
Abstract
Background
Care coordination (CC) interventions involve systematic strategies to address fragmentation and enhance continuity of care. However, it remains unclear whether CC can sufficiently address patient needs and improve outcomes.
Methods
We searched MEDLINE, CINAHL, Embase, Cochrane Database of Systematic Reviews, AHRQ Evidence-based Practice Center, and VA Evidence Synthesis Program, from inception to September 2019. Two individuals reviewed eligibility and rated quality using modified AMSTAR 2. Eligible systematic reviews (SR) examined diverse CC interventions for community-dwelling adults with ambulatory care sensitive conditions and/or at higher risk for acute care. From eligible SR and relevant included primary studies, we abstracted the following: study and intervention characteristics; target population(s); effects on hospitalizations, emergency department (ED) visits, and/or patient experience; setting characteristics; and tools and approaches used. We also conducted semi-structured interviews with individuals who implemented CC interventions.
Results
Of 2324 unique citations, 16 SR were eligible; 14 examined case management or transitional care interventions; and 2 evaluated intensive primary care models. Two SR highlighted selection for specific risk factors as important for effectiveness; one of these also indicated high intensity (e.g., more patient contacts) and/or multidisciplinary plans were key. Most SR found inconsistent effects on reducing hospitalizations or ED visits; few reported on patient experience. Effective interventions were implemented in multiple settings, including rural community hospitals, academic medical centers (in urban settings), and public hospitals serving largely poor, uninsured populations. Primary studies reported variable approaches to improve patient-provider communication, including health coaching and role-playing. SR, primary studies, and key informant interviews did not identify tools for measuring patient trust or care team integration. Sustainability of CC interventions varied and some were adapted over time.
Discussion
CC interventions have inconsistent effects on reducing hospitalizations and ED visits. Future work should address how they should be adapted to different healthcare settings and which tools or approaches are most helpful for implementation.
Trial Registration
PROSPERO #CRD42020156359
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
INTRODUCTION
Complexity of healthcare services and care fragmentation contribute to adverse health outcomes and poor patient experiences.1–4 To help address fragmentation of health services, the Center for Medicare and Medicaid Innovation (CMMI) has undertaken several demonstration projects evaluating new payment models to incentivize integration of services across the continuum of care.5, 6 Over the past 20 years, there has also been substantial interest in care coordination interventions to address fragmentation, particularly aimed at reducing utilization of acute care services (i.e., hospital admissions and emergency department [ED] visits).7, 8 Care coordination models usually involve systematic strategies to improve continuity and bridge transitions of care.7, 9, 10 These often take the form of care or case management, whereby a designated person or team helps patients manage their medical care and navigate interactions with healthcare system(s). These interventions are frequently targeted at populations thought to be at higher risk for acute care utilization, determined using variable criteria.7, 8 While a variety of care coordination models have been studied across diverse settings, it remains unclear whether these interventions can sufficiently address gaps in care and improve patient outcomes. Additionally, for those considering implementation of care coordination models, there is a need to better understand the evidence for tools and approaches used to assist with and monitor implementation progress.
In support of ongoing efforts to standardize and integrate care coordination services across Veterans Health Administration (VHA) facilities,11 the VA Evidence Synthesis Program (ESP) was asked to review evidence on implementation and outcomes of care coordination models for community-dwelling adults at high risk for acute care use.12 This multi-staged evidence report included a systematic review of reviews,13 examination of primary research studies included by eligible reviews, and key informant interviews. We first present qualitative summaries of results from eligible systematic reviews on key characteristics and effectiveness of care coordination interventions. Then, we describe results from primary research studies of effective interventions (i.e., those able to reduce hospitalizations and/or ED visits) regarding settings, and tools and approaches to assess patient trust and care team integration and to improve patient-provider communications. Finally, we provide results from key informant interviews to address remaining gaps in the published literature, particularly with regard to tools and approaches used by various interventions. We also discuss gaps and limitations in the evidence base, and offer recommendations for future research and policy.
METHODS
Conceptual Model and Scope
Collaboratively with our stakeholders (VA Offices of Nursing Services, and Care Management and Social Work) and expert advisory panel, we selected the framework for Care Coordination in Chronic and Complex Disease Management10(Table 1) to guide scope refinement and protocol development. We examined multiple resources and other existing models for care coordination (e.g., AHRQ Care Coordination Atlas7 and Integrated Team Effectiveness Model14). We chose this particular framework because it delineates specific, potentially measurable concepts within larger domains that largely follow the classic structure-process-outcome model for quality of health care.15 Additionally, this framework delineated relevant concepts within and between healthcare teams; our stakeholders indicated that communications and mechanisms between teams were key issues for VHA programs. We further adapted the selected framework by: (1) specifying that within coordination mechanisms, team roles include who contacted patients (and in what manner); and (2) reorganizing outcomes into those relevant for patients (e.g., patient experience, quality of life, and survival), healthcare teams (e.g., work satisfaction and burnout), and health systems (e.g., acute care utilization) (Table 1). While healthcare utilization may be measured at the patient level (e.g., number of admissions per person), we considered such outcomes to be oriented towards priorities of healthcare systems rather than patients.
Applying this framework, and in accordance with stakeholder priorities, we defined effective interventions as those that reduced hospitalizations and/or ED visits. We sought information on key characteristics of effective interventions, particularly with regard to elements depicted in Context and Setting, and Coordinating Mechanisms. Examples of such characteristics include multidisciplinary teams (vs. primarily single case manager) and home visits (vs. telephone contacts and/or outpatient visits). We also searched for evidence on tools and approaches that were used to assess Emergent Integrating Conditions (e.g., trust within teams) and Coordinating Actions (e.g., within team communication); our stakeholders identified that these tools were as important for monitoring implementation progress of VHA programs before other outcomes may be available. Finally, to better understand the applicability of results, we sought information on characteristics of healthcare systems and communities where effective interventions had been implemented.
