
Abstract
Introduction
On July 1, 2021, North Carolina’s Medicaid Transformation mandatorily switched 1.6 million Medicaid beneficiaries from fee-for-service to managed care plans. We examined the early enrollee experience in terms of engagement in plan selection, provider continuity, use of primary care visits, and assistance with social needs.
Methods
Using electronic health records (EHR) covering pre- and post-transition periods (1/1/2019–5/31/2022) from the largest provider network in western North Carolina, we identified all children and adults under age 65 with continuous Medicaid or private coverage. We conducted primary surveys of a random sample of Medicaid-covered enrollees and obtained self-reported rates of engagement in plan selection, continuity of provider access, and receipt of social need assistance. We used comparative interrupted time series models to estimate the relative change in primary care visits associated with the transition.
Results
Our EHR-based study cohorts included 4859 Medicaid and 5137 privately insured enrollees, with 398 Medicaid enrollees in the primary surveys. We found that 77.3% of survey participants reported that the managed care plan they were on was not chosen but automatically assigned to them, 13.1% reported insufficient information about the transition, and 19.2% reported lacking assistance with plan choice. We found that 5.9% were assigned to a different primary care provider. Over 29% reported not receiving any additional social need assistance. The transition was associated with a 7.1% reduction (95% CI, –11.5 to –2.7%) in the volume of primary care visits among Medicaid enrollees relative to privately insured enrollees.
Conclusions
Medicaid enrollees in North Carolina may have had limited awareness and engagement in the transition process and experienced a reduction in primary care visits. As the state’s transition process gains a foothold, future policy needs to improve enrollee engagement and develop evidence on healthcare utilization and patient outcomes.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Following approval of an 1115 waiver by the Centers for Medicare and Medicaid Services (CMS), North Carolina (NC) launched the “Medicaid Transformation” initiative, to move all Medicaid enrollees from a centralized fee-for-service to a managed care system.1 On July 1, 2021, 1.6 million of NC’s 2.5 million Medicaid enrollees in the “standard” fee-for-service plan—excluding “special populations” with intellectual and developmental disabilities and older adults—switched to one of six private managed care plans.1 For Medicaid enrollees, the process of transition from fee-for-service to managed care had the potential to adversely affect the continuity of care and access to existing providers.2
North Carolina is the 41st state to transition Medicaid to managed care.3 As most transitions occurred over two decades ago, the NC transition provides an opportunity to reassess the transition experience in the current healthcare landscape.4,5 Transition to managed care was a key milestone in the state’s major reforms toward alternative payment models.6 Informed by prior transitions, the transition in NC involved a wide-ranging set of interconnected system changes covering private and public stakeholders.7 Extensive notification strategies to the target beneficiaries were used, including mail, a mobile application, a website portal, and a call center with access to an enrollment broker.7 Reflecting the growing recognition of the critical role of social risk factors, the new managed care plans were responsible for screening and providing assistance for social needs, such as food and transportation.8,9 The ongoing public health and economic impact of the coronavirus-19 (COVID19) pandemic may have further exacerbated the transitional challenges.10,11
Despite the extensive preparation, “initial disruptions in access and administrative hassle for providers” were anticipated and reported in focus groups and interviews prior to transition.7,12,13 To assess the early enrollee experience following NC’s transition, we conducted primary surveys and extracted healthcare records data for a representative population of Medicaid enrollees in Forsyth County, the fourth largest NC county. Our focus was on enrollee awareness of the transition, active participation in the choice of a managed care plan, continuity with their primary care provider, and the volume of primary care visits.14 Additionally, we examined if enrollees’ choices of managed care plans were influenced by the additional services that each plan offered by each to address social risk factors.
Methods
Our study design utilized data covering pre- and post-transition time periods. In launching managed care, effective July 1, 2021, the state contracted with six managed care plans covering different regions of the state.15 Medicaid enrollees could enroll in a plan starting March 15, 2021; those who did not enroll by May 21, 2021, were auto-enrolled into one of the managed care plans.16 Enrollees were provided a grace period to switch plans until September 30, 2021. The state also extended the provision of care (and providers) under the prior plan to September 29, 2021. Therefore, we treated October 1, 2021, as the effective start of the post-transition period.
