
Abstract
Background
Chronic disease patients who are the greatest users of healthcare services are often referred to as high-need, high-cost (HNHC). Payers, providers, and policymakers in the United States are interested in identifying interventions that can modify or reduce preventable healthcare use among these patients, without adversely impacting their quality of care and health. We systematically reviewed the evidence on the effectiveness of complex interventions designed to change the healthcare of HNHC patients, modifying cost and utilization, as well as clinical/functional, and social risk factor outcomes.
Methods
We searched 8 electronic databases (January 2000 to March 2021) and selected non-profit organization and government agency websites for randomized controlled trials and observational studies with comparison groups that targeted HNHC patients. Two investigators independently screened each study and abstracted data into structured forms. Study quality was assessed using standard risk of bias tools. Random-effects meta-analysis was conducted for outcomes reported by at least 3 comparable samples.
Results
Forty studies met our inclusion criteria. Interventions were heterogenous and classified into 7 categories, reflecting the predominant service location/modality (home, primary care, ambulatory intensive caring unit [aICU], emergency department [ED], community, telephonic/mail, and system-level). Home-, primary care-, and ED-based interventions resulted in reductions in high-cost healthcare services (ED and hospital use). ED-based interventions also resulted in greater use of primary care. Primary care- and ED-based interventions reduced costs. System-level transformation interventions did not reduce costs.
Discussion
We found limited evidence of intervention effectiveness in relation to cost and use, and additional evidence is needed to strengthen our confidence in the findings. Few studies reported patient clinical/functional or social risk factor outcomes (e.g., homelessness) or sufficient details for determining why individual interventions work, for whom, and when. Future evaluations could provide additional insights, by including intermediate process outcomes and patients’ experiences, in assessing the impact of these complex interventions.
PROSPERO Registration Number
CRD42020161179
Similar content being viewed by others

Avoid common mistakes on your manuscript.
INTRODUCTION
Patients referred to as high-need, high-cost (HNHC) constitute a small percentage of all US patients but account for a disproportionally high level of healthcare use and cost.1 Often these patients have multiple chronic conditions, and their care may be complicated by functional limitations, behavioral health concerns, and social risk factors (e.g., homelessness).1 HNHC patients often use higher levels of high-cost care, particularly emergency department (ED) visits or hospitalizations. Some of this care is believed to be potentially preventable or modifiable through better management of chronic conditions in primary care or other ambulatory care settings.2
Finding effective interventions to address HNHC patient needs is a pressing concern for the US healthcare system. One 2014 US-focused systematic review of HNHC patient interventions found that care and case management models improved patient satisfaction, clinical outcomes, and healthcare use and spending.3 Other prior reviews have been limited to specific settings (e.g., ED),4,5,6,7,8,9,10 included studies conducted outside the USA,4,5,6,7,9 or included study designs that may lead to biased results (e.g., no comparison groups).7,11,12 In contrast, this review focuses on more rigorous evaluations to understand the effectiveness of a broad set of HNHC interventions, tested across US healthcare system settings.
The objective of this review was to evaluate the effectiveness of interventions targeting HNHC patients that intend to improve the quality of care while reducing potentially preventable or modifiable healthcare use and cost. This work is particularly timely as US payers, particularly the Centers for Medicare & Medicaid Services (CMS), increasingly require payment through alternative payment models that incorporate financial risk. Health systems and providers recognize that their success in these models can depend on their effectiveness in addressing the care and costs of HNHC patients.
METHODS
This systematic review was developed through a larger project conducted by the RTI-University of North Carolina Evidence-Based Practice Center for the Agency for Healthcare Research and Quality (AHRQ). We adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines.13 This review followed an a priori protocol14 and is registered with PROSPERO (CRD42020161179). The full report provides additional details on the methods and results.15
Search Strategy and Study Selection
We searched PubMed, the Cochrane Library, CINAHL, Embase, PsycINFO, Web of Science, Academic Search Premier, and Scopus for English-language articles published from January 1, 2000, to March 4, 2021, using relevant medical subject headings (MeSH) and keywords associated with HNHC patients and interventions (full search strategy provided in Appendix 1). We also searched for gray literature from selected websites (e.g., CMS). Reference lists of pertinent articles were hand-searched to identify additional studies.
Two reviewers independently screened titles and abstracts and reviewed full-text articles. Disagreements were resolved by consensus or a third reviewer.
The detailed eligibility criteria are in Appendix 2. Briefly, any approach to a HNHC patient intervention was included if it was conducted in a noninstitutional setting; initial contact could be before hospital discharge. The overall goal across these interventions was to improve the healthcare use and outcomes of HNHC patients. Studies were eligible if they presented intervention findings on noninstitutionalized, US adults identified as HNHC based on having high healthcare use or cost, measured over ≥6 months. High use or cost was defined by study authors. Study designs included randomized controlled trials (RCTs) and observational studies. Studies had to compare intervention participant results with those of a comparison group.
Data Extraction and Quality Assessment
We abstracted data on study characteristics, including design, participants, intervention, and outcome measures (changes in healthcare utilization, cost, clinical and functional outcomes, and social risk factors). Abstracted outcomes are listed in Appendix 3. One reviewer abstracted data into a structured evidence table and a second reviewer checked for completeness and accuracy. Two independent reviewers assessed the risk of bias (RoB) for each study as low, some concerns, or high using the Cochrane RoB 2.0 tool16 for RCTs and the ROBINS-I tool17 for observational studies. Discrepancies in ratings between reviewers were resolved through discussion.