Key Questions (KQ)
For community-dwelling adults with a variety of ambulatory care sensitive conditions and/or at higher risk of having repeat hospitalization or ED visits:
-
KQ1—What are the key characteristics of care coordination models (of varying types) that aim to reduce hospitalization or ED visits?
-
KQ2—What is the effect of implementing these care coordination models on hospitalizations, ED visits, and patient experience (e.g., Consumer Assessment of Healthcare Providers and Systems)?
-
KQ3—What are the characteristics of settings in which effective models have been implemented?
-
KQ4—Among effective models, which approaches/tools have been used to:
-
Measure patient trust or working alliance?
-
Measure team integration?
-
Improve communication between patients and providers?
-
Search Strategy
We first focused on identifying eligible systematic reviews that examined a variety of care coordination models. We searched for English-language systematic reviews, from inception until September 2019, in the following: MEDLINE, CINAHL, Embase, Cochrane Database of Systematic Reviews, AHRQ Evidence-based Practice Center, and VA ESP reports. Search terms included MeSH and free text for care coordination interventions (e.g., care or case management, interdisciplinary care, and intensive primary care) and systematic reviews (Appendix 1 in the supplementary material).
Based on our experience with published evidence on care coordination and information reported by systematic reviews, we anticipated that eligible reviews may not provide sufficient information, particularly regarding characteristics of settings and tools and approaches used (KQ 3 and 4). Therefore, we planned a priori to undertake the following additional steps: (1) examination of primary research studies included by eligible reviews; (2) updated search for relevant randomized controlled trials (RCT) of care coordination interventions in MEDLINE and Embase (from year of most recent eligible review until February 2020) (Appendix 1 in the supplementary material); and (3) key informant interviews with team members who implemented interventions described in primary research studies (see below).
Screening and Selection
Using prespecified criteria (Appendix 2 in the supplementary material), systematic review search results were evaluated and excluded with the consensus of 2 individuals. Eligible populations included community-dwelling adults with a range of ambulatory care sensitive conditions (per AHRQ quality metrics), including conditions like heart failure and chronic lung disease16and/or at higher risk for acute care episodes (as defined by authors of review and/or primary studies). If a review focused exclusively on a single health condition, it was excluded. Eligible interventions covered diverse models, including care or case management and home-based primary care. Eligible reviews included hospitalizations and/or ED visits as outcomes of interest in objectives or results. At full-text review, two individuals separately determined inclusion and resolved conflicts through discussion.
From each eligible review, we also identified all included primary studies and 2 individuals evaluated them for potential relevance to KQ 3–4. As noted above, relevant studies for KQ 3 reported effective care coordination models that reduced acute care visits; if a model was only shown to improve patient experience, it was not considered applicable to KQ 3. In addition to the criteria described above, we also applied the following: conducted in the USA, and RCT or quasi-experimental observational studies (e.g., comparative control cohort or interrupted time series).17 We similarly screened and reviewed results from the additional search of RCT published 2018 to February 2020.
Data Abstraction and Quality Assessment
We assessed quality using criteria adapted from AMSTAR 2,18 rating overall quality as high, medium, or low (Appendix 3 in the supplementary material). We also noted if review authors evaluated for small studies and reporting outcome biases. From all eligible reviews, we abstracted the following: target populations (e.g., frequent utilizers of ED or those with complex chronic conditions); dates of search queries; and number and characteristics of included primary research studies (location, setting, and study design). From high- and medium-quality reviews, we planned to abstract detailed information on the following: characteristics of care coordination models; pooled effects or qualitative summaries of results on hospitalizations, ED visits, and/or patient experience; setting characteristics; and tools and approaches used to measure patient trust or working alliance, assess healthcare team integration, and/or improve patient-provider communications.
From relevant primary studies reporting successful reductions in hospitalizations and/or ED visits, we abstracted the following: effects on main outcomes; participant, intervention, and setting characteristics; and relevant tools and approaches. We also examined associated studies referenced by primary studies for intervention characteristics.
Data Synthesis
Due to heterogeneity of eligible reviews and studies, we undertook qualitative synthesis focusing on key characteristics and effectiveness of care coordination models. If reported, we abstracted strength of evidence determinations by review authors. For primary studies reporting effective interventions, we summarized setting and intervention characteristics; effects on main outcomes; and tools and approaches.
Key Informant Interviews
We conducted semi-structured interviews with researchers and team members who implemented care coordination models, as described in relevant primary studies (regardless of intervention effectiveness). We invited 25 individuals and completed interviews with 11 participants.
The main focus of interviews was to address gaps in published studies regarding intervention tools and approaches (KQ4). We also included questions on intervention uptake and sustainability. A general version of the interview guide is provided in Appendix 4 in the supplementary material; individual guides were adapted using published and online information. Interviews lasted about 30 min and were audio-recorded. We reviewed contemporaneous notes and audio-recordings to develop summaries for each intervention. We then examined all interview summaries to generate key takeaways across major topics.