Study Cohorts
We used electronic health records (EHR) to identify all Medicaid enrollees who received primary care within the Atrium Health Wake Forest Baptist (AHWFB) network. The network is the largest provider in western North Carolina, with the flagship medical center and an extensive outpatient clinic network—including the county’s largest safety-net clinic—based in Forsyth County. We identified all patients with at least one primary care visit covered by Medicaid in 2019 and who remained in the AHWFB network through May 2022, ascertained by at least one encounter (e.g., medication pick-up, laboratory test, phone call to provider’s office, outpatient visit, or hospitalization) within the network during each calendar year (Appendix aFigure 1a). We excluded those who were 65 or older and those who died during the study period (1/2019–5/2022). We also excluded those who did not reside in Forsyth County at baseline. The resulting cohort (N = 4859) represented all eligible Medicaid enrollees in the network (“Medicaid EHR Cohort”) (see Appendix Section A for more details). For comparison, we obtained an analogous cohort of individuals with private insurance in the network (“Private EHR Cohort”) (N = 5137; Appendix aFigure 1b). We recruited and conducted primary surveys with a stratified random sample of adults and parents of children (< 18 years of age) from the Medicaid EHR Cohort (N = 398), to obtain data on patient experience (“Medicaid Survey Cohort”) (Appendix aFigure 2). A subgroup of 335 (84.2%) completed the second survey (Appendix aTable 1). See Appendix Section A for description of survey sampling, recruitment strategies, and survey response rates.
Data Sources
Data on patient experience were collected from two surveys of the Medicaid Survey Cohort. The surveys were developed in collaboration with a stakeholder advisory council that included Medicaid enrollees, community organizations, safety-net providers, hospital/clinic administrators, and clinician providers. We used questions from prior studies to assess healthcare access, utilization, costs, health literacy, and social risk factors.17,18 The first survey, administered during October 2021–February 2022, obtained data on enrollee characteristics—including social risk factors—and measures of healthcare access and utilization prior to transition. The second survey, administered during March–June 2022, obtained information on the participants’ early post-transition experiences including their awareness about transition to a managed care plan, continuity of care, and access to healthcare and social need services. We obtained EHR data on healthcare utilization during January 1, 2019, to May 31, 2022, for the Medicaid and Private EHR Cohorts (EpiCare, Verona, WI). The protocol for data acquisition and evaluation was approved by the Wake Forest University School of Medicine Institutional Review Board.
Measures
This study focused on indicators covering four domains: (1) engagement in managed care plan selection, (2) continuity of care, (3) receipt of social need services, and (4) primary care use. Data for the first three domains were obtained from the primary surveys of the Medicaid Survey Cohort and data on primary care use were obtained from patient EHR records of the Medicaid and Private EHR Cohorts. We used three dichotomous indicators of engagement in plan selection. We identified respondents who were auto-assigned to a managed care plan based on their response to the question, “Did you choose your plan or was one assigned to you?” (additional information on the survey items and responses are in Appendix Section B). Respondents who reported “completely disagree” and “somewhat disagree’ to the statement, “I had enough information about the change in Medicaid and that I was supposed to choose one among several Medicaid managed care plans,” were identified as lacking sufficient information. Respondents who responded “No” to the question, “Do you have someone you can call with questions about your Medicaid plan?” were identified as lacking assistance with Medicaid plans. We defined four dichotomous indicators of lack of continuity in healthcare: (1) lack of continuity with primary care provider, (2) lack of continuity with specialist provider, (3) lack of timely primary care access, and (4) respondent report of barriers to healthcare use. We defined a dichotomous indicator of respondents who reported not using any social need services from their managed care plan during the post-transition period. For individuals in the Medicaid and Private EHR Cohorts, we obtained a monthly count of the number of primary care visits from January 2019 to May 2022; as secondary outcomes, we obtained a monthly count of telehealth primary care visits, emergency department (ED) visits, and hospitalizations.