Data Synthesis and Analysis
Given the diversity of HNHC interventions, we adapted Bodenheimer’s scheme to group care management models by predominant service location/modality to classify each study into one intervention category for synthesis.18 Included studies were categorized as follows: home-based care; primary care; ambulatory intensive caring unit (aICU); ED; community; telephonic/mail; or system-level transformation. The predominant service location for interventions that incorporated multiple locations/modalities was determined through consensus. Some studies included multiple distinct intervention cohorts. We refer to each cohort-comparison group pair as a “sample.” For broader interventions (e.g., practice-wide interventions), only HNHC patient findings were included.
We synthesized study outcomes narratively or, when possible, quantitatively. When an outcome was reported in ≥3 samples in an intervention category and study design, we conducted a random-effects meta-analyses, using the Sidik-Jonkman model with Knapp-Hartung standard errors in Stata 16.19
The strength of evidence (SoE) of outcomes was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach,20 as modified by the AHRQ Evidence-based Practice Center Program.21 Assessing study limitations, directness, consistency, precision, and reporting bias, each outcome reported by ≥2 studies within an intervention category was assigned a grade of high, moderate, low, or insufficient (Appendix 4 defines these levels).22 Two senior reviewers independently graded each relevant outcome. Disagreements were resolved through discussion. High RoB studies were solely used to qualitatively consider their impact on SoE grades.17
RESULTS
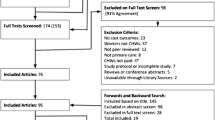
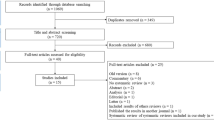
A total of 40 studies (reported in 46 articles) met eligibility criteria. Figure 1 depicts the article flowchart. We identified 19 RCTs and 21 observational studies. We rated 4 RCT studies as low RoB23,24,25,26 and 15 RCTs as some concerns.27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42 We rated 12 observational studies as some concerns for RoB.43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58 Nine observational studies59,60,61,62,63,64,65,66,67,68 were rated as high RoB because of critical flaws in ≥1 category. Of these, 7 high RoB studies59,61,62,63,64,65,66,68 inadequately controlled for confounding: 459,63,64,66 did not control for confounding at all, 261,62,65 were unclear about the variables included in models, and 168 did not control for important baseline characteristics that differed in the treatment and control groups. Two studies64,67 inadequately controlled for potential selection bias, and one60 for potential bias due to missing data. Appendix 5 shows the study-specific RoB ratings.

Flowchart of study selection.
Our analysis included 31 studies reporting on 38 samples (Table 1). Most samples focused on adults of all ages (n=33). Samples mostly included participants with Medicare coverage (n=19) or a mix of insurance types (n=10). Most samples were conducted in multiple study sites (n=29). Only 2 samples had fewer than 100 participants (minimum: 72). All but one sample27 was compared with usual care.
Participant eligibility varied widely across studies and was based on study author established minimum thresholds that they considered represented high cost and/or utilization. Some samples also used diagnoses and/or risk scores. Criteria for high use ranged from ≥1 hospitalization to ≥11 outpatient visits. Criteria for high cost included thresholds by dollar values (e.g., ≥$5000) and percentiles (e.g., top 10% of expenditures). Samples were mostly based on high use alone (n=13) or high cost or use with ≥1 chronic condition (n=15).
Intervention Effectiveness by Intervention Category
We present the results for outcomes with a grade of low SoE or better, organized by intervention category (Table 2). Although samples reported over 100 unique outcomes, only 25 outcomes were reported by ≥2 samples within an intervention category. Only a limited number of clinical and functional outcomes and no social risk factor outcomes were graded. No outcomes were graded as high SoE. Sensitivity analyses including the 9 high RoB, observational studies did not impact final SOE grades. All study and intervention characteristics and SoE grades are available in Appendix 6.
Home-Based Care Interventions
One RCT (2 samples)37 and one observational study56 evaluated interventions providing in-home care for patients who had difficulty leaving their homes. The RCT37 assessed in-home care management through a visiting physician as part of the larger Medicare’s Care Management for High Cost Beneficiaries (CMHCB) demonstration, which tested various pay-for-performance and care management/coordination approaches among high-cost complex Medicare patients. The observational study, Independence at Home (IAH)56, evaluated the effectiveness of providing home-based primary care to Medicare patients with multiple chronic conditions and functional limitations.
Home-based care interventions resulted in reductions in hospitalizations for ambulatory care sensitive conditions (ACSC) (a quality indicator for preventable utilization)69, increases in receipt of influenza vaccinations (a quality measure), and no change in mortality (all findings low SoE).
Primary Care–Based Interventions
Five RCTs (6 samples)23,29,30,38,40 and 1 observational study58 evaluated interventions embedded in primary care practices. Three RCTs23,38,40 tested team-based care or case management interventions. One23 of the RCTs examined providing psychiatric nurse-led case management to high-using patients. Another38 (2 samples), a Medicare CMHCB intervention, tested embedding comprehensive nurse-led case management, and a third40 tested community health worker (CHW)–led complex care management for Medicaid patients. A fourth RCT30, conducted in a health maintenance organization (HMO), examined providing depression management to high outpatient users, while an observational study58 tested providing care coordination and disease management to Medicaid managed care organization patients. A fifth RCT29 tested providing group visits to older adults to support them in managing their chronic conditions.