RESULTS
Overview of Eligible Systematic Reviews
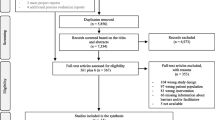
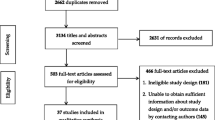
We screened 2,324 unique citations, reviewed 72 full texts, and identified 16 eligible systematic reviews (Figure 1). Fourteen reviews examined case management or transitional care interventions,19–32 and 2 evaluated intensive primary care models (e.g., home-based primary care)33, 34; all reviews included a variety of models within these broad categories. Four reviews included only RCT,19, 25, 26, 31 while others allowed observational studies. Most reviews included studies from different countries, but 3 were limited to US studies.20, 24, 28 Seven reviews focused on patients at higher risk for acute care utilization (i.e., high utilizers),19, 22–24, 27, 28, 30 and one examined interventions for frail adults.31 Six reviews were high quality,23, 26, 27, 29, 30, 34 6 were medium,19, 22, 24, 25, 31, 33 and 4 were low20, 21, 28, 32 (Appendix 3 in the supplementary material). Overall, 8 reviews evaluated selective outcomes reporting bias (7 high and medium quality); of 3 reviews that conducted quantitative meta-analyses, 2 used funnel plots to assess for publication bias (Appendix 3 in the supplementary material). We focused on high- and medium-quality reviews for detailed results, as described below and in Appendix 5 in the supplementary material.

Search and selection for eligible systematic reviews. AHRQ EPC, Agency for Healthcare Research and Quality Evidence-based Practice Centers; VA ESP, Department of Veterans Affairs Evidence Synthesis Program.
Primary research studies included by all eligible reviews were examined for relevance (see METHODS). Among 272 unique primary studies, we identified 16 RCT35–50 and 9 observational studies51–59 that evaluated relevant interventions conducted in the USA. Most studies were included by 1–2 eligible reviews, but 7 studies36, 38, 42, 48, 52, 57 were included by 3 or more reviews (Appendix 6 in the supplementary material). The updated search for RCT (published in 2018 or later) identified 1048 unique citations. We reviewed 21 full texts, finding 2 more relevant RCT; both reported interventions were not effective for reducing hospitalizations and/or ED visits.60, 61 Overall, 20% of relevant RCT (4 of 20)38, 43, 46, 49 showed reductions in hospitalizations and/or ED visits. In contrast, 78% of relevant observational studies (7 of 9)51, 52–55, 57, 58 reported effectiveness for these outcomes.
KQ1: What Are the Key Characteristics of Care Coordination Models?
All reviews summarized different components included by interventions, with variation in team composition and components (e.g., multidisciplinary care plan). Communication with patients was mainly in person (in a clinical setting or at home) or via telephone. Four reviews specifically addressed key characteristics for care coordination models23, 29, 31, 34; all included primary studies conducted in and outside of the USA (e.g., Canada, European countries, and Australia). Among these, Hudon et al.23 used qualitative comparative analysis to examine characteristics of effective case management models, finding that careful participant selection was necessary but not sufficient; additional required elements were high intensity (defined using caseload, frequency, and types of patient contacts) or a multidisciplinary care plan. Smith et al.29 also conducted a qualitative synthesis, reporting that interventions targeting specific risk factors were more likely to be effective. In contrast, Van der Elst et al.31 conducted quantitative subgroup analyses by intervention duration and different approaches to address frailty, finding no significant differences in effect. Finally, Totten et al.34 examined home-based primary care interventions and, using qualitative synthesis, found no specific pattern of components were associated with effectiveness. Additionally, 2 reviews19, 33 sought to determine key components but were unable to draw conclusions; challenges included lack of published information describing components and implementation fidelity.
KQ2: What Is the Effect of Implementing Care Coordination Models?
Effects of care coordination interventions on hospitalizations, ED visits, and patient experience are summarized in Figure 2 and described in detail in Appendix 5 in the supplementary material. Of 12 high- and medium-quality reviews, most used qualitative synthesis, and most found unclear or mixed effects across the different outcomes (Figure 2).

Summary results from eligible high- and medium-quality systematic reviews—effects of care coordination interventions on hospitalizations, emergency department visits, and patient experience.
Case Management and Transitional Care Interventions
Of 10 reviews examining case management or transitional care interventions, 6 evaluated effectiveness for reducing hospitalizations, with 4 reporting mixed or unclear results19, 23, 25, 26 and 2 finding lack of effectiveness29, 31(Figure 2 and Appendix 5 in the supplementary material). Populations addressed by these reviews included high utilizers,19, 23 those with chronic disease or multimorbidity,25, 26, 29 and frail older adults.31 Le Berre et al.26 evaluated transitional care interventions using quantitative meta-analyses; incorporating data from 11 to 35 RCT across different follow-up periods, there was no effect at 1 month (risk difference [RD] −0.03 [−0.05, 0]) but some reduction at 3–18 months (RD range −0.05 to−0.11) (Appendix 5 in the supplementary material). Van der Elst et al.31 conducted quantitative meta-analyses to evaluate diverse case management interventions for frail community-dwelling older adults; pooled results from 5 RCT showed no reduction in hospitalizations (odds ratio [OR] 1.13, 95% confidence interval [CI] 0.95, 1.35) (Appendix 5 in the supplementary material).
Seven reviews examined effects on ED visits, with only 2 indicating that care coordination reduced ED visits.25, 27 Joo et al.25 focused on adults with chronic disease and described 6 studies that showed reductions in ED visits. Moe et al.27 addressed results for high utilizers and reported that the median rate ratio (of care coordination vs. control) was 0.63, with an interquartile range of 0.41–0.71. Le Berre et al.26 also examined care coordination for high utilizers, and reported pooled meta-analyses showing a reduction at 3 months (RD −0.08 [−0.15, −0.01]) but no differences at 1, 6, and 12 months. All 4 remaining reviews22–24, 30 evaluated results for high utilizers, used qualitative synthesis and reported unclear or mixed effects on ED visits (Figure 2 and Appendix 5 in the supplementary material).