To characterize the variation in the prevalence of the survey-based outcome measures across the study cohorts, individual data were obtained from the surveys on a broad range of self-reported socio-demographic indicators and social risk factors. We used individual residential zip code to obtain area-level socio-demographic characteristics such as zip code-level poverty rate.19
Estimation
We obtained summary measures of the prevalence of main outcome measures, overall and by race/ethnicity. To characterize differences in the survey-based outcome measures across the study population, we used logit regression models to estimate the likelihood of an outcome measure associated with patient demographics, social risk factors, and area-level characteristics. As the Medicaid Survey Cohort is a stratified sample of the Medicaid EHR Cohort, we obtained individual sampling weights based on the stratification group, sampling rate, and survey response rate, and applied the sampling weights and stratification identifiers in all the statistical analyses. To measure changes in healthcare utilization associated with transition, we used a comparative interrupted time-series design to compare pre-transition (October 2020 to May 2021) to post-transition (October 2021 to May 2022) changes in the Medicaid EHR Cohort relative to the changes during the same period in the Private EHR Cohort.20 We used linear regression models with individual fixed effects to estimate within-individual changes in primary care visits between the pre- and post-transition periods overall and by age and race/ethnicity (Appendix Section B). This estimation specification adjusts for unobserved factors affecting healthcare utilization—such as family or social supports—that are likely to be constant during the study period. We performed sensitivity analyses using alternative model specifications: (1) we included data from the period in between the pre- and post-transition periods (“wash-out” period) and (2) we used an alternative pre-transition period of October 2019–February 2020 (i.e., pre-COVID period; Appendix Section C).
Tests of model estimates were 2-sided, with significance assessed at a p-value ≤ 0.05. All statistical analyses were performed using Stata Version 16.1 from May 1, 2022, to August 26, 2022.21
Results
Children accounted for 70% of the Medicaid enrollees in the Survey and EHR Cohorts (Table 1). Non-Hispanic Black and Hispanic enrollees comprised 50% and 33% of the Medicaid cohort, respectively. Nearly 60% of the cohort resided in a zip code with a poverty rate exceeding 20%. The Medicaid Survey Cohort exhibited a high prevalence of social risk factors, including food insecurity (41.3%), housing insecurity (41.3%), financial insecurity (13.5%), and low health literacy (26.9%) (Appendix aTable 2).
In the Medicaid Survey Cohort, 13.1% of enrollees reported lacking sufficient information about Medicaid Transformation and 19.2% lacked assistance with Medicaid plans (Table 2). Over 77% reported that the managed care plan they were on was assigned and not chosen; this rate was higher among Hispanic (92.0%) and non-Hispanic Black (72.8%) compared to non-Hispanic White (59.4%) enrollees. The proportion of enrollees who were assigned to a different primary care provider was 5.9%. The incidence of lack of timely primary care access was 20.5% overall and 40.1% among Hispanic enrollees. The reported incidence of barriers to healthcare use was 25.2% overall and 40.1% among Hispanic enrollees. Over 29% reported not receiving any additional resources or social needs services from their new managed care plan. The proportion of enrollees who reported obtaining assistance were food (8.9%), housing (5.2%), transportation (17.5%), medical care coordination (23.7%), medications (50.7%), and breast pump (15.7%) (Appendix aTable 3).
Adjusted for social risk factors, and relative to non-Hispanic White enrollees, Hispanic enrollees were more likely to report being assigned to a managed care plan (odds ratio (OR) = 3.41; 95% confidence interval (CI), 1.49 to 7.78) and a lack of timely primary care access (OR = 9.15; 95% CI, 1.46 to 57.45), and were less likely to report not obtaining additional resources and services from their new managed care plan (OR = 0.34; 95% CI, 0.15 to 0.73) (Table 3). Based on regression estimates of awareness and continuity measures, those with the highest level of education were more likely to report a lack of sufficient information about transition (odds ratio (OR) = 14.99; 95% CI, 1.75 to 128.54) relative to those who did not complete high school. Enrollees who reported housing and transportation challenges were more likely to report a lack of timely primary care access and barriers to healthcare use.