Primary care–based interventions resulted in reductions in hospitalizations and total costs (−$4,119 [95% CI, −7,935 to −302] (Fig. 2)) (both low SoE). However, based on evidence from the 2 CMHCB independent samples, these interventions also resulted in a reduction in receipt of influenza vaccinations (low SoE for unfavorable findings).

Forest plot of annual total costs for primary care-based, telephonic/mail, and system-level transformation interventions for HNHC patients. The size of the squares reflects the study’s relative weight and horizontal lines represent 95% CIs of the estimates. Diamonds represent the pooled mean with the points of the diamonds representing 95% CIs. Studies with multiple listed entries included multiple, non-overlapping samples. Four system-level transformation samples52,53,54 reported the total sample size but not the sample size specific to their HNHC patient population; the total sample size for the FQHC APCP52 was 730,353; 1,730,958 for CPC53; 5,163,969 for CPC+54 Track 1 practices sample; and 4,804,265 for CPC+54 Track 2 practices sample. Abbreviations: CHW, community health worker; CI, confidence intervals; CMHCB, Medicare Care Management for High Cost Beneficiaries Demonstration; CPC, Comprehensive Primary Care initiative; CPC+, Comprehensive Primary Care Plus initiative; ED, emergency department; FQHC APCP, Federally Qualified Health Center Advanced Primary Care Practice; HNHC, high-need, high-cost; IAH, Independence at Home; NR, not reported; OBS, observational study; RCT, randomized controlled trial.
Ambulatory Intensive Caring Unit–Based Interventions
aICUs are a separate clinic or a separate team within a clinic providing enhanced care. One RCT31,32 and 2 observational studies45,50,51 evaluated aICU interventions for HNHC patients. The RCT31,32 compared a Veterans Affairs intensive care management and coordination initiative to its ongoing patient-centered medical home (PCMH) model. One observational study45 evaluated intensive chronic care management from a specialized team in a university healthcare system. A second observational study50,51 evaluated a multidisciplinary team providing care coordination and referral to intensive primary care in a Medicaid accountable care organization. All outcomes received an SoE grade of insufficient evidence, primarily because of inconsistent findings.
Emergency Department–Based Interventions
Four RCTs25,28,39,42 and 1 observational study47 evaluated interventions for high-ED use patients recruited in the ED and providing care by an ED-affiliated team. All interventions provided care/case management to coordinate clinical care and support services and promoted increasing the receipt of care in ambulatory settings. Two RCTs provided patient navigation; one25 for Medicaid patients at an ED in Connecticut and a second39 at multiple EDs in Tennessee. Another RCT28 evaluated case management, conducted by psychiatric social workers, that included assistance with psychosocial problems (e.g., homelessness). A fourth RCT42 provided ED-based clinical care planning followed by CHW-led care coordination. The observational study47 telephonically provided nurse-led decision support to elderly ED patients.
ED-based interventions resulted in reductions in ED visits (moderate SoE) and ED costs (low SoE). Further, greater use of primary care visits (low SoE) suggested a shift to lower-cost care. ED-based interventions resulted in reductions in hospitalizations but no difference in hospital costs (both low SoE).
Community-Based Interventions
Community-based interventions, where the care team provides services primarily at community sites convenient to their HNHC patients, were evaluated in three RCTs24,26,41 and 3 observational studies43,44,46,49. The Camden model identifies HNHC patients in real time and uses multidisciplinary relationship-based care management to address medical and psychosocial concerns. This model was evaluated in three studies, one RCT24 and 2 observational study replications (one46,49 among Medicare patients and another44 among mostly Medicaid-eligible patients). Another RCT26 provided nurse-led care management to disabled, Medicaid patients with behavioral health problems. A third RCT41 examined a housing intervention with case management and other supportive services for chronically homeless adults. One observational study43 evaluated social worker-led, post-hospital discharge care transitions tailored to patients’ care coordination needs.
Evidence from three samples found no difference in mortality (low SoE). All cost and use outcomes were graded as insufficient.
Telephonic/Mail Interventions
Five RCTs27,33,34,35,36 (8 samples) and 1 observational study48 evaluated interventions where most services were provided remotely by telephone, mail, or a device. Four of the RCTs33,34,35,36 examined Medicare CMHCB interventions. One34 provided multidisciplinary care management telephonically or in writing and one35 (2 samples) provided home monitoring devices to support health monitoring and communication with nurse care managers. Two other studies were HMO-based. One RCT27 mailed personalized health promotion materials to high-use members with arthritis, hypertension, or diabetes. An observational study48 telephonically provided social needs screening and navigation to members predicted to be high users. All outcomes received an SoE grade of insufficient evidence.
Two of the CMHCB RCTs33,36 (4 samples) tested disease and care management delivered telephonically to chronic kidney disease patients. This evidence was graded separately because, unlike other studies in the review, it focuses on patients with one condition. The evidence is summarized in Appendix 7.
System-Level Transformation Interventions
Four large, observational studies52,53,54,55,56,57 (5 samples), testing care delivery and payment innovations to lower cost and improve quality of care across all Medicare patients at a practice, separately measured outcomes for HNHC patient subgroups. Comprehensive Primary Care (CPC)53 and CPC Plus (2 samples)54,55 aimed to reform care delivery in primary care practices using care management fees to support improvements, while the Federally Qualified Health Center Advanced Primary Care Practice (FQHC APCP) initiative52 aimed to help FQHCs transform into APCPs through PCMH recognition. The IAH study56,57 (one sample discussed in the “Home-Based Care Interventions” section) assessed, in a separate sample, the effect of providing global incentive payments to home-based primary care practices.
