. VA Recommendations to the Asset and Infrastructure Review Commission. Available at: https://www.va.gov/aircommissionreport/. Accessed May 22, 2022.
Economic Research Service U.S. Department of Agriculture. Rural-Urban Commuting Area Codes. Available at: https://www.ers.usda.gov/data-products/rural-urban-commuting-area-codes/. Accessed January 17, 2022.
Kallio H, Pietilä A-M, Johnson M., Kangasniemi M. Systematic methodological review: developing a framework for a qualitative semi-structured interview guide. J Adv Nurs. 2016;72(12):2954-2965.
Malterud K, Siersma VD, Guassora AD. Sample size in qualitative interview studies: guided by information power. Qual Health Res. 2016;26(13):1753-1760.
Clarke V, Braun V. Thematic analysis: a practical guide. Thematic Analysis, 2021; p. 1–100.
Creswell JW, Miller DL. Determining validity in qualitative inquiry. Theory Into Pract. 2000;39(3):124-130.
Sayre GG, et al. Accessing care through the Veterans Choice Program: the Veteran experience. J Gen Intern Med. 2018;33(10):1714-1720.
Affairs, D.o.V., Integrated Case Management Standards of Practice. Veterans Health Administration: Washington, DC. 2019.
Garvin LA, et al. Interorganizational Care Coordination of Rural Veterans by Veterans Affairs and Community Care Programs: A Systematic Review. Med Care. 2021;59(Suppl 3):S259-S269.
Cordasco KM, et al. Health and health care access of rural women veterans: Findings from the National Survey of Women Veterans. J Rural Health. 2016;32(4):397-406.
Adams MA, Sayre GG, Saini SD. The VA MISSION Act and Community Care for Veterans: What Every Community GI Doc Needs to Know. Am J Gastroenterol. 2019;114(8):1189-1191.
Kinney RL, et al. Coordinating women's preventive health care for rural veterans. J Rural Health. 2022;38(3):630-638.
Hynes DM, et al. Veterans’ Use of Veterans Health Administration Primary Care in an Era of Expanding Choice. Medical Care. 2021;59:S292-S300.
Sullivan E, Zahnd WE, Zhu JM, Kenzie E, Patzel M, Davis M. Mapping Rural and Urban Veterans' Spatial Access to Primary Care Following the MISSION Act. J Gen Intern Med. 2022; 37:12 2941–2947.
Douthit N, et al. Exposing some important barriers to health care access in the rural USA. Public Health. 2015;129(6):611-20.
Weeks WB, et al. Rural-urban disparities in health-related quality of life within disease categories of Veterans. J Rural Health. 2006;22(3):204-11.
Davila H, et al. Rural Veterans' Experiences With Outpatient Care in the Veterans Health Administration Versus Community Care. Med Care. 2021;59(Suppl 3):S286-s291.
Acknowledgements:
Contributors: We appreciate Veterans who participated in this study. We thank Jack Lazar for conducting interviews and Will Moore for providing his perspective during data analysis. We appreciate Alex Moore for their contributions to the drafting, editing, and submission support for this manuscript.
Funding
Funding for this research was provided by the U.S. Department of Veterans Affairs (VA) Office of Rural Health. The views expressed in this manuscript are those of the authors and do not necessarily reflect the views of the VA or the US government. Visit www.ruralhealth.va.gov to learn more.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest:
The authors declare that they do not have a conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Prior Presentations
This paper has not been presented elsewhere.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ramalingam, N.S., Barnes, C., Patzel, M. et al. “It’s Like Finding Your Way Through the Labyrinth”: a Qualitative Study of Veterans’ Experiences Accessing Healthcare. J GEN INTERN MED 39, 596–602 (2024). https://doi.org/10.1007/s11606-023-08442-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-023-08442-7