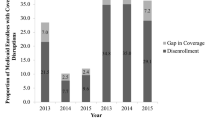
Figure 1 gives the monthly volume of all primary care visits for the EHR Cohorts with Medicaid and private coverage. To assess the change in utilization after the transition to managed care, we compared the volumes in the October-to-May periods (shaded) before and after the Medicaid Transformation. In the pre-transition period, there were an aggregate of 590.6 primary care visits per 1000 Medicaid enrollees per month, of which 35.7 were telehealth visits (Table 4). Treating the cohort with private coverage as the reference group and using the October 2020 to May 2021 period as the reference period, the comparative interrupted time-series regression analysis indicated that Medicaid-covered enrollees experienced a decrease of 41.8 primary care visits (7.1%; 95% confidence interval (CI), –11.5 to –2.7%) after the transition compared to patients with private coverage. The transition was also associated with a reduction of 9.3 telehealth primary care visits (26.1%; 95% CI, –36.2 to –15.7%) and no change in the volume of ED visits and hospitalizations. Stratified analysis indicated a significant decrease in primary care visits among (a) children (–9.2%; 95% CI, –16.2 to –2.3%) and adults (–11.3%; 95% CI, –16.6 to –6.0%), and (b) non-Hispanic White (–9.2%; –18.2 to –0.2%) and non-Hispanic Black adults (–8.2%; 95% CI, –15.5 to –1.0%) (Appendix aTable 4). Among Hispanic adults, the change was not statistically significant (–9.3%; 95% CI, –23.3 to 4.8%). In sensitivity analysis, including data for the wash-out period and use of a Poisson regression specification yielded consistent findings (Appendix aTable 5). When we used the alternative pre-COVID period as a pre-transition period, the transition was associated with a reduction in the volume of primary care visits (25.2%; 95% CI, –29.1 to –21.1%) (Appendix aTable 5).

Number of primary care provider visits (EHR cohorts). For the Medicaid-covered and privately covered EHR cohorts we obtained the number of primary care physician (PCP) visits from 1/1/2019 to 4/30/2022. The count of primary care provider visits includes in-person and telehealth visits. The gray blocks represent the 8-month Oct to May periods during the study period. The last gray block (Oct 2021 to May 2022) is the post-transition period while the other block represents the pre-transition period.
Discussion
Our study of the early enrollee experience of NC’s Medicaid Transformation highlights three findings. First, a sizable proportion of enrollees reported that they were not adequately informed or engaged in the transition process. Second, most enrollees were able to keep their primary care provider. Third, enrollees experienced a reduction in the volume of primary care visits after the transition to managed care.
Despite extensive planning, public hearings, and the multipronged “information blitz” preparing Medicaid enrollees about the transition process, we found multiple indicators of a lack of adequate information.14,22 Over 77% reported being automatically assigned to their managed care plan. This share was 59% among non-Hispanic White, 73% among non-Hispanic Black, and 92% among Hispanic enrollees. To our knowledge, there is no population-level evidence for all of NC. One state-level qualitative study of enrollees and other key informants by the Urban Institute found high rates of auto-enrollment.12 Much of the prior literature is based on transitions to managed care that occurred in the 1990s, with 35 of the 40 states that preceded NC having transitioned prior to 2003.3,4,5 One national survey reported that among 16 states that used auto-enrollment to managed care, the median rate of enrollees auto-assigned was 25%.23 Use of auto-assignment was associated with unfavorable patient experiences with providers.24,25 Morton (1998) noted that “auto-assignment … can be an important signal within the state system that information is not flowing to the Medicaid individual” and enrollees who actively discussed their options were more likely to make enrollment decisions.23 In the Urban Institute study, state officials suggested that the high rate of auto-enrollment in NC may be indicative of the superior performance of the auto-enrollment algorithm in ensuring provider continuity for most enrollees.12 However, two qualitative studies found that enrollees reported being unaware of the transition and lacked information about plan selection.12,13 Also, our study found that those with higher educational achievement were more likely to report not having sufficient information, suggesting an expectation to receive further information about the Medicaid transition among this subgroup. In the eight months following the transition, less than 10% of the surveyed enrollees reported receiving assistance for most social needs, including food, housing, and utilities. The highest rate of assistance was for medications (51%), care coordination (23%), and transportation (18%). Lack of awareness about services covered may be behind the low uptake of assistance.12,13