The pooled estimate of changes in annual costs, using data from all 5 samples, showed no difference between treatment and control HNHC patients (−$13 [95% CI, −132 to 106] (Fig. 2)) (low SoE for no difference).
DISCUSSION
In this review, we sought to inform policy and clinical practice by identifying intervention categories that have been effective in reducing HNHC patients’ preventable healthcare use or modifying high-cost to lower-cost services, while maintaining or improving clinical outcomes. To our knowledge, this is the most comprehensive and rigorous systematic review of the effectiveness of interventions for HNHC patients across multiple US healthcare settings. Because we identified a diverse group of interventions, we sorted samples into 7 categories. As a result, some intervention categories were limited to a small number of samples, especially home-based and aICU-based care.
Despite considerable interest and investment in improving care and reducing costs for HNHC patients, studies demonstrated limited effectiveness. Most outcomes across intervention categories were graded as insufficient because of limited evidence or inconsistent results across samples. Future research providing additional data on the effectiveness of interventions for HNHC patients is essential.
Our review found limited evidence that some HNHC intervention categories reduce costs and use of high-cost services. ED- and primary care-based interventions were associated with reductions in cost. ED-, primary care-, and home-based interventions were associated with reductions in hospitalizations. ED-based interventions were also associated with reductions in ED use. Samples reported few intermediate or clinical, functional, and social risk factor outcomes. Home-based care and community-based interventions were associated with no difference in mortality. Evidence was too limited to assess any social risk factor outcomes.
ED-based interventions identified HNHC patients based on high ED use and changed their ED services through care/case management. Similarly, a previous systematic review found ED-based case management interventions were effective for reducing frequent ED use among high-risk, US. patients.10 We also found that ED-based interventions were successful at reducing hospitalizations and increasing primary care visits. While increases in primary care use suggest that these interventions may change where patients receive care, future studies directly measuring the pathway of individual patient replacement of higher cost ED care with lower cost primary care is needed.
Primary care-based interventions used multidisciplinary care teams to support and coordinate care. Otherwise, these interventions were heterogenous in their approach and team composition. Consistent with a prior review,70 we found these interventions to be associated with reductions in hospitalizations. Our further finding of overall reductions in costs suggests that reductions in hospitalizations outweighed increases in other care. Further investigations of how care was modified and its effect on health outcomes are needed.
Home-based care was the only category with evidence to assess changes in ACSC hospitalizations, a direct measure of preventable utilization. These interventions resulted in reductions in ACSC hospitalizations among infirm patients with prior hospitalizations whose conditions could be managed in ambulatory settings.69 However, the evidence was insufficient to determine if at-home care also reduced total costs.
Changes in receipt of influenza vaccinations were found to be favorable in home-based care but unfavorable in primary care-based interventions. Study authors of the primary care evaluation explained the unexpected finding as due to a higher baseline rate in intervention patients that limited the intervention’s ability to show improvement.38
Community-based interventions largely delivered services outside the healthcare system. Besides supporting improved self-care and access to medical and mental health services, these interventions assumed the additional challenge of addressing HNHC participants’ social risk factors by helping them navigate access to community resources and social services. Interventions included the Camden model that identified HNHC patients in real time and provided them with intensive, relationship-based assistance.24,44,46,49 Community-based interventions were associated with no difference in mortality and findings related to healthcare use and costs were inconclusive. However, this body of complex interventions generally lacked reporting on intermediate outcomes, like changes in access to social services. Therefore, we cannot know if these ambitious interventions were on a path to eventual success that needed more time to be realized.
System-level transformation interventions that sought to change practice-wide care delivery did not decrease costs among HNHC subgroups. These interventions may have been too distal or limited in intensity to effectively change HNHC patient behaviors. The lack of success in these larger-scope interventions reflects the challenges that stakeholders are likely to continue to face in implementing alternative payment models if required savings goals are contingent on changing HNHC patients’ healthcare services use.
Finally, the evidence was insufficient to reach a conclusion across all outcomes assessed for telephonic/mail and aICU-based interventions. Telephonic care management was shown previously to be unsuccessful among elderly patients with chronic diseases.71 Future studies assessing telemedicine may test whether adding video can facilitate HNHC patient-provider relationships to improve outcomes. While some authors propose using specialized clinics like aICU-based interventions for HNHC patients to provide individualized attention using multidisciplinary teams and high patient-staff ratios,72,73 the limited number of samples and insufficient evidence to reach conclusions suggest that additional studies are needed to determine if aICU interventions can improve care.
Our review highlights the dual need for evaluations to report a standard and larger set of outcomes. Few comparable outcomes were reported by multiple samples within an intervention category. Notably, health and social risk factor outcomes were rarely measured, despite the goal of many interventions of addressing these needs. While healthcare use and cost are key outcomes for healthcare systems, these measures do not necessarily reflect changes in patients’ experience in managing their health. Similarly, many interventions acknowledge that social risk factors can impact access to healthcare services and health; measuring changes in these outcomes may provide insights into their role in mediating clinical outcomes. Future research evaluating these outcomes may help us understand what interventions are accomplishing and why many have not achieved their ultimate healthcare use and cost goals.
Strengths and Limitations
This systematic review was strengthened by its ability to identify relevant studies through the inclusion of gray literature evaluations of federally funded interventions and a broad definition of HNHC patients. This review focused on the most rigorous evidence by only including samples with comparison groups. Many samples had large, representative sample sizes which increase the generalizability of findings for the US healthcare system. We also included a range of interventions, settings, and patients with various chronic conditions.