One review addressed effects on patient experience and, using qualitative synthesis, found inconsistent results.23
Intensive Primary Care Interventions
Two reviews evaluated intensive primary care interventions, and both used qualitative synthesis. Totten et al.34 focused on home-based primary care for adults with chronic illness and/or disabilities, reporting reduced hospitalizations (moderate strength of evidence) and ED visits (low strength of evidence), along with higher patient and caregiver satisfaction (low strength of evidence) (Figure 2 and Appendix 5 in the supplementary material). In contrast, Edwards et al.33 addressed several different models of intensive primary care for those at high risk for hospital admission and/or death, finding inconsistent results across studies.
KQ3: What Are the Characteristics of Settings in Which Effective Models Have Been Implemented?
Few reviews addressed specific setting characteristics, outside of countries of studies. Soril et al.30 examined case management models and reported that 15 of 16 included studies were single site, usually in an urban setting. Totten et al.34 sought to address organizational settings for home-based primary care but were unable to find published information.
To better understand setting characteristics, we also examined 11 relevant primary studies reporting effective interventions in the USA. We categorized these interventions as transitional care (n=5),37, 43, 51, 53, 54 outpatient care or case management (led by nurse or social worker) (n=4),46, 48, 57, 58 or other intensive primary care models (n=2)52, 55(Table 2). Settings were diverse, including rural community hospitals, academic medical centers (in urban settings), and public hospitals serving largely poor and uninsured populations. Detailed intervention characteristics and effects are also presented in Table 2. There was no clear connection between differences in settings, types of intervention, and various patient populations.
KQ4: What Are Tools and Approaches Used by Effective Models?
No review commented on tools and approaches used to measure patient trust or care team integration, or to improve patient-provider communication. Among relevant primary studies, 5 described various approaches to improve patient-provider communications, such as coaching patients, making lists of key concerns, and role-playing.38, 46, 53, 57, 62 In 2 studies, care coordinators also attended outpatient visits with patients and their providers.46, 57 No study described specific measures to assess patient trust or care team integration. We identified an accompanying article for one study38 that described results from qualitative interviews to evaluate patient experiences and relationship with care coordinators.45
Key Informant Interviews
Main takeaways from interviews and selected supporting quotes are presented in Table 3. We did not identify any additional tools or approaches to assess patient trust or care team integration, or to improve patient-provider communications. Additional materials provided by interviewees indicated that sometimes, assessments of patient experience included factors conceptually related to patient trust (e.g., perception that care coordinator was knowledgeable and understood patients’ needs).
Overall, several elements were noted to work well: multidisciplinary collaboration; dedicated staff for intervention (e.g., who contacted providers and patients); relationships with community organizations and services; and staff dedication, compassion, and ability to establish relationships with relevant actors (Table 3). There was variation in sustainability of interventions, with some stopping after completion of research studies. Challenges encountered by interventions (and successfully addressed by some) included the following: need to meet readmission metrics; adaptation to changing health system priorities; and achieving buy-in and ownership (e.g., of staffing costs) from key health system stakeholders (Table 3).
For future interventions, some suggested that interventions may work better for patients with less severe conditions and/or modifiable factors; an important challenge with such an approach is that interventions may need to serve a larger number of patients before there are appreciable differences in acute care utilization. One individual stated, “You can allocate a lot of resources to extremely high need patients…or you can allocate resources to a larger population and … have a smaller impact on individual level, but on population level have greater impact…”
DISCUSSION
We conducted a multi-staged evidence review and key informant interviews to evaluate care coordination interventions. Interventions were complex and differed along multiple dimensions, presenting substantial challenges in comparing and summarizing the evidence. Most reviews reported unclear or inconsistent effects in reducing hospitalizations or ED visits. Two reviews drew conclusions about key characteristics; both highlighted the importance of selection criteria focused on clear risk factors and/or needs. One of these further indicated the requirement for a high-intensity model (defined by lower caseload and more patient contacts) or use of multidisciplinary plans.
Among 11 primary studies demonstrating effective interventions, none reported specific tools or approaches for measuring patient trust or healthcare team integration. Approaches used to improve patient-provider communication included coaching and role-playing. In some interventions, care coordinators directly communicated with providers on patients’ behalf, including participation at clinic appointments. Key informants highlighted multiple challenges to implementation and sustainability of interventions, including difficulty with impacting short-term readmission metrics, adapting to changing health system priorities, and stakeholder engagement.
Among multiple factors contributing to healthcare fragmentation in the USA, foremost are complex payment policies and a regulatory environment that present substantial barriers to service integration.63, 64 These factors make it financially challenging for healthcare entities to invest in programs aiming to improve long-term health outcomes. Existing barriers also limit the potential impact of care coordination interventions, which must work to patch ongoing gaps in care and manage misaligned incentives among various providers. CMMI demonstration projects are testing several new payment models to incentivize restructuring of healthcare delivery, including bundled payments to promote integration of care across settings for certain indications,5 and establish patient-centered medical homes in outpatient care.6 Results from these demonstrations may lead to longer-term policy changes that will support greater integration of US healthcare services.