Prior studies of longitudinal experience with managed care have reported a narrowing of the number of primary care physicians and specialists covered over time (in-network providers) thereby increasing discontinuity of care with regular providers.26 Our survey indicated a high level of continuity of care, with 5.9% and 13.4% of enrollees reporting an inability to continue care with their primary care provider and specialists, respectively. High provider continuity may be due to the fact that the AHWFB network accepted all the new plans. Another qualitative study reported that many providers did not accept all plans due to administrative burden and complexity.12 Relative to earlier transitions in other states, higher provider continuity may also be due to better matching from the auto-enrollment algorithm taking prior provider relationships into account.12,16,27
The number of primary care visits decreased in the post-transition period among Medicaid and privately insured patients, with a larger reduction among Medicaid enrollees. National studies of healthcare utilization since the COVID-19 pandemic outbreak have found multiple periods of reduction and recovery in healthcare utilization.28,29 The extent to which the larger reduction among Medicaid enrollees is associated with the transition to managed care is unclear; qualitative studies indicate enrollee concerns with timeliness of access and changes in providers.12,13 We cannot rule out the role of other factors, particularly the economic and policy changes arising from the pandemic.30,31
As Medicaid Transformation continues, and as the state transitions the remaining Medicaid enrollees, our study has important implications for future policy. Going forward, enrollees have a choice to switch plans and providers every year, and the available managed care plans and providers may change over time. Lack of enrollee engagement may lead to unexpected consequences, including delays in accessing care, ED use for untreated primary care concerns, and loss of provider continuity.
We recognize several limitations of the study. Firstly, our study is limited to Forsyth County and may not represent the statewide experience. Second, our findings represent the early experience following the transition. Some enrollees may have had limited engagement with healthcare providers under their new managed care plan. Third, our analysis relating to the change in the volume of primary care visits following transition does not establish a causal relationship, given the potential changes in healthcare utilization patterns following the COVID-19 public health emergency. While our data do not include care received outside the AHWFB network, in our estimation of the change associated with transition, we compare pre- with post-transition change in the volume for the same cohort of individuals within AHWFB. If the transition caused a change in the relative use of AWFBH and non-AWFBH providers, then our estimate may not fully capture the change associated with the transition. As our study cohort included those who were alive during the study period, we cannot examine the impact of the transition on mortality.
Our study is the first to develop population-level evidence on the early experience of enrollees following North Carolina’s Medicaid Transformation. We found a clear indication of inadequate engagement in the choice of a plan and use of social need services. Over time, as Medicaid managed care gains further foothold, an improvement in the awareness of the policy and choices relating to plan choice and assistance for social needs will be important in attaining greater enrollee engagement and improved patient experience, healthcare utilization, and patient outcomes.
Data Availability
The data are not publicly available due to patient’s privacy and consent. The deidentified data that support the findings of this study may be available upon reasonable request to the corresponding author.
References
North Carolina Department of Health and Human Services. North Carolina’s Proposed Program Design for Medicaid Managed Care. 2017. Available at: https://files.nc.gov/dhhs/documents/files/MedicaidManagedCare_ProposedProgramDesign_REVFINAL_20170808.pdf. Accessed July 17, 2023.
Donnelly-DeRoven C. Three months into Medicaid transformation, providers say the new administrative burdens are crushing. North Carolina Health News. 2022. Available at: https://www.northcarolinahealthnews.org/2021/10/19/three-months-into-medicaid-transformation-providers-say-the-new-administrative-burdens-are-crushing/. Accessed July 17, 2023.
Kaiser Family Foundation. Medicaid Managed Care Tracker. 2022. Available at: https://www.kff.org/statedata/collection/medicaid-managed-care-tracker/. Accessed July 17, 2023.