Our review has several limitations. First, findings were limited by both the small numbers and inconsistent reporting of outcomes across samples. Second, no standard definition of HNHC patients exists and samples varied considerably in their eligibility criteria. Thus, we cannot be sure if differences in success across samples were related to differences in sample populations. Third, system-level samples included in the meta-analysis measuring total cost had high heterogeneity (i.e., I2≥75%) and may reflect the variability and complexity among these interventions. Fourth, we grouped samples based on the intervention’s predominant service location/modality. SoE conclusions may be sensitive to these classifications. An alternative approach would be to group samples based on their key components (e.g., care management).3 However, interventions were complex and multi-faceted; study descriptions were often broad overviews of their multiple and overlapping components. We concluded that categorizing samples would be the most useful for stakeholders considering implementing interventions in particular settings.
Finally, an unachieved goal of the review was to distinguish changes in care that was potentially preventable or modifiable. Because of the focus on populations with high needs as well as high costs, some reductions in high-cost care will likely need to be replaced by ambulatory care. However, no studies defined or tracked changes in an individual patient’s preventable or modifiable care separately from unavoidable care. Also, no studies directly evaluated the success of interventions, shifting needed care from high-cost to lower-cost settings or reducing need through better management of chronic conditions.
Conclusions
We found limited evidence of effectiveness in relation to use and cost, particularly among ED- and primary care–based interventions. Intervention studies provided little information for determining why individual programs work, for whom, and within what contexts. Intermediate process outcomes and patient-centered experience outcomes may provide upstream results that can help explain and improve the likelihood of positive clinical and more distal policy outcomes.
Data Availability
The datasets generated during and analyzed during the current study are available from the corresponding author on reasonable request.
References
National Academy of Medicine. Effective care for high-need patients. Opportunities for improving outcomes, value, and health. National Academy of Sciences; 2017.
Figueroa JF, Joynt Maddox KE, Beaulieu N, Wild RC, Jha AK. Concentration of potentially preventable spending among high-cost Medicare subpopulations: an observational study. Ann Intern Med. 2017;167(10):706-713. https://doi.org/10.7326/m17-0767.
Bleich SN, Sherrod C, Chiang A, et al. Systematic review of programs treating high-need and high-cost people with multiple chronic diseases or disabilities in the United States, 2008-2014. Prev Chronic Dis. 2015;12:E197. https://doi.org/10.5888/pcd12.150275.
Moe J, Kirkland SW, Rawe E, et al. Effectiveness of interventions to decrease emergency department visits by adult frequent users: a systematic review. Acad Emerg Med. 2017;24(1):40-52. https://doi.org/10.1111/acem.13060.
Soril LJ, Leggett LE, Lorenzetti DL, Noseworthy TW, Clement FM. Reducing frequent visits to the emergency department: a systematic review of interventions. PLoS ONE. 2015;10(4):e0123660. https://doi.org/10.1371/journal.pone.0123660.
Althaus F, Paroz S, Hugli O, et al. Effectiveness of interventions targeting frequent users of emergency departments: a systematic review. Ann Emerg Med. 2011;58(1):41-52 e42. https://doi.org/10.1016/j.annemergmed.2011.03.007.
Iovan S, Lantz PM, Allan K, Abir M. Interventions to decrease use in prehospital and emergency care settings among super-utilizers in the United States: a systematic review. Med Care Res Rev. 2019:1077558719845722. https://doi.org/10.1177/1077558719845722.
Kumar GS, Klein R. Effectiveness of case management strategies in reducing emergency department visits in frequent user patient populations: a systematic review. J Emerg Med. 2013;44(3):717-729. https://doi.org/10.1016/j.jemermed.2012.08.035.
Di Mauro R, Di Silvio V, Bosco P, Laquintana D, Galazzi A. Case management programs in emergency department to reduce frequent user visits: a systematic review. Acta Biomed. 2019;90(6-s):34-40. https://doi.org/10.23750/abm.v90i6-S.8390.
Raven MC, Kushel M, Ko MJ, Penko J, Bindman AB. The effectiveness of emergency department visit reduction programs: a systematic review. Ann Emerg Med. 2016;68(4):467-483 e15. https://doi.org/10.1016/j.annemergmed.2016.04.015.
Goodwin A, Henschen BL, O’Dwyer LC, Nichols N, O’Leary KJ. Interventions for frequently hospitalized patients and their effect on outcomes: a systematic review. Review. J Hosp Med. 2018;13(12):853-859. https://doi.org/10.12788/jhm.3090.
Delaney RK, Sisco-Taylor B, Fagerlin A, Weir P, Ozanne EM. A systematic review of intensive outpatient care programs for high-need, high-cost patients. Review. Transl Behav Med. 2020;10(5):1187-1199. https://doi.org/10.1093/tbm/ibaa017.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. https://doi.org/10.1371/journal.pmed.1000097.
Jiang L, Berkman N, Porterfield DS, et al. HSRProj (Health Services Research Projects in Progress). https://hsrproject.nlm.nih.gov/view_hsrproj_record/20202652
Berkman ND, Chang E, Seibert J, et al. AHRQ Comparative Effectiveness Reviews. Management of High-Need, High-Cost Patients: A “Best Fit” Framework Synthesis, Realist Review, and Systematic Review. Agency for Healthcare Research and Quality (US); 2021.
Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898.