Evidence Gaps and Future Research
Primary research studies using observational designs were more likely to report reductions in hospitalizations and/or ED visits. Observational studies may have residual confounding, be more affected by selective outcomes and publication bias, and are susceptible to false-positive results from regression to the mean (particularly for pre-post cohort designs). Also, there was very limited evidence for intensive primary care models; the 2 eligible reviews on these models included a total of 4 relevant primary studies.40, 50, 55, 56
Additionally, studies did not report standardized tools used to assess patient trust or care team integration. Key informant interviews revealed that some assessments of patient experience included concepts closely related to patient trust, but interviews did not identify any measures of care team integration. Gaps in our knowledge about tools to reliably assess these important aspects of patient coordinator and health team relationships may reflect the general focus of many care coordination studies on impacting acute care utilization; there may have been relatively less attention on verifying successful implementation as demonstrated by improvements in communication and relationships. Lack of standardized and validated tools to assess these aspects may hinder evaluation of existing services and implementation of new programs.
Finally, multiple reviews found a lack of information on intervention implementation and fidelity. To improve evaluation and interpretation of effectiveness, future studies should consider application of frameworks and designs that address implementation outcomes (e.g., hybrid effectiveness implementation designs, Consolidated Framework for Implementation Research [CFIR], and Reach, Effectiveness, Adoption, Implementation, and Maintenance [RE-AIM]).65–68 Studies should clearly define the “core” set of key components and the “adaptable periphery” of elements that can be adjusted to accommodate the local context.66
Therefore, we recommend the following:
-
Evaluate future care coordination interventions using randomized designs
-
Develop and apply standardized tools to assess patient trust or working alliance, healthcare team integration, and communication between patients and providers
-
Consider study designs that explicitly consider implementation outcomes in future studies of care coordination models
-
Define “core” intervention components and describe local adaptations, particularly in multisite studies
Implications for Policy and Practice
It remains unclear whether specific care coordination models should be implemented and how adaptations may improve effectiveness and sustainability. Current VHA initiatives have piloted new tools for evaluating patient needs and matching the level of care coordination services.11 It will be important to evaluate feasibility of wider implementation and downstream effects on service delivery and patient outcomes. Additionally, it will be important to understand differences in utility across large and small medical centers and clinics, and those located in urban and more rural communities. These evaluations may also be informative for non-VHA health systems seeking better tools to match services to patient needs. As local adaptations were noted to be important for uptake and sustainability, it may also be valuable to develop materials and resources to guide adaptations. Such guidance must necessarily depend on further work to better understand the rationale and impacts of various adaptations in different settings.
As noted above, fragmentation of healthcare services in the USA is unlikely to improve without substantial policy changes to better align incentives and remove regulatory hurdles. Our results suggest that high intensity and multidisciplinary care are needed for effective interventions, and these care coordination models are likely to incur higher costs and potentially more regulatory burden in the current environment. Thus, longer-term investments to implement such models, and improve patient outcomes, are likely not feasible until substantial changes in policy have occurred.
Finally, there may be specific patient populations that require care models beyond additional care coordination services (e.g., by a nurse and/or social worker). For example, VHA has implemented a collaborative model of collocated primary care and mental health, to improve access to mental health services.69 Another collaborative (often collocated) model involves longitudinal integration of oncology and palliative care for cancer patients.70 Notably, these care models target specific needs that are prevalent among the relevant populations, and for which there are clearly effective treatments.
Limitations
To address our VA stakeholder priorities, we focused on interventions effective in reducing hospitalizations and/or ED visits; reviews and studies not addressing these outcomes were excluded. While we acknowledge the importance of patient experience, our stakeholders and key informant interviews all indicated that impacting acute care utilization was often the top priority for health system leadership, and particularly important for sustainability. Because interventions occurring outside the USA may be less informative, due to substantial differences in healthcare financing and delivery, we limited relevant primary studies to those conducted in the USA. We completed interviews with less than half of those whom we invited; it is possible there was unpublished information on tools and approaches that we did not identify. Finally, we relied on determinations of overall effectiveness and strength of evidence from high- and medium-quality systematic reviews; thus, methodological concerns with the conduct of these reviews would affect the validity of our results.
CONCLUSIONS
Existing evidence on care coordination interventions indicates inconsistent effects on reducing hospitalizations and/or ED visits for high-risk community-dwelling adults. It remains unclear whether such interventions should be implemented and how they may be adapted to different healthcare settings. Implementation of new care coordination models should be carefully evaluated using randomized designs. Policymakers should also consider whether a larger scale redesign of healthcare services may be necessary to improve continuity and collaboration for certain patient populations.
References
Coleman EA, Berenson RA. Lost in transition: challenges and opportunities for improving the quality of transitional care. Ann Intern Med. 2004;141(7):533-6. doi:https://doi.org/10.7326/0003-4819-141-7-200410050-00009
Gadbois EA, Tyler DA, Shield R, McHugh J, Winblad U, Teno JM, et al. Lost in Transition: a Qualitative Study of Patients Discharged from Hospital to Skilled Nursing Facility. J Gen Intern Med. 2019;34(1):102-9. doi:https://doi.org/10.1007/s11606-018-4695-0
Harrison A, Verhoef M. Understanding coordination of care from the consumer’s perspective in a regional health system. Health Serv Res. 2002;37(4):1031-54. doi:https://doi.org/10.1034/j.1600-0560.2002.64.x
Montgomery JE, Irish JT, Wilson IB, Chang H, Li AC, Rogers WH, et al. Primary care experiences of medicare beneficiaries, 1998 to 2000. J Gen Intern Med. 2004;19(10):991-8. doi:https://doi.org/10.1111/j.1525-1497.2004.30381.x
Centers for Medicare and Medicaid Services. Bundled Payments for Care Improvement (BPCI) Initiative: General Information. 2021. https://innovation.cms.gov/innovation-models/bundled-payments. Accessed 08/10/21.
Centers for Medicare and Medicaid Services. Comprehensive Primary Care Plus. 2021. https://innovation.cms.gov/innovation-models/comprehensive-primary-care-plus. Accessed 08/10/21.