Franco Montoya D, Chehal PK, Adams EK. Medicaid Managed Care's Effects on Costs, Access, and Quality: An Update. Annu Rev Public Health. 2020;41(1): 537-549.
Sparer M. The Synthesis Project, Report No. 23. Medicaid managed care: Costs, access, and quality of care. Robert Wood Johnson Foundation. 2012. Available at: https://www.cancercarediff.org/wp-content/uploads/2020/12/managed-care-rwjf.pdf. Assessed July 17, 2023.
McClellan M, Alexander M, Japinga M, Saunders RS. North Carolina: The New Frontier For Health Care Transformation. Health Affairs Blog. 2019. Available at: https://www.healthaffairs.org/do/10.1377/forefront.20190206.576299/.
Allen EH, Johnston E, Courtot B, Caraveo CA, Gonzalez D, Long J. North Carolina Medicaid’s Transition to Risk-Based Managed Care. 2022. Urban Institute. Available at: https://www.urban.org/research/publication/north-carolina-medicaids-transition-risk-based-managed-care. Accessed July 17, 2023.
Apenteng BA, Kimsey L, Opoku ST, Owens C, Peden AH, Mase WA. Addressing the Social Needs of Medicaid Enrollees Through Managed Care: Lessons and Promising Practices from the Field. Popul Health Manag. Feb 2022;25(1):119-125.https://doi.org/10.1089/pop.2021.0142
North Carolina Department of Health and Human Services. North Carolina's Proposed Program Design for Medicaid Managed Care. 2017. Available at: https://medicaid.ncdhhs.gov/proposed-program-design. Accessed July 17, 2023.
Allen HL, Sommers BD. Medicaid and COVID-19: At the Center of Both Health and Economic Crises. JAMA. 2020;324(2):135-136.https://doi.org/10.1001/jama.2020.10553
Patel S., McGinnis T. Inequities Amplified By COVID-19: Opportunities For Medicaid To Address Health Disparities. 2020. Health Affairs Blog. Available at: www.healthaffairs.org/do/10.1377/hblog20200527.351311/full/. Accessed July 17, 2023.
Allen EH, Verdeflor A, Alvarez Caraveo C. Findings from the First Year of Medicaid Managed Care in North Carolina. 2022. Urban Institute. Available at: https://www.urban.org/research/publication/findings-first-year-medicaid-managed-care-north-carolina. Accessed July 17, 2023.
Zimmer RP, Hanchate AD, Palakshappa D, Aguilar A, Wiseman K, Crotts CI, Abdelfattah L, Sostaita D, Montez K. Perceptions of North Carolina’s Medicaid Transformation: A Qualitative Study. N.C. Med J. 2023; 84(6). doi:https://doi.org/10.18043/001c.83956.
Engel-Smith L. NC Medicaid managed care information blitz did not reach all enrollees. North Carolina Health News. 2021. Available at: https://www.northcarolinahealthnews.org/2021/06/22/nc-medicaid-managed-care-information-blitz-did-not-reach-all-enrollees/. Accessed July 17, 2023.
North Carolina Department of Health and Human Services. North Carolina's Transformation to Medicaid Managed Care. 2022. Available at: https://medicaid.ncdhhs.gov/transformation. Accessed July 17, 2023.
North Carolina Department of Health and Human Services. NC Medicaid Managed Care Health Plan Assignments Completed for Beneficiaries. 2021. Available at: https://www.ncdhhs.gov/news/press-releases/2021/05/26/nc-medicaid-managed-care-health-plan-assignments-completed-beneficiaries. Accessed July 17, 2023.
Hamilton CM, Strader LC, Pratt JG, et al. The PhenX Toolkit: get the most from your measures. Am J Epidemiol. 2011;174(3): 253-260.
Sarkar U, Schillinger D, López A, Sudore R. Validation of self-reported health literacy questions among diverse English and Spanish-speaking populations. J Gen Intern Med. Mar 2011;26(3):265-71.https://doi.org/10.1007/s11606-010-1552-1
Agency for Healthcare Research & Quality. Social Determinants of Health Database. 2022. Available at: https://www.ahrq.gov/sdoh/data-analytics/sdoh-data.html. Accessed July 17, 2023.