Sterne JA, Hernan MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919. https://doi.org/10.1136/bmj.i4919.
Bodenheimer T. Strategies to reduce costs and improve care for high-utilizing Medicaid patients: reflections on pioneering programs. Center for Health Care Strategies. October 2013.
Stata Meta-Analysis Reference Manual. Stata Press; 2021:344. https://www.stata.com/manuals/meta.pdf
Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924-6. https://doi.org/10.1136/bmj.39489.470347.AD.
Berkman ND, Lohr KN, Ansari MT, et al. Grading the strength of a body of evidence when assessing health care interventions: an EPC update. J Clin Epidemiol. 2015;68(11):1312-24. https://doi.org/10.1016/j.jclinepi.2014.11.023.
Berkman ND, Lohr KN, Ansari M, et al. Grading the strength of a body of evidence when assessing health care interventions for the effective health care program of the agency for healthcare research and quality: an update. 2013. AHRQ Publication No. 13(14)-EHC130-EF. November. www.effectivehealthcare.ahrq.gov/reports/final.cfm
Sledge WH, Brown KE, Levine JM, et al. A randomized trial of primary intensive care to reduce hospital admissions in patients with high utilization of inpatient services. Journal Article; Randomized Controlled Trial; Research Support, Non-U.S. Gov't. Dis Manag. 2006;9(6):328-338. https://doi.org/10.1089/dis.2006.9.328.
Finkelstein A, Zhou A, Taubman S, Doyle J. Health care hotspotting - a randomized, controlled trial. N Engl J Med. 2020;382(2):152-162. https://doi.org/10.1056/NEJMsa1906848.
Kelley L, Capp R, Carmona JF, et al. Patient navigation to reduce emergency department (ED) utilization among Medicaid insured, frequent ED users: a randomized controlled trial. Article. J Emerg Med. 2020;58(6):967-977. https://doi.org/10.1016/j.jemermed.2019.12.001.
Bell JF, Krupski A, Joesch JM, et al. A randomized controlled trial of intensive care management for disabled Medicaid beneficiaries with high health care costs. Health Serv Res. 2015;50(3):663-89. https://doi.org/10.1111/1475-6773.12258.
Dally DL, Dahar W, Scott A, Roblin D, Khoury AT. The impact of a health education program targeting patients with high visit rates in a managed care organization. Clinical Trial; Journal Article; Randomized Controlled Trial. Am J Health Promot. 2002;17(2):101-111. https://doi.org/10.4278/0890-1171-17.2.101.
Shumway M, Boccellari A, O'Brien K, Okin RL. Cost-effectiveness of clinical case management for ED frequent users: results of a randomized trial. Am J Emerg Med. 2008;26(2):155-64. https://doi.org/10.1016/j.ajem.2007.04.021.
Coleman EA, Eilertsen TB, Kramer AM, Magid DJ, Beck A, Conner D. Reducing emergency visits in older adults with chronic illness. A randomized, controlled trial of group visits. Eff Clin Pract. 2001;4(2):49-57.
Katzelnick DJ, Simon GE, Pearson SD, et al. Randomized trial of a depression management program in high utilizers of medical care. Arch Fam Med. 2000;9(4):345-351. https://doi.org/10.1001/archfami.9.4.345.
Yoon J, Chang E, Rubenstein LV, Zulman DM, Asch SM. Impact of primary care intensive management on high-risk veterans' costs and utilization. Ann Intern Med. 2018;169(7):515-516. https://doi.org/10.7326/l18-0461.
Zulman DM, Chang ET, Wong A, et al. Effects of intensive primary care on high-need patient experiences: survey findings from a Veterans Affairs randomized quality improvement trial. J Gen Intern Med. 2019;34(Suppl 1):75-81. https://doi.org/10.1007/s11606-019-04965-0.
McCall N, Cromwell J, Urato C, Eng T. Evaluation of Medicare Care Management for High Cost Beneficiaries (CMHCB) Demonstration: VillageHealth’s Key to Better Health (KTBH): final report. RTI International. Research Triangle Park, NC: 2010. https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Reports/downloads/McCall_KTBH_Final_2010.pdf
McCall N, Cromwell J, Urato C, Eng T. Evaluation of Medicare Care Management for High Cost Beneficiaries (CMHCB) Demonstration: Texas Senior Trails (TST): final report. RTI International. Research Triangle Park, NC: 2010. https://www.cms.gov/reports/downloads/CMHCB_TST_McCall_2010.pdf
McCall N, Cromwell J, Smith K, Urato C. Evaluation of Medicare Care Management for High Cost Beneficiaries (CMHCB) Demonstration: the Health Buddy® Consortium (HBC): revised final report. RTI International. Research Triangle Park, NC: 2011. https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Reports/downloads/mccall_eval_of_cmhcb_demo_april_2011.pdf
Urato C, McCall N, Cromwell J, Lenfestey N, Raeder D. Evaluation of the Extended Medicare Care Management for High Cost Beneficiaries (CMHCB) Demonstration: VillageHealth’s Key to Better Health (KTBH): final report. RTI International. Research Triangle Park, NC: 2013. https://innovation.cms.gov/files/reports/cmhcb-villagehealth.pdf
McCall N, Cromwell J, Urato C, Eng T. Evaluation of Medicare Care Management for High Cost Beneficiaries (CMHCB) Demonstration: Care Level Management (CLM). RTI International. Research Triangle Park, NC: 2010. https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Reports/downloads/CMHCB_CLM_McCall_2010.pdf
McCall N, Cromwell J, Urato C. Evaluation of Medicare Care Management for High Cost Beneficiaries (CMHCB) Demonstration: Massachusetts General Hospital and Massachusetts General Physician Organization (MGH): final report. RTI International. Research Triangle Park, NC: 2010.