MacDonald K, Schultz E, Albin L, Pineda N, Lonhart J, Sundaram V, et al. Care Coordination Atlas Version 4 (AHRQ Publication No. 14-0037-EF). Rockville, MD: Agency for Healthcare Research and Quality, 2014.
Shojania KG, Wachter RM, Owens DK, Ranji SR, Shetty K, Posley KA, et al. Closing the quality gap: a critical analysis of quality improvement strategies. Care Coordination. 2007;7.
Peterson K, Anderson J, Bourne D, Boundy E. Scoping Brief: Care Coordination Theoretical Models and Frameworks: VA ESP Project #09-199. 2018.
Weaver SJ, Che XX, Petersen LA, Hysong SJ. Unpacking Care Coordination Through a Multiteam System Lens: A Conceptual Framework and Systematic Review. Med Care. 2018;56(3):247-59. https://doi.org/10.1097/MLR.0000000000000874
Greenstone CL, Peppiatt J, Cunningham K, Hosenfeld C, Lucatorto M, Rubin M, et al. Standardizing Care Coordination Within the Department of Veterans Affairs. J Gen Intern Med. 2019;34(Suppl 1):4-6. doi:https://doi.org/10.1007/s11606-019-04997-6
Duan-Porter W UK, Majeski B, Miake-Lye I, Diem S, Wilt TJ. Evidence review: care coordination models and tools. VA ESP Project #09-009. 2020.
Smith V, Devane D, Begley CM, Clarke M. Methodology in conducting a systematic review of systematic reviews of healthcare interventions. BMC Med Res Methodol. 2011;11(1):15. doi:https://doi.org/10.1186/1471-2288-11-15
Lemieux-Charles L, McGuire WL. What do we know about health care team effectiveness? A review of the literature. Med Care Res Rev. 2006;63(3):263-300. doi:https://doi.org/10.1177/1077558706287003
Donabedian A. Evaluating the quality of medical care. 1966. Milbank Q. 2005;83(4):691-729. doi:https://doi.org/10.1111/j.1468-0009.2005.00397.x
AHRQ Quality Indicators. Guide to Prevention Quality Indicators: Hospital Admission for Ambulatory Care Sensitive Conditions (AHRQ Pub. No. 02-R0203). Rockville, MD: Agency for Healthcare Research and Quality, 2001.
Rockers PC, Rottingen JA, Shemilt I, Tugwell P, Barnighausen T. Inclusion of quasi-experimental studies in systematic reviews of health systems research. Health Policy. 2015;119(4):511-21. doi:https://doi.org/10.1016/j.healthpol.2014.10.006
Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. Bmj. 2017;358:j4008.
Baker JM, Grant RW, Gopalan A. A systematic review of care management interventions targeting multimorbidity and high care utilization. BMC Health Serv Res. 2018;18(1):65. doi:https://doi.org/10.1186/s12913-018-2881-8
Bleich SN, Sherrod C, Chiang A, Boyd C, Wolff J, DuGoff E, et al. Systematic Review of Programs Treating High-Need and High-Cost People With Multiple Chronic Diseases or Disabilities in the United States, 2008-2014. Prev Chronic Dis. 2015;12:E197. doi:https://doi.org/10.5888/pcd12.150275
De Pourcq K, Meijboom B, Trybou J, Mortier E, Eeckloo K. The role of hospitals in bridging the care continuum: a systematic review of coordination of care and follow-up for adults with chronic conditions. BMC Health Serv Res. 2017;17(1):550.
Di Mauro R, Di Silvio V, Bosco P, Laquintana D, Galazzi A. Case management programs in emergency department to reduce frequent user visits: a systematic review. Acta Biomed. 2019;90(6-S):34-40. doi:https://doi.org/10.23750/abm.v90i6-S.8390
Hudon C, Chouinard MC, Pluye P, El Sherif R, Bush PL, Rihoux B, et al. Characteristics of Case Management in Primary Care Associated With Positive Outcomes for Frequent Users of Health Care: A Systematic Review. Ann Fam Med. 2019;17(5):448-58. doi:https://doi.org/10.1370/afm.2419
Iovan S, Lantz PM, Allan K, Abir M. Interventions to Decrease Use in Prehospital and Emergency Care Settings Among Super-Utilizers in the United States: A Systematic Review. Med Care Res Rev. 2020;77(2):99-111. doi:https://doi.org/10.1177/1077558719845722
Joo JY, Liu MF. Case management effectiveness in reducing hospital use: a systematic review. Int Nurs Rev. 2017;64(2):296-308. doi:https://doi.org/10.1111/inr.12335
Le Berre M, Maimon G, Sourial N, Gueriton M, Vedel I. Impact of Transitional Care Services for Chronically Ill Older Patients: A Systematic Evidence Review. J Am Geriatr Soc. 2017;65(7):1597-608. doi:https://doi.org/10.1111/jgs.14828
Moe J, Kirkland SW, Rawe E, Ospina MB, Vandermeer B, Campbell S, et al. Effectiveness of Interventions to Decrease Emergency Department Visits by Adult Frequent Users: A Systematic Review. Acad Emerg Med. 2017;24(1):40-52. doi:https://doi.org/10.1111/acem.13060
Raven MC, Kushel M, Ko MJ, Penko J, Bindman AB. The Effectiveness of Emergency Department Visit Reduction Programs: A Systematic Review. Ann Emerg Med. 2016;68(4):467-83 e15. doi:https://doi.org/10.1016/j.annemergmed.2016.04.015