Shadowen H, Alexander M, Guerra L, et al. Virginia Medicaid Expansion: New Members Report Reduced Financial Concerns During The COVID-19 Pandemic. Health Affairs. 2022;41(8): 1078-1087.
StataCorp. 2019. Stata Statistical Software: Release 16. College Station, TX, StataCorp LP.
North Carolina Department of Health and Human Services. Proposed Program Design. 2017. Available at: https://medicaid.ncdhhs.gov/proposed-program-design. Accessed July 17, 2023.
Morton LW. Medicaid enrollment choice into managed care health plans. Med Care Res Rev. Jun 1998;55(2):211-38.https://doi.org/10.1177/107755879805500204
McDonnell DD, Graham CL. Medicaid beneficiaries in California reported less positive experiences when assigned to a managed care plan. Health Aff (Millwood) 2015;34(3): 447-454.
Davis K, Collins KS, Schoen C, Morris C. Choice matters: enrollees' views of their health plans. Health Aff (Millwood). 1995;14(2): 99-112.
Ndumele CD, Staiger B, Ross JS, Schlesinger MJ. Network Optimization And The Continuity Of Physicians In Medicaid Managed Care. Health Aff (Millwood). Jun 2018;37(6):929-935.https://doi.org/10.1377/hlthaff.2017.1410
North Carolina Department of Health and Human Services. What is auto-enrollment and how does it work? 2021. Available at: https://files.nc.gov/ncdma/documents/Providers/playbook/AutoEnrollment-FACTSHEET_FINAL_202310525.pdf. Accessed July 17, 2023.
Mafi JN, Craff M, Vangala S, et al. Trends in US Ambulatory Care Patterns During the COVID-19 Pandemic, 2019-2021. JAMA. 2022;327(3):237-247.https://doi.org/10.1001/jama.2021.24294
Mehrotra A, Chernew M, Linetsky D, Hatch H, Cutler DM, Schneider EC. The Impact of the COVID-19 Pandemic on Outpatient Care: Visits Return to Prepandemic Levels, but Not for All Providers and Patients. The Commonwealth Fund. 2020. Available at: https://www.commonwealthfund.org/publications/2020/oct/impact-covid-19-pandemic-outpatient-care-visits-return-prepandemic-levels. Accessed July 17, 2023.
Artiga S, Garfield R, Orgera K. Communities of Color at Higher Risk for Health and Economic Challenges due to COVID-19. K. F. Foundation. 2020. Available at: https://www.kff.org/coronavirus-covid-19/issue-brief/communities-of-color-at-higher-risk-for-health-and-economic-challenges-due-to-covid-19/. Accessed July 17, 2023.
Azar KMJ, Shen Z, Romanelli RJ, et al. Disparities In Outcomes Among COVID-19 Patients In A Large Health Care System In California. Health Affairs. 2020;39(7): 1253-1262.
Funding
This research has been supported by a grant from the Kate B. Reynolds Charitable Trust. The Trust had no participation in the “design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and the decision to submit the manuscript for publication.” Deepak Palakshappa is supported by the National Heart, Lung, and Blood Institute of the National Institutes of Health under Award Number K23HL14690. Rachel Zimmer is supported by the Department of Health and Human Services Geriatric Academic Care Award Number K01HP33462. Amresh Hanchate and Lindsey Abdelfattah had full access to the data used for the study and take responsibility for the integrity of the data and the accuracy of the data analysis. The views expressed in this article are those of the authors and do not necessarily represent the views of the Kate B. Reynolds Charitable Trust and Wake Forest University School of Medicine.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest:
None.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Hanchate, A.D., Abdelfattah, L., Palakshappa, D. et al. North Carolina’s Medicaid Transformation: the Early Enrollee Experience. J GEN INTERN MED 38, 3295–3302 (2023). https://doi.org/10.1007/s11606-023-08319-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-023-08319-9