Seaberg D, Elseroad S, Dumas M, et al. Patient navigation for patients frequently visiting the emergency department: a randomized, controlled trial. Acad Emerg Med. 2017;24(11):1327-1333. https://doi.org/10.1111/acem.13280.
Powers BW, Modarai F, Palakodeti S, et al. Impact of complex care management on spending and utilization for high-need, high-cost Medicaid patients. Am J Manag Care. 2020;26(2):e57-e63. https://doi.org/10.37765/ajmc.2020.42402.
Raven MC, Niedzwiecki MJ, Kushel M. A randomized trial of permanent supportive housing for chronically homeless persons with high use of publicly funded services. Health Serv Res. 2020;55 Suppl 2(Suppl 2):797-806. https://doi.org/10.1111/1475-6773.13553.
Lin MP, Blanchfield BB, Kakoza RM, et al. ED-based care coordination reduces costs for frequent ED users. Am J Manag Care. 2017;23(12):762-766.
Weerahandi H, Basso Lipani M, Kalman J, et al. Effects of a psychosocial transitional care model on hospitalizations and cost of care for high utilizers. Soc Work Health Care. 2015;54(6):485-498. https://doi.org/10.1080/00981389.2015.1040141.
Capp R, Misky GJ, Lindrooth RC, et al. Coordination program reduced acute care use and increased primary care visits among frequent emergency care users. Health Affairs. 2017;36(10):1705-1711. https://doi.org/10.1377/hlthaff.2017.0612.
Durfee J, Johnson T, Batal H, et al. The impact of tailored intervention services on charges and mortality for adult super-utilizers. Healthcare (Amsterdam, Netherlands). 2018;6(4):253-258. https://doi.org/10.1016/j.hjdsi.2017.08.004.
Peterson G, Blue L, Moreno L, et al. Evaluation of Health Care Innovation Awards (HCIA): Primary Care Redesign Programs: third annual report. Mathematica Policy Research. Princeton, NJ: 2017. https://downloads.cms.gov/files/cmmi/hcia-primarycareredesign-thirdannualrpt.pdf
Navratil-Strawn JL, Hawkins K, Wells TS, et al. An emergency room decision-support program that increased physician office visits, decreased emergency room visits, and saved money. Popul Health Manag. 2014;17(5):257-64. https://doi.org/10.1089/pop.2013.0117.
Schickedanz A, Sharp A, Hu YR, et al. Impact of social needs navigation on utilization among high utilizers in a large integrated health system: a quasi-experimental study. J Gen Intern Med. 2019;34(11):2382-2389. https://doi.org/10.1007/s11606-019-05123-2.
Sevak P, Stepanczuk CN, Bradley KWV, et al. Effects of a community-based care management model for super-utilizers. Am J Manag Care. 2018;24(11):e365-e370.
Vickery KD, Shippee ND, Menk J, et al. Integrated, accountable care for Medicaid expansion enrollees: a comparative evaluation of Hennepin Health. Article in Press. Med Care Res Rev. 2020; https://doi.org/10.1177/1077558718769481.
Sandberg SF, Erikson C, Owen R, et al. Hennepin Health: a safety-net accountable care organization for the expanded Medicaid population. Health Aff (Millwood). 2014;33(11):1975-84. https://doi.org/10.1377/hlthaff.2014.0648.
Kahn KL, Timbie JW, Friedberg MW, et al. Evaluation of CMS’s Federally Qualified Health Center (FQHC) Advanced Primary Care Practice (APCP) Demonstration: final report. RAND Corporation. Santa Monica, CA: 2017. https://www.rand.org/pubs/research_reports/RR886z2.html
Peikes D, Anglin G, Dale S, et al. Evaluation of the Comprehensive Primary Care initiative: fourth annual report. Mathematica Policy Research. Princeton, NJ: 2018. https://www.mathematica.org/publications/evaluation-of-the-comprehensive-primary-care-initiative-fourth-annual-report
Peikes D, Anglin G, Harrington M, et al. Independent evaluation of comprehensive primary care plus (CPC+) first annual report. Mathematica Policy Research. Princeton, NJ: 2019. https://www.mathematica.org/publications/independent-evaluation-of-comprehensive-primary-care-plus-cpc-first-annual-report
Anglin G, Peikes D, Petersen D, et al. Independent evaluation of comprehensive primary care plus (CPC+): second annual report. Mathematica Policy Research. Princeton, NJ: 2020. https://www.mathematica.org/publications/independent-evaluation-of-comprehensive-primary-care-plus-cpc-second-annual-report
Kimmey L, Anderson M, Cheh V, et al. Evaluation of the Independence at Home Demonstration: an examination of the first four years. Mathematica Policy Research. Princeton, NJ: 2019. https://www.mathematica.org/publications/evaluation-of-the-independence-at-home-demonstration-an-examination-of-the-first-four-years
Li E, Kimmey L, Cheh V. Evaluation of the independence at home demonstration: an examination of the first five years. Mathematica Policy Research. Princeton, NJ: 2020. https://innovation.cms.gov/files/reports/iah-yr5evalrpt.pdf
Harrison JM, Oganisian A, Grande DT, Mitra N, Chhabra M, Chaiyachati KH. Economic outcomes of insurer-led care management for high-cost medicaid patients. Article. Am J Manag Care. 2020;26(7):310-316. https://doi.org/10.37765/ajmc.2020.43769.