Smith SM, Wallace E, O’Dowd T, Fortin M. Interventions for improving outcomes in patients with multimorbidity in primary care and community settings. Cochrane Database Syst Rev. 2016;3:CD006560. doi:https://doi.org/10.1002/14651858.CD006560.pub3
Soril LJ, Leggett LE, Lorenzetti DL, Noseworthy TW, Clement FM. Reducing frequent visits to the emergency department: a systematic review of interventions. PLoS ONE. 2015;10(4):e0123660. doi:https://doi.org/10.1371/journal.pone.0123660
Van der Elst M, Schoenmakers B, Duppen D, Lambotte D, Fret B, Vaes B, et al. Interventions for frail community-dwelling older adults have no significant effect on adverse outcomes: a systematic review and meta-analysis. BMC geriatr. 2018;18(1):249. doi:https://doi.org/10.1186/s12877-018-0936-7
Weeks LE, Macdonald M, Martin-Misener R, Helwig M, Bishop A, Iduye DF, et al. The impact of transitional care programs on health services utilization in community-dwelling older adults: a systematic review. JBI Database System Rev Implement Rep. 2018;16(2):345-84. https://doi.org/10.11124/JBISRIR-2017-003486
Edwards ST, Peterson K, Chan B, Anderson J, Helfand M. Effectiveness of Intensive Primary Care Interventions: A Systematic Review. J Gen Intern Med. 2017;32(12):1377-86. doi:https://doi.org/10.1007/s11606-017-4174-z
Totten AM, White-Chu EF, Wasson N, Morgan E, Kansagara D, Davis-O’Reilly C, et al.Home-based primary care interventions. Review. Rockville, MD: Agency for Healthcare Research and Quality2016 02 Contract No.: 16.
Balaban RB, Galbraith AA, Burns ME, Vialle-Valentin CE, Larochelle MR, Ross-Degnan D. A patient navigator intervention to reduce hospital readmissions among high-risk safety-net patients: a randomized controlled trial. J Gen Intern Med. 2015;30(7):907-15.
Boult C, Reider L, Leff B, Frick KD, Boyd CM, Wolff JL, et al. The effect of guided care teams on the use of health services: results from a cluster-randomized controlled trial. Archives of internal medicine. 2011;171(5):460-6.
Coleman EA, Grothaus LC, Sandhu N, Wagner EH. Chronic care clinics: a randomized controlled trial of a new model of primary care for frail older adults. J Am Geriatr Soc. 1999;47(7):775-83. doi:https://doi.org/10.1111/j.1532-5415.1999.tb03832.x
Coleman EA, Parry C, Chalmers S, Min SJ. The care transitions intervention: results of a randomized controlled trial. Arch Intern Med. 2006;166(17):1822-8. doi:https://doi.org/10.1001/archinte.166.17.1822
Hughes SL, Cummings J, Weaver F, Manheim LM, Conrad KJ, Nash K. A randomized trial of Veterans Administration home care for severely disabled veterans. Med Care. 1990;28(2):135-45. doi:https://doi.org/10.1097/00005650-199002000-00004
Hughes SL, Weaver FM, Giobbie-Hurder A, Manheim L, Henderson W, Kubal JD, et al. Effectiveness of team-managed home-based primary care: a randomized multicenter trial. Jama. 2000;284(22):2877-85. doi:https://doi.org/10.1001/jama.284.22.2877
Lin MP, Blanchfield BB, Kakoza RM, Vaidya V, Price C, Goldner JS, et al.ED-based care coordination reduces costs for frequent ED users. Am J Manag Care. 2017;23(12):762-6.
Linden A, Butterworth S. A comprehensive hospital-based intervention to reduce readmissions for chronically ill patients: a randomized controlled trial. Am J Manag Care. 2014;20(10):783-92.
Naylor MD, Brooten D, Campbell R, Jacobsen BS, Mezey MD, Pauly MV, et al. Comprehensive discharge planning and home follow-up of hospitalized elders: a randomized clinical trial. Jama. 1999;281(7):613-20. doi:https://doi.org/10.1001/jama.281.7.613
Newcomer R, Maravilla V, Faculjak P, Graves MT. Outcomes of preventive case management among high-risk elderly in three medical groups: a randomized clinical trial. Eval Health Prof. 2004;27(4):323-48.
Parry C, Min S-J, Chugh A, Chalmers S, Coleman EA. Further application of the care transitions intervention: results of a randomized controlled trial conducted in a fee-for-service setting. Home Health Care Serv Q. 2009;28(2-3):84-99.
Peikes D, Chen A, Schore J, Brown R. Effects of care coordination on hospitalization, quality of care, and health care expenditures among Medicare beneficiaries: 15 randomized trials. Jama. 2009;301(6):603-18.
Shannon GR, Wilber KH, Allen D. Reductions in costly healthcare service utilization: findings from the Care Advocate Program. J Am Geriatr Soc. 2006;54(7):1102-7. doi:https://doi.org/10.1111/j.1532-5415.2006.00799.x
Shumway M, Boccellari A, O’Brien K, Okin RL. Cost-effectiveness of clinical case management for ED frequent users: results of a randomized trial⋆. Am J Emerg Med. 2008;26(2):155-64.
Sledge WH, Brown KE, Levine JM, Fiellin DA, Chawarski M, White WD, et al. A randomized trial of primary intensive care to reduce hospital admissions in patients with high utilization of inpatient services. Dis Manag. 2006;9(6):328-38. doi:https://doi.org/10.1089/dis.2006.9.328
Zulman DM, Pal Chee C, Ezeji-Okoye SC, Shaw JG, Holmes TH, Kahn JS, et al. Effect of an Intensive Outpatient Program to Augment Primary Care for High-Need Veterans Affairs Patients: A Randomized Clinical Trial. JAMA Intern Med. 2017;177(2):166-75. doi:https://doi.org/10.1001/jamainternmed.2016.8021
Capp R, Misky GJ, Lindrooth RC, Honigman B, Logan H, Hardy R, et al. Coordination program reduced acute care use and increased primary care visits among frequent emergency care users. Health Affairs. 2017;36(10):1705-11.
Crane S, Collins L, Hall J, Rochester D, Patch S. Reducing utilization by uninsured frequent users of the emergency department: combining case management and drop-in group medical appointments. J Am Board Fam Med. 2012;25(2):184-91. doi:https://doi.org/10.3122/jabfm.2012.02.110156
Gardner R, Li Q, Baier RR, Butterfield K, Coleman EA, Gravenstein S. Is implementation of the care transitions intervention associated with cost avoidance after hospital discharge? J Gen Intern Med. 2014;29(6):878-84.
Hamar B, Rula EY, Wells AR, Coberley C, Pope JE, Varga D. Impact of a scalable care transitions program for readmission avoidance. Am J Manag Care. 2016;22(1):28-34.
Meret-Hanke LA. Effects of the program of all-inclusive care for the elderly on hospital use. The Gerontologist. 2011;51(6):774-85.
Schubert CC, Myers LJ, Allen K, Counsell SR. Implementing Geriatric Resources for Assessment and Care of Elders Team Care in a Veterans Affairs Medical Center: Lessons Learned and Effects Observed. J Am Geriatr Soc. 2016;64(7):1503-9. doi:https://doi.org/10.1111/jgs.14179
Shah R, Chen C, O’Rourke S, Lee M, Mohanty SA, Abraham J. Evaluation of care management for the uninsured. Med Care. 2011;49(2):166-71. doi:https://doi.org/10.1097/MLR.0b013e3182028e81
Sommers LS, Marton KI, Barbaccia JC, Randolph J. Physician, nurse, and social worker collaboration in primary care for chronically ill seniors. Arch Intern Med. 2000;160(12):1825-33. doi:https://doi.org/10.1001/archinte.160.12.1825
Weerahandi H, Basso Lipani M, Kalman J, Sosunov E, Colgan C, Bernstein S, et al. Effects of a Psychosocial Transitional Care Model on Hospitalizations and Cost of Care for High Utilizers. Soc Work Health Care. 2015;54(6):485-98. doi:https://doi.org/10.1080/00981389.2015.1040141
Finkelstein A, Zhou A, Taubman S, Doyle J. Health Care Hotspotting - A Randomized, Controlled Trial. N Engl J Med. 2020;382(2):152-62. doi:https://doi.org/10.1056/NEJMsa1906848
Yoon J, Chang E, Rubenstein LV, Park A, Zulman DM, Stockdale S, et al. Impact of Primary Care Intensive Management on High-Risk Veterans’ Costs and Utilization: A Randomized Quality Improvement Trial. Ann Intern Med. 2018;168(12):846-54. doi:https://doi.org/10.7326/M17-3039
Brown R, Peikes D, Chen A, Ng J, Schore J, Soh C, editors. The evaluation of the Medicare coordinated care demonstration: Findings for the first two years. Second Report to Congress. Mathematica Policy Research, Inc. Princeton, NJ; 2007.
Wolfe A. Institute of Medicine report: crossing the quality chasm: a new health care system for the 21st century. Policy, Politics, & Nursing Practice. 2001;2(3):233-5.
Elhauge E. The fragmentation of US health care: causes and solutions: Oxford University Press on Demand; 2010.
Curran GM, Bauer M, Mittman B, Pyne JM, Stetler C. Effectiveness-implementation hybrid designs: combining elements of clinical effectiveness and implementation research to enhance public health impact. Med Care. 2012;50(3):217-26. doi:https://doi.org/10.1097/MLR.0b013e3182408812
Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009;4(1):50.
Rabin BA, McCreight M, Battaglia C, Ayele R, Burke RE, Hess PL, et al. Systematic, Multimethod Assessment of Adaptations Across Four Diverse Health Systems Interventions. Front Public Health. 2018;6:102. doi:https://doi.org/10.3389/fpubh.2018.00102
Glasgow RE, Vogt TM, Boles SM. Evaluating the public health impact of health promotion interventions: the RE-AIM framework. Am J Public Health. 1999;89(9):1322-7. doi:https://doi.org/10.2105/ajph.89.9.1322
Wray LO, Szymanski BR, Kearney LK, McCarthy JF. Implementation of primary care-mental health integration services in the Veterans Health Administration: program activity and associations with engagement in specialty mental health services. J Clin Psychol Med Settings. 2012;19(1):105-16. doi:https://doi.org/10.1007/s10880-011-9285-9
Fulton J, Williams J, LeBlanc T, McDuffie J, Porter K, Adam S, et al. Integrated Outpatient Palliative Care in Oncology. VA ESP. 2017.
Funding
This work was supported by VA Health Services Research & Development funding for ESP (VA-ESP Project No. 09-009; 2020). The funder had no role in study design, data collection, analysis and interpretation of data, writing of the report, or decision to submit article for publication.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they do not have a conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM 1
(DOCX 145 kb)
Rights and permissions
About this article

Cite this article
Duan-Porter, W., Ullman, K., Majeski, B. et al. Care Coordination Models and Tools—Systematic Review and Key Informant Interviews. J GEN INTERN MED 37, 1367–1379 (2022). https://doi.org/10.1007/s11606-021-07158-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-021-07158-w