Crane S, Collins L, Hall J, Rochester D, Patch S. Reducing utilization by uninsured frequent users of the emergency department: combining case management and drop-in group medical appointments. J Am Board Fam Med. 2012;25(2):184-91. https://doi.org/10.3122/jabfm.2012.02.110156.
Shah R, Chen C, O'Rourke S, Lee M, Mohanty SA, Abraham J. Evaluation of care management for the uninsured. Med Care. 2011;49(2):166-71. https://doi.org/10.1097/MLR.0b013e3182028e81.
DeHaven M, Kitzman-Ulrich H, Gimpel N, et al. The effects of a community-based partnership, Project Access Dallas (PAD), on emergency department utilization and costs among the uninsured. J Public Health (Oxf). 2012;34(4):577-83. https://doi.org/10.1093/pubmed/fds027.
Gimpel N, Marcee A, Kennedy K, Walton J, Lee S, DeHaven MJ. Patient perceptions of a community-based care coordination system. Health Promot Pract. 2010;11(2):173-81. https://doi.org/10.1177/1524839908320360.
Adam P, Brandenburg DL, Bremer KL, Nordstrom DL. Effects of team care of frequent attenders on patients and physicians. Families, Systems & Health : the Journal of Collaborative Family Healthcare. 2010;28(3):247-57. https://doi.org/10.1037/a0020944.
Enard KR, Ganelin DM. Reducing preventable emergency department utilization and costs by using community health workers as patient navigators. J Healthc Manag. 2013;58(6):412-27; discussion 428.
Thompson MP, Podila PSB, Clay C, et al. Community navigators reduce hospital utilization in super-utilizers. Am J Manag Care. 2018;24(2):70-76.
Valluru G, Yudin J, Patterson CL, et al. Integrated home- and community-based services improve community survival among independence at home Medicare beneficiaries without increasing Medicaid costs. J Am Geriatr Soc. 2019;67(7):1495-1501. https://doi.org/10.1111/jgs.15968.
McCormack RP, Hoffman LF, Wall SP, Goldfrank LR. Resource-limited, collaborative pilot intervention for chronically homeless, alcohol-dependent frequent emergency department users. Am J Public Health. 2013;103 Suppl 2(Suppl 2):S221-4. https://doi.org/10.2105/ajph.2013.301373.
Horn BP, Crandall C, Moffett M, et al. The economic impact of intensive care management for high-cost medically complex patients: an evaluation of New Mexico's care one program. Popul Health Manag. 2016;19(6):398-404. https://doi.org/10.1089/pop.2015.0142.
NCQA. Hospitalization for potentially preventable complications (HPC). NCQA. Accessed August 26, 2020. https://www.ncqa.org/hedis/measures/hospitalization-for-potentially-preventable-complications/
Edwards ST, Peterson K, Chan B, Anderson J, Helfand M. Effectiveness of intensive primary care interventions: a systematic review. J Gen Intern Med. 2017;32(12):1377-1386. https://doi.org/10.1007/s11606-017-4174-z.
McCall N, Cromwell J. Results of the Medicare Health Support disease-management pilot program. N Engl J Med. 2011;365(18):1704-12. https://doi.org/10.1056/NEJMsa1011785.
Lewis J, Hoyt A, Kakoza RM. Enhancing quality of primary care using an ambulatory ICU to achieve a patient- centered medical home. J Prim Care Community Health. 2011;2(4):234-9. https://doi.org/10.1177/2150131911410063.
Hochman M, Asch SM. Disruptive models in primary care: caring for high-needs, High-Cost Populations. J Gen Intern Med. 2017;32(4):392-397. https://doi.org/10.1007/s11606-016-3945-2.
Funding
This work was funded under Contract No. HHSA-290-2015-00011-I from the Agency for Healthcare Research and Quality (AHRQ), U.S. Department of Health and Human Services (HHS). Investigators worked with AHRQ staff to develop the scope, analytic framework, and key questions for this review. AHRQ had no role in study selection, quality assessment, or synthesis. AHRQ staff provided project oversight, reviewed the report to ensure that the analysis met methodological standards, and distributed the draft for peer review. Otherwise, AHRQ had no role in the conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript findings. The authors of this paper are responsible for its content. Statements in the paper do not necessarily represent the official views of or imply endorsement by AHRQ or HHS.
Author information
Authors and Affiliations
Contributions
We gratefully acknowledge the following individuals for their contributions to this project: current or prior AHRQ staff, Christine Chang, MD, Elise Berliner, PhD; current or prior RTI International–University of North Carolina at Chapel Hill EPC staff, Sharon Barrell, MA, Christopher Beadles, PhD, Linda Jiang, BA, Loraine Monroe, BS, Deborah Porterfield, MD, Caroline Rains, MPH, Meera Viswanathan, Ph.D., Lynn Whitener, DrPH., Roberta C. Wines, MPH, and Carol Woodell, BSPH.
Corresponding author
Ethics declarations
Conflicts of Interest
The authors declare that they do not have a conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM 1
(DOCX 528 kb)
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Chang, E., Ali, R., Seibert, J. et al. Interventions to Improve Outcomes for High-Need, High-Cost Patients: A Systematic Review and Meta-Analysis. J GEN INTERN MED 38, 185–194 (2023). https://doi.org/10.1007/s11606-022-07809-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-022-07